



Social withdraw and social anxiety are overlapping but distinct concepts, yet little is known about the extent of overlap, the sequential timing of their development, and the mechanisms through which they may become interrelated. This is because few studies have linked developmental and clinical approaches in the study of social withdrawal and social anxiety (Kingerly, Erdley, Marshall, Whitaker, & Reuter, Reference Kingerly, Erdley, Marshall, Whitaker and Reuter2010). The current study combines these two approaches by taking a developmental psychopathology perspective. Through this framework, we aim to better understand how social withdrawal and social anxiety influence one another, concurrently and longitudinally at the within-person level, and how they are related to peer victimization and peer acceptance. We use longitudinal data spanning 6 years from a large population-based and a clinically referred cohort to investigate within-person cross-lagged associations between self-reported social withdrawal, parent-reported social withdrawal, and self-reported social anxiety, peer victimization, and perceived peer acceptance during early and middle adolescence (ages 11 to 16 years).
Social Withdrawal and Social Anxiety: Overlapping But Distinct Concepts
Social withdrawal is an umbrella term referring to an individual's voluntary self-isolation from familiar or unfamiliar peers through consistent display of solitary behaviors (Rubin, Coplan, & Bowker, Reference Rubin, Coplan and Bowker2009), such as spending excessive time alone and avoiding peer interaction. Underlying motivations to withdraw may differ between individuals (Asendorpf, Reference Asendorpf1990; Wang, Rubin, Laursen, Booth-LaForce, & Rose-Krasnor, Reference Wang, Rubin, Laursen, Booth-LaForce and Rose-Krasnor2013). In the current manuscript, we use the term social withdrawal to refer to the global, multidimensional, behavioral phenotype of voluntary self-isolation. Social anxiety refers to the marked and persistent fear of situations involving social interaction due to the potential for judgment, negative evaluation, or rejection (Rapee & Heimberg, Reference Rapee and Heimberg1997). Positive moderate concurrent correlations between social withdrawal and social anxiety have been reported (e.g., Biggs, Vernberg, & Wu, Reference Biggs, Vernberg and Wu2012; Erath, Flanagan, & Bierman, Reference Erath, Flanagan and Bierman2007; Smith, Barstead, & Rubin, Reference Smith, Barstead and Rubin2017). However, while high levels of withdrawal or social anxiety may place individuals at higher risk for the other, not all withdrawn youth become more socially anxious and not all socially anxious youth become more withdrawn. In a study that examined the categorical overlap between social withdrawal and social anxiety, 30% of withdrawn youth met the criteria for social anxiety disorder (compared to 12.5% of nonwithdrawn youth; Gazelle, Workman, & Allen, Reference Gazelle, Workman and Allan2010). The authors did not report the percentage of socially anxious youth who were withdrawn. Results from these studies point toward a distinction in concepts, but do not offer insights into the order, timing, or mechanisms that link social withdrawal and social anxiety.
The Social Withdrawal and Social Anxiety Feedback Loop
Much of the research that assesses both social withdrawal and social anxiety has been guided by the idea that these constructs may have a bidirectional, cyclical influence on one another. Rubin et al. (Reference Rubin, Coplan and Bowker2009) theorized that there may be a feedback loop from increasing social anxiety to increasing withdrawal to increasing social anxiety, and so on. This feedback loop suggests two temporal sequences: from social anxiety to social withdrawal; and from social withdrawal to social anxiety. In the first sequence, social anxiety contributes to increasing withdrawal over time. When in social situations, adolescents experiencing social anxiety may start to withdraw in order to manage or decrease their fears. The decrease of anxiety during periods of withdrawal reinforces future withdrawal behaviors, and through this reinforcement, social anxiety may lead to increasing withdrawal over time. The effect of social anxiety on social withdrawal has been tested in two studies, both in population-based samples. The first found that social anxiety was marginally concurrently associated with high withdrawal in 84 young adolescents (Erath et al., Reference Erath, Flanagan and Bierman2007); the other found that social anxiety predicted high social withdrawal 2 months later in girls, but not in boys, in a sample of 214 adolescents (Biggs et al., Reference Biggs, Vernberg and Wu2012).
In the second sequence, social withdrawal contributes to increasing social anxiety over time. Social withdrawal interferes with friendship formation and the development and practice of social skills. When in social situations, withdrawn youth may be socially ill equipped and, consequently, experience negative appraisals from others and negative self-appraisals of their social performance (Kingerly et al., Reference Kingerly, Erdley, Marshall, Whitaker and Reuter2010; Rubin et al., Reference Rubin, Coplan and Bowker2009). Repeated negative social interactions could exacerbate social anxiety. Three studies have found evidence for this sequence. Social withdrawal at 8 years of age was associated with increased rates of social anxiety a decade later in a study by Goodwin, Fergusson, and Horwood (Reference Goodwin, Fergusson and Horwood2004); in addition, Smith et al. (Reference Smith, Barstead and Rubin2017) found that social withdrawal in early adolescence was associated with increases in general anxiety (not specifically social anxiety) 1 year later, after controlling for baseline internalizing problems. Ding et al. (Reference Ding, Coplan, Deng, Ooi, Li and Sang2018) explored the associations between social anxiety and three motivational aspects underlying social withdrawal: social avoidance, shyness, and unsociability. Bidirectional effects could only be tested between social avoidance and social anxiety. In their sample of 601 Chinese youth (ages 10 to 12 years), they did not find any cross-lagged associations between social avoidance and social anxiety across a 9-month time interval. They did, however, find that shyness and unsociability had an effect on social anxiety, but reciprocal effects (from social anxiety to shyness and unsociability) were not tested.
These previous studies on the association between social withdrawal and social anxiety had several limitations. Most were cross-sectional and assessed social withdrawal and social anxiety only once, and the few studies that did explore longitudinal associations between withdrawal and social anxiety yielded results that can be interpreted solely at the between-person level. In other words, the body of work conducted thus far has not yet disaggregated between-person differences from within-person processes. The between-person level provides information about interindividual differences in traits, such as whether adolescents who are more socially anxious are also more socially withdrawn. Intraindividual changing states of social withdrawal or social anxiety cannot be captured at the between-person level. The feedback loop suggested by previous research is a process that occurs at the within-person level. In contrast to between-person hypotheses, investigating within-person processes can reveal if individuals become more withdrawn when they experience a prior increase in social anxiety, or vice versa. Untangling within- from between-person effects is important because analyses at the two levels may produce divergent or conflicting results. For example, adolescents who are more withdrawn tend to be more socially anxious (between person), but if adolescents become more withdrawn over time, their social anxiety levels may still remain stable, or even decrease, over time (within person).
The Role of Peer Victimization and Peer Acceptance
Both social withdrawal and social anxiety occur in response to or in relation to one's peers, who become increasingly important for youth's social functioning during early adolescence. Peer victimization and peer acceptance are two peer experiences that are highly relevant to adolescent adjustment. Both have been suggested to be predictors, correlates, or consequences of social withdrawal (Rubin et al., Reference Rubin, Coplan and Bowker2009) and social anxiety (Epkins & Heckler, Reference Epkins and Heckler2011) and may be a potential mechanism linking social withdrawal and social anxiety over time. To illustrate, socially withdrawn and socially anxious youth are both more likely than nonwithdrawn and nonanxious youth to be victimized because they are perceived as “easy targets” who are unlikely to retaliate (Burgess, Wojslawowicz, Rubin, Rose-Krasnor, & Booth-LaForce, Reference Burgess, Wojslawowicz, Rubin, Rose-Krasnor and Booth-LaForce2006; Hodges & Perry, Reference Hodges and Perry1999). Victimized youth may withdraw from peers to cope with and attempt to decrease victimization (Gazelle & Rudolph, Reference Gazelle and Rudolph2004), and form negative self-evaluations that exacerbate social anxiety (Siegel, La Greca, & Harrison, Reference Siegel, La Greca and Harrison2009).
Peer acceptance may also influence and be influenced by social withdrawal and social anxiety. When peer acceptance is high, youth increase their motivation to engage with peers, thereby decreasing social withdrawal (Gazelle & Rudolph, Reference Gazelle and Rudolph2004). When withdrawal decreases, youth have more opportunities to disprove negative self-evaluations, thereby lowering social anxiety (Biggs, Sampilo, & McFadden, Reference Biggs, Sampilo, McFadden, Alfano and Beidel2011). Lower anxiety and lower withdrawal are, in turn, related to higher peer acceptance (Boivin, Hymel, & Bukowski, Reference Boivin, Hymel and Bukowski1995; Chang, Reference Chang2004; Epkins & Heckler, Reference Epkins and Heckler2011), perpetuating a protective peer acceptance loop.Footnote 1
The—possibly bidirectional—associations between social withdrawal, social anxiety, and peer victimization or peer acceptance have not been tested thus far. Two cross-sectional studies examined peer experiences as outcomes in the social withdrawal and social anxiety pathway. In these studies, higher social anxiety was associated with higher social withdrawal, which in turn was associated with higher peer victimization, lower peer acceptance (Erath et al., Reference Erath, Flanagan and Bierman2007), and lower friend companionship (Biggs et al., Reference Biggs, Vernberg and Wu2012). Again, these studies were cross-sectional, preventing conclusions about the temporal sequencing of events. In the only longitudinal study linking social withdrawal, social anxiety, and peer acceptance, Teachman and Allen (Reference Teachman and Allen2007) found that low peer acceptance mediated the association between social withdrawal in early adolescence and social anxiety in late adolescence. Alternative directions of effects among these variables were not tested. The limited research on where certain peer experiences fit in the withdrawal–social anxiety feedback loop precludes conclusions about the specific order or strength of effects. Of note, previous studies suggest between-person differences in the relationships between social withdrawal, social anxiety, and peer experiences, but no study to date has investigated if within-person changes in peer experiences influence within-person changes in social withdrawal or social anxiety.
Overview of the Current Study
In sum, few studies have measured both social withdrawal and social anxiety in the same sample, and none have examined the temporal sequencing of these constructs. Our study adds to the existing body of literature in four important ways. First, we investigated if the relationship between social withdrawal and social anxiety is bidirectional, as has been suggested. Second, we investigated two peer variables, peer victimization and perceived peer acceptance, as potential mechanisms in the longitudinal relationship between social withdrawal and social anxiety. More specifically, we tested whether peer victimization and acceptance predicted, mediated, or resulted from the withdrawal–social anxiety pathway. Third, using random intercept cross-lagged panel models allowed us to disentangle the within-person processes from stable between-person differences. The previous studies conducted on social anxiety and social withdrawal only reported between-person effects. Focusing on within-person processes is a developmentally relevant, person-centered approach for examining the associations between social withdrawal, social anxiety, peer victimization, and peer acceptance over time. Fourth, whereas the experience of social anxiety is intrinsically individual and can therefore only be assessed by means of self-report, social withdrawal can also be observed (and rated) by others. The current study investigated within-person associations with both self-reported social withdrawal and parent-reported social withdrawal in order to explore how pathways differ by informant of withdrawn behaviors.
Method
Participants
The data used in this study came from the first three measurement waves of a population-based and a clinically referred cohort, together forming the Tracking Adolescents' Individual Lives Survey (TRAILS). TRAILS is a prospective cohort study aiming to track the social, psychological, and physical development of preadolescents throughout adolescence and young adulthood. Extensive information about the recruitment, representativeness, and assessment procedure has been reported by De Winter et al. (Reference De Winter, Oldehinkel, Veenstra, Brunnekreef, Verhulst and Ormel2005), Huisman et al. (Reference Huisman, Oldehinkel, de Winter, Minderaa, de Bildt, Huizink and Verhulst2008), and Oldehinkel et al. (Reference Oldehinkel, Rosmalen, Buitelaar, Hoek, Ormel, Raven and Reijneveld2005).
The population-based cohort consisted of 2,229 participants (response rate 76%) during the first measurement wave in 2001 (Time 1 [T1]; M ageT1 = 11.11, SD = 0.56; 50.7% female). The participants were born between October 1989 and September 1991 and resided in the North of the Netherlands. The two subsequent waves, Time 2 and Time 3 (T2 and T3), occurred every 2 or 3 years, and included 81%–96% of the T1 participants. The first measurement wave of the clinically referred cohort was in 2004, when 543 participants (M ageT1 = 11.11, SD = 0.50; 34.1% female) were recruited from one of two child psychiatric outpatient clinics in the North of the Netherlands. Inclusion criterion was a referral to one of these two clinics at any point in life. Comparable to the population-based cohort, the two subsequent waves occurred every 2 or 3 years, and included 77%–85% of the T1 participants.
Aggregating the data from the two cohorts resulted in 2,772 participants approximately 11 years of age at T1, 13 years at T2, and 16 years at T3 (M ageT1 = 11.11, SD = 0.55; M ageT2 = 13.44, SD = 0.61; M ageT3 = 16.21; SD = 0.72; 47.5% female). The large majority of participants were from an ethnically Dutch origin (88.6%). Table 1 shows the participant demographics at each measurement wave of the TRAILS population-based and clinically referred cohorts and of the total sample.
Table 1. Participant demographics at each measurement wave of the TRAILS population-based and clinically referred cohorts and the total sample

Note: Other refers to ethnicities including Surinam, Antillean, Indonesian, Turkish, Moroccan, or another ethnicity not specified.
Data collection procedure
The TRAILS study was approved by the Dutch Central Committee on Research Involving Human Subjects. Adolescent participants of the study provided written consent at the second and third measurement waves. A parent or guardian provided written parental consent for adolescent participation and written consent to participate at all measurement waves. At the first measurement wave, well-trained interviewers visited one of the parents or guardians (95.6% mothers) at home to conduct interviews regarding their child's developmental history and somatic health. Additional interviews about parental psychopathology were also conducted. During the visit, parents also completed a written questionnaire. During the second and third measurement waves, parents completed a questionnaire that they received via mail. At the first through third measurement waves, adolescents completed questionnaires in groups at school, under the supervision of at least one research assistant.
Measures
Self-reported social withdrawal was assessed at every measurement wave by four items from the Youth Self-Report (YSR; Achenbach, Reference Achenbach2001) depressive/withdrawn scale. In a sample of 11- to 18-year-olds, the YSR withdrawn/depressed scale had moderate 8-day test–retest reliability (r = .67), and scores were positively correlated with measures of withdrawal (rs > .58, ps < .001; Achenbach & Rescorla, Reference Achenbach and Rescorla2007). Items used in the current study were selected based on face validity and previous research: “I would rather be alone than with others,” “I am secretive or keep things to myself,” “I refuse to talk,” and “I keep from getting involved with others.” All depression items from the depressive/withdrawn scale were excluded. Although fitting in our global conceptualization of social withdrawal, the “I am too shy or timid” item was also excluded due to the item's overlap with social anxiety. Several previous studies have used these withdrawal-related items, or similar items from the depressive/withdrawn scale, to measure social withdrawal or related constructs in childhood, adolescence, and early adulthood (Barzeva, Meeus, & Oldehinkel, Reference Barzeva, Meeus and Oldehinkel2019; Booth-LaForce & Oxford, Reference Booth-LaForce and Oxford2008; Eggum et al., Reference Eggum, Eisenberg, Spinrad, Valiente, Edwards, Kupfer and Reiser2009; Tang et al., Reference Tang, Van Lieshout, Lahat, Duku, Boyle, Saigal and Schmidt2017). These items were found to be longitudinally measurement invariant in the current study (see online-only Supplementary Materials, Table S.4 and S.5), and from adolescence to early adulthood in a previous study (Barzeva et al., Reference Barzeva, Meeus and Oldehinkel2019). A group of adolescents who endorsed persistently high levels of global social withdrawal, as assessed by these items (and the “too shy or timid” item), had significantly higher levels of shyness, general anxiety, and reduced social contact, and lower social affiliation, compared to a group endorsing low levels of withdrawal (Barzeva et al., Reference Barzeva, Meeus and Oldehinkel2019). These results point to the validity for using these withdrawal-related items to measure social withdrawal in adolescence. Items were rated on a 3-point scale, with 0 = not true, 1 = somewhat or sometimes true, and 2 = very or often true in the past 6 months. Cronbach's α for the four YSR items at T1 to T3 was .49, .55, and .62, respectively. Greatest lower bound (GLB), a preferred alternative to α that indicates the smallest possible reliability coefficient that is still consistent with the data structure (Ten Berge & Socan, Reference Ten Berge and Socan2004; Trizano-Hermosilla & Alvarado, Reference Trizano-Hermosilla and Alvarado2016), for these items was .55, .61, and .67 at T1 to T3, respectively.
Parent-reported social withdrawal was measured at all three waves by aggregating the same four items from the parent-report Child Behavioral Checklist (CBCL; Achenbach & Rescorla, Reference Achenbach and Rescorla2001) depressive/withdrawn scale as the self-reported social withdrawal items from the YSR. These parent-reported social withdrawal items were found to be longitudinally measurement invariant from T1 to T3 (see online-only Supplementary Materials, Tables S.4 and S.6), indicating that parents interpreted items in the same way at each measurement wave. Cronbach's α for the four CBCL items at T1 to T3 was .66, .67, and .71, respectively. GLB for these items was .70, .76, and .78 at T1 to T3, respectively.
Although our preregistered analytic plans intended to aggregate the self- and parent-reported social withdrawal items in a single social withdrawal variable, we could not meet the assumptions required to validly combine the social withdrawal data from these two informants. More specifically, the weak correlations between self- and parent-reported social withdrawal items, as well as the lack of convergence when attempting to specify a model that aggregates self- and parent-reported social withdrawal items, indicated that adolescents and their parents had unique views on adolescents’ withdrawn behavior that differed substantially from one another. We therefore decided to examine self-reported and parent-reported social withdrawal as separate variables that capture distinct, but equally valid, perspectives of withdrawn behaviors.
Social anxiety was measured at every wave by the nine-item social phobia subscale of the self-report Revised Children's Anxiety and Depression Scale (Chorpita, Yim, Moffitt, Umemoto, & Francis, Reference Chorpita, Yim, Moffitt, Umemoto and Francis2000). Items in this scale assess symptoms of social anxiety, including “I worry what other people think of me” and “I feel afraid that I will make a fool of myself in front of people.” Responses are given on a 4-point Likert-type scale (0 = never, 1 = sometimes, 2 = often, 3 = always). In another sample of Dutch early adolescents, the social phobia subscale had good 3-month stability (ICC = .84) and was sensitive to change up to 12 months postintervention for anxiety and depression (Kösters, Chinapaw, Zwaanswijk, van der Wal, & Koot, Reference Kösters, Cinapaw, Zwaanswijk, van der Wal and Koot2015). Cronbach's α for T1 to T3 in the current sample was .78, .85, and .86, respectively, and GLB was .82, .88, and .90, respectively.
Peer victimization was measured at every wave by aggregating the self-report YSR item “I get teased a lot” and the CBCL item “Gets teased a lot” via their mean item score. Items were rated on a 3-point scale, with 0 = not true, 1 = somewhat or sometimes true, and 2 = very or often true in the past 6 months. This item is from the social problems subscale of the YSR and CBCL and can be used to assess potential peer victimization (La Greca, Lai, Chan, & Herge, Reference La Greca, Lai, Herge, Chan, McLeod, Jensen-Doss and Ollendick2013; La Greca & Landoll, Reference La Greca, Landoll, Silverman and Field2011). Preliminary validity information for this single-item measure of peer victimization comes from two studies. The first study reported that the teacher-report version of this item was significantly moderately correlated with maternal and paternal reports of a two-item victimization scale (Kerr, Gini, Own, & Capaldi, Reference Kerr, Gini, Owen and Capaldi2018). The second found that when children reported being teased in an autism diagnostic interview, 88.9% of parents also indicated that their child was victimized with the CBCL peer victimization item (Nowell, Brewton, & Goin-Kochel, Reference Nowell, Brewton and Goin-Kochel2014). Similar single-item peer victimization scales are widely used (e.g., Branson & Cornell, Reference Branson and Cornell2009; Fekkes, Pijpers, Fredriks, Vogels, & Verloove-Vanhorick, Reference Fekkes, Pijpers, Fredriks, Vogels and Verloove-Vanhorick2006; Giletta, Scholte, Engels, & Larsen, Reference Giletta, Scholte, Engels and Larsen2010; Larsen et al., Reference Larsen, Vermulst, Eisinga, English, Gross, Hofman and Scholte2012; Solberg & Olweus, Reference Solberg and Olweus2003). Correlations between the YSR and CBCL victimization items at T1 to T3 were r = .44, .44, and .41, respectively. The peer victimization variable therefore reflects child and/or parent reports of being bullied.
Perceived peer acceptance was measured at every wave by the mean score of four items of the classmate affection subscale and four items of the classmate behavioral affirmation subscale of the self-report Social Production Function (Lindenberg, Reference Lindenberg, Ganzeboom and Lindenberg1996; Ormel, Lindenberg, Steverink, & Vonkorff, Reference Ormel, Lindenberg, Steverink and Vonkorff1997). This self-report measure includes items such as “Many classmates like to do things together with me,” “Many classmates help me if there is something I need help with,” and “I can really trust my classmates.” Responses are given on a 5-point Likert scale from 1 = never to 5 = always and higher scores indicate greater perceived well-being among peers. Previous research in early adolescence has reported that these perceived peer acceptance subscales are not associated with future levels of delinquency (van der Laan, Veenstra, Bogaerts, Verhulst, & Ormel, Reference van der Laan, Veenstra, Bogaerts, Verhulst and Ormel2010) and there is no difference between truants and nontruants on these subscales (Veenstra, Lindenberg, Tinga, & Ormel, Reference Veenstra, Lindenberg, Tinga and Ormel2010). However, lower levels of perceived peer acceptance was significantly associated with suicidal ideation (Herba et al., Reference Herba, Ferdinand, Stijnen, Veenstra, Oldehinkel, Ormel and Verhulst2008). Test–retest reliability for the Social Production Function has not been investigated. Results from our longitudinal measurement invariance test (see Statistical Analyses section and Supplementary Materials, Tables S.4 and S.8) concluded that youth interpreted the perceived peer acceptance items consistently across all measurement waves, thereby providing evidence for the reliability of these eight items. Cronbach's α for the eight items at T1 to T3 was .91, .89, and .88, and GLB was .93, .91, and .91, respectively.
Statistical analyses
Analyses were conducted in MPlus Version 8.0 (Muthén & Muthén, Reference Muthén and Muthén1998–2017) using maximum likelihood with robust standard errors estimation. All analyses were preregistered on the Open Science Framework (osf.io/mztf5). First, an a priori Monte Carlo simulation was conducted to determine if our sample size of 2,772 was sufficiently large to detect effects in the subsequent random intercept cross-lagged panel models (RI-CLPMs; Muthén & Muthén, Reference Muthén and Muthén2002). RI-CLPM is a modified version of the traditional cross-lagged panel model that disentangles the within-person process from stable between-person differences through the inclusion of a random intercept (Hamaker, Kuiper, & Grasman, Reference Hamaker, Kuiper and Grasman2015). This model requires at least three waves of data and is “considered quite suitable to determine ‘what comes first’” (Keijsers, Reference Keijsers2016). Masselink et al. (Reference Masselink, Van Roekel, Hankin, Keijsers, Lodder, Vanhalst and Oldehinkel2018) investigated the power of RI-CLPMs, in comparison to the traditional cross-lagged panel model. They reported that a large sample size (>1500) would be needed to detect small effects (.11–.12) within a three-wave RI-CLPM (see Appendix A of Masselink et al., Reference Masselink, Van Roekel, Hankin, Keijsers, Lodder, Vanhalst and Oldehinkel2018); however, each RI-CLPM requires its own power analysis because of the variation in expected effect sizes, variance distributions, number of measurement waves, and amount of missing data. More information about the procedure of the a priori power analysis of the current study can be found in the online-only Supplementary Materials of the current manuscript. Next, to get a preliminary understanding of how much variance in our variables stems from between-group differences versus within-person fluctuations, we calculated the intraclass correlations (ICCs) for self-reported social withdrawal, parent-reported social withdrawal, and self-reported social anxiety, peer victimization, and perceived peer acceptance. A high ICC (>.50) indicates proportionately higher between-group variance while a low ICC (<.50) indicates proportionately higher within-person variance. We then checked longitudinal measurement invariance for the self-reported social withdrawal, and parent-reported social withdrawal, social anxiety, and perceived peer acceptance items. Longitudinal measurement invariance could not be tested for peer victimization because there were too few items to investigate model fit via structural equation modeling. More information about the analytic procedure of the longitudinal measurement invariance testing can be found in the online-only Supplementary Materials.
The first RI-CLPM (RI-CLPM 1) modeled the associations between self-reported social withdrawal, parent-reported social withdrawal, and social anxiety over the three measurement waves. Following the procedure described by Hamaker et al. (Reference Hamaker, Kuiper and Grasman2015) and by Keijsers (Reference Keijsers2016), we specified the first RI-CLPM by regressing each observed score on its own latent factor, with each loading constrained at 1, resulting in nine latent factors, namely, self-reported social withdrawal, parent-reported social withdrawal, and social anxiety at three time points each. We specified the stability paths, T1 correlations, within-wave associations, and cross-lagged effects between the latent self-reported withdrawal, latent parent-reported withdrawal, and latent social anxiety variables. Three random intercept factors were added to capture the between-person differences in self-reported withdrawal, parent-reported withdrawal, and social anxiety. The observed scores and indicators of these factors, and all factor loadings, were constrained to 1. The variances of the observed scores were constrained to zero, forcing all variation in the observed measures to be captured by the within- and between-person latent factor structure. The correlations between the overarching latent factors reflect how stable between-person differences in self-reported social withdrawal, parent-reported social withdrawal, and social anxiety are associated with each other. To interpret results at the within-person level, we examined the stability paths, T1 correlations, within-wave associations, and cross-lagged effects. The stability paths indicate the extent to which within-person deviations in the level of social withdrawal or social anxiety can be predicted by the individual's prior deviation from his or her own scores. The T1 correlations indicate whether individuals’ deviations from their own expected scores in one variable are linked to deviations from their own scores in another, while the within-wave correlations indicate if within-person changes in withdrawal are linked to within-person changes in social anxiety. The cross-lagged effects indicate whether within-person changes in one variable are predicted by deviations from their own expected scores on another variable, assessed one measurement wave earlier.
In subsequent RI-CLPMs, we examined self-reported social withdrawal and parent-reported social withdrawal in separate models that included social anxiety and either peer victimization or perceived peer acceptance. Due to a lack of power, we could not examine both self- and parent-reported social withdrawal in one model. This led to the building of four additional RI-CLPMs including the following three variables at every time point: RI-CLPM 2, self-reported social withdrawal, social anxiety, and peer victimization; RI-CLPM 3, parent-reported social withdrawal, and self-reported social anxiety and peer victimization; RI-CLPM 4, self-reported social withdrawal, social anxiety, and perceived peer acceptance; and RI-CLPM 5, parent-reported social withdrawal, and self-reported social anxiety and perceived peer acceptance. These models were used to investigate the role of peers in the withdrawal–anxiety relationships while accounting for differences in self-reported withdrawal and parent-reported withdrawal. The peer-related RI-CLPMs were specified in the same way as the first model, resulting in nine within-person latent factors and three overarching between-person random intercept factors per model. For all RI-CLPMs, good model fit was determined by the following criteria: comparative fit index (CFI) >.90; standardized root mean residual (SRMR) <.08; and root mean square error of approximation (RMSEA) <.06.
As a sensitivity check, we tested for differences between girls and boys for all five RI-CLPMs by specifying gender as a grouping variable and setting the intercepts for all RI-CLPM latent and observed variables to 0 for identification. First, we ran a freely estimated model, where girls and boys could differ on all parameters (i.e., stabilities, within-wave associations, and cross-paths). Good model fit was determined by the following criteria: CFI > .90, SRMR < .08, RMSEA < .06. Second, we constrained all parameters to be equal between girls and boys and compared the model fit between the freely estimated and constrained models via the Satorra–Bentler scaled chi-square difference test (ΔSBχ2; Satorra & Bentler, Reference Satorra and Bentler2001). When the model fit of the constrained model was significantly worse than the freely estimated model, we checked the modification indices for suggestions about which parameter to free to improve model fit. Parameters were freed until the partly constrained model fit the data as well as the freely estimated model. The freed parameters give insight into which parameters differ between girls and boys. As an additional sensitivity check, we excluded the 543 participants from the clinically referred cohort and reran the power analyses and all RI-CLPMs (methods and results of the population-based cohort only RI-CLPMs can be found in the online-only Supplementary Materials and Figures S.1–S.3).
Results
A priori power analyses indicated that our sample size is sufficiently large to detect small within-person effects ≥.10 in the RI-CLPMs with power >.80 (see Supplementary Materials for the analytic procedure and results of the Monte Carlo simulations). This means that paths <.10 may be due to chance and will therefore not be interpreted unless a path is <.10 in one RI-CLPM but ≥.10 in another RI-CLPM, for consistency. The means, standard deviations, and correlations of all variables at every measurement wave are reported in Table 2. At the between-person level, self-reported social withdrawal, parent-reported social withdrawal, social anxiety, peer victimization, and perceived peer acceptance were moderately stable over time, with correlations at consecutive waves (i.e., T1 to T2 and T2 to T3) ranging from r = .33 to .61. Self-reported withdrawal and parent-reported withdrawal were weakly correlated both within wave and at consecutive waves (r = .22–.33). Self-reported withdrawal and social anxiety were moderately correlated within wave (r = .33–.35), but parent-reported withdrawal and self-reported social anxiety only weakly (r = .05–.08). The ICCs were .33 for self-reported social withdrawal, .57 for parent-reported social withdrawal, .44 for social anxiety, .38 for peer victimization, and .34 for peer acceptance, indicating that there was sufficient within-person variance to use RI-CLPMs to investigate within-person changes over time. Results from the longitudinal measurement invariance testing are shown in the online-only Supplementary Materials (Tables S.4–S.8). We found partial scalar longitudinal measurement invariance for self-reported social withdrawal, parent-reported social withdrawal, social anxiety, and peer acceptance. This means that informants generally interpreted the items from all variables in the same way over time.
Table 2. Means, standard deviations, and correlations between variables
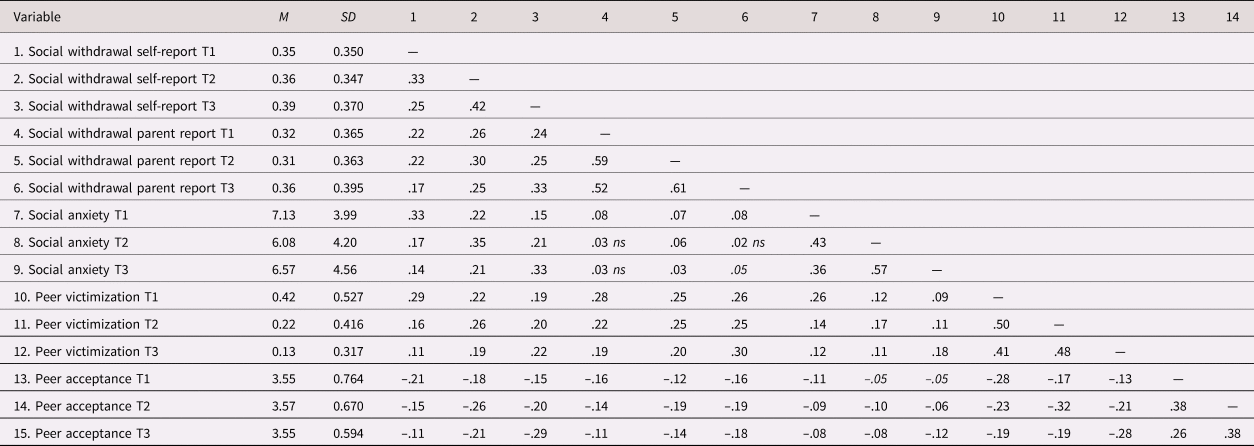
Note: ns, not significant at p < .05; p < .05 in italics; all other correlations were significant at p < .01.
Between-person associations across RI-CLPMs
The lower parts of Figures 1–3 show the between-person associations between variables in RI-CLPMs 1–5. The between-person associations of self-reported withdrawal with all other variables were moderate, indicating that adolescents reporting higher social withdrawal across the three measurement waves had higher parent-reported social withdrawal, higher social anxiety, higher peer victimization, and lower perceived peer acceptance across the three measurement waves than youth with lower withdrawal. The associations between parent-reported withdrawal and self-reported social anxiety were weak and positive in two RI-CLPMs, but nonsignificant in a third, meaning that adolescents who were rated as being more withdrawn by their parents across the three waves were at most somewhat more socially anxious than adolescents who were rated as being less withdrawn. Finally, adolescents with higher parent-reported social withdrawal or higher social anxiety across the three waves were also more victimized and less accepted by peers than nonwithdrawn or non-socially anxious adolescents.
RI-CLPM 1: Self-reported social withdrawal, parent-reported social withdrawal, and social anxiety
In RI-CLPM 1 (Figure 1) we investigated the relationship between self-reported social withdrawal, parent-reported social withdrawal, and social anxiety across three time points. The model had excellent fit to the data: χ2 (3) = 4.254 p = .235; RMSEA = .012, 90% confidence interval; CI [.000, .036]; SRMR = .006; CFI = 1.00. There were no significant within-person stability paths from T1 to T2 for any variables. The stability paths from T2 to T3 were small to moderate and positive for all variables, indicating that within-person deviation from a variable's expected T3 score was predicted by within-person deviations from the variable's expected T2 score. Within-wave associations at the within-person level were moderate and positive between self-reported withdrawal and social anxiety at all time points, meaning that within-person increases in self-reported withdrawal were associated with within-person increases in social anxiety. Within-wave associations were weak between self-reported and parent-reported withdrawal at T2 and T3. No significant associations were found at T1 between self- and parent-reported withdrawal, and at any time point between parent-reported withdrawal and self-reported social anxiety. Finally, one within-person cross-lagged effect emerged: an increase in social anxiety at T1 predicted an increase in self-reported social withdrawal at T2.
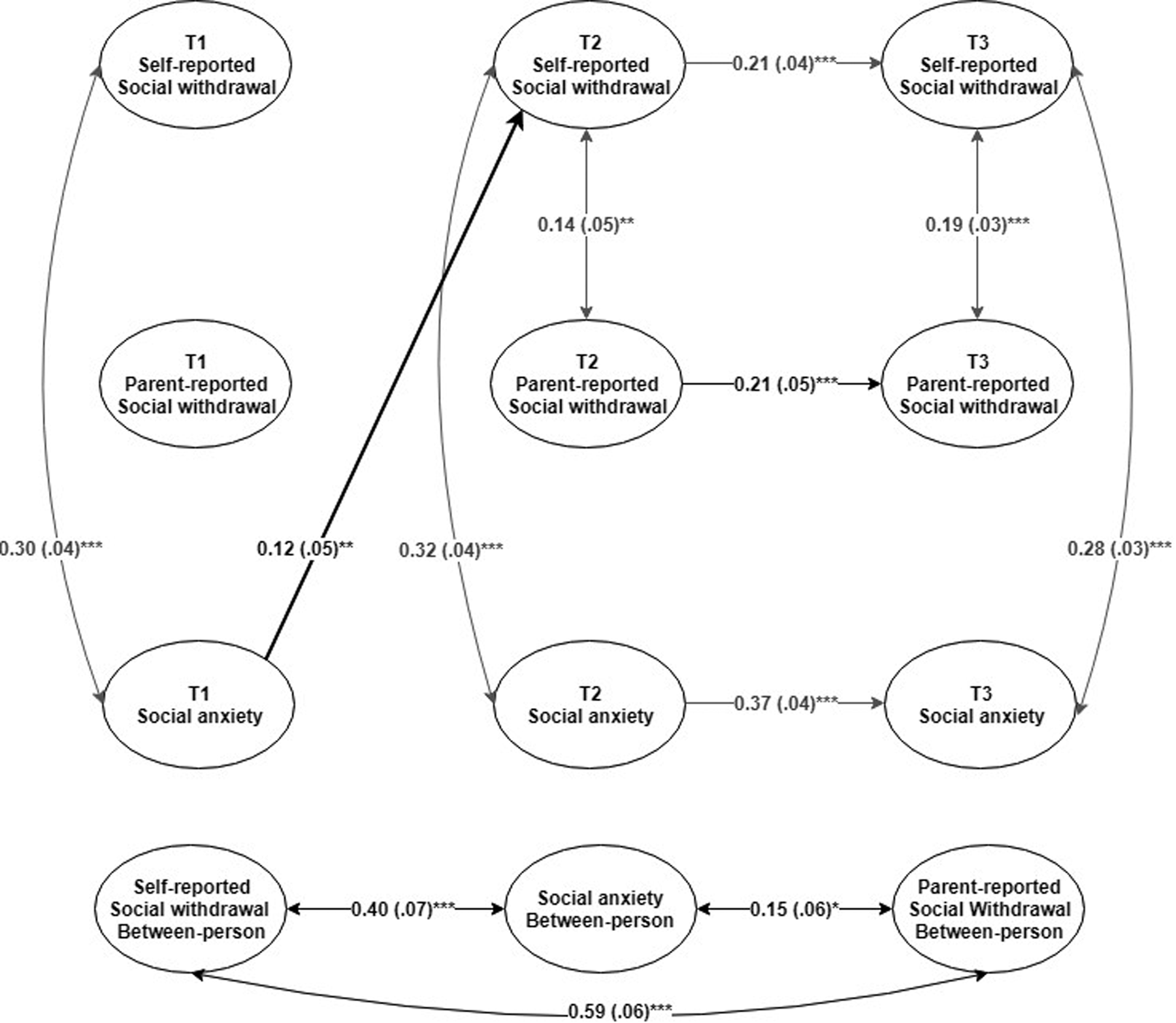
Figure 1. RI-CLPM 1 standardized estimates (standard errors) for self-reported social withdrawal, parent-reported social withdrawal, and social anxiety. Model depicts only paths >.10 that were significant. Paths <.10 are not interpreted except for when the path was >.10 and significant in other models, for consistency. *p < .05, **p < .01, ***p < .001.
RI-CLPM 2: Self-reported social withdrawal, social anxiety, and peer victimization
In RI-CLPM 2 (Figure 2) the relationship between self-reported social withdrawal, social anxiety, and peer victimization was investigated. The model had good fit to the data: χ2 (3) = 13.397 p = .004; RMSEA = .035, 90% CI [.018, .056]; SRMR = .011; CFI = .997. There were small to moderate stability paths for self-reported withdrawal and social anxiety from T2 to T3 and for peer victimization from T1 to T2. There were no significant within-person stability paths from T1 to T2 for self-reported withdrawal and social anxiety, and from T2 to T3 for peer victimization. Similar within-person, within-wave associations between self-reported withdrawal and social anxiety were found as in RI-CLPM 1. The within-wave associations were weak to moderate between self-reported withdrawal and peer victimization and between social anxiety and peer victimization. Within-person cross-lagged effects emerged from T1 social anxiety and victimization to T2 self-reported withdrawal, and from T2 self-reported withdrawal to T3 victimization.

Figure 2. RI-CLPM 2 standardized estimates (standard errors; left) for child-reported social withdrawal, victimization, and social anxiety; and RI-CLPM 3 standardized estimates (standard errors; right) for parent-reported social withdrawal, victimization, and social anxiety. Models are depicting only paths >.10 that were significant. Paths <.10 are not interpreted except for when the path was >.10 and significant in other models, for consistency. *p < .05, **p < .01, ***p < .001.
RI-CLPM 3: Parent-reported social withdrawal social anxiety, and peer victimization
In RI-CLPM 3 (Figure 2) we investigated the relationship between parent-reported social withdrawal and self-reported social anxiety and peer victimization. The model had good fit to the data: χ2 (3) = 29.727, p < .001; RMSEA = .057, 90% CI [.039, .076]; SRMR = .016; CFI = .993. There were small to moderate within-person stability paths for parent-reported withdrawal and victimization from T1 to T2 and for parent-reported withdrawal and social anxiety from T2 to T3. There were no significant stability paths for social anxiety from T1 to T2 or for victimization from T2 to T3. Like in RI-CLPM 1, there were no within-wave associations between parent-reported withdrawal and social anxiety. The within-wave associations between parent-reported withdrawal and peer victimization were weak and the within-wave associations between social anxiety and peer victimization were almost identical to those in RI-CLPM 2. Finally, within-person cross-lagged effects were consistently found from victimization to the next measurement wave of parent-reported withdrawal. This means that within-person increases in victimization consistently predicted an increase in parent-reported withdrawal at the consecutive measurement wave.
RI-CLPM 4: Self-reported social withdrawal, social anxiety, and perceived peer acceptance
In RI-CLPM 4 (Figure 3) the relationship between self-reported social withdrawal, social anxiety, and perceived peer acceptance was investigated. The model had excellent fit to the data: χ2 (3) = 3.658 p = .301; RMSEA = .009, 90% CI [.000, .034]; SRMR = .005; CFI = 1.00. There were no significant within-person stability paths from T1 to T2 for self-reported withdrawal or for social anxiety. The within-person stability path for peer acceptance from T1 to T2 was positive and small. The stability paths for self-reported withdrawal, social anxiety, and peer acceptance from T2 to T3 were small to moderate. The within-wave associations between self-reported withdrawal and social anxiety were almost identical to those in RI-CLPMs 1 and 2. The within-wave associations between self-reported withdrawal and peer acceptance were weak to moderate at T1 to T3 and there were no significant within-wave associations between social anxiety and peer acceptance. Consistent with RI-CLPM 2, within-person cross-lagged effects emerged from T1 social anxiety and peer acceptance to T2 self-reported withdrawal, and from T2 self-reported withdrawal to T3 peer acceptance.
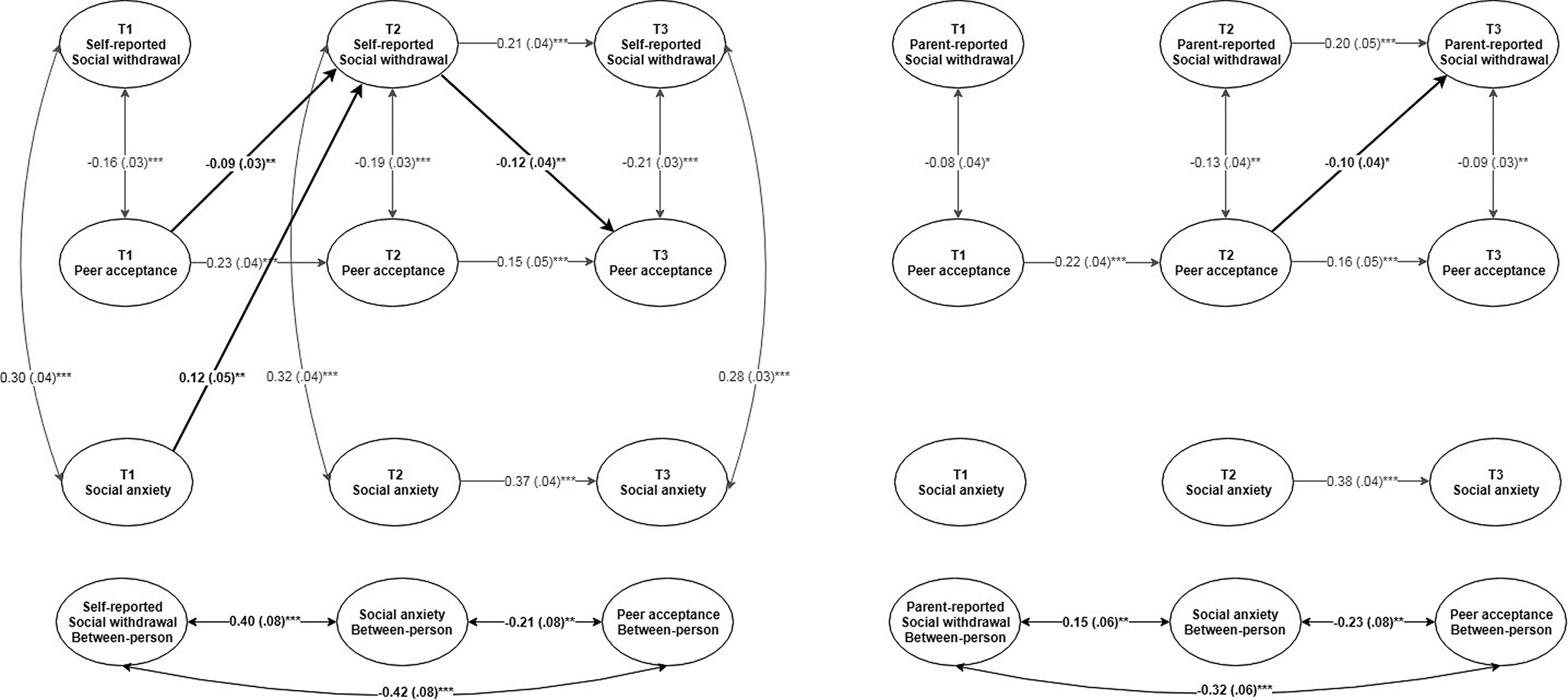
Figure 3. RI-CLPM 4 standardized estimates (standard errors; left) for child-reported social withdrawal, peer acceptance, and social anxiety; and RI-CLPM 5 standardized estimates (standard errors; right) for parent-reported social withdrawal, peer acceptance, and social anxiety. Models are depicting only paths >.10 that were significant. Paths <.10 are not interpreted except for when the path was >.10 and significant in other models, for consistency. *p < .05, **p < .01, ***p < .001.
RI-CLPM 5: Parent-reported social withdrawal, social anxiety, and perceived peer acceptance
In RI-CLPM 5 (Figure 3) we investigated the relationship between parent-reported social withdrawal and self-reported social anxiety and perceived peer acceptance. The model had excellent fit to the data: χ2 (3) = 6.896 p = .075; RMSEA = .022, 90% CI [.000, .043]; SRMR = .008; CFI = .999. There were no significant within-person stability paths for parent-reported withdrawal or social anxiety from T1 to T2. The stability path for peer acceptance from T1 to T2 was small and the stability paths for parent-reported withdrawal, social anxiety, and peer acceptance from T2 to T3 were small to moderate. There were no significant within-wave associations between parent-reported withdrawal and social anxiety nor between peer acceptance and social anxiety at any time point. The within-wave associations between parent-reported withdrawal and peer acceptance were weak and negative at every time point. One cross-lagged effect emerged: a within-person increase in peer acceptance at T2 predicted a decrease in parent-reported withdrawal at T3.
Sensitivity checks
Girls vs. Boys
There were no strong differences between girls and boys in any RI-CLPM (Table 3). For RI-CLPMs 2, 3, and 5, constraining all parameters to be equal between girls and boys fit the data as well as the freely estimated model, indicating no differences between girls and boys in the pathways between the variables in these models whatsoever. For RI-CLPMs 1 and 4, the constrained model fit the data significantly worse than the freely estimated model. The modification indices suggested that freeing the within-wave association between self-reported withdrawal and social anxiety at T3 would improve model fit. Allowing this parameter to vary between girls and boys resulted in a model fit no worse than the freely estimated model. Results indicated that for both RI-CLPMs this association was .33 for girls and .21 for boys (ps < .001), a negligible difference.
Table 3. Sensitivity results from the model fit comparisons of RI-CLPMs 1–5 between girls and boys

Note: SWs, self-reported social withdrawal. SWp, parent-reported social withdrawal. SA, social anxiety. V, peer victimization. P, peer acceptance. SB, Satorra–Bentler scaled. CFI, comparative fit index. RMSEA, root mean square error of approximation. SRMR, standardized root mean residual. AIC, Akaike information criterion. BIC, Bayesian information criterion.
Discussion
The present study used three waves of longitudinal data from a population-based and a clinically referred cohort to investigate the bidirectional, within-person associations between social withdrawal and social anxiety in adolescence, and the role of peer victimization and perceived peer acceptance in the pathways. Four main findings will be discussed. First, contrary to suggestions from previous research, there was no feedback loop between social withdrawal and social anxiety. Only social anxiety at 11 years predicted self-reported social withdrawal at 13 years. Second, results indicated that there was discontinuity of social withdrawal and social anxiety between 11 and 13 years, when adolescents transitioned to secondary education. Third, peer experiences played a central role in predicting levels of both self- and parent-reported social withdrawal. Fourth, there were notable differences between self- and parent-reported social withdrawal that likely relate to differing interpretations by informants of adolescents’ withdrawn behaviors.
Before discussing these within-person findings, we briefly mention the between-person results. At the between-person level, adolescents who perceived themselves as withdrawn across the three waves had greater parent-reported social withdrawal, social anxiety, and peer victimization, and lower peer acceptance than adolescents who rated themselves as less withdrawn. Likewise, adolescents who were more socially anxious across the three waves experienced more peer victimization and lower peer acceptance than adolescents with lower social anxiety. The positive, moderate between-person associations found between these variables are consistent with previous research (Biggs et al., Reference Biggs, Vernberg and Wu2012; Erath et al., Reference Erath, Flanagan and Bierman2007; Smith et al., Reference Smith, Barstead and Rubin2017), and indicate that social withdrawal and social anxiety are overlapping but distinct concepts that are both associated with problems with peers. The between-person associations between parent-reported withdrawal and self-reported peer experiences were comparable to those of self-reported withdrawal, but parent-reported withdrawal was only weakly associated with self-reported social anxiety. This might be due to diverging interpretations of adolescents’ withdrawn behaviors between adolescents and their parents, which will be discussed further on.
No evidence for a feedback loop between social withdrawal and social anxiety
The possibility of a feedback loop between social withdrawal and social anxiety has been suggested repeatedly (Kingerly et al., Reference Kingerly, Erdley, Marshall, Whitaker and Reuter2010; Richards & Hadwin, Reference Richards and Hadwin2011; Rubin, Bowker, & Gazelle, Reference Rubin, Bowker, Gazelle, Rubin and Coplan2010; Rubin & Burgess, Reference Rubin, Burgess, Vasey and Dadds2001; Rubin et al., Reference Rubin, Coplan and Bowker2009; Weeks, Ooi, & Coplan, Reference Weeks, Ooi and Coplan2016). Studies that empirically tested unidirectional parts of this loop (Biggs et al., Reference Biggs, Vernberg and Wu2012; Ding et al., Reference Ding, Coplan, Deng, Ooi, Li and Sang2018; Erath et al., Reference Erath, Flanagan and Bierman2007; Goodwin et al., Reference Goodwin, Fergusson and Horwood2004; Smith et al., Reference Smith, Barstead and Rubin2017) only examined associations at the between-person level, thereby neglecting that the feedback loop is inherently a within-person process. One main aim of the current study was to investigate if there are bidirectional, within-person associations between social withdrawal and social anxiety. Results indicated that there is no such reciprocal relationship during adolescence at the within-person level.
Social withdrawal did not predict future changes in social anxiety in any model. A path from social withdrawal to social anxiety is theorized to occur through social skill deficits, whereby socially withdrawn youth have fewer opportunities to practice social skills, making them socially ill equipped, and consequently experiencing negative self-appraisals in social situations that then exacerbate social fears. There is evidence that socially withdrawn youth have poorer social skills compared to nonwithdrawn youth (Kingerly et al., Reference Kingerly, Erdley, Marshall, Whitaker and Reuter2010), and the current study found that social withdrawal was associated with peer problems. Leading cognitive models of social anxiety suggest that poor social skills do not intrinsically cause social fears, but the negative peer experiences of youth with social skills deficits increase the risk for social anxiety (Rapee & Spence, Reference Rapee and Spence2004), likely via negative beliefs about the self that are more central to the development of social anxiety (Epkins & Heckler, Reference Epkins and Heckler2011; Findlay, Coplan, & Bowker, Reference Findlay, Coplan and Bowker2009; Kingsbury, Coplan, & Rose-Krasnor, Reference Kingsbury, Coplan and Rose-Krasnor2013; Rapee & Heimberg, Reference Rapee and Heimberg1997). The fact that we did not find that social withdrawal predicted social anxiety, despite associations with peer problems, might be related to the heterogeneous nature of withdrawal. Multiple motivations may underlie withdrawn behaviors, and not all withdrawn youth have negative social–cognitive biases (Markovic, Rose-Krasnor, & Coplan, Reference Markovic, Rose-Krasnor and Coplan2013). Furthermore, social–cognitive biases are mitigated when socially withdrawn youth have a close mutual friendship (Burgess et al., Reference Burgess, Wojslawowicz, Rubin, Rose-Krasnor and Booth-LaForce2006) or when they are able to utilize problem-solving coping (Kingsbury et al., Reference Kingsbury, Coplan and Rose-Krasnor2013). No study to date has investigated if different aspects of withdrawal have differing associations with self-appraisals. Possibly, certain aspects of withdrawal, such as social aversion, are more predictive of future increases in social anxiety than others, such as social disinterest. Using a heterogeneous conceptualization may occlude associations from social withdrawal to social anxiety, especially if certain withdrawal aspects are not associated with negative self-appraisals.
The reverse cross-lagged association, from social anxiety to social withdrawal, was found only for self-reported withdrawal. A within-person increase in social anxiety at 11 years predicted a within-person increase in self-reported withdrawal at 13 years. This cross-lagged path supports the theorized avoidance mechanism: socially anxious youth avoid peers in order to manage or decrease their fears, and over time, the decrease in anxiety during periods of withdrawal reinforces future withdrawal behaviors (Rubin et al., Reference Rubin, Coplan and Bowker2009). Although not tested in the current study, there is ample evidence that socially anxious youth use avoidance coping to manage their social fears (Hofmann, Reference Hofmann2007; Spence & Rapee, Reference Spence and Rapee2016). The avoidance mechanism has been discussed as a potential mediator between social anxiety and social withdrawal in three previous studies that investigated between-person associations from social anxiety to social withdrawal (Biggs et al., Reference Biggs, Vernberg and Wu2012; Ding et al., Reference Ding, Coplan, Deng, Ooi, Li and Sang2018; Erath et al., Reference Erath, Flanagan and Bierman2007), but no study to date has directly investigated avoidance as the within-person mechanism linking social anxiety to withdrawal. Of note, we did not find a cross-lagged path from social anxiety at 13 years to self-reported social withdrawal at 16 years. If avoidance is the underlying mechanisms linking social anxiety to future social withdrawal, we would expect to see a cross-lagged association also during later adolescence because the use of avoidance increases throughout adolescence (Seiffge-Krenke, Reference Seiffge-Krenke2000; Sumter, Bokhorst, & Westenberg, Reference Sumter, Bokhorst and Westenberg2009; Valiente, Eisenberg, Fabes, Spinrad, & Sulik, Reference Valiente, Eisenberg, Fabes, Spinrad and Sulik2015) and tends to generalize to multiple social situations (Rao et al., Reference Rao, Beidel, Turner, Ammerman, Crosby and Sallee2007). The presence of a cross-lagged path from 11 to 13 years, with the subsequent lack of a cross-lagged path in older ages, may be related to the transition to secondary education, occurring between 11 and 13 years in the Netherlands. It is plausible that the transition to secondary education is especially distressing to socially anxious youth, who may have already had a smaller peer group in primary school. In the transition to secondary school, socially anxious adolescents may become more socially withdrawn due to the smaller peer network they bring with them to their new environments (Biggs et al., Reference Biggs, Vernberg and Wu2012). Furthermore, if this peer network, albeit small, previously helped socially anxious youth to approach new peers, anxious youth may be unable to consolidate new relationships without support from their peer network, thus becoming more socially withdrawn in the school transition. This delayed effect may be reflected in the cross-lagged path from social anxiety at 11 years to social withdrawal at 13 years, during the secondary education transition. Posttransition, as socially anxious adolescents become habituated to their new social environment, they may experience more opportunities for social interactions with new adolescents, reducing associations from social anxiety levels to subsequent social withdrawal.
Discontinuity of social withdrawal and social anxiety during the transition to secondary education
We found additional evidence for the effects of the transition to secondary education on social withdrawal and social anxiety in the absence of within-person stability paths from 11 to 13 years. Specifically, deviations from an adolescent's expected self-reported social withdrawal, parent-reported social withdrawal, and social anxiety levels at 11 years did not predict their expected levels of these respective variables at 13 years. This indicates that social withdrawal and social anxiety are discontinuous during the transition to secondary education, but become moderately stable after 13 years, when youth have habituated to their new social environments. School transitions are turning points for better or for worse psychological outcomes because they are both stressors and opportunities (Nelemans, Hale, Branje, Meeus, & Rudolph, Reference Nelemans, Hale, Branje, Meeus and Rudolph2018; Schulenberg, Sameroff, & Cicchetti, Reference Schulenberg, Sameroff and Cicchetti2004). On the one hand, the transition to secondary school may be especially distressing for adolescents who are withdrawn or socially anxious because the novel social environment requires them to form new social relations and groups by meeting unfamiliar peers. Withdrawn or socially anxious adolescents may struggle to overcome these social challenges. On the other hand, unfamiliar peers in secondary school are unaware of withdrawn or anxious youth's reputations from primary school, and may therefore approach them more often to initiate relationships and treat them more positively (Schulenberg et al., Reference Schulenberg, Sameroff and Cicchetti2004). This, along with solitude becoming less socially stigmatizing into adolescence (Freeman, Csikszentmihalyi, & Larson, Reference Freeman, Csikszentmihalyi and Larson1986; Goossens & Marcoen, Reference Goossens, Marcoen, Rotenberg and Hymel1999; Larson, Reference Larson1997) and becoming increasingly adaptive in late adolescence and early adulthood (for a detailed review, see Coplan, Ooi, & Baldwin, Reference Coplan, Ooi and Baldwin2019), may give socially withdrawn or socially anxious youth a “fresh start” in their new schools. The dual nature of the social consequences of the transition to secondary education suggests that the discontinuity in social withdrawal and social anxiety during this transition occurs because some socially withdrawn or socially anxious youth cope well, while others encounter more challenges in adapting to their new social environments. As discussed previously, adolescents who increased in social anxiety during the transition became more socially withdrawn, indicating that these youth experienced the greatest challenges in adapting to their new social environments during the school transition. Likewise, increases in peer victimization and decreases in perceived peer acceptance also predicted increasing levels of self-reported social withdrawal during the transition to secondary education, pointing to the centrality of peer experiences in adolescents’ withdrawal levels, especially during the stressful transitional period.
The roles of peer experiences
Peer experiences emerged as central factors influencing social withdrawal in adolescence. Peer victimization and perceived peer acceptance predicted both self- and parent-reported social withdrawal levels and were predicted by self-reported withdrawal. Results indicated an interesting feedback loop between social withdrawal and peer victimization and peer acceptance. When adolescents increased in peer victimization at 11 years, they rated themselves as more withdrawn at 13 years. In turn, increasing withdrawal predicted greater victimization at 16 years. This finding is consistent with the hypothesis that victimized youth withdraw from peers to cope with or attempt to decrease victimization, and when youth become more withdrawn, they are more likely to be victimized because they are seen as “easy targets” that exhibit nonnormative behaviors (Gazelle & Rudolph, Reference Gazelle and Rudolph2004). The level of peer victimization became less linked to adolescents’ withdrawal levels over time (i.e., within-wave associations between these variables became weaker), probably due to an overall decrease in victimization throughout adolescence (Pellegrini & Long, Reference Pellegrini and Long2002; Shell, Gazelle, & Faldowski, Reference Shell, Gazelle and Faldowski2014; Williford, Brisson, Bender, Jenson, & Forrest-Bank, Reference Williford, Brisson, Bender, Jenson and Forrest-Bank2011). Similarly, perceiving to becoming more accepted by peers at 11 years predicted lower self-reported withdrawal at 13 years, and in turn, decreasing withdrawal at 13 years predicted increases in peer acceptance at 16 years. When peer acceptance is high, youth may increase their motivation to interact with their peers, thereby decreasing withdrawal behaviors, and decreasing withdrawal leads to more acceptance by peers (Gazelle & Rudolph, Reference Gazelle and Rudolph2004). Peer acceptance became more intertwined with self-reported social withdrawal across these ages, highlighting the increased influence of feeling accepted by the peer group on adolescents’ well-being (Brown & Larson, Reference Brown, Larson, Lerner and Steinberg2009; La Greca & Harrison, Reference La Greca and Harrison2005; Sentse, Lindenberg, Omvlee, Ormel, & Veenstra, Reference Sentse, Lindenberg, Omvlee, Ormel and Veenstra2010).
Similar to the self-reported social withdrawal models, parent-reported social withdrawal was consistently predicted by peer victimization and perceived peer acceptance. This provides consistent evidence that youth who have increasingly problematic peer experiences are especially at risk for becoming more socially withdrawn, and rated as withdrawn by both self-reports and parent reports. Yet, there were differences between the two withdrawal informants and peer experiences. Unlike self-reported withdrawal, parent-reported withdrawal at 13 years did not predict changes in peer experiences at 16 years; in addition, unlike parent-reported withdrawal, self-reported withdrawal at 16 years was not predicted by peer experiences at 13 years.
Differences between self- and parent-reported social withdrawal
Differences between informants of social withdrawal have been investigated by Rubin, Althoff, Walkup, and Hudziak (Reference Rubin, Althoff, Walkup and Hudziak2013), who found that parents, teachers, and youth (aged 6 to 18 years) each had unique interpretations of youth's socially withdrawn behaviors. In the current study, notable differences emerged between models with self-reported social withdrawal and models with parent-reported social withdrawal. These differences may be caused by divergent interpretations and attributions of adolescents’ withdrawn behaviors. We found a discrepancy between self- and parent-reported social withdrawal, which prevented the creation of a combined multi-informant social withdrawal score. Perhaps adolescents place more weight on the emotional and motivational aspects of withdrawal than their parents because they have introspective knowledge about their apprehension in social situations that their parents do not have direct access to. We found strong within-wave associations between self-reported withdrawal and social anxiety, and social anxiety predicted future levels of self-reported withdrawal, whereas the association did not reach significance in the parent-reported withdrawal models. One might argue that this difference is caused by shared method variance (social anxiety was based on self-reports), but that is unlikely to be the sole reason because self-reported peer experiences did consistently predict changes in parent-reported social withdrawal. Possibly, parents observe the same withdrawn behaviors that adolescents report, but only attribute these behaviors to their adolescent's past or present peer problems rather than to the adolescent's underlying feelings of social anxiety. More specifically, parents have extensive knowledge of their child's developmental history (Spangler & Gazelle, Reference Spangler and Gazelle2009) and may perceive socially reticent behaviors as normative for the child (Rubin et al., Reference Rubin, Althoff, Walkup and Hudziak2013). Increases in social withdrawal may therefore be salient for parents only when parents know that their child experiences or has experienced a hostile peer environment. Discussing who is a better informant of social withdrawal during adolescence is out of the scope of the current paper, and we recommend the use of multi-informant approaches to fill the gaps in knowledge between informants and to obtain a more comprehensive assessment of social withdrawal during these ages.
Strengths, limitations, and directions for future research
A main strength of this study is its prospective longitudinal design with data from two cohorts, together comprising a sample size large enough to detect small within-person effects. Furthermore, using RI-CLPMs allowed us to disentangle within- from between-person effects when investigating the bidirectional associations between social withdrawal, social anxiety, and peer experiences, which was not done in previous studies. We investigated both negative (victimization) and positive (acceptance) peer experiences, thereby providing a more comprehensive account of adolescents’ peer experiences than studies investigating only relational problems. Taking a multi-informant approach by including both self-reported and parent-reported social withdrawal provided a broader account of adolescents’ withdrawn behaviors across different environments and allowed for an exploration of differences in pathways by informant of withdrawal. Finally, the a priori power analysis and longitudinal measurement invariance tests provide evidence for the robustness of our results.
Several limitations should be noted when interpreting the findings of this study. First, we used a global conceptualization of social withdrawal, and underlying motivations to withdrawal were not accounted for. It is possible that some aspects of social withdrawal are more strongly or differentially linked to social anxiety than others. It is also possible that only specific aspects of withdrawal predict increases in social anxiety, and that these associations are occluded by other, nonpredictive aspects of social withdrawal. Tying to this point, the reliability of the self-reported social withdrawal items was quite low. However, other indices of reliability (i.e., GLB) were higher, and through longitudinal measurement invariance testing, we found that adolescents interpreted the withdrawal items in a similar way across the three measurement waves. Furthermore, despite the low reliability of items, we found significant effects >.10, which may be lower than the true effects because low reliability reduces effect sizes rather than inflates them (Furr & Bacharach, Reference Furr, Bacharach, Furr and Bacharach2014). Future research could examine if different aspects of social withdrawal differ in their within-person associations with social anxiety.
Second, we used a two-item measure of peer victimization, which did not disaggregate between different types of victimization, such as physical and relational victimization. Although inconclusive (Crick et al., Reference Crick, Nelson, Morales, Cullerton-Sen, Casas, Hickman, Juvonen and Graham2001; Leadbeater, Boone, Sangster, & Mathieson, Reference Leadbeater, Boone, Sangster and Mathieson2006; Olweus & Breivik, Reference Olweus, Breivik, Ben-Arieh, Casas, Frønes and Korbin2014), research suggests that there may be gender differences between these two forms of victimization, with boys experiencing more physical victimization and girls more relational victimization (Cullerton-Sen & Crick, Reference Cullerton-Sen and Crick2005). It is possible that we did not find differences between girls and boys in the associations with peer victimization because of our nonspecific measure.
Third, peer victimization and peer acceptance are not comprehensive indicators of an adolescent's peer experiences. Other peer experiences, such as number and quality of friendships, involvement in romantic relationships, and extracurricular activities, influence social anxiety and social withdrawal as well, perhaps via different pathways. In addition, while our perceived peer acceptance measure focused on classmate peers, adolescents likely have contact with peers outside of the school setting. It would be worthwhile to use more comprehensive peer measures than we did in the present study.
Fourth and finally, the large majority of participants in the current study were from a Dutch background. This limits the generalizability of our findings because there may be ethnic differences in associations between social withdrawal and social anxiety, and in the role of peers in these pathways. Studies consistently report differences between individualistic and collectivistic cultures on the perceptions, associations, and outcomes of socially withdrawn behaviors. In Canadian youth, shyness–sensitivity, an aspect of social withdrawal, is associated with lower peer acceptance, lower self-perceptions of social competence, and higher levels of loneliness, peer rejection, and victimization. In contrast, shyness in Chinese or Canadian–Chinese youth is associated with greater peer acceptance and more positive responses from peers, and is not related to self-perceptions of social competence, loneliness, or victimization (Chen, DeSouza, Chen, & Wang, Reference Chen, DeSouza, Chen and Wang2006; Chen & French, Reference Chen and French2008; Chen et al., 2004a, 2004b; Chen, Rubin, & Sun, Reference Chen, Rubin and Sun1992; Chen & Tse, Reference Chen and Tse2008). It is important to note, however, that the perception and outcomes of shyness in Chinese youth are changing and becoming increasingly negative due to rapid economic and social changes in urban mainland China (Coplan, Liu, Cao, Chen, & Li, Reference Coplan, Liu, Cao, Chen and Li2017; Liu, Xiao, Coplan, Chen, & Li, Reference Liu, Xiao, Coplan, Chen and Li2018). Cross-cultural differences in other aspects of social withdrawal have not been investigated extensively, but recent research suggests that both Canadian and Chinese peers perceive unsociable-withdrawn youth less positively compared to shy or sociable youth (Coplan, Zheng, Weeks, & Chen, Reference Coplan, Zheng, Weeks and Chen2012). Furthermore, the influence of school transitions on social withdrawal and social anxiety may differ from those in the current study, depending on the educational structure in a specific country or region. The Netherlands has one school transition during adolescence, while many regions in the United States and in other countries have a second transition occurring between primary and secondary school. A greater number of transitions during adolescence could alter the pathways via more discontinuities in social withdrawal or social anxiety. Replications of the current study with more heterogeneous samples, different ethnic groups, or various educational systems is warranted.
Conclusion
This was the first study to investigate within-person associations in the theorized social withdrawal–social anxiety feedback loop, and to highlight the importance of peer experiences in the pathways. Results indicated that there was no feedback loop between social withdrawal and social anxiety during adolescence. Adolescents who increased in social anxiety and peer problems during the transition to secondary education were especially at risk for greater social withdrawal posttransition. In turn, adolescents who became more socially withdrawn posttransition had greater peer problems 3 years later. Parent-reported social withdrawal was consistently predicted by adolescents’ peer problems, and was not significantly associated with social anxiety, within person. These results provide insight to the longitudinal, within-person associations, sequential timing, and underlying mechanisms linking social withdrawal, social anxiety, and peer experiences during adolescence.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/S0954579419001354
Financial Support
This research is part of the TRacking Adolescents' Individual Lives Survey (TRAILS). Participating centers of TRAILS include various departments of the University Medical Center and University of Groningen, the University of Utrecht, the Radboud Medical Center Nijmegen, and the Parnassia Bavo group, all in the Netherlands. TRAILS has been financially supported by various grants from the Netherlands Organization for Scientific Research (NWO), ZonMW, GB-MaGW, the Dutch Ministry of Justice, the European Science Foundation, the European Research Council, BBMRI-NL, and the participating universities.
Acknowledgments
We are grateful to everyone who participated in this research or worked on this project to make it possible.









 Open access
Open access