


Platybasia, flattening of the skull base, causes upward displacements of the odontoid process through the foramen magnum (basilar invagination), which reduces the space of the posterior fossa.Reference Pearce 1 Platybasia mostly produces headaches induced by coughing, lower cranial nerve palsies, pyramidal signs, syringomyelia, and hydrocephalus.Reference Pearce 1 Despite about a quarter of patients with platybasia experiencing vertigo,Reference Ibrahim and Crockard 2 detailed descriptions on the neuro-otologic findings are not available in the literature. Here we report on a patient with platybasia who showed Bruns’ nystagmus and bilaterally positive head impulse tests (HITs), which are regarded as characteristic signs of a large cerebellopontine angle tumor compressing the cerebellum.
A 55-year-old man presented paroxysmal vertigo and imbalance for five years, precipitated by neck extension and associated with rushing water tinnitus in the left ear. He had also suffered from choking, drooling, and right-side weakness for years. He had lost his permanent teeth in early childhood and had been taking calcitriol for osteoporosis, but had sustained a compression fracture of the lumbar vertebra. Neurologic examination showed small right beating spontaneous nystagmus in the light. In darkness the nystagmus increased and accompanied the upbeat component. Rightward gaze increased right beating nystagmus with a linear slow phase, and leftward gaze produced left beating nystagmus with a decelerating slow phase (Fig. 1A, Video), which is consistent with Bruns’ nystagmus. Other findings included right hemiparesis with muscular atrophy, loss of thermal and painful sensation in the right arm, generalized hyperreflexia, and bilaterally positive Babinski sign. HITs documented decreased gains for all semicircular canals (Fig. 1B). Bithermal caloric tests were normal. Audiometry showed high frequency sloping in both ears. Bone densitometry showed severe osteoporosis. Brain MRIs disclosed platybasia and basilar invagination into the distorted posterior fossa, which caused a compression of the lower brainstem and the cerebellar flocculus (Figure 1C, D). Cervical MRI showed a narrowing of upper cervical canal and myelomalacia (Figure 1E).
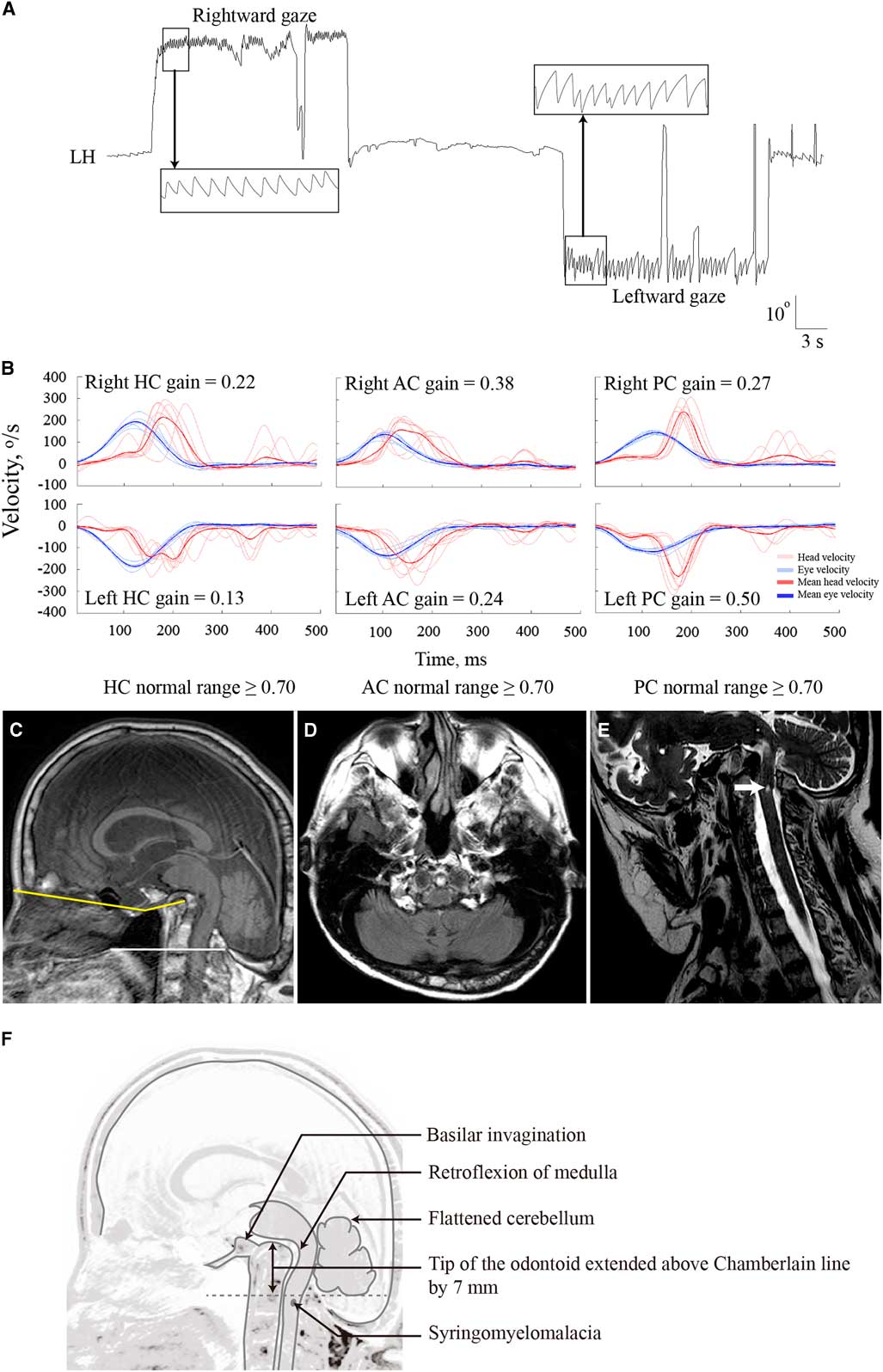
Figure 1 (A) Horizontal gaze produces Bruns’ nystagmus. (B) Head impulse tests documents decreased vestibular-ocular reflex gains for all canals. (C) Brain MRI shows a widened angle of the skull base (yellow) and a protruded odontoid process >5 mm above the Chamberlain’s line (white). (D) Axial view discloses compression of the caudal brainstem and cerebellar flocculus by a distorted posterior fossa. (E) Cervical MRI shows narrow canal and myelomalacia at C2. (F) Illustration depicts the anomaly observed on MRIs. LH=horizontal plane of the left eye; HC=horizontal canal; AC=anterior canal; PC=posterior canal
Our patient with platybasia and secondary basilar invagination presented paroxysmal vertigo and progressive imbalance that was exacerbated by head motion. Neurologic examination showed Bruns’ nystagmus and bilaterally positive HITs. Severely reduced skeletal mass and the history of fragile teeth and vertebrae were suggestive of osteogenesis imperfecta.Reference Ibrahim and Crockard 2 Bruns’ nystagmus is generally regarded as indicative of a large cerebellopontine angle tumor compressing the cerebellum. However, our patient shows that those findings can be observed in other lesions that may cause both vestibular imbalance and integration failure.Reference Venkateswaran, Gupta and Swaminathan 3 The spontaneous nystagmus from unilateral vestibular deficits has a linear slow phase, and usually follows Alexander’s law, which makes the nystagmus increase with gaze into the contralesional side. On the other hand, the nystagmus induced during ipsilesional gaze has decreasing slow phases and arises from injury to the neural integrator, which normally holds the eyes in the eccentric position. In our patient, right beating spontaneous and Bruns’ nystagmus may be ascribed to compression of the lower brainstem and cerebellum due to basilar invagination, which leads to vestibular imbalance with a lesser tone on the left side as well as integration failure. In addition the paroxysmal vertigo with unilateral tinnitus, triggered by neck extension, may suggest vulnerability of left vestibulocochlear nerve to stretching. Whereas unilateral peripheral vestibular lesion usually produces a positive head impulse response to the lesion side, our patient showed bilaterally decreased gains of the vestibulo-ocular reflex during head impulses in the presence of normal caloric responses. Especially when associated with other ocular motor abnormalities but normal caloric tests, decreased head impulse vestibulo-ocular reflex gains suggest central vestibular dysfunction. Similarly, bilateral vestibular deficits combined with gaze-evoked nystagmus have been found in strokes involving central vestibular structures.Reference Kim, Lee, Park, Choi and Kim 4 , Reference Park, Kim, Strupp and Zee 5 Our patient extended the etiology of Bruns’ nystagmus and bilateral vestibular deficits to platybasia and basilar invagination from osteogenesis imperfecta. Bruns’ nystagmus along with bilaterally impaired head impulse VORs can be useful clinical signs indicating dysfunction of both the cerebellum and the brainstem.
Disclosures
The authors have nothing to disclose.
Statement of Authorship
SHK and MRK contributed to analysis and interpretation of the data and drafting of the manuscript. HJK. contributed to technical support. JSK contributed to the design of the study and critical revision of the manuscript.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/cjn.2016.453


