



The Canadian population has experienced an unprecedented aging trend with an increased longevity. In 2014, approximately 6 million Canadians were aged 65 or older, and the older adult population is expected to reach 9.5 million by 2030 (Government of Canada, 2014). Promoting and maintaining mental health is a top priority in achieving healthy and quality aging. Similar to other age groups, older adult populations are vulnerable to stressful life events and psychological distress, such as functional impairment and bereavement (Chao, Reference Chao2014; Feng et al., Reference Feng, Ji and Xu2014). Overlooking late-life mental health status may lead to serious health ramifications, such as increased risk of developing mental health disorders (Chao, Reference Chao2014) and mortality (Imaeva et al., Reference Imaeva, Shalnova, Kapustina, Balanova and Shkolnikov2021). In 2017, roughly 14 per cent of Canadian older adults experienced mental health problems, such as depression and anxiety (Canadian Institute for Health Information, 2017). Thus, having adequate, effective prevention and intervention programs is necessary to benefit late-life mental health and the health care system.
Recent research efforts have underscored the protective role of age-friendly residential environments, mostly the community environment, in late-life mental health. In this study, the residential environment is defined as individuals’ home and neighbourhood environments. However, little research has taken a holistic approach to understanding how the home environment, in addition to the community, may predict late-life mental health. Furthermore, there has been a lack of attention on how the mental health of older adults with differential gender and educational backgrounds may be associated with their residential environments. Hence, this study aimed to understand the relationships between two important dimensions of residential environments, home and community, and self-rated mental health (SRMH) among community-dwelling Canadian older adults and how the relationships vary by education and gender.
Residential environments and mental health
In response to older adults’ increasing preference for aging in place (Lewis & Buffel, Reference Lewis and Buffel2020), age-friendly residential environments play a critical role in improving the mental health of older adults (World Health Organization, 2007). Growing research has examined the direct relationship between residential environments and mental health status among older adults. Because SRMH could be conceptualized as a proxy for various types of mental health outcomes, this literature review was conducted using the following keywords: mental health, psychological well-being, depression, loneliness, and anxiety.
In terms of the home environment, dissatisfaction with the structure and conditions of personal residences may be a stressor to mental health, because older adult populations often spend more time in their residential environments than other age groups (Spalt et al., Reference Spalt, Curl, Allen, Cohen, Adar, Stukovsky, Avol, Castro-Diehl, Nunn, Mancera-Cuevas and Kaufman2016). Qiu et al. (Reference Qiu, Li, Li and Xu2020) found an inverse association between dwelling size and late-life depression; dwelling size may be a proxy for socioeconomic status, such as income and social status, an important predictor of mental health. Moreover, living in limited dwelling space may indicate problems of perceived overcrowding and inadequate personal space, especially for those living with others, which can hinder the development of physical and emotional spaces for socially supportive relationships and intensify the level of psychological distress (Firdaus, Reference Firdaus2017).
A similar rationale could also be applied to understanding the effect of residing in low-income housing. Older residents living in poorly maintained residences due to limited financial resources may experience greater risks to their mental health (Howden-Chapman et al., Reference Howden-Chapman, Chandola, Stafford and Marmot2011). Similarly, living in substandard dwelling conditions could be associated with a reduced sense of home attachment and more psychological distress (Howden-Chapman et al., Reference Howden-Chapman, Chandola, Stafford and Marmot2011; Phillips et al., Reference Phillips, Siu, Yeh and Cheng2005). Furthermore, residents in low-income housing often have little control over their property maintenance and repairs because the responsibility lies primarily with the government authority or a nongovernmental organization’s management office (Holding et al., Reference Holding, Blank, Crowder, Ferrari and Goyder2020), leading to greater feelings of frustration and loss of control.
Comparatively speaking, much more scholarly attention has been paid to understanding the effect of the community environment. For example, having a negative perception of the neighbourhood design could be a stressor that affects older adults’ mental health status (Toma et al., Reference Toma, Hamer and Shankar2015). Residing in an unsatisfying neighbourhood is associated with more daily hassles that potentially lead to psychological distress and poor mental health (Leslie & Cerin, Reference Leslie and Cerin2008). The availability of local community services and social resources is another important factor; attending neighbourhood senior centres is associated with better mental health among older adults (Sun & Lyu, Reference Sun and Lyu2020). Having access to community resources also promotes social support, social and human capital (Chao et al., Reference Chao, Katigbak, Zhang and Dong2018), and opportunities for volunteering and physical activities (Wang et al., Reference Wang, Li, Gao and Fu2021). Similarly, the availability and accessibility of mental health services are closely correlated with older adults’ willingness to seek help and help-seeking behaviour (Polacsek et al., Reference Polacsek, Boardman and McCann2019).
In addition, previous studies have identified significant relationships between community safety and mental health status among older adults, particularly in terms of depression (Barnett et al., Reference Barnett, Zhang, Johnston and Cerin2018; Choi & Matz-Costa, Reference Choi and Matz-Costa2018). Feeling insecure and unsafe may jeopardize older adults’ mental health, because an unsafe community may discourage individuals from engaging in meaningful social interactions with neighbours or enjoying physical activities in communal areas (Roh et al., Reference Roh, Jang, Chiriboga, Kwag, Cho and Bernstein2011). Furthermore, lacking a strong sense of belonging to the community may present a major risk to their psychological and subjective well-being (Guo et al., Reference Guo, Liu, Lu, Chan, Chui and Lum2021), mental health (Young et al., Reference Young, Russell and Powers2004), and life satisfaction (Au et al., Reference Au, Lai, Yip, Chan, Lai, Chaudhury, Scharlach and Leeson2020). Overall, although existing studies have highlighted the important link between residential environments and late-life mental health, significantly less attention has been given to the home environment.
Education and gender differences in mental health
The associations between residential environments and late-life mental health are heterogeneous among individuals with different gender and educational backgrounds. For example, research has indicated that older women, compared to men, are more likely to encounter mental health problems (Sialino et al., Reference Sialino, van Oostrom, Wijnhoven, Picavet, Verschuren, Visser and Schaap2021), such as depression, loneliness (Carmel, Reference Carmel2019; Chen et al., Reference Chen, Simon and Dong2014), and anxiety (Sialino et al., Reference Sialino, van Oostrom, Wijnhoven, Picavet, Verschuren, Visser and Schaap2021). Particularly, older women’s mental health may be associated with accumulative socioeconomic disadvantages (Sialino et al., Reference Sialino, van Oostrom, Wijnhoven, Picavet, Verschuren, Visser and Schaap2021), such as lower income (Chen et al., Reference Chen, Simon and Dong2014) and lower levels of early-life education (Matud et al., Reference Matud, Bethencourth, Ibáñez and Fortes2020). Sociologically speaking, older women may also continue their caregiving roles with family members, causing caregiving strain and burdens that can endanger their mental health (Carmel, Reference Carmel2019).
In terms of educational differences, previous studies have established a robust relationship between early-life education and late-life mental health, though the findings were inconclusive. On the one hand, older adults who obtained higher levels of education may have better mental health due to more human and social capital and better access to health care services and information (Lee, Reference Lee2011). On the other hand, those with higher levels of education may experience more psychological distress due to higher life expectations after retirement (Belo et al., Reference Belo, Navarro-Pardo, Pocinho, Carrana and Margarido2020). Nevertheless, the literature has established a reasonable foundation to hypothesize that the relationship of home and neighbourhood environments with late-life SRMH significantly varies by education and gender.
Theoretical framework
The design of this study was guided by stress process theory and the socioecological method. Stress process theory emphasizes the effects of multilevel exposure to stress on the psychological well-being and health of individuals, particularly in terms of mental health (Cho, Reference Cho2022; Pearlin et al., Reference Pearlin, Menaghan, Lieberman and Mullan1981). Early stages of the theory focused on the assumption that greater exposure to life adversity and other individual-level stressors contribute to accumulating stress and worsening mental health outcomes (Pearlin et al., Reference Pearlin, Menaghan, Lieberman and Mullan1981). Aneshensel (Reference Aneshensel, Avison, Aneshensel, Schieman and Wheaton2010) expanded the theory and examined the contextual effect of environmental stressors on mental health. This theory has been used as a theoretical framework in recent literature to study the associations between environmental stressors and mental health (Gilster, Reference Gilster2014; Wang et al., Reference Wang, Chen, Shen and Morrow-Howell2018). In addition to direct effects, the theory also pays attention to the moderating and mediating mechanisms by which psychological resources (e.g. social support and coping resources) and individual factors (e.g. age, health status, financial conditions, living arrangement, gender, and education) may alter the association between environmental stress exposure and mental health (Gilster, Reference Gilster2014; Pearlin et al., Reference Pearlin, Menaghan, Lieberman and Mullan1981). Additionally, the socioecological model highlights the impact of interactions with surrounding environments, such as home and community, on health and social behaviours. The model focuses on understanding the intertwined relationships of multilevel factors among people, social relationships, and environments with late-life health (Bengston & Settersten, Reference Bengtson and Settersten2016). This study considered microsystem (a person’s sociodemographic characteristics, self-rated health, and life satisfaction) and mesosystem (satisfaction with and feelings towards home and community) factors. This classification is similar in stress process theory, which categorizes stressors and coping resources at the individual level, defined by a person’s characteristics that directly influence SRMH, and at the contextual level, defined by their interaction with and exposure to contextual environments (e.g. home and community). Following theoretical guidelines, this study aimed to understand the direct associations between residential environmental factors – home and community – and SRMH for Canadian older adults and how education and gender may moderate these associations.
Methods
Data were from the 2018 Canadian Housing Survey, the first wave of a nationwide housing survey that collects data every 2 years to examine Canadian households’ housing needs, dwelling characteristics, socioeconomic status, health, perceptions of and satisfaction with neighbourhood services, social interaction with the community, and homelessness (Statistics Canada, 2021). From November 2018 to March 2019, the survey assessed a sample of 126,465 dwellings across 10 provinces and three territories, with a two-step sampling design. This study featured a national sample of 16,304 community-dwelling Canadians aged 65 or older (2,686 men with high school education; 5,003 women with a high school education; 2,254 men with some college education; 2,949 women with some college education; 1,906 men with a university education; and 1,506 women with a university education). Given missing data in the Northwest Territories, 304 respondents in these areas were excluded in this study.
Measures
The outcome variable, SRMH, was a single-item measurement. Respondents evaluated their overall mental health status on a 5-point scale (from 1 = poor to 5 = excellent). This measurement has been popularly adopted in population health research as a proxy of overall mental health status; the self-reporting mechanism can capture important information pertaining to different aspects of physical and mental health (Jang et al., Reference Jang, Park, Kim, Kwag, Roh and Chiriboga2012; Kim et al., Reference Kim, DeCoster, Chiriboga, Jang, Allen and Parmelee2011).
Two levels of key independent variables were used to indicate residential environmental factors: home and community environments. Home environmental characteristics included variables directly related to the evaluation of or satisfaction with respondents’ home environment. Dwelling size indicated the number of rooms as a proxy for the physical size of respondents’ dwellings; higher scores denoted larger dwellings. A dichotomous variable, living in low-income housing, was used to indicate whether respondents resided in social or affordable housing (0 = no; 1 = yes). Another dichotomous variable, needed home maintenance, was measured based on respondents’ perceptions of whether any minor or major repair was needed in their home (0 = no; 1 = yes). Satisfaction with dwelling design was a composite score that measured the average of respondents’ satisfaction with five home conditions with a 4-point scale (from 1 = very dissatisfied to 4 = very satisfied): safety, accessibility, energy efficiency, temperature during summer and winter, and soundproofing (Cronbach’s α = .82). The composite score was generated by principal component analysis; factor loadings of .30 or higher were used as the threshold. Inhabitable conditions were another single-item measure that indicated whether a respondent experienced any of the following conditions at home: mould or mildew, pests, undrinkable water, and poor indoor air quality (0 = no; 1 = yes).
Community environmental characteristics refer to variables that measured respondents’ perception of and feeling towards their community environment. Satisfaction with the neighbourhood was a single-item variable that evaluated respondents’ satisfaction with their neighbourhood on a 4-point scale (from 1 = very dissatisfied to 4 = very satisfied). Community service need measured if respondents expressed any need for community support services for their daily activities (0 = no; 1 = yes). Community safety was assessed based on the respondents’ perception of safety when walking alone at night (from 1 = very unsafe to 4 = very safe). Sense of belonging evaluated respondents’ satisfaction with being a part of their community on a 9-point scale (1 = very dissatisfied to 9 = very satisfied).
Based on the literature, the following sociodemographic and health factors were adjusted in regressions as covariates: age (65–85), self-rated health (a proxy of health status on a 5-point scale), life satisfaction (a proxy of psychological well-being on a 9-point scale), economic hardship (a proxy of income and financial status; if respondents asked for financial help from family and friends, took on debts, sold assets, or turned to charity for help; 0 = no; 1 = yes), living alone (a proxy of social isolation; 0 = no; 1 = yes), and civic engagement (a proxy of social participation; 0 = no; 1 = yes; Cheung & Mui, Reference Cheung and Mui2023). Two moderating variables were also included: education (1 = high school or less; 2 = some college; 3 = university) and gender (0 = men; 1 = women).
Analysis
Weighted descriptive statistics were calculated to describe the covariates and home and community environmental factors for the whole sample and each education-by-gender group. To offer a comprehensive knowledge of within-group differences between older men and women by educational background, multiple comparisons with Bonferroni’s corrections were implemented: high school, some college, and university degree or higher. A p-value less than .05 was considered statistically significant. Prior to running regressions, an intraclass correlation coefficient of the null model was tested to estimate the level of variability in SRMH between communities. The intraclass correlation coefficient in this study was .017, indicating weak variability by cluster. In other words, only 1.7 per cent of the variance in SRMH was due to between-community differences. Due to the low coefficient and fewer than five respondents in most communities (Settels & Leist, Reference Settels and Leist2021), multilevel regressions may be inappropriate.
Instead, this study conducted hierarchical linear regression analyses. Model 1 included the following covariates only: age, self-rated health, life satisfaction, economic hardship, living alone, and civic engagement. Home (Model 2) and community (Model 3) environmental factors were then added to the model separately. Model 4 included both sets of environmental factors to better understand whether they remained statistically significant alongside each other. In Model 5, education and gender were added to estimate whether these two moderating variables significantly predicted SRMH, after controlling for covariates and environmental factors. This analytic approach determined the extent to which each set of variables in home and community environments explained SRMH and the potential moderating effects of education and gender. In the last model (Model 6), interaction terms (gender-by-education) were added to verify whether SRMH was stratified by education and gender. If any interaction terms were statistically significant, separate regression analyses were implemented for each subgroup (education-by-gender) to identify significant group-specific environmental predictors of SRMH.
Results
Descriptive statistics
Table 1 suggests significant gender differences in covariates and home and community environmental variables across educational groups. Older men who received a university education reported better SRMH (M = 4.03, standard deviation (SD = 0.89) than other groups. Significant gender differences in SRMH emerged for those with a high school education or less (p < .001), with men reporting better scores (M = 3.70, SD = 0.96) than women (M = 3.65, SD = 0.95). In terms of home environment, across groups, older men tended to live in larger dwellings than women (p < .001). Also, compared to men, more women with a high school (10.15% vs. 5.53%, respectively; p < .001) or some college education (5.56% vs. 2.82%; p < .001) lived in low-income housing. For neighbourhood environmental factors, overall older women reported feeling less safe in their communities, compared to men (p < .001). A more significant difference was observed in the group of high school education or less (men: M = 2.92, SD = 1.08; women: M = 1.92, SD = 1.14; p < .001).
Table 1. Weighted descriptive statistics of study variables by stratified samples (n = 16,304)

Note: Multiple comparisons with Bonferroni’s correction were implemented to examine the significance of differences between groups of older men and women by educational background: high school or less, some college, and university or higher. A p-value less than.05 was considered statistically significant. Covariates included age, self-rated health, life satisfaction, economic hardship, living alone, and civic engagement.
Hierarchical linear regressions
Multiple linear regressions were first conducted (see Table 2). Model 1 suggested that self-rated health (b = 0.37, standard error (SE) = 0.01, p < .001), life satisfaction (b = 0.11, SE = 0.00, p < .001), economic hardship (b = −0.03, SE = 0.01, p < .001), and living alone (b = −0.06, SE = 0.01, p < .001) were significant predictors of SRMH. Home and community environmental factors were added to the base model separately. Model 2 showed that after adjusting for covariates, dwelling size (b = 0.03, SE = 0.01, p < .001), living in low-income housing (b = −0.06, SE = 0.02, p = .002), satisfaction with dwelling design (b = 0.04, SE = 0.00, p < .001), and uninhabitable conditions (b = 0.02, SE = 0.00, p = .012) significantly predicted SRMH. Model 3 showed that all community factors were statistically significantly associated with SRMH: satisfaction with neighbourhood (b = 0.07, SE = 0.01, p < .001), community service need (b = −0.08, SE = 0.02, p < .001), community safety (b = 0.03, SE = 0.00, p < .001), and sense of belonging (b = 0.03, SE = 0.01, p < .001). Model 4 suggested that the two sets of environmental factors remained statistically significant even after controlling for each other. The coefficients of environmental factors only reduced slightly, which may suggest that all environmental factors uniquely contributed to explaining SRMH.
Table 2. Hierarchical analysis of SRMH for the total sample
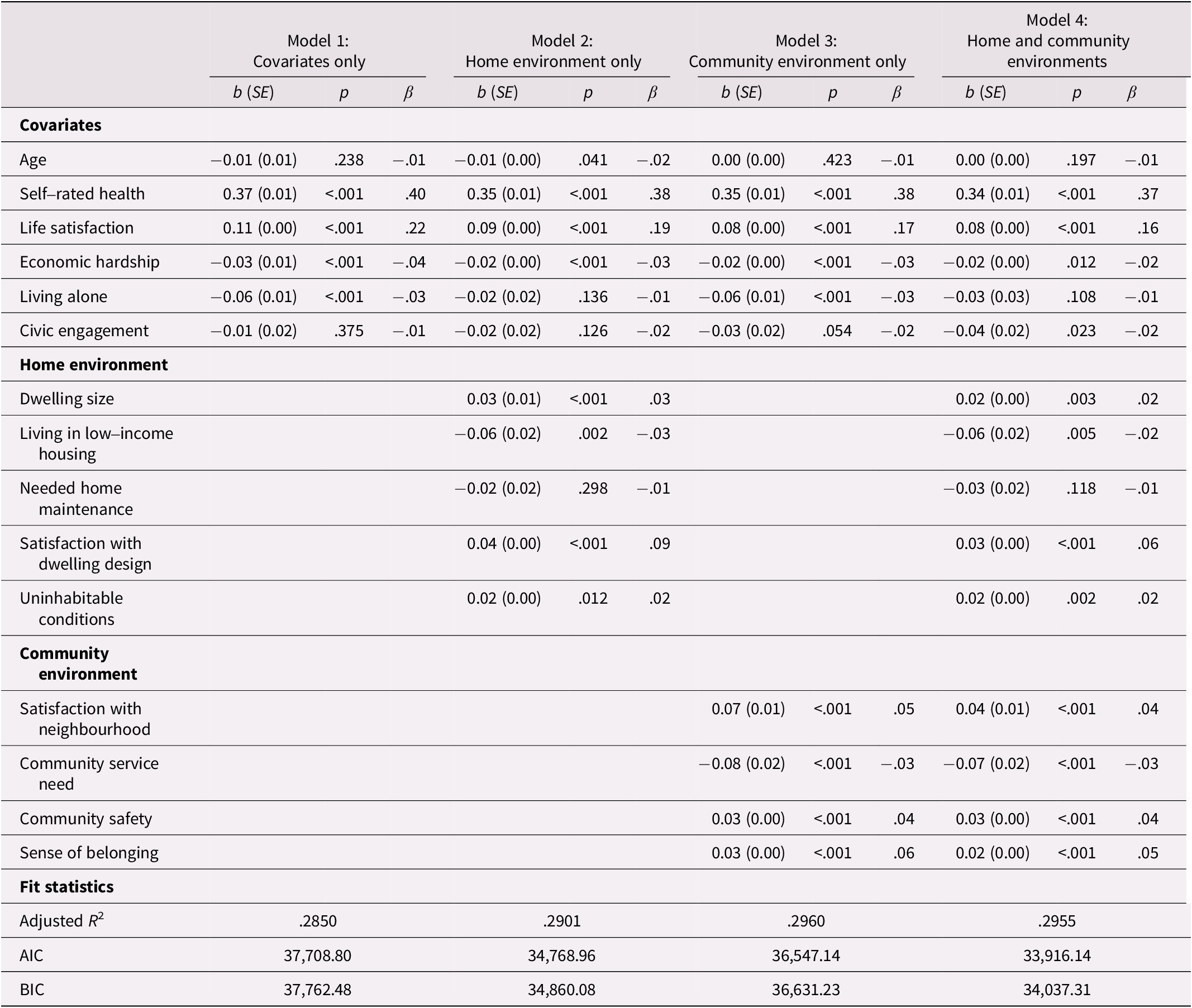
Note. b, unstandardized coefficient; SE, standard error; β, standardized coefficient; AIC, Akaike information criterion; BIC, Bayesian information criterion.
In Model 5, gender and education were added to the model, and both variables were statistically significant predictors of SRMH (see Table 3). Model 6 revealed that an interaction term was statistically significant (women × university; b = −0.08, SE = 0.04, p = .017), suggesting a significant interaction effect of gender and education on the associations between environmental factors and SRMH. In other words, the significant interaction effect justified the need for between-group analyses to further identify group-specific predictors of SRMH.
Table 3. Interactive effects of gender and education on SRMH for the total sample

Note. b, unstandardized coefficient; SE, standard error; β, standardized coefficient; AIC, Akaike information criterion.
BIC, Bayesian information criterion.
Between-group regressions
As shown in Tables 4 and 5, regression results suggested that of the home environmental factors, dwelling size was uniquely associated with SRMH for women with a high school education or less (b = 0.04, SE = 0.02, p = .012). Satisfaction with dwelling design was positively associated with SRMH across all groups, except for women with some college education. Uninhabitable conditions were a unique predictor of SRMH for men (b = 0.04, SE = 0.02, p = .002) and women (b = 0.04, SE = 0.01, p = .004) with some college education. Regarding community environment, satisfaction with the neighbourhood was positively associated with SRMH among women with higher school education or less (b = 0.08, SE = 0.02, p < .001) or some college education (b = 0.07, SE = 0.02, p = .004). Additionally, community service need was a common predictor of SRMH among women with a high school degree or less (b = −0.08, SE = 0.03, p = .010) and men who had completed some college (b = −0.12, SE = 0.04, p = .007) or a university degree (b = −0.10, SE = 0.05, p = .039). Community safety was a significant predictor for men with some college education (b = 0.05, SE = 0.02, p = .035) and women with a university education (b = 0.05, SE = 0.02, p = .011). Last, sense of belonging was a common predictor of SRMH among men and women who completed some college education or less.
Table 4. Regression models for SRMH by education and gender

Note. b, unstandardized coefficient. SE, standard error; β, standardized coefficient; AIC, Akaike information criterion; BIC, Bayesian information criterion.
Table 5. Regression models for SRMH by education and gender (cont’d)

Note. b, unstandardized coefficient; SE, standard error; β, standardized coefficient.
AIC, Akaike information criterion; BIC, Bayesian information criterion.
Discussion
Using a nationally representative sample of Canadian older adults, this study provided an empirical understanding of significant associations between SRMH and home and community environmental factors and, more precisely, how gender and education moderated these associations. The following section discusses home and community environmental predictors of SRMH for each education and gender group.
In terms of home environment, group-level regression results indicated that dwelling size was positively related to SRMH among women with a high school education. Living in homes with inadequate space may be a source of psychological distress for older residents, leading to poor mental health (Qiu et al., Reference Qiu, Li, Li and Xu2020). This result may be particularly true for women who live in intergenerational households because crowded living environments may jeopardize family relationships, exacerbating the risk of poor SRMH. Also, this might explain why dwelling size was a significant predictor only for this group, because descriptive statistics indicated that older women with a high school education or less had the smallest living spaces across all groups. This finding indicates the need for mental health services tailored to this group of older adults such as stress management, cognitive behavioural therapy, or creative space management of their homes. Future housing policy should also be mindful of the potential effect of dwelling size on the SRMH of older residents, especially women with fewer socioeconomic resources, when providing design guidelines for low-income, age-friendly housing.
Satisfaction with dwelling design was positively associated with SRMH across all groups, with one exception: older women with some college education. The results align with the literature that feeling dissatisfied with the home environment has a negative impact on mental health (Phillips et al., Reference Phillips, Siu, Yeh and Cheng2005). Housing designers and developers, especially for senior housing projects, could consider consulting with or involving older residents throughout the housing design and modification process. This could be an empowering and engaging process that could improve the mental health of potential residents. Yet it remains unclear why this predictor was not statistically significant for women with some college education; more research is warranted. Another significant predictor in the home environment was residing in a home with uninhabitable conditions, which was related to better SRMH among older adults with some college education only. This result is very intriguing because the direction of the relationship was opposite to what the literature has suggested. One possible explanation is that this specific educational group of older adults may have greater tolerance and better coping strategies regarding uninhabitable conditions than other groups; however, more research is needed to unpack this relationship.
Regarding community environmental predictors, the data indicated that greater satisfaction with the neighbourhood was significantly associated with better SRMH among older women with high school or some college education. The direction of this association corresponds to prior studies that suggested feeling satisfied with the community diminishes the impact of daily hassles and protects mental health (Leslie & Cerin, Reference Leslie and Cerin2008). In terms of between-group differences, older women with high school or some college education may engage in their communities more often when they feel satisfied, thereby reaping more psychological benefits. If this is a reciprocal relationship, older women in these groups may be more willing to engage in their communities when they have more psychological resources, meaning better SRMH, thus providing them with greater satisfaction with their communities. This result seems to suggest the reciprocal impact of neighbourhood quality on the SRMH of older residents. Well-designed social programs for these women may improve their community satisfaction and mental health.
Additionally, higher community service needs uniquely predicted lower levels of SRMH for women with high school education or less and men with some college or university education. This unmet service need may generate feelings of helplessness and frustration, putting their SRMH at greater risk. The effect of unmet service needs was greater for men, possibly indicating that older men generally may be less likely to seek professional help when needed. This may be due to gender role socialization such that older men may feel the need to show resilience and strength to assert their masculinity; thus, their mental health may be at greater risk when experiencing an unmet need. Regardless, the results point to the need to design appropriate and accessible outreach mental health programs for older adults in these groups.
Moreover, community safety was positively associated with SRMH for men with some college education and women with a university education. This is consistent with the literature, indicating that the feeling of insecurity may disincentivize older adults from physical and social activities in their communities and that the lack of meaningful interaction may place their mental health at risk (Barnett et al., Reference Barnett, Zhang, Johnston and Cerin2018; Choi & Matz-Costa, Reference Choi and Matz-Costa2018). Overall, results suggest the need for community safety programs that improve the SRMH of older residents, particularly for men with some college education and women with a university education.
SRMH was positively associated with the sense of belonging among older adults who received high school or some college education, regardless of gender. The sense of belonging to the community may reflect an individual’s psychological need for close connections to familiar people and places. A greater sense of belonging may facilitate meaningful social engagement and interaction among neighbours, improving the mental health of these older adults. Interestingly, this result did not apply to participants with a university education. Perhaps older individuals with higher education may be more established and feel more attached to their professional community, rather than their local community. This result underscores the importance of community-based interventions to cultivate a sense of belonging to improve SRMH for older adults with relatively lower levels of education.
Furthermore, it is interesting to note that multiple environmental variables were significantly associated with SRMH, even after controlling for the experience of economic hardship, which contrasts with some prior studies (Howden-Chapman et al., Reference Howden-Chapman, Chandola, Stafford and Marmot2011; Qiu et al., Reference Qiu, Li, Li and Xu2020). Two possible reasons could explain these discrepancies. The first may be related to differences in sampling. Prior studies have investigated the mental health of older adult populations in other countries, such as China (Qiu et al., Reference Qiu, Li, Li and Xu2020) and the United Kingdom (Howden-Chapman et al., Reference Howden-Chapman, Chandola, Stafford and Marmot2011), whereas this study focused on the Canadian population. Similarly, a previous study paid particular attention to a specific group of British civil servants (Howden-Chapman et al., Reference Howden-Chapman, Chandola, Stafford and Marmot2011), who typically have higher levels of education. In contrast, this study explored the well-being of the general Canadian population, irrespective of income, occupation, and education. These sampling variations in the literature may suggest potential cultural and national discrepancies in older adults’ susceptibility to varying socioeconomic resources and their interactions with and expectations of their environments, contributing to differential influences on mental health. Second, the discrepancies may be due to differences in measuring economic hardship. This study adopted three questions (i.e. whether respondents sought financial assistance from family and friends, sought charity, or took on debts or sold assets). In contrast, other studies employed a single measure of economic hardship, such as difficulty paying bills (Howden-Chapman et al., Reference Howden-Chapman, Chandola, Stafford and Marmot2011) or per capita household income (Qiu et al., Reference Qiu, Li, Li and Xu2020) – information not available in the original dataset of this study. This measurement difference may have contributed to the varying role of socioeconomic status in the relationships between home and neighbourhood environment variables and SRMH.
To conclude, the findings provide insights into potential environmental interventions in terms of urban design and social programs to create a supportive environment that promotes late-life mental health. However, this study has several limitations. First, because the Canadian Housing Survey is a cross-sectional survey, it was difficult to determine any statistical causation. Second, most environmental predictors in the survey were subjective assessments of older adults’ residential environments, which may be subject to self-reporting bias. Third, because the sample size in this study was relatively large, there could be statistically significant differences in certain results despite the lack of meaningful associations. It is necessary to interpret these study findings with additional caution. Last, SRMH, as a self-reported, one-item global measure, did not capture information on specific mental health problems or disorders, such as depression and anxiety. Future studies could consider collecting primary data and investigating the role of objectively measured home and environmental predictors in explaining clinically diagnosed mental health problems among Canadian older adults.
Acknowledgements
The author is grateful to Professor Ada C. Mui at Columbia University for her guidance and support in this manuscript. Also, the author appreciates Statistics Canada for making the data available. All opinions expressed in this manuscript are those of the author and should not be attributed to Statistics Canada.
Financial support
No funding was received for conducting this study.
Competing interest
The author has no relevant financial or non-financial interests to disclose.





