



This article deals with an illuminating case of unintended consequences — how the misapplication of scientific knowledge against one disease, in the economically and politically peripheral hinterlands of a British colony in West Africa, unwittingly contributed to a subsequent and severe epidemic of another disease affecting the colony's African subjects. The place was the British Gold Coast, where an outbreak of sleeping sickness (human African trypanosomiasis) caused extensive mortality in communities across the northern savannah from the late 1920s. The northern protectorate of the Gold Coast was developed and subsequently neglected as a migrant labour reserve by colonial planners from the early 1900s, and the North's sleeping sickness epidemic received almost no official recognition until the 1930s, when it began to affect the southwards supply of labour for the Gold Coast's mines and cocoa farms. Facing the prospect of diminished revenues, at this point the colonial administration invested heavily in short-term control measures against the outbreak itself (using quarantine camps and drug treatments) and in a more expansive control programme against the disease's insect vector, the tsetse fly.
This vector control programme was run by the Gold Coast Anti-Tsetse Department. It operated for almost two decades, with generous funding and little supervision either from the central government and Medical Department at Accra or from local health officials in the North. The programme's particular methods for tsetse control, and for subsequent resettlement of African communities, were based almost entirely on the theories of one entomologist, Kenneth Morris, who oversaw the North's vast anti-tsetse campaign from its inauguration until shortly before Ghana's independence in 1957. But Morris's ideas and methods were blind to another serious parasitic disease, onchocerciasis (also known as ‘river blindness’), which was present in the same area and among the same communities where his anti-tsetse campaign operated.
In the historiography of the colonial Gold Coast (and to a lesser extent of independent Ghana), both sleeping sickness and onchocerciasis have been the focus of earlier research. This paper extends and critiques earlier work by charting links between the two diseases: between the northern Gold Coast's tsetse control programme — often represented in the existing literature as a success for colonial science — and a serious epidemic of onchocerciasis which was only recognised shortly before independence. In 1953, a survey of blindness in West Africa revealed that communities in the northern Gold Coast suffered the highest known incidence of onchocerciasis-related blindness in Africa. In fundraising literature and international reportage, the region became known as Africa's ‘Country of the Blind’.Footnote 1
It now seems likely that at least part of this exceptional incidence of onchocerciasis was the result of earlier actions taken by the anti-tsetse campaign. The relationship between colonial tsetse control and independence-era onchocerciasis reveals much about public health work on the margins of the state, about the striking degree of agency vested in individuals operating with little oversight during and after the Second World War, and about the misapplication of colonial-era science, which was subordinated to the broader economic and political concerns of the Gold Coast government.
The North
There is a relatively well-developed literature on the peripheral relationship of the Gold Coast's northern region, also known as the Northern Territories Protectorate, to the southern Gold Coast's centres of political and economic power. In the first five years after the region's incorporation into the British Gold Coast in 1903, the administration made efforts to promote export agriculture, notably cotton production, and to locate the kind of mineral reserves that had helped make the southern colony one of Britain's most profitable possessions in colonial Africa.Footnote 2 When these initiatives failed, the government at Accra instead developed the North as a migrant labour reserve (see Fig. 1). From 1908 increasing numbers of northerners, making up a large proportion of the region's agricultural workforce, were recruited or compelled to journey for work on gold mines in the southwest of the colony and the central forest belt, and on cocoa plantations across the South. By 1920 an enduring pattern had been established. Although a succession of concerned northern officials disagreed, the central government saw the North as a zone of ‘negligible’ economic importance, placing ‘a burden on the Gold Coast for which it makes no adequate return’.Footnote 3 It nevertheless constituted ‘the chief source of labour supply in the south’ and provided the majority of men enlisted into Britain's Gold Coast Regiment. In part because the region itself generated little revenue for the colonial government, and perhaps, as some have argued, to amplify the ‘push’ factor for labour migration, the Northern Territories remained markedly less developed than the South over the colonial period, and their administration was disproportionately underfunded relative to its population. Formal education in the North was deliberately restricted to basic levels — most Christian missions were prevented from establishing outposts or offering schooling and health services in the region until the mid-1930s — and there were severe shortfalls in public water supply, including in the regional capital at Tamale, which continued even as piped water and treatment plants were expanded further south.Footnote 4
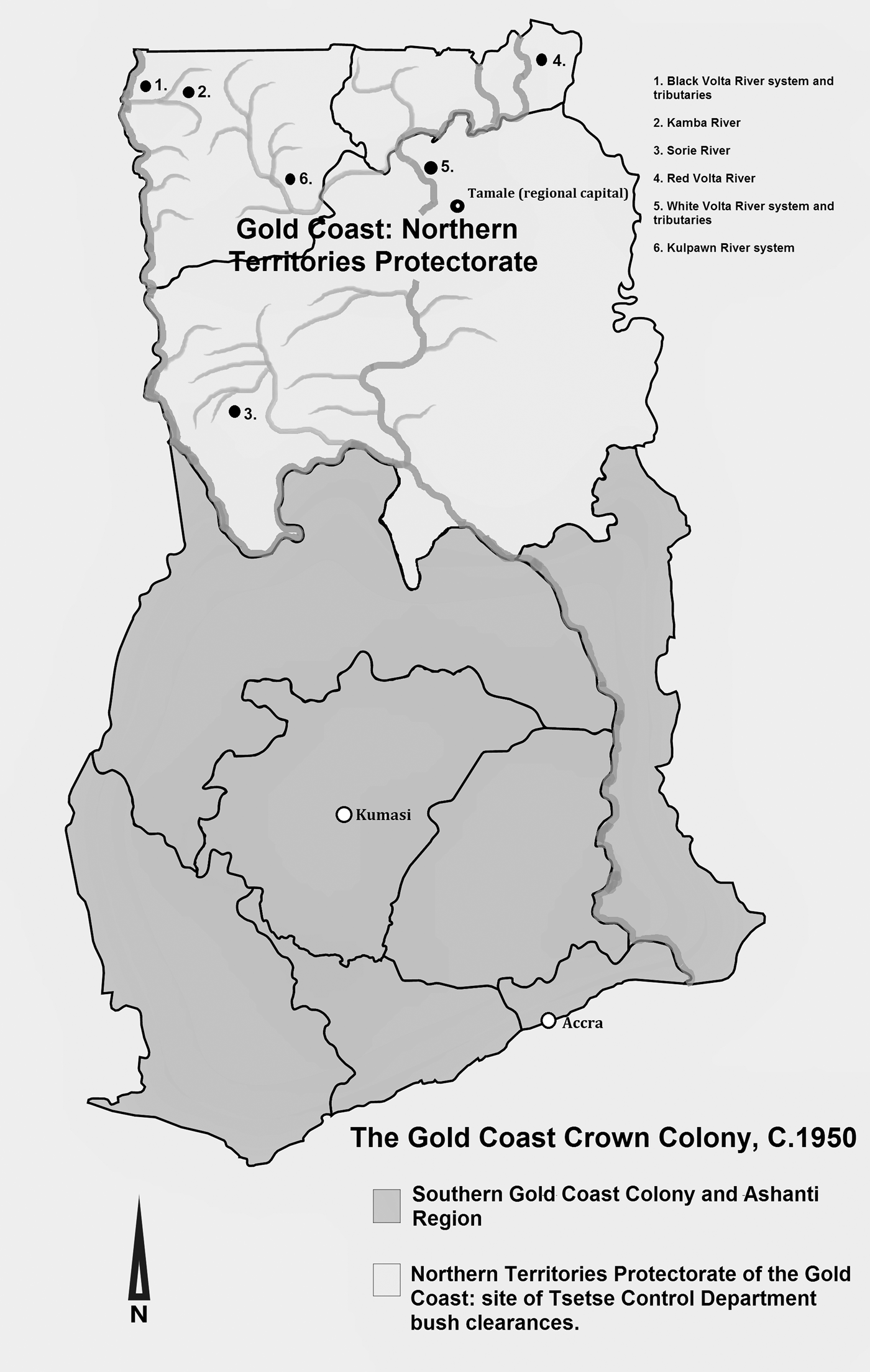
Fig. 1. Map of the Gold Coast showing northern river systems.
Southwards labour migration and relative northern underdevelopment continued until the end of the colonial period and have persisted into the present in independent Ghana. Beneath these longstanding patterns of economic distribution and political access, there are other reasons to consider the North as distinctive whole. As a dry tropical savannah separated from the coast by the West African forest belt, the region's weather patterns, terrain, and agricultural potentials were (and are) substantially different from the rest of the country. Crucially, unlike the South, the North was not a zone where cocoa, the crop most valued and consistently supported by different colonial and postcolonial governments, was produced. Partly as a result of its different climate and ecology, the North was host to diseases that had less impact in the forest belt or at the coast: notably sleeping sickness but also epidemic cerebrospinal meningitis, a disease which only reaches epidemic proportions in the dry savannah or Sahelian climates of the ‘African meningitis belt’ and does not extend into southern Ghana. Ethnic, linguistic, and cultural differences further sustain the idea of a discrete North and South. The North saw intense slaving activity during the years of the Atlantic slave trade, when slaving raids were conducted by the southern Asante Confederacy, and after abolition, when the region was raided by Samori Toure and the Zabarima militias of Babatu Zatu.Footnote 5 Jean Allman and John Parker note that the blanket terms Gurunsi and nnonkofoo (suggesting ‘an identity outside of jural corporateness and indeed on the fringe of perceptions of humanity’) were applied by the southern Akan states of the nineteenth century to many decentralised societies in the Northern Territories, and that these states similarly saw the region as a slaving reserve.Footnote 6 Over the course of the twentieth century, Islam spread more extensively in the North than any other region of Ghana, becoming the predominant religion across the North as a whole (at 42 per cent of the region's total population in 2010).Footnote 7 The South became increasingly Christianised over the same period, and in 2010 approximately 90 per cent of the southern population was Christian. The evolving religious difference between North and South overlay an older ethnolinguistic division. In the South, most people speak languages of what has been called the Kwa family of the Niger-Congo group — Ga, Ewe, and the mutually intelligible Akan languages of Fante and Twi — while most northern communities speak languages of the Niger-Congo Gur family.Footnote 8
The region's colonial political economy constitutes a foundational basis for this article's discussion of a discrete ‘North’ and ‘South’, despite the extensive internal variety of both regions. Here I use ‘the North’ both as a useful shorthand metonym for the whole region and its inhabitants (whom I sometimes refer to as ‘northerners’) and as a marker of comparison with ‘the South’. The marginalised history of the North as a colonial subregion — developed as a migrant labour reserve with little influence in Accra, and persistently underfunded in terms of health and education — underpinned a more specific ignorance of African health knowledge and local disease burdens, which characterised the approach of the anti-tsetse campaign and contributed to an epidemic of blindness.
Diseases, literature and sources
At this relatively developed stage in the historiography of disease in Africa, there is perhaps less need to introduce the two diseases which feature in this article, although more has been written on sleeping sickness than onchocerciasis. It may be inconsistent, but here I use the common name for one disease, sleeping sickness, while keeping the scientific name for the other, onchocerciasis. This is because onchocerciasis is still widely known by northern Ghanaians as ‘oncho’, a result of publicity surrounding the 1974–2002 Onchocerciasis Control Programme in West Africa managed by the World Health Organization (WHO). The disease's more common name in Europe and the United States, ‘river blindness’, was promoted by a charitable organisation working in the North in the 1950s to facilitate fundraising and advocacy work in Britain.
Often called human African trypanosomiasis to distinguish it from other human and non-human forms of the disease, sleeping sickness is caused by a class of parasites that can attack both humans and animals, causing the disease called ‘nagana’ in both wild and domesticated ungulates. The causative agents are microscopic protozoan organisms called trypanosomes, spread by the bite of blood-sucking flies in the genus Glossina, commonly known as the ‘tsetse’ flies. Here it is worth noting that both ‘riverine’ (Glossina palpalis) and ‘savannah’ (Glossina morsitans) species of tsetse are found in northern Ghana, meaning that sleeping sickness could be spread away from rivers or lakes. Both the flies and trypanosomes are distributed in an east-west band across sub-Saharan Africa, from the fourteenth parallel (southern Niger) to the twentieth parallel (northern Namibia).Footnote 9 The two trypanosome species that cause disease in humans are Trypanosoma brucei rhodesiense, found in East and Southern Africa and which causes an acute form of the disease that kills within weeks, and Trypanosoma brucei gambiense, which causes the chronic form that affects people in West and Central Africa, taking an average of three years between infection and death without treatment.Footnote 10
The common English term for animal trypanosomiasis, nagana, is taken from the Zulu ngana (weak or useless), indicating the symptoms it produced in livestock. Infected animals become progressively anaemic and lethargic, followed by death in some species, and cannot be used for ploughing or transport — there were economic imperatives to control the disease in both people and animals.Footnote 11 In humans, the trypanosome enters the circulatory system after infection from a tsetse bite, and the haemolymphatic stage of the disease begins, causing fever, headache, severe itching, and visible swelling of the lymph glands. At the second, neurological stage of the disease, the organism crosses the blood-brain barrier and begins to destroy the nervous system. The progression of symptoms varies, but often includes tremors, limb paralysis, speech disorders, excessive salivation, psychotic episodes, and periods of aggression or intense apathy and inactivity. A principal symptom of the disease is its disruption of the circadian sleep/wake rhythm, meaning that sufferers fall asleep uncontrollably at irregular intervals. Untreated trypanosomiasis invariably progresses to coma and death.Footnote 12
Like sleeping sickness, onchocerciasis is also spread by a biting fly, the river-breeding blackflies of the genus Simulium. The flies transmit the larvae of a parasitic filarial worm, Onchocerca volvulus, which uses humans as its exclusive host. Once inside a host, the larvae migrate through the tissues and develop into adult worms, creating hard nodules in the skin where they mate and begin the human-fly stage of the reproductive cycle. Each day during their 10-to-15-year lifespan, adult female worms release into the body 750 to 1,000 ‘microfilaria’ — microscopic larval worms that pervade the outer tissues, skin, and eyes of the person, awaiting collection by a biting blackfly. The microfilaria may not cause noticeable discomfort during their 6-to-24-month lifespan, but complications begin when they start to die in the tissues, causing an immune response which leads to intense itching and disfiguration of the skin and scar formation in the eyes that causes blindness over the course of several years.Footnote 13 The history of sleeping sickness in the British Gold Coast has been studied by David Patterson, Jeff Grischow and David Scott, among others.Footnote 14 Patterson also examined the slow accumulation of medical knowledge around onchocerciasis from 1900 to 1950, noting how evidence of the disease was repeatedly overlooked by Gold Coast medical officers before the 1940s. Like Grischow, who was focused specifically on sleeping sickness, Patterson did not examine the linkages between the two diseases, although both observed that sleeping sickness and onchocerciasis were prevalent in the same areas.Footnote 15 This paper builds on Patterson's study of northern onchocerciasis before 1950, using sources which were unavailable at the time of his research, and makes close reference to Grischow's work while charting new links between the two diseases.Footnote 16 The article also contributes to a growing body of literature on the historical misapplication or disregard of scientific knowledge in Africa. In their studies of water systems and the experience of lakeside communities in Ghana, Emmanuelle Kwesi Akyeampong and Dzodzi Tsikata have discussed the explosive increase in schistosomiasis (bilharzia) infections that accompanied the construction of the Akosombo Dam and impoundment of Lake Volta in the 1960s, a project which began with the foreknowledge that construction would have this effect.Footnote 17 This is an area of ongoing research, for construction of the dam also had the effect of reducing onchocerciasis infection in some areas because the Simulium blackfly that spreads the disease requires flowing water to reproduce.Footnote 18 Beyond the Gold Coast and Ghana, Guillaume Lachenal's book The Lomidine Files developed a subtle and detailed reflection on the drug Lomidine, an extensively-promoted sleeping sickness drug which was used preventively on large numbers of people in Cameroon and other French colonies in Africa. This was despite evidence that the drug was both ineffective in preventing sleeping sickness and carried the risk of serious or fatal side effects — an example of what Lachenal calls bêtise, the overconfident ‘unreason’ of some colonial medical science in the face of countervailing evidence.Footnote 19
All of these works raise questions about the intentionality (or wilful blindness) of scientific, civil engineering, and other technical interventions that reshaped the lives of people across Africa, in which actions towards an enduring or ephemeral ‘good’ had unintended, disregarded, or sometimes entirely foreseen negative consequences for disease and public health. The following account discusses the consequential relationship between sleeping sickness, tsetse control, and onchocerciasis in the colonial North.Footnote 20
Epidemic sleeping sickness in the northern Gold Coast
Patterson and Scott have argued that sleeping sickness did not assume epidemic proportions or present a major public health problem in the Gold Coast before the 1930s, but there are many indications that by this time the disease was significantly more widespread in the North than has previously been recognised.Footnote 21 Certainly by the late 1920s, sleeping sickness appears to have reached epidemic proportions in the Northern Territories and neighbouring French Upper Volta, even though the outbreak went officially unrecognised until 1935. In 1924 a medical officer toured the Lawra District in the northwest, on the request of a district commissioner concerned about high numbers of infected people who were brought to the district station in an attempt to find medical assistance, at a time when very few people made the journey to colonial healthcare facilities. His survey covered 27 villages, and 3,654 people were examined by the relatively crude method of checking for ‘Winterbottom's Sign’ — the visible enlargement of the cervical glands at the back of the neck, a symptom of the early-stage disease. The medical officer found that almost 8 per cent of the population appeared to be infected with sleeping sickness, with the most intense prevalence of symptoms in 16 villages located within three miles of the Black Volta and Kamba Rivers. Here the infection rate was approximately 14 per cent, with more than one in eight people potentially affected.Footnote 22 These early findings were important not only because they indicated the increasingly epidemic scale of the disease, when this was largely unrecognised in Accra, but also because this was the first report which identified the Kamba valley and its surroundings as a zone of high human sleeping sickness prevalence. It would subsequently become a focal point for the anti-tsetse fly campaign, and then for epidemic onchocerciasis.
By 1928–9, the colony's Annual Medical Report argued defensively that
human trypanosomiasis has attracted more attention than in previous years, and a greater number of cases are recorded, but it would be entirely premature to conclude that it is on the increase. In all probability the correct explanation is that greater facilities have occurred for observing the disease.Footnote 23
At this time French medical authorities in colonial Upper Volta had already recognised the epidemic scale of sleeping sickness infection just across the border from the northern Gold Coast, and a British entomologist had been dispatched northwards to conduct an investigation into rapidly rising numbers of cases. Even so, the Gold Coast's annual report concluded that ‘it was the opinion of the Medical Department that as human sleeping sickness appeared to be of minor medical importance, the investigation should end.’Footnote 24 The medical department's survey of sleeping sickness that year was written by K. R. S. Morris, an assistant entomologist who had only recently arrived in the Gold Coast.Footnote 25 Ten years later, Morris oversaw the vast campaign of anti-tsetse forest clearance that fed into the onchocerciasis revelations of the independence era.
By the mid-1930s the extent of epidemic sleeping sickness in the North had become undeniable, giving rise to recriminations from local officials. In 1937, the Chief Commissioner of the Northern Territories observed:
In 1928 it was reported that ‘both human and animal trypanosomiasis is relatively unimportant’; while so recently as 1933 an Assistant-Director of Medical Service, although recording an increase in the number of cases treated, found it impossible to convince himself that ‘human trypanosomiasis is such a serious cause of morbidity and mortality as to justify the diversion of large sums of money to eradicate it at the expense of other medical services needed by the inhabitants of the Colony’. But officers with long local experience of the Protectorate did not share the optimism implied in the extracts quoted above, and pointed to the areas where to their certain knowledge the high mortality caused by trypanosomiasis had led to the gradual depopulation and eventual abandonment of many villages.Footnote 26
This unusual public criticism indicated the extent to which perceptions of the severity of the epidemic had diverged, between a more distant southern administration and northern officials who had directly witnessed its effects.
The anti-tsetse bush clearing campaign and onchocerciasis
The years after 1935 were a time of revelation, as far as official recognition of sleeping sickness was concerned. In 1936 the Gold Coast's annual report acknowledged nearly 5,000 cases in the Northern Territories, and a survey of the far northwest indicated that 35 to 40 per cent of people were suffering from the disease.Footnote 27 Understatement was no longer an option, and the Accra government allocated significant funds towards a medical campaign based on short-term epidemic control though a network of quarantine camps and treatment with a range of drugs. This successfully reduced the infection rate by the early 1940s.Footnote 28 Also in the late 1930s, as the treatment campaign against sleeping sickness continued to expand, a more expansive and enduring campaign was launched against the disease's vector, the tsetse fly. The work of this campaign — which proceeded with relatively little supervision from the North's political administration or its medical department — seems to have inadvertently contributed to the subsequent epidemic of onchocerciasis, a disease which came to local and international prominence during the independence transition.
Apart from immediate treatment and quarantine measures, it was recognised that, in the long term, epidemic trypanosomiasis in both humans and livestock would only be brought under control by breaking the cycle of tsetse fly transmission. In the mid-1920s, the Imperial Bureau of Entomology had already made enquiries about the potential application of the ‘Swynnerton Method’ for tsetse control in the Northern Territories, an approach which had been successfully used in British Tanganyika.Footnote 29 This involved the destruction of habitat vegetation where the fly lived and reproduced, through large-scale cutting and burning, with the aim of reducing fly populations and limiting the spread of trypanosomes to existing settlements. In the North, some limited measures of this type were used by the late 1920s. Clearing took place in narrow corridors along the principal labour and cattle routes running from Upper Volta through the North, and around the principal transit towns on the borders with Ashanti and the Colony — part of an ongoing epidemiological and economic detachment of North from South, with northern health problems contained in the region while labour and livestock continued to move.Footnote 30
This limited bush clearance work was suspended with the onset of global economic depression in 1929, but it was resumed on a much larger scale after the extent of epidemic sleeping sickness was recognised in the mid-1930s.Footnote 31 K. R. S. Morris, recently dismissed in post-depression staff cuts in 1930, was reemployed to devise and oversee the anti-tsetse scheme, which operated between 1937 and 1955. Morris's work is one of few aspects of the history of medicine in northern Ghana to have attracted previous research attention. Jeff Grischow's research approaches Morris as an agent of progress, emblematic of the ‘developmental’ phase of colonial rule, who achieved success in reducing sleeping sickness despite his idiosyncratic theories of disease transmission.Footnote 32
Although limited anti-tsetse bush clearing was carried out along labour and cattle routes in the preceding decades, this had been accompanied by local administrative resistance to any major clearance campaign away from main roads.Footnote 33 When the Imperial Bureau of Entomology had asked the Gold Coast administration in 1925 to examine how the Swynnerton Method might be applied in the North after its success in British East Africa, the Chief Commissioner of the Northern Territories replied that tsetse eradication schemes of this kind were unsuitable to the region: there was insufficient local labour available, and any major scheme of bush clearance would disrupt economic activity (including the recruitment of migrant workers for the South). The administration's counterproposal recommended that any bush clearing should instead be left to native farmers and mining companies, who were ‘already doing good work for civilisation by encroaching into it yearly’, and that the tsetse fly problem should instead be addressed through a major resettlement campaign. This proposed that immigrants from French territory and communities from the northern border areas should be offered farming tools, livestock, and exemption from forced labour for 25 years as inducements to resettle and farm in areas of high tsetse prevalence to the immediate south. The administration argued that this would lead naturally to clearance of the bush.Footnote 34
Although it was not enacted at the time, the 1925 scheme embodied a longstanding aim of the colonial administration: to move communities away from the densely populated northern frontier and closer to the southern labour markets. As a related aim, the administration considered that there was underpopulated land in the Northern Territories — particularly the southern Gonja districts — which could be turned to export agriculture and increased food production. In 1937 these goals were clearly articulated in Morris's new proposals for an anti-tsetse bush clearing scheme which, unlike the Swynnerton Method, was explicitly directed towards the large-scale resettlement of the cleared areas. The ‘discovery’ of the 1930s sleeping sickness epidemic certainly also gave rise to its own immediate pressures for a tsetse eradication programme. Faced with mass infection, the Colonial Office requested in 1935 that urgent action should be taken to avert a potential disruption to the mine labour supply.Footnote 35 Grischow argues that the Gold Coast government may also have conceived of the anti-tsetse campaign ‘as a hedge against political resistance’, although this is doubtful — there was no nationalist resistance in the North in the 1930s, when the campaign was conceived.Footnote 36
Once these proximate pressures are taken into account, however, Morris's proposals appear to have won support because they chimed with the long-term preferences of the Gold Coast government for the resettlement of northern communities towards the southern labour markets and for the local development of productive agriculture. As the Northern Territories annual report observed in the martial idiom of disease control:
[The situation] presents an excellent opportunity for a large-scale experiment of an aggressive attack upon trypanosomiasis. Briefly stated, the plan comprises simultaneous fly eradication and treatment of the disease, to be followed by repopulation and intensive development of the area. . . . [Morris's] plan of campaign differs basically from the policy adopted in Tanganyika. The latter involves the abandonment of territory to the enemy and may be described as a defensive retreat whereas the former, if successful in operation, will result in the recapture of valuable territory.Footnote 37
In other words, Morris and the administration saw the induced repopulation of cleared bush areas as central to their ‘experiment’, in light of its anticipated economic benefits and in contrast to the relocation of communities away from tsetse clearances in East Africa.
The resettlement aspect of Morris's plan was attractive to an administration which had already been looking for a way to achieve this goal. But it was also this element that would bring northern peoples into increased contact with onchocerciasis, a disease which was not contemplated when designing the scheme. In his proposed explanation of unusual population distributions in the North, Morris only paid attention to one disease. During entomological surveys as a junior official, he had observed the ruins of long-abandoned villages along river valleys in the North and had read scattered reports on sleeping sickness from preceding decades. In conversation with local peoples, some northern officers in the early 1900s had recorded that sleeping sickness and general poor health were occasionally associated with slave raiding by Zabarima forces under Babatu Zatu in the 1880s, more than 50 years previously.Footnote 38 Morris combined these amateur archaeological and historical observations with his knowledge of tsetse ecology, resulting in an elaborate theory which he believed accounted for the depopulation of river valleys and the impacts of sleeping sickness in the North. Grischow gives a summary of this theory:
Ecological collapse was triggered by slave raiding in the nineteenth century, which reduced population densities to a point where the people could not fend off wild game or cultivate their bush farms. Tsetse flies invaded the farms, infested the wild game and moved into the villages to attack the people themselves. Production declines caused further food shortages and depopulation until entire villages disappeared. By the 1930s the cycle of decline had set the conditions for a trypanosomiasis epidemic to wipe out many of the settlements along the Black Volta and its tributaries . . . Faced with this situation, Morris and his team took on the challenge of reversing the process of ecological imbalance in the Northern Territories.Footnote 39
Here Morris had extrapolated from one or two brief observations from past district officers, regarding a nineteenth-century association between slave raiding and sleeping sickness among northern communities, to construct a long-term epidemiological history of the disease in the North that accounted for the depopulation of fertile river valleys.
His theory was already present in a report that Morris submitted as a subordinate entomologist in 1929, before he was dismissed in the staff cuts which followed the onset of the Great Depression. Then a junior officer, Morris conceded that his ideas ‘may be over dogmatic, and the observations carried out in a comparatively short space of time’.Footnote 40 When he was reemployed in the late 1930s to implement a major campaign of anti-tsetse bush clearance, he showed no such doubts. Morris promoted his work through a number of metropolitan journals, and his ideas were perhaps more widely disseminated in London than in the Gold Coast.Footnote 41
Morris insisted that his theory of sleeping sickness accounted for the historical depopulation of river valleys and that his clearance and resettlement methods would therefore open the way to an agricultural boom. But his campaign was based upon a critical misunderstanding of the northern disease environment, indicated here for example in 1946:
The removal of tsetse throughout the river system . . . has the following additional advantages: It makes possible a sound agricultural development . . . It enables the population to live with impunity in the vicinity of permanent water and to avoid concentrations on dry, hilly country away from rivers; thus the possibilities of over-farming and erosion are avoided and the watersheds and headwaters can be reserved for afforestation. By these means, instead of ground being abandoned to the tsetse, the fly is replaced by a healthy agricultural population.Footnote 42
Onchocerciasis was almost (but not entirely) unknown in the colony at this time, and Morris's ideas convinced the Gold Coast government, which already had the aim of resettling northern populations.Footnote 43 The bush clearing campaign operated with generous funding allocations from 1937 to 1952.Footnote 44 It began on the valleys of the Kamba River, a tributary of the Black Volta in the northwest, and by the 1950s major clearances had been carried out on many of the Volta system rivers of the North. The clearances employed thousands of northern people, although it appears that at least some of this was unpaid or coerced labour, obtained through the Native Authority system.Footnote 45 After the Second World War these labourers were paid, although on relatively austere terms — in some cases workers were required to pay the government for their cutting tools.Footnote 46 In addition to archival sources, this paper examines interviews with individuals who were employed on the anti-tsetse campaign from the late 1940s, usually as youths.Footnote 47
The campaign's central method was ‘selective clearing’: the removal of rough-boled tree species which were considered to harbour the tsetse fly, leaving other riverine vegetation intact. In practice this meant the felling and burning of most vegetation along the banks of each watercourse (see Figs. 2, 3, and 4).Footnote 48 With resettlement and farming as an aim, the clearing was intended to be permanent. Some of those who worked on the anti-tsetse gangs recalled that their pay was docked if there was any regrowth of new shoots, with inspections carried out months after clearance.Footnote 49

Fig. 2. Clearing of riverine forest along river systems in the northern Gold Coast. Reproduced from a pamphlet published by the Gold Coast Public Relations Department and K. R. S Morris, Fighting a Fly (Accra, 1950), 14. Courtesy of PRAAD-Accra.

Fig. 3. Clearing of riverine forest along river systems in the northern Gold Coast. Reproduced from Morris, Fighting a Fly, 14. Courtesy of PRAAD-Accra.

Fig. 4. Burning of riverine forest along river systems in the northern Gold Coast. Reproduced from Morris, Fighting a Fly, 14. Courtesy of PRAAD-Accra.
There is no way to gauge the full extent of the clearance work carried out between 1937 and the mid-1950s. It appears that regular activity reports were not required by other branches of the administration. The data relating to some river valleys or communities does not appear to have been retained in any archives, while other rivers and settlements listed by the campaign have since been renamed. In part this was because the North's Tsetse Control Department (TCD) functioned as an independent organisation under Morris and his deputies, reporting to the Department of Agriculture in Accra and operating largely without supervision from the Medical Department and the Northern Territories administration.Footnote 50 However, an indication of the scale of the campaign comes from the TCD's retrospective summary of its work in early 1950s, when the Gold Coast's governance was being reoriented towards independence and the public health value and costs of the campaign were increasingly called into question. The department reported that in the small northwest region alone it had cleared over 2,000 square miles of riverine bush (approximately twenty times the area of contemporary urban Accra, or three times the area of Greater London), including 600 square miles along the Kamba valley.Footnote 51
Around 500 people had been ‘placed’ here in an initial post-clearance resettlement scheme in the early 1940s, and by 1949 Morris noted that a further 1,500 people had voluntarily resettled in the valley and established over 4,000 acres of new farmland. Multiple dams were built on the river and its tributaries, and roads were constructed to allow access for communities and livestock — Morris reported that 90,000 people now had tsetse-free access to river valleys in the Lawra area.Footnote 52 The Kamba clearances were often cited as the model by which the overall campaign proceeded, and similar developments took place across the North. In the Damongo area of the Gonja district, for example, on the Sorie tributary of the Black Volta, 1,000 square miles of bush was cleared and 1,200 people resettled between 1944 and 1952, with a further sixty families resettled at a location referred to as ‘Piri Lake’.Footnote 53
This was the most expansive public health measure undertaken in the North during the colonial period, mobilising many communities and spanning more than twenty years. Patterson and Grischow have approached the campaign as a scientific or a developmental success, and the sources suggest that, in tandem with the Medical Department's quarantine and mass treatment campaign, it was indeed successful at reducing the incidence of sleeping sickness.Footnote 54 The campaign was shaped by Morris's theory about the historical abandonment of river valleys in response to trypanosomiasis and driven by the desire of the colonial administration to increase revenues from the North. Grischow argues that it represented a successful colonial engineering of socioeconomic behaviour, which ‘set out to reverse a process of maldevelopment by redistributing the African population in the Kamba and Kulpawn river valleys’. Seen through this developmental lens, the campaign was not simply a contingent intervention against the immediate epidemic, but instead ‘the long-term goal of tsetse eradication was to even out population densities across the Northern Territories, as a basis for sustained community development’.Footnote 55
The relationship between tsetse control and epidemic blindness
The TCD's work secured Morris a reputation as an international expert, and its campaign has been hailed as a success in subsequent research. However, the anti-tsetse programme's public health benefits in reducing the spread of sleeping sickness, or its economic benefits in bringing agriculture to unpopulated valleys, must be considered in tandem with its unintended consequences. By 1950 anti-tsetse bush clearance had been under way along northern watercourses for more than 15 years. The project had begun with smaller-scale clearings at river crossings and around settled areas, but under Morris it expanded into a sweeping campaign for the clearance of Volta-system river valleys and their tributary streams, accompanied by a resettlement programme which encouraged people to move into the cleared zones and provided dams and access roads to make these areas attractive. The campaign promoted the idea that in these areas it was now possible for northern communities, in Morris's words, ‘to live with impunity in the vicinity of permanent water’.Footnote 56 In the Kamba valley, the TCD had even tried to develop fishing as a principal economic activity (see Fig. 5).Footnote 57

Fig. 5. Cleared riverbank on the upper Kamba River ca. 1938. Morris's caption suggested that, following the clearance and resettlement work of his department, ‘the people [we]re free to draw water, wash and linger by the waterside without danger.’ Reproduced from Morris, Fighting a Fly, 15. Courtesy of PRAAD-Accra.

Fig. 6. Members of a resettled community farming beans on the cleared riverbank of the northern Volta, ca. 1937–50. Reproduced from Morris, Fighting a Fly, 17. Courtesy of PRAAD-Accra.

Fig. 7. The Tsetse Control Department set out to encourage fishing as an economic activity on the Kamba and other rivers. Morris's caption to this image proposes: ‘Fishing is now a safe (and happy!) occupation on the Kamba river, with the impenetrable fringing bush, that held so many tsetse, now cleared away.’ Reproduced from Morris, Fighting a Fly, 20. Courtesy of PRAAD-Accra.
All of this had been done in ignorance of the risk from onchocerciasis, a disease with an infection rate which, unlike sleeping sickness, is strictly determined by proximity to flowing water. The tsetse flies which transmit human sleeping sickness require shade and woodland, often close to water, but can live and reproduce in any area where these and a mammalian food supply come together, in some cases far from river valleys.Footnote 58 But the Simulium blackflies that transmit the Onchocerca parasite require flowing water to breed, and infection rates from onchocerciasis decline with the distance of a community from a river or stream.Footnote 59 Morris's anti-tsetse campaign had resettled people directly into zones of increased onchocerciasis transmission, and by building dams it had also improved the breeding conditions for the disease's insect vector — it has been demonstrated that dam spillways provide an optimal, well-oxygenated breeding environment for Simulium damnosum blackflies.Footnote 60 Even where settlements were not established in cleared areas, the campaign increased exposure to the disease by opening access roads to valley floors that had been cleared of dense vegetation, turning them into convenient low-lying routes for travel or for grazing livestock. As well as directly exposing surrounding communities to the disease, the changes brought by the mobile clearing campaign may have worsened the overall epidemiological picture for onchocerciasis and related blindness in the North. Increased transmission of onchocerciasis in campaign areas contributed to a greater total number of people and blackflies hosting the parasite, amplifying the disease as both carried it to new districts away from the cleared valleys.
Morris's TCD was apparently uninformed about onchocerciasis, although the disease had been the subject of research interest and active control programmes for years both within Britain's colonial health system and the broader transnational medical community. In Kenya over the same period, for example, the colony's medical department also ran a campaign to clear the Kodera River valley of biting flies so that people could be resettled there. But the flies it targeted were not tsetse. Instead the campaign was against the Simulium blackfly vector of onchocerciasis, because in Kenya it was recognised that resettlement of such valleys was ‘an impossibility’ until the blackfly had been eradicated.Footnote 61 Across the border from the northern Gold Coast, authorities in French Upper Volta had also reported widespread onchocerciasis infection and begun control measures by the early 1940s.Footnote 62 But despite evident knowledge of the public health risks of onchocerciasis circulating in the worlds of colonial health, and despite various imperial conferences and memoranda from the health section of the Colonial Office, personnel working in one part of Africa could remain uninformed about what was happening in relation to the same disease or control method elsewhere.Footnote 63 In regions like the Northern Territories, where interventions took place with little coordination from the central government let alone from London, colonial-era public health work was very much the product of individual officials, their theories, and the knowledge they did or did not possess. This was true even in the 1950s and has at times been the case in northern Ghana since independence.
The TCD not only worked in ignorance of an accumulating body of colonial knowledge about onchocerciasis. It also paid little attention to knowledge of the disease among African communities, evident in colonial reports over decades, and actively encouraged its personnel to act in contradiction of this knowledge. The campaign took place at a time when northerners were increasingly turning to state-sponsored healthcare, which had demonstrated its curative capacity against some of the region's most prevalent diseases, including drug treatments for malaria and yaws, and effective vaccination against smallpox. From the mid-1930s, the new sulphonamide antibiotics and then penicillin offered a new way to cure many serious diseases affecting northern peoples — when sulphonamides were used during meningitis epidemics from 1939–45, for example, the mortality rate fell from 80 per cent to 10 per cent of those infected.Footnote 64
By the late 1930s, therefore, local political and health officials and the Gold Coast Medical Department reported that some curative successes had increased the confidence of northern communities in colonial healthcare. They argued that this was further demonstrated by the increased uptake of drugs and clinical and preventative services.Footnote 65 Without further evidence from the perspective of northerners themselves, these assertions about increased confidence are hard to evaluate. If this were the case, it is possible that the medical successes described above may also have led people to trust the message promulgated by the bush clearing and resettlement campaign: that it was now safe to live and spend time in river valleys, with further inducements in the form of agricultural equipment for those who settled there. But in promoting this message, as with planning the overall clearance and resettlement campaign, Morris and the TCD were apparently unaware of a substantial body of local onchocerciasis knowledge which might have indicated to them why the valleys were previously avoided.Footnote 66 At least some northern communities were aware of the link between nodules caused by the Onchocerca parasite and eventual blindness, and they had effective ways of treating the condition.
In 1928, among other examples, a medical officer recorded that villagers in the northwest had the same practical understanding of the disease as villagers in Guatemala, whose information had led the physician Rodolfo Robles to first propose a link between the parasite and blindness:
Both in Lawra and Tumu it is believed that the nodules of Onchocerca volvulus cause eye disease when situated on the scalp. For this reason a considerable number of people come to have them removed . . . Native surgeons remove them by burning the skin and then extracting the tumours with a knife; this is often neatly done. The extraordinary fact of finding the same belief in Guatemala and in Lawra-Tumu calls for some remarks.Footnote 67
The underlying understanding of the disease among northwestern villagers and rural Guatemalans may in fact have differed substantially. But the perceived link between nodules and blindness, and the resulting surgical technique, was a testament to the aetiological reasoning of people whose medical practices were often depicted as distinct from or less effective than those of biomedicine. Northerners were also aware of the association between river valleys and blindness, and this was why they settled and farmed at a distance from flowing water. In his landmark survey covering most major river valleys of the North in 1949, which first indicated the scale of the region's onchocerciasis problem, the British medical officer B. B. Waddy observed that ‘the probability of going blind is consistently given by natives as their reason for not farming close to rivers where onchocerciasis is endemic. It is notable that practically no natives of the Northern Territories fish: such fishing as is done is by immigrants from the coast.’Footnote 68 The same apparently longstanding knowledge was found among rural communities across the North after independence, during initial visits by the Onchocerciasis Control Programme in the early 1970s:
The interesting thing about the onchocerciasis — it was something that everybody, virtually everybody around knew. They knew that this is what was making the people blind, because they associated it with people staying by the river area. So when the programme came it was absolutely no problem in engaging the people.Footnote 69
On several occasions then, from the mid-colonial period and into the independence era, northern communities had communicated at least some prior knowledge of a link between river valleys and the risk of blindness.
In Northern Nigeria this local onchocerciasis knowledge was taken into account by colonial authorities, at least in some cases. Here communities also associated blindness with drinking river water. When the British administration tried to convince people to move into abandoned valleys in the late 1940s, it found that ‘the natives attribute the original depopulation of these areas to onchocerciasis, and resettlement will not be accepted until onchocerciasis is controlled.’Footnote 70 This stood in contrast to the theories of the Gold Coast TCD, whose work was shaped by Morris's belief that sleeping sickness had led to the abandonment of watercourses, and whose resettlement policy operated on the basis that river valleys had been made safe for habitation. The implications of this misunderstanding were revealed in onchocerciasis infection data that was compiled in two successive surveys conducted in 1949 and 1952–5: the first by Waddy, a concerned local medical officer, and the second funded by the British Empire Society for the Blind. The latter survey, which covered colonies across Africa, showed that the Northern Territories of the Gold Coast had the highest known levels of onchocerciasis infection worldwide.Footnote 71
Here Northern Nigeria makes another useful counterexample. Apart from the upper Sahelian edge of Northern Nigeria, the two regions span the same latitudes and are comparable in terms of climate, ecology, and the presence of many diseases. In Nigeria the colonial administration had also undertaken a tsetse-clearing and resettlement project, but on a more limited scale, using methods which reduced exposure to onchocerciasis infection. This was the Anchau Scheme in Zaria Province, implemented by the entomologist T. A. Nash from 1938 to the late 1940s.Footnote 72 The project cleared and resettled a tsetse-free corridor covering 712 square miles, less than the 1,500 square miles that were reported to have been cleared in the Northern Territories’ Kamba valley alone. Crucially, the Anchau resettlement villages were constructed at some distance from water, around concrete wells intended to reduce the need for communities to risk infection by entering valleys.Footnote 73 In the Northern Territories, however, the TCD instead built dams in the valleys to provide water, with spillways which provided an optimum breeding habitat for the blackfly and which compelled people to constantly visit these breeding sites. When the British Empire Society for the Blind surveyed Northern Nigeria and the Northern Territories for total blindness, the differences were evident. In Northern Nigeria, 0.8 per cent of the population were found to be blind. In the northern Gold Coast, the number of blind people was more than three times higher, at 3 per cent of the population, with approximately 60 per cent of this blindness estimated to have been caused by onchocerciasis.Footnote 74 This soon became a headline figure in global activity against the disease, quoted by charities, transnational organisations, and governments, thus making northern Ghana the regional ‘poster child’ for a newly recognised public health emergency.Footnote 75
By the early 1950s, serious levels of endemic onchocerciasis were being discovered across West Africa, and it is likely the disease would have been widespread in the North even in the absence of anti-tsetse clearance and resettlement. But in survey data from the late colonial period, it is striking how closely zones of the most severe onchocerciasis infection can be mapped onto the activities of the TCD. The 1952 survey indicated that the single worst-affected location in West Africa was the valley of the Kamba River, where Morris had begun his clearance work and where resettlement and dam building had been sustained for the longest time. More than one in ten people living here were blind from onchocerciasis — 12.6 per cent of all adults and children. The Kamba River valley was described in international reportage and fundraising publications as West Africa's ‘Valley of the Blind’, while northern Ghana was labelled the ‘Country of the Blind’.Footnote 76 The Simulium blackfly was found to be breeding in large numbers below the laterite dams that had been constructed on the river and its tributaries during the tsetse resettlement campaign. The Kamba subsequently became the initial focus of efforts to eradicate the disease in the North and continued to be a principal focus of onchocerciasis control work into the 1960s.Footnote 77
Similarly high rates of onchocerciasis infection and blindness were found in the Damongo area, another centre of TCD clearance and resettlement, where its work had proceeded alongside a large-scale colonial project to boost groundnut production.Footnote 78 Bush clearing, dam building, and resettlement had been underway for more than six years by 1953, when the British Empire Society for the Blind's onchocerciasis survey arrived.Footnote 79 The survey found that people who lived and farmed in the areas cleared by the anti-tsetse campaign had significantly worse onchocerciasis infection rates (over 20 per cent of the population) than those who lived in the old town of Damongo itself, 4 km distant from the cleared Sorie River system (5 per cent), indicating that the resettlement programme had brought people into closer contact with the disease.Footnote 80 It is also possible that the parasites may have been carried to new areas by the anti-tsetse campaign itself, as large clearance teams moved between relatively isolated valleys and villages. Bush clearance and resettlement proceeded in the Damongo area until independence in 1957, and the prevalence of the disease worsened. In the early 1960s, a WHO study recorded that the district was among the most severely affected by onchocerciasis in northern Ghana, with up to 25 per cent blindness in some villages. Here dam-building had also increased the breeding habitat for Simulium blackflies.Footnote 81
Beyond these two examples there were many further strong overlaps between anti-tsetse work and high rates of onchocerciasis infection at various sites. These included the Kulpawn valley and its tributaries (notably the Sissili River), the White Volta system which runs north of the Gambaga escarpment, and almost all river valleys of the far northwest. Here, by 1953 the TCD reported that it was clearing ‘the last important river’, with re-clearance and additional dam building under way on several rivers that had previously been cleared.Footnote 82 From the available sources, it is impossible to definitively conclude that the tsetse control programme was responsible for these high rates of infection and blindness in the North, relative to other areas in the Gold Coast or neighbouring colonies. Onchocerciasis was increasingly recognised as a serious disease across West Africa at this point, and infection would likely have been widespread in any case. But it seems probable that Morris's Tsetse Control Department unwittingly and significantly increased the prevalence of onchocerciasis in the areas where it operated — and across the Northern Territories as a whole — by transporting potentially-infected staff from district to district, opening valleys for grazing and passage, building dams and access roads, resettling people in valleys, and spreading the message that rivers were now safe.
Contexts
It is worth asking how onchocerciasis was neglected in northern Ghana for so long, although it was increasingly well known elsewhere in colonial Africa, and how the anti-tsetse campaign was able to proceed for years with a project that evidently exposed people to the disease. As I have suggested previously, the roots of these problems lie in the peripheral situation of the North, regarded as a region of low economic importance (unlike the areas cleared in Kenya or Uganda), with African populations that had little or no political influence on the colonial administration (unlike Northern Nigeria). Stemming from this general marginality, there were several proximate factors which meant that anti-tsetse policy was never called into question. Perhaps most importantly, the TCD functioned as an independent unit of the Gold Coast government, with its own staff and budget. It reported principally to the Department of Agriculture in Accra, with limited oversight from either the Gold Coast Medical Department or the Northern Territories administration. Correspondence from the early 1950s shows the extent to which the campaign had operated in isolation from local officials. For years, the North's Chief Regional Officer (previously Chief Commissioner) tried unsuccessfully to obtain a report from the TCD on its activities in the region. But details of these activities were only issued in 1954, when the new Ministry for Agriculture (created on the eve of independence and under the leadership of a Ghanaian) eventually intervened to demand that the information be handed over.Footnote 83
There appears to have been similarly little oversight of the tsetse control campaign from the Medical Department at Accra, and apart from Morris, himself a medical entomologist, there was no local medical oversight of its work in the North. Staffing levels meant that some of the rural areas where the campaign operated were rarely visited by other Medical Department staff during the late colonial period, with ‘only one medical officer (two before the war) being available for the entire Northern Territories west of the White Volta-Sissili line’.Footnote 84 This was precisely the region where anti-tsetse work had been most active. The location of the campaign within the Department for Agriculture suggests another reason why the clearance and resettlement scheme was not called into question: because Morris's ideas tallied with the economic goals of the administration, unrelated to human disease or public health. To use Grischow's term, the government had for decades been seeking a way to correct what it saw as the ‘maldevelopment’ that had led communities to avoid the most productive valley land.Footnote 85 The long-run history of public health in northern Ghana shows some repetition in this regard. Well-meaning solutions to economic problems, championed by bodies outside of the public health system, posed similar risks to the health of northern people after independence. In the mid-1960s, for example, the WHO became aware that another United Nations agency, the Food and Agriculture Organisation (FAO), was collaborating with Ghana's Ministry of Agriculture to survey the North in advance of a vast dam-building and irrigation scheme that involved large-scale resettlement with the similar aim of improving agricultural production. The WHO intervened to restrict the project, noting that Ghana's own Ministry of Health had never been consulted in the FAO's proposal and that the North's water-related diseases had again not been taken into account.Footnote 86
In the absence of official knowledge about onchocerciasis, Morris's proposal had seemed to offer a solution to a long-standing problem. His well-funded campaign ran for years with little oversight, the product of ecological and developmental theories which disregarded relevant local knowledge of disease and vested a great deal of intellectual and practical power in a single well-intentioned but misinformed individual. It was perhaps unsurprising that relevant African knowledge was discounted — this appears to have been a principle established in the early days of tsetse control. In instructions issued to the Gold Coast government in 1914, for example, the Imperial Bureau of Entomology had emphasised that entomologists ‘should in no case rely on native evidence’ when investigating the distribution of tsetse and other biting flies.Footnote 87 But failure to identify the risk from onchocerciasis during the 15-year anti-tsetse campaign also indicated the gaps in institutional knowledge which separated the various departments of the colonial government. These were particularly pronounced in a remote region like the North, where low funds and staffing meant there was little possibility for even incidental supervision of independent projects.
It is nevertheless somewhat surprising that nobody commented on the confluence of the anti-tsetse bush clearing campaign, extensive blindness, and existing local knowledge regarding the abandonment of river valleys, particularly in light of a slow but significant accumulation of medical knowledge about onchocerciasis in the Gold Coast.Footnote 88 Sleeping sickness and tsetse control were abiding sources of concern, but onchocerciasis was increasingly recognised as a serious public health risk in many of Britain's African colonies, and none had pursued valley clearance and resettlement in the same way as the northern Gold Coast. The colonial sources record no recognition that the TCD's clearance and resettlement campaign may have exposed people to the disease, although some individuals did raise implicit criticisms of the project. Once onchocerciasis in the Northern Territories started to receive international attention in the mid-1950s, the idea that valleys had once been abandoned due to sleeping sickness was quite suddenly considered ‘very far-fetched’: it was now ‘known’ that onchocerciasis had driven people away.Footnote 89 The low importance and staffing accorded to the North meant that the relationship between tsetse control and onchocerciasis may simply have gone unnoticed. As with sleeping sickness in the late 1920s, there might also have been an official reluctance to recognise potentially costly health problems in the region, or perhaps even an unstated calculus that increased blindness was an acceptable price to pay for reductions in sleeping sickness and livestock trypanosomiasis. Shortly before he died in 1981, retired northern medical officer B. B. Waddy recalled that when he presented the results of his 1949 onchocerciasis survey to the Gold Coast's Director of Medical Services, he was ‘accused of being a madman’ and that the ‘very existence’ of onchocerciasis in the North was denied for many years.Footnote 90
Conclusion
This paper has explored the connections between two public health problems over a long period of time. A campaign against sleeping sickness in the colonial period unwittingly intensified the infection of northern communities with onchocerciasis, which eventually led on to a postindependence onchocerciasis control campaign that encompassed many of the same areas, actions, and developmental objectives. From the 1920s to 1950s, the northern Gold Coast's persistent marginality meant both that colonial sleeping sickness went unrecognised until it impinged on the southern economy and that onchocerciasis infection only became a matter of concern when a metropolitan charity surveyed the disease on the brink of independence. The North's peripheral situation allowed Morris's bush clearing to proceed with little oversight. His proposals were accepted not only because of the immediate sleeping sickness epidemic, but because they offered a way for the administration to achieve its longstanding goal of redistributing the northern population.
Blindness was the most noticeable effect of widespread onchocerciasis, but its systemic impact on northern communities was probably much greater. Recent research, which tracked the health of 300,000 people in West Africa between 1971 and 2001, suggests that populations burdened by a heavy microfilarial load — the presence of onchocerciasis parasites in the skin and tissues — experience an excess mortality rate of around 5.2 per cent independently of the incidence of blindness.Footnote 91 The persistent high transmission of onchocerciasis over decades in the North, exacerbated by the anti-tsetse campaign and by a lack of systematic control efforts until 1974, would have contributed to further divergence in the health and productivity of northern peoples relative to the South, even when other interventions (the provision of better education, for example) were seeking to narrow this gap.
What is missing from this account are the experiences of those who suffered from onchocerciasis or sleeping sickness, or who witnessed the sweeping control measures against each disease. It is interesting to note that the two diseases have become elided in the memories of many interview subjects across the North, and both are now being forgotten as the threat they pose recedes. In some communities, I met people who had worked on the anti-tsetse campaign as teenagers or children — they remembered seeing or hearing about ‘Dr. Morrow’ (Morris) and his stringent requirements for bush clearing. Few communities remembered encountering anyone who suffered from sleeping sickness, however, and in general only older people were familiar with the symptoms of the disease. This stands in contrast to the first decades of colonial rule, when, as one official noted,
the people considered the disease shameful and kept those suffering from it confined to a hut on the outskirts of the village. Those dying of it were denied the ordinary burial, and before burial the bones of their right hand were broken and the hand bent back.Footnote 92
Officials recorded that many northern communities treated sleeping sickness as a grave affliction.
But by the late 1930s, as the medical campaign had success in treating the disease, it was observed that ‘the former widespread practice of separate burial for victims of trypanosomiasis is now dying out’.Footnote 93 During my interviews, most questions about disease control pertaining to rivers, or diseases spread by biting flies (as opposed to mosquitoes or other insects) were answered with ‘oncho’. Some people insisted that Dr. Morrow's colonial-era work on the same river valleys had in fact been part of the WHO Onchocerciasis Control Programme of the 1970s. Many people recalled the decades of onchocerciasis control work that came after independence. By 1985, communities around northern Ghana had lived through 50 years of near-constant vector control work along their river valleys, against the different flies that carry sleeping sickness and onchocerciasis. But in 2015, onchocerciasis as a disease was also being forgotten, and other causes of blindness and itching were more prominent sources of concern for old and young interview subjects.Footnote 94 In a sense this shows the achievements of the colonial-era campaign against sleeping sickness and the postcolonial campaign against onchocerciasis — which was to some extent produced by colonial anti-tsetse work. Both campaigns reduced the disease which they set out to control. Despite the serious unintended consequences outlined above, forgetting is the result of this success.
Financial Support
This research was funded by the Arts and Humanities Research Council (Doctoral Grant No. 1351945), and was supported by the European Research Council (Project No. 759820 - ‘Universal Health Coverage and the Public Good in Africa’).








 Open access
Open access