


Attention-deficit hyperactivity disorder (ADHD) is a childhood-onset neurodevelopmental condition, with symptoms persisting into adulthood in approximately 50% of individuals.Reference Wilens, Faraone and Biederman 1 As most of the research is done with children, the role of personality traits – in particular impulsivity, reward sensitivity and sensation seeking – in the psychopathology of the ADHD phenotype is not well understood in adults with ADHD. It is unclear whether these personality traits are predisposing risk factors for the disorder or are aspects of the clinical phenotype of ADHD.
Preliminary evidence on trait impulsivity in adults diagnosed with ADHD shows that they have significantly higher levels of impulsive traits on the Barratt Impulsiveness Scale (BIS-11) when compared with healthy controls.Reference Malloy-Diniz, Fuentes, Leite, Correa and Bechara 2 Rodriguez-Jimenez and his team found similar results; pathological gamblers with a childhood history of ADHD had significantly greater impulsive traits on the BIS-11 than controls.Reference Rodriguez-Jimenez, Avila, Jimenez-Arriero, Ponce, Monasor and Jimenez 3 Similar results have been found using other measures. On neuroticism, which also includes impulsive traits, adults with ADHD scored significantly higher than controls.Reference Salgado, Bau, Grevet, Fischer, Victor and Kalil 4 , Reference Lopresti, Maes, Meddens, Maker, Arnoldussen and Drummond 5
ADHD is claimed to be in part the results of both low sensitivity to negative feedback and punishment, and higher sensitivity to reward,Reference Luman, Oosterlaan and Sergeant 6 though further research shows some doubts on this claim.Reference Luman, van Meel, Oosterlaan and Geurts 7 Other studies using measures such as the Sensitivity to Punishment and Sensitivity to Reward Questionnaire (SPSRQ) demonstrate low sensitivity to punishment yet not necessarily oversensitivity to reward, which instead is thought to be predictive of ADHD with comorbid conduct disorder.Reference Matthys, van Goozen, de Vries, Cohen-Kettenis and van Engeland 8 Sensation seeking defined as ‘a need for varied, novel, and complex sensations and experiences and the willingness to take physical and social risks for the sake of such experiences’ is thought to be a predisposing risk factor for externalising behavioural problems such as those seen in ADHD.Reference Handley, Chassin, Haller, Bountress, Dandreaux and Beltran 9 However, studies using measures of sensation seeking such as the Sensation Seeking Scale form-V, SSS-V, have shown that children with ADHD did not differ from controls.Reference Blaskey, Harris and Nigg 10 In a study using a multidimensional rating scale, adults with ADHD scored higher on a measure of sensation seeking; however, the presence of personality disorders might have had a role in explaining the results.Reference Lopresti, Maes, Meddens, Maker, Arnoldussen and Drummond 5
ADHD runs in families and relatives of individuals with ADHD show two- to eightfold increased risk of developing ADHD compared with controls.Reference Biederman 11 According to the endophenotype model,Reference Almasy and Blangero 12 , Reference Gottesman and Gould 13 also encompassing the concept of predisposing risk factors,Reference Braff, Freedman, Schork and Gottesman 14 if impulsivity traits, sensation seeking, and sensitivity to punishment and reward are predisposing factors for developing ADHD, high levels of these traits would be observed not only in individuals with ADHD but also in their biological first-degree relatives who do not have a diagnosis of ADHD. On the contrary, if measured personality traits in adults are only associated with ADHD diagnosis but are not seen in relatives or controls to the same extent, such traits will more likely be part of, or overlap with, the clinical phenotype of ADHD, rather than being predisposing factors. To test these two competing hypotheses, we compared personality traits of impulsivity, sensation seeking, and sensitivity to punishment and reward using three standardised questionnaires in 20 adults with ADHD, 20 unaffected biological first-degree relatives and 20 typically developing controls.
Method
Participants
Twenty ADHD patients, 20 unaffected first-degree relatives (siblings and parents) of ADHD patients and 20 typically developing participants matched for age were included in this study. Participants were recruited over a period of 12 months and written consent was obtained in person from all participants. The study was approved by the Cambridgeshire 3 Research Ethics Committee (REC: 09/H0306/38). ADHD proband–relative pairs were recruited from the Adult ADHD Research Clinic, Addenbrooke's Hospital, Department of Psychiatry, University of Cambridge. Patients received a diagnosis of ADHD according to DSM-IV-TR, 15 based on a full clinical interview with the patient and an informant who had known the patient since childhood. The clinical assessment also included rating scales: Barkley Adult ADHD Rating Scale, self-report and informant report, childhood and adulthood symptoms,Reference Barkley and Murphy 16 assessing childhood and adulthood symptoms from the perspective of the patient and the informant. Eligible patients were asked to contact a first-degree relative who undertook the same clinical protocol to screen for undiagnosed ADHD. Control participants were recruited via posters in the local community and underwent the same screening procedure.
On the testing day, all participants were interviewed using the Mini-International Neuropsychiatric InventoryReference Sheehan, Lecrubier, Sheehan, Amorim, Janavs and Weiller 17 to screen for DSM-IV Axis I disorders and completed the Barkley Adult ADHD Rating Scale and self-report.Reference Barkley and Murphy 16 Estimate of full IQ was obtained using the National Adult Reading Test.Reference Nelson and O'Connell 18 Neither controls nor first-degree relatives of ADHD probands showed ADHD symptoms meeting the DSM-IV-TR diagnostic threshold for ADHD. Moreover, they did not show clinically significant symptoms of another DSM-IV-TR disorder. Finally, ADHD participants did not have relevant symptoms of a comorbid disorder reaching clinical significance for a formal DSM-IV-TR diagnosis. To reduce confounds resulting from other major psychiatric and neurological conditions, exclusion criteria were as follows: (a) full IQ ≤90; (b) current or past history of pervasive developmental disorder, any neurological disorder (including tic disorders), bipolar disorder, substance-use disorders, schizophrenia or other psychotic disorders; and (c) current major depressive disorder. To minimise the impact of psychotropic medications on outcomes, participants were asked to omit taking those 24 h before testingReference Gualtieri, Wargin, Kanoy, Patrick, Shen and Youngblood 19 and were asked to refrain from consuming alcohol or caffeine-containing drinks on the day of testing. The ADHD group comprised 16 patients with combined type and 4 with inattentive type; 16 of them were ordinarily medicated with methylphenidate, and 4 were not receiving medication for ADHD. None of the individuals had to be excluded because of a NART full IQ below 90.
All participants completed the BIS 11,Reference Patton, Stanford and Barratt 20 which measures trait impulsivity over three subscales: (1) attentional impulsiveness (inattention and cognitive instability), (2) motor impulsiveness (spontaneous actions) and (3) non-planning impulsiveness (lack of forethought); the SPSRQ,Reference Torrubia, Ávila, Moltó and Caseras 21 which consists of two orthogonal subscales: (1) sensitivity to punishment and (2) sensitivity to reward; and the Sensation Seeking Scale form-V (SSS-V),Reference Zuckerman 22 which consists of four subscales: (1) thrill and adventure seeking (a desire to participate in dangerous activities), (2) experience seeking (search for new experiences in a nonconformist manner), (3) disinhibition (interest in socially and sexually disinhibited activities) and (4) boredom susceptibility (intolerance of routines and repetitiveness).
Data were analysed using the Statistical Package for Social Sciences, version 18 (SPSS, Inc., Chicago, Illinois). Univariate analysis of covariance models was fit to the BIS-11, SPSRQ and SSS-V total scores, whereas the subscales of these three instruments were analysed using separate multivariate analysis of covariance models. Age was included as covariate in all analyses. For post hoc comparisons, Bonferroni correction was applied. All tests were two-tailed and a significance level of 0.05 was assumed.
We also ran subsidiary analyses with gender and NART-estimated full IQ (full) as covariates to partial out the effect of full IQ on the outcome measures (personality traits). All effects remained unchanged.
Results
Demographic and clinical characteristics
The three groups did not differ in age. The ADHD group scored four points lower than typically developing controls on NART full IQ. ADHD participants differed from unaffected first-degree relatives and controls in self-reported current and childhood ADHD symptoms. Relatives were significantly different from ADHD and control groups on self-reported current hyperactive/impulsive symptoms, childhood total symptoms, childhood hyperactive/impulsive and inattentive symptoms (Table 1).
Table 1 Sample characteristics and clinical measures
| ADHD | Relatives | Controls | F (2,57) | P | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | s.d. | Mean | s.d. | Mean | s.d. | |||
| Age | 32.20 | 10.31 | 38.85 | 15.31 | 32.55 | 5.80 | 2.26 | 0.115 |
| Gender, % female | 15 | 50 | 35 | 5.55 | 0.062 a | |||
| NART full IQ | 115.26 | 6.15 | 116.59 | 5.28 | 119.49 | 3.27 | 3.68 | 0.031 b |
| BAARS current total symptoms | 36.15 | 12.39 | 10.00 | 7.38 | 5.20 | 4.29 | 73.50 | <0.001 b , c |
| BAARS current hyperactive/impulsive | 18.40 | 6.98 | 5.25 | 4.13 | 2.50 | 2.50 | 60.11 | <0.001 b , c , d |
| BAARS current inattentive symptoms | 17.75 | 5.96 | 4.75 | 3.89 | 2.70 | 2.77 | 68.44 | <0.001 b , c |
| BAARS childhood total symptoms | 41.35 | 11.93 | 14.20 | 10.28 | 4.85 | 6.65 | 73.78 | <0.001 b , c , d |
| BAARS childhood hyperactive/impulsive | 20.65 | 6.23 | 6.60 | 4.45 | 2.15 | 3.44 | 79.45 | <0.001 b , c , d |
| BAARS childhood inattentive symptoms | 20.70 | 6.04 | 7.60 | 6.23 | 2.70 | 4.07 | 56.57 | <0.001 b , c , d |
a χ 2.
b The ADHD group differs significantly from the controls.
c The ADHD group differs significantly from the relatives.
d Relatives differ significantly from controls.
Personality measures
Results showed that the three groups differed significantly on overall score of trait impulsivity [F(2, 56)=67.783, P<0.0001] and sensitivity to punishment/reward [F(2, 56)=10.513, P<0.0001]. No significant effect of group was found for sensation seeking [F(2, 56)=1.291, P=0.283]. Post hoc comparisons showed that the ADHD group was higher than relatives and controls on impulsivity and sensitivity to punishment/reward (BIS-11: ADHD v. Relatives P<0.001, ADHD v. Controls P<0.001; SPSRQ: ADHD v. Relatives P<0.007, ADHD v. Controls P<0.001). There were no differences between controls and relatives on the overall score and all subscales, for all three personality measures (Fig. 1).
For subscales of BIS-11, the ADHD group scored significantly higher than both relatives and controls on all three subscales (all P<0.0001), Fig. 2 panel A. On the SPSRQ subscales, group differences were significant on the sensitivity to reward subscale but not on the sensitivity to punishment subscale. The ADHD group was more sensitive to reward than both relatives (P=.003) and controls (P<0.001), Fig. 2 panel B. Although there were no differences between the three groups in the total sensation seeking score, comparisons on the four subscales revealed that the ADHD group scored higher on the boredom susceptibility subscale than relatives (P=0.006) and controls (P=0.016). No significant group differences were present for the remaining three subscales, Fig. 2 panel C.
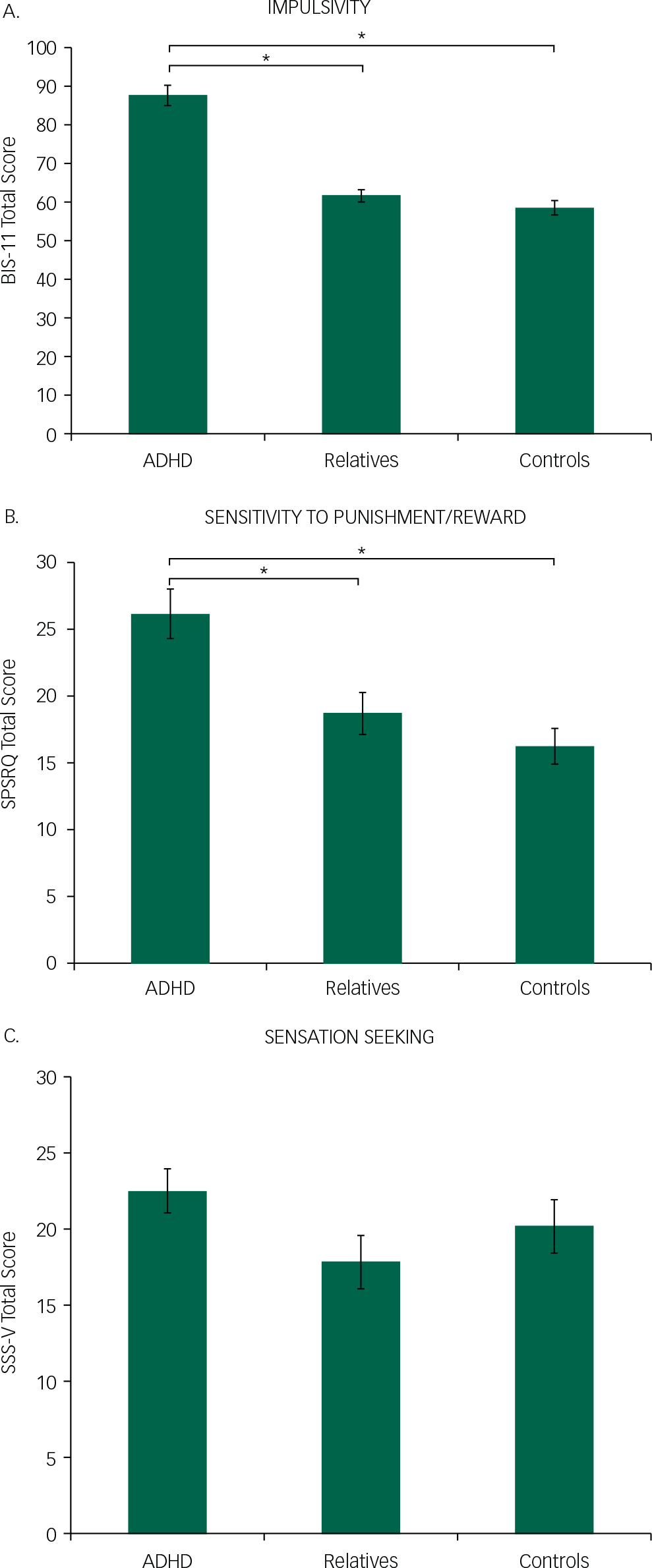
Fig. 1 Panel A: Overall impulsivity score according to BIS-11. Individuals with ADHD showed higher impulsivity than relatives and controls. Panel B: Sensitivity to reward and sensitivity to punishment overall score according to SPSRQ. The ADHD group scored significantly higher than relatives and controls. Panel C: Sensation seeking overall score according to SSS-V. *For significant differences. Bars represent standard error of the mean.
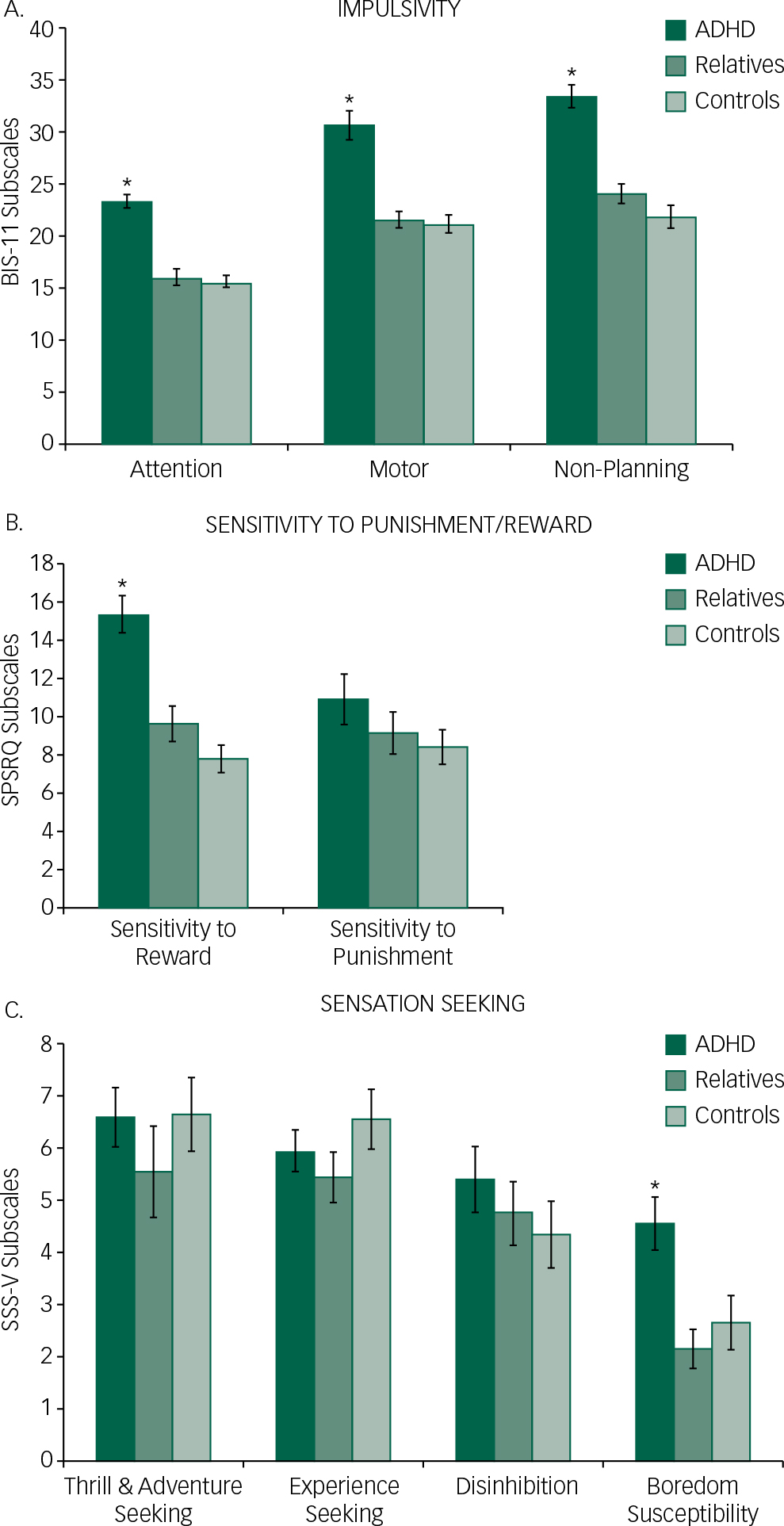
Fig. 2 Panel A: Impulsive traits according to BIS-11 subscales. Individuals with ADHD showed higher impulsive traits on all three subscales. Panel B: Sensitivity to reward and sensitivity to punishment. The ADHD group scored significantly higher than relatives and controls only on the SPSRQ Sensitivity to Reward subscale. Panel C: Sensation seeking subscales according to group. The ADHD group scores significantly higher than relatives and controls only on boredom susceptibility. *For significant differences. Bars represent standard error of the mean.
Discussion
The aim of this study was to test whether personality traits of impulsivity, sensitivity to punishment and reward, and sensation seeking were associated with adults with ADHD and to test whether these measured traits were aspects of the clinical phenotype or instead predisposing personality risk factors for ADHD. Our results suggest that high impulsivity traits, hypersensitivity to reward and susceptibility to boredom are part of the clinical phenotype of adults with ADHD, rather than personality traits harbouring an increased risk for the disorder, as unaffected first-degree relatives did not show a similar pattern of traits. Moreover, results also show that in this study adults with ADHD are not more indifferent to punishment or more sensation seekers than their relatives and controls. These results could not be explained by nonspecific confounds such as age since it was not statistically different between groups. A limitation of the study may be the difference in IQ between ADHD and control participants, but ADHD relatives did not differ from either controls or the ADHD group. Furthermore, all groups were within the same full IQ range of 111–120. When considering gender, whilst there were no statistically significant gender differences between groups, there was a trend. Increased trait impulsivity in adults with ADHD is characterised by higher impulsivity in all three components measured: motor, attentional and non-planning. This is consistent with previous research on trait impulsivity.Reference Malloy-Diniz, Fuentes, Leite, Correa and Bechara 2 Increased impulsive personality traits in our adult ADHD group might be the expression of self-regulation impairments linked to underlying brain mechanisms contributing to the pathophysiology of ADHD. It has been shown that high trait impulsivity is correlated with low D2/D3 autoreceptor availability in the substantia nigra/ventral tegmental area; specifically, individual differences in expression of impulsive traits are mediated by midbrain D2/D3 availability,Reference Reeves, Polling, Stokes, Lappin, Shotbolt and Mehta 23 and this effect is modulated through diminished inhibitory autoreceptor control over stimulated striatal dopamine release.Reference Buckholtz, Treadway, Cowan, Woodward, Li and Ansari 24 Our results might correspond to the speculation that impulsive traits in adult ADHD are associated with atypical dopaminergic neuronal projections from the midbrain to the ventral striatum, which are linked with the integration and modulation of motivation and reward processing,Reference Robbins and Everitt 25 particularly implicated in impulsive behaviour.Reference Cardinal, Winstanley, Robbins and Everitt 26 High score on trait impulsivity is also linked to reduced grey matter density and cortical thickness in regions related to the pathophysiology of ADHD, namely orbitofrontal cortex (OFC) and anterior cingulate.Reference Matsuo, Nicoletti, Nemoto, Hatch, Peluso and Nery 27 , Reference Schilling, Kuhn, Romanowski, Schubert, Kathmann and Gallinat 28 Specifically, small left OFC volume is linked to high motor impulsivity, and small right OFC volume is related to high non-planning impulsivity.Reference Matsuo, Nicoletti, Nemoto, Hatch, Peluso and Nery 27
Our results suggest that impulsive personality traits are associated with the clinical phenotype in adults with ADHD. Research also shows that, albeit partially overlapping, personality traits of impulsivity are to some extent different from hyperactive/impulsive behaviours measured by clinical scales. Self-report measures of trait impulsivity are constructed to grasp personality traits, which are shaped by internal and external developmental variables over extended period of time, and embed individual's subjective experience, therefore constituting a long-term pattern of behaviour; instead, clinical scales tend to measure symptoms within a relatively short and definite time frame.Reference Keilp, Sackeim and Mann 29 , Reference Moeller, Barratt, Dougherty, Schmitz and Swann 30 Moreover, further evidence shows that impulsive personality traits as measured by the BIS-11 are partially independent from other dimensions of impulsivity such as impulsive action and impulsive choice, and non-significant or low correlations between these dimensions are not uncommon.Reference Aichert, Wostmann, Costa, Macare, Wenig and Moller 31 – Reference Reynolds, Ortengren, Richards and de Wit 34 This is consistent with our results showing that unaffected first-degree relatives of ADHD participants presented with increased hyperactive/impulsive symptoms (but still significantly lower than ADHD participants) and comparable impulsive traits as controls. Along with previous evidence, our results support the hypothesis that impulsive personality traits and clinical symptoms of hyperactivity and impulsivity do not entirely overlap and that impulsive personality traits are a feature of the clinical phenotype of ADHD. Adding a measure of personality traits to a clinical diagnostic protocol for ADHD in adults might prove to be useful in order to improve diagnostic sensitivity. Future research might address these hypotheses.
When measuring sensitivity to reward and sensitivity to punishment using the SPSRQ scale, results showed that the ADHD group was more sensitive to reward than relatives and controls. However, their self-reported sensitivities were not different from relatives or controls. Theoretically, the sensitivity to reward and sensitivity to punishment subscales are linked to two different but collaborative subsystems that modulate behaviour, the behavioural activation system (BAS) and the behavioural inhibition system (BIS). The neural underpinnings of BAS have been suggested to involve ventral and dorsal striatum, and ventro-medial prefrontal cortex, modulated by dopamine; these are known to be associated with ADHD. The BIS has instead been shown to involve the amygdala.Reference Kennis, Rademaker and Geuze 35 It is then possible to postulate that the heightened sensitivity to reward might be related to atypical functioning of the ventral/dorsal striatum and ventro-medial prefrontal cortex, as well as their dopaminergic projections. In unaffected individuals, the BIS and the BAS cooperate to meet situational demands. For example, when response inhibition is required, the BIS is activated and temporarily inhibits the BAS, thereby inhibiting an approach behaviour.Reference Quay 36 Equilibrium between the two is required for meeting situational demands. Children with ADHD are thought to be relatively insensitive to negative feedback or reprimands whilst being oversensitive to rewards.Reference Luman, Oosterlaan and Sergeant 6 Usually, this is explained by ADHD being associated with underactive BIS, causing hyposensitivity to punishment which in turn would lead to difficulty in inhibiting ongoing and anticipated behaviour, ending in overt impulsive behaviour.Reference Quay 36 Our results partly contradict this view since our adult ADHD group did not show low sensitivity to punishment. On the contrary, our findings of higher sensitivity to reward in ADHD cannot be explained by co-occurring substance use disorders or history of conduct disorders which are linked to high impulsivity and high sensitivity to reward,Reference Genovese and Wallace 37 , Reference Ersche, Jones, Williams, Turton, Robbins and Bullmore 38 as individuals with these comorbidities were not present in our study. In sum, it is intriguing to postulate that in adult ADHD at least, in situations where reward is available but contingencies suggest preventing a response (i.e. conflicts between BAS and BIS since both appetitive and aversive stimuli are concomitant), it is an overactive BAS (oversensitivity to reward) that prevents a normal inhibition system (BIS) from working successfully in inhibiting the BAS.
One hypothesis often mentioned is that ADHD is linked to sensation seeking. Our results show that only one of the dimensions measured by the Sensation Seeking Scale, namely boredom susceptibility, is higher in adults with ADHD compared with controls and relatives. This is consistent with the results found elsewhere in childrenReference Blaskey, Harris and Nigg 10 and adults with ADHDReference Avisar 39 where sensation seeking overall was not significantly higher compared with controls. It has also been shown that high boredom-prone individuals perform poorly on measures of sustained attention and show increased inattentive and impulsive/hyperactive behaviour,Reference Malkovsky, Merrifield, Goldberg and Danckert 40 which are all well-known dimensions of ADHD. These novel and significant findings remain to be replicated in a larger sample of patients, which may also include comorbidities. In a future study with a larger sample size, it may also be possible to determine the relationship between personality traits and forms of cognition. To summarise, we found that in adult ADHD, high impulsive traits and reward sensitivity were not vulnerability factors for ADHD but facets of the clinical phenotype. Moreover, there were no overall differences between groups on sensation seeking, but a closer look at contributing dimensions revealed that the ADHD group was more susceptible to boredom compared with first-degree relatives and controls. This is in line with other research showing that sensation seeking and impulsive personality traits can dissociate and are underpinned but partially distinct neurobiological substrates.Reference Steinberg, Albert, Cauffman, Banich, Graham and Woolard 41 Recent research shows that impulsive traits but not overall sensation seeking are predisposing personality risk factors for drug addiction.Reference Ersche, Turton, Pradhan, Bullmore and Robbins 42 Given the relative increased association between ADHD and comorbid substance misuse,Reference Goodman 43 it is intriguing to hypothesise that personality characteristics, namely high impulsive traits, may be risk factors for comorbid ADHD and substance misuse instead of for solely ADHD. This hypothesis awaits further investigation. Finally, we found that adults with ADHD showed dissociation between reward and punishment sensitivity. Reward sensitivity is associated with poor impulse control and externalising behaviour and correlates with the functional network underpinning motor impulsivity.Reference Fosco, Hawk, Rosch and Bubnik 44 , Reference Fuentes-Claramonte, Avila, Rodriguez-Pujadas, Costumero, Ventura-Campos and Bustamante 45 Previous research also showed that the effect of reinforcement on performance on cognitive tests is higher in children with ADHD who have heightened sensitivity to reward.Reference Fosco, Hawk, Rosch and Bubnik 44 Since the ADHD group in this study showed increased reward sensitivity but no increase in sensitivity to punishment, it is reasonable to postulate that adults with ADHD might benefit from a therapeutic strategy including reinforcement to foster change in several domains such as impulse-driven behaviours. Moreover, this might also facilitate treatment discovery informed by a back-translation approach.
Funding
This work was funded by a Core Award from the Medical Research Council and the Wellcome Trust to the Behavioural and Clinical Neuroscience Institute (MRC Ref G1000183; WT Ref 093875/ Z/10/Z). V.A.P. was supported by a Medical Research Council (MRC) Doctoral Training Grant.




 Open access
Open access
eLetters
No eLetters have been published for this article.