



Introduction
A prominent demographic trend throughout the industrialized world is population aging (Cooke, Reference Cooke2006). Caused by lower fertility rates and rising life expectancies, population aging has led to concerns about economic growth and labour force shortages, as larger proportions of the population are retired (Yenilmez, Reference Yenilmez2015). In response, many European nations have enacted policies, including annulling early retirement options and increasing ages of eligibility for pension benefits, to keep older persons employed (Eurofound, 2019). Accordingly, a pressing current research topic is whether and under what circumstances involvement and transitions in paid work are beneficial for older persons’ health and well-being.
The present study addresses this topic through an analysis of a European sample of persons from 50 to 75 years of age. Accordingly, this is a study of late-middle-aged and senior adults. The introduction and review of the literature begin with descriptions of two theories relevant to how, for persons 50–75 years of age, paid work is associated with health: activity theory and the theory of cumulative advantage/disadvantage. This is followed by discussion of current empirical trends in middle-aged and senior persons’ involvements and transitions in paid work, as well as how methodological differences within studies of their health and well-being associations have led to mixed results. These mixed findings highlight the importance of studying sources of heterogeneity in the effects of workforce involvement/transitions for persons 50–75 years of age, among which are financial difficulties. Furthermore, this study considers interactions with gender, emphasizing that late-middle-aged and senior women came of age during times in which feminism was at a relatively early stage of development, affecting the quality of their workforce histories. This background and literature review lead to the research questions and hypotheses guiding this study.
This study thus aims to uncover how workforce involvement/transitions are associated with health in persons from 50 to 75 years of age. Furthermore, it investigates heterogeneity in these associations by financial difficulties and gender. This article contributes to the literature a more thorough and nuanced understanding of how paid work among late-middle-aged and senior adults is associated with health.
Theoretical Perspectives
Activity Theory of Aging
Scholarship emphasizing that older persons are healthier and happier if they maintain high levels of activity (e.g., Bassett, Bourbonnais, & McDowell, Reference Bassett, Bourbonnais and McDowell2007; Chapman, Reference Chapman2005) follows from Older People (Havighurst & Albrecht, Reference Havighurst and Albrecht1953/1980). For example, Burgess (Reference Burgess1960) highlighted that older persons who substitute lost social roles, community engagements, and activities with new involvements benefit in their self-perceptions and quality of life. Concordant with this theory, scholarship promoting later-life employment emphasizes that it keeps older persons physically, cognitively, and socially active, while maintaining their positive self-conceptions and life purpose (Lemon, Bengtson, & Peterson, Reference Lemon, Bengtson and Peterson1972).
Theory of Cumulative Advantage/Disadvantage
This theory proposes that advantages (and disadvantages) earlier in life beget later advantages (and disadvantages) (O’Rand, Reference O’Rand1996; Ross & Wu, Reference Ross and Wu1996). These include socio-economic advantages, such as higher education, income, wealth, and occupational prestige. For example, higher education earlier in life leads to a greater accumulation of income through time (Brown & Sessions, Reference Brown and Sessions1999; Muller, Reference Muller2002). This theory thus explains the increasing heterogeneity in important aspects of quality of life, including employment, family, health, and financial circumstances, among members of the same cohort as they age (O’Rand, Reference O’Rand1996; Ross & Wu, Reference Ross and Wu1996).
More specifically, this study considers that even more than younger women, late-middle-aged and senior women faced sexist labour markets and societal assumptions concerning women’s roles as they reached employment age, resulting in fragmented employment histories (Davis, Reference Davis2003) within work of lower quality and status (Quinn & Kozy, Reference Quinn and Kozy1996). Combined with generally fewer years of education (Domenico & Jones, Reference Domenico and Jones2007), this implies that many late-middle-aged and senior women have not accumulated the workforce experiences and skills that would allow them to work in high quality and health-promoting jobs.
Current Trends in Late-Middle-Aged and Senior Adults’ Paid Work
Concurrent with population aging, present-day Europeans are working until later ages than in the past (Eurofound, 2019). In fact, rates of early retirement in Europe have decreased through time (Been & van Vliet, Reference Been and van Vliet2017). This prolonged paid work is associated with the growing prevalence of defined contribution instead of defined benefit pension plans (PensionsEurope, 2017). The former tie earnings in retirement with funds contributed into the plan by the employee, the employer, or both, and they incentivize remaining employed until later ages (Broadbent, Palumbo, & Woodman, Reference Broadbent, Palumbo and Woodman2006).
Furthermore, there is growing variability in workforce involvement patterns among those in their late middle-age and senior years. For example, many present-day Europeans are returning to paid work after some time spent in retirement (Dingemans, Henkens, & Solinge, Reference Dingemans, Henkens and Van Solinge2016). Nonetheless, most studies of workforce transitions within this age group still focus only on retirement. Understanding present-day economic and labour market realities requires broader studies addressing the complexity of late-middle-aged and senior persons’ workforce involvements.
Associations of Workforce Involvements with Middle-Aged and Senior Adults’ Health
These trends underscore the importance of studying how involvements and transitions in paid work affect the health and well-being of middle-aged and senior adults. Persons within this age group are more likely to work effectively (Platis, Reklitis, & Zimeras, Reference Platis, Reklitis and Zimeras2015) and remain employed (Smeaton & White, Reference Smeaton and White2016) if their paid work is not causing them harm. This study addresses this key research priority.
Scholarship on this topic has produced mixed results. Although some scholars argue for the benefits of employment among middle-aged and senior adults (e.g., Arpino & Solé-Auró, Reference Arpino and Solé-Auró2019; Hao, Reference Hao2008; Hinterlong, Morrow-Howell, & Rozario, Reference Hinterlong, Morrow-Howell and Rozario2007), others suggest that it is generally detrimental to health and well-being (e.g., Kerkhofs & Lindeboom, Reference Kerkhofs and Lindeboom1997; Lindeboom & Kerkhofs, Reference Lindeboom and Kerkhofs2002; Neuman, Reference Neuman2008). The above studies that found benefits of employment utilized samples of similar ages to those of the present study. On the other hand, two of the above studies that found detriments to paid work (Kerkhofs & Lindeboom, Reference Kerkhofs and Lindeboom1997; Lindeboom & Kerkhofs, Reference Lindeboom and Kerkhofs2002) studied a sample over two waves (wave 1: 1993, wave 2: 1995) that was initially 43–63 years of age, and therefore younger. These diverging conclusions might be because the health benefits of the physical, social, and cognitive activity involved in employment are prominent at ages during which functional declines become more prevalent. Concerning Neuman (Reference Neuman2008), it is notable that respondents (within an age range similar to that of the present study) were categorized as retired if they worked fewer than 1,200 hours per year. As such, full retirees were not distinguished from part-time workers. Neuman’s (Reference Neuman2008) finding of beneficial effects of retirement on subjective health might be because part-time work is particularly suitable for middle-aged and senior persons and is therefore beneficial for their health. This idea further concords with Neuman’s (Reference Neuman2008) finding that increased annual hours of paid work are associated with subjective health detriments. Although studies finding health benefits of employment in the middle-age and senior years concord with the activity theory of aging, those finding the opposite emphasize the demands that employment places on physical and mental endurance (Kerkhofs & Lindeboom, Reference Kerkhofs and Lindeboom1997; Lindeboom & Kerkhofs, Reference Lindeboom and Kerkhofs2002). Contrastingly, studies of unemployment (involuntary uninvolvement in paid work), in specific, have consistently revealed detrimental effects among middle-aged and senior adults (e.g., Gallo et al., Reference Gallo, Teng, Falba, Kasl, Krumholz and Bradley2006; Kachan et al., Reference Kachan, Fleming, Christ, Muennig, Prado and Tannenbaum2015; Noelke & Beckfield, Reference Noelke and Beckfield2014).
These mixed results suggest that further research on the associations of employment with health in the late middle-age and senior years is necessary, including interaction analyses. This study contributes to this scholarship through examining how a comprehensive set of patterns of workforce involvement/transitions are associated with the health of persons from 50 to 75 years of age, along with sources of heterogeneity in these associations.
Although it is beyond the scope of the present study to investigate associations with health of specific features of late-middle-aged and senior persons’ paid employment, it is notable that this employment tends to be marked by beneficial characteristics. One study found that older workers are more advantaged than their younger counterparts through investigating work schedules and options for working fewer hours, stability and permanence of employment contracts, quality of training received on the job, qualifications required for successful job performance (including matches between these requirements and workers’ particular sets of skills), and extents of requirements for working non-standard hours (which can hamper desirable work-life balance) (Arranz, García-Serrano, & Hernanz, Reference Arranz, García-Serrano and Hernanz2019). Another study found that older workers are more likely to be employed on a part-time basis (which might be less physically and mentally taxing, therefore advantageous for older workers) and to work primarily from their homes, are less likely to be required to work overtime, and report higher job satisfaction and less employment stress, as well as profiting from more autonomy, more support from their supervisors, and lower likelihoods of experiencing work-related injuries (Grosch, Reference Grosch2017). Nonetheless, quality of employment varies among late-middle-aged and senior workers. It is plausible that the more limited physical and mental endurance that comes with the aging process (Wong & Tetrick, Reference Wong and Tetrick2017) accentuates the extent to which jobs that are physically or mentally stressful pose obstacles to maintained or improved health and well-being. In particular, jobs that do not permit reduced work hours might place insalubrious demands on some workers. As such, specific characteristics of late-middle-aged and senior adults’ employment are among the sources of heterogeneity that should be studied.
Another important consideration is that health issues and difficult work circumstances motivate many late-middle-aged adults to retire early. Poor health, depressive symptoms, physically strenuous work (especially difficult with advancing age), pressured circumstances at work, lack of appreciation at one’s work, regular conflicts within one’s workplace (de Wind, Geuskens, Ybema, Bongers, & van der Beek, Reference de Wind, Geuskens, Ybema, Bongers and van der Beek2015; Van Den Berg, Elders, & Burdorf, Reference Van Den Berg, Elders and Burdorf2010), and desire to work fewer hours (Silver, Settels, Schafer, & Schieman, Reference Silver, Settels, Schafer and Schieman2019) increase likelihood of early retirement. The financial capability to do so comfortably further predicts early retirement (de Wind et al., Reference de Wind, Geuskens, Ybema, Blatter, Burdorf and Bongers2014, Reference de Wind, Geuskens, Ybema, Bongers and van der Beek2015). These motivating circumstances suggest that some early retirees might experience more favourable health than if they kept working for pay.
The Importance of Financial Circumstances
Financial circumstances are a potential source of heterogeneity in the health outcomes of workforce involvement patterns in the late middle-age and senior years. Financial difficulties, for example, are stressors that damage physical and mental health (Drentea & Reynolds, Reference Drentea and Reynolds2015). These stressors might be especially intense for late-middle-aged and senior persons who are married and/or parents, and therefore likely to have financial responsibilities for their close family members (Cooney & Uhlenberg, Reference Cooney and Uhlenberg1992; Huang, Perales, & Western, Reference Huang, Perales and Western2021). Accordingly, older persons with lower wages are more likely than those with medium wages to engage in paid work after retirement from their main careers to address financial difficulties (Cahill, Giandrea, & Quinn, Reference Cahill, Giandrea and Quinn2006; Settels & McMullin, Reference Settels and McMullin2017). Furthermore, troubled financial circumstances incline older persons to delay retirement (Damman, Henkens, & Kalmijn, Reference Damman, Henkens and Kalmijn2015). Employment in the late middle-age and senior years that ameliorates financial difficulties might be especially health promoting.
On the other hand, the typically less-advantaged employment histories of late-middle-aged and senior adults in difficult financial circumstances might reduce opportunities for higher status and better paid work. Lower paid work tends to be more precarious, more physically strenuous (thus posing risks for safety and health), and marked by fewer benefits and paid sick leave provisions, while providing fewer opportunities for training in workforce-relevant skills (Hund-Mejean & Escobari, Reference Hund-Mejean and Escobari2020; Zhang & Zuberi, Reference Zhang and Zuberi2017). Precarious employment causes frustration and depression (Han, Chang, Won, Lee, & Ham, Reference Han, Chang, Won, Lee and Ham2017; Zhang & Zuberi, Reference Zhang and Zuberi2017). Lower paid employment also increases the need to work longer hours (Zhang & Zuberi, Reference Zhang and Zuberi2017). These negative features of lower-status employment potentially pose health risks for workers of all ages. However, because of their generally lower physical and mental endurance (Wong & Tetrick, Reference Wong and Tetrick2017), late-middle-aged and senior workers might be especially vulnerable to these health risks.
At the other end of the spectrum, late-middle-aged and senior persons experiencing financial ease might have more freedom concerning their employment and retirement decisions. Older persons of higher socio-economic status, based on wages, education, and occupational prestige, have a higher propensity than those of middling socio-economic status to voluntarily undertake paid work after retirement to remain socially and intellectually active and engaged (Cahill et al., Reference Cahill, Giandrea and Quinn2006). Furthermore, in accordance with the theory of cumulative advantage/disadvantage, their more advantaged workforce pasts position them for finding high quality employment with scheduling (e.g., flexibility), content (e.g., lack of physical strenuousness), and conditions (e.g., calm pace and good coworker relationships) that are especially beneficial for late-middle-aged and senior persons. Employment might therefore be most favourable for the health of late-middle-aged and senior persons in good financial standing.
In most nations of the European Union, late-middle-aged and senior adults are more likely than the general population to be in poverty (World Health Organization, 2015). The consequentiality of countries’ specific policies is evident in how some nations (e.g., Luxembourg, Poland, The Netherlands, Czechia, Hungary, and France) effectively protect their late-middle-aged and senior residents from financial hardship (World Health Organization, 2015). This has led to cross-national differences in rates of poverty among adults in this age group (Organisation for Economic Co-operation and Development, 2020b). In higher-income nations, one’s financial adequacy generally varies only slightly between one’s earlier and later years (World Health Organization, 2015). As such, residents of lower-income nations have stronger reason to fear falling into financial difficulties in their late middle-age and senior years.
The Importance of Gender
These associations might further differ by gender. From the mid-1960s to the mid-1980s, women throughout the developed world joined in contesting and overcoming their restricted life circumstances and societal roles (Bruley & Forster, Reference Bruley and Forster2016). This social movement has been termed the “women’s liberation movement” and “second-wave feminism” (Bruley & Forster, Reference Bruley and Forster2016). Since the late 1970s, women have attained higher levels of education and skills development, as well as occupational prestige, including in traditionally masculine occupations (Domenico & Jones, Reference Domenico and Jones2007; Hakim, Reference Hakim2016). These gains were partly the result of legislation counteracting gender discrimination in employment (Hakim, Reference Hakim2016). Nevertheless, these gains are far from complete, as women throughout the world still have higher rates of poverty than men (World Health Organization, 2015).
Late-middle-aged and senior women, however, came of age during times in which this progress was at an early stage. Accordingly, many have had fragmented work trajectories (Davis, Reference Davis2003), including numerous spells of part-time and temporary employment (Quinn & Kozy, Reference Quinn and Kozy1996), in workplaces marked by sex segregation, prejudice, and discrimination (Perkins, Reference Perkins1994). Combined with less education and prevalent ageism (sexism and ageism might be intersectional) within the labour market (McMullin & Duerden Comeau, Reference McMullin, Duerden Comeau and McMullin2011), and in accordance with the theory of cumulative advantage/disadvantage, these fragmented work histories might disadvantage late-middle-aged and senior women seeking high quality and well-paying employment favourable for health. Circumstances might therefore be especially harsh for present-day late-middle-aged and senior women undergoing financial hardship, especially because older women across the world are less likely to have obtained pension entitlements throughout their employment trajectories (World Health Organization, 2015).
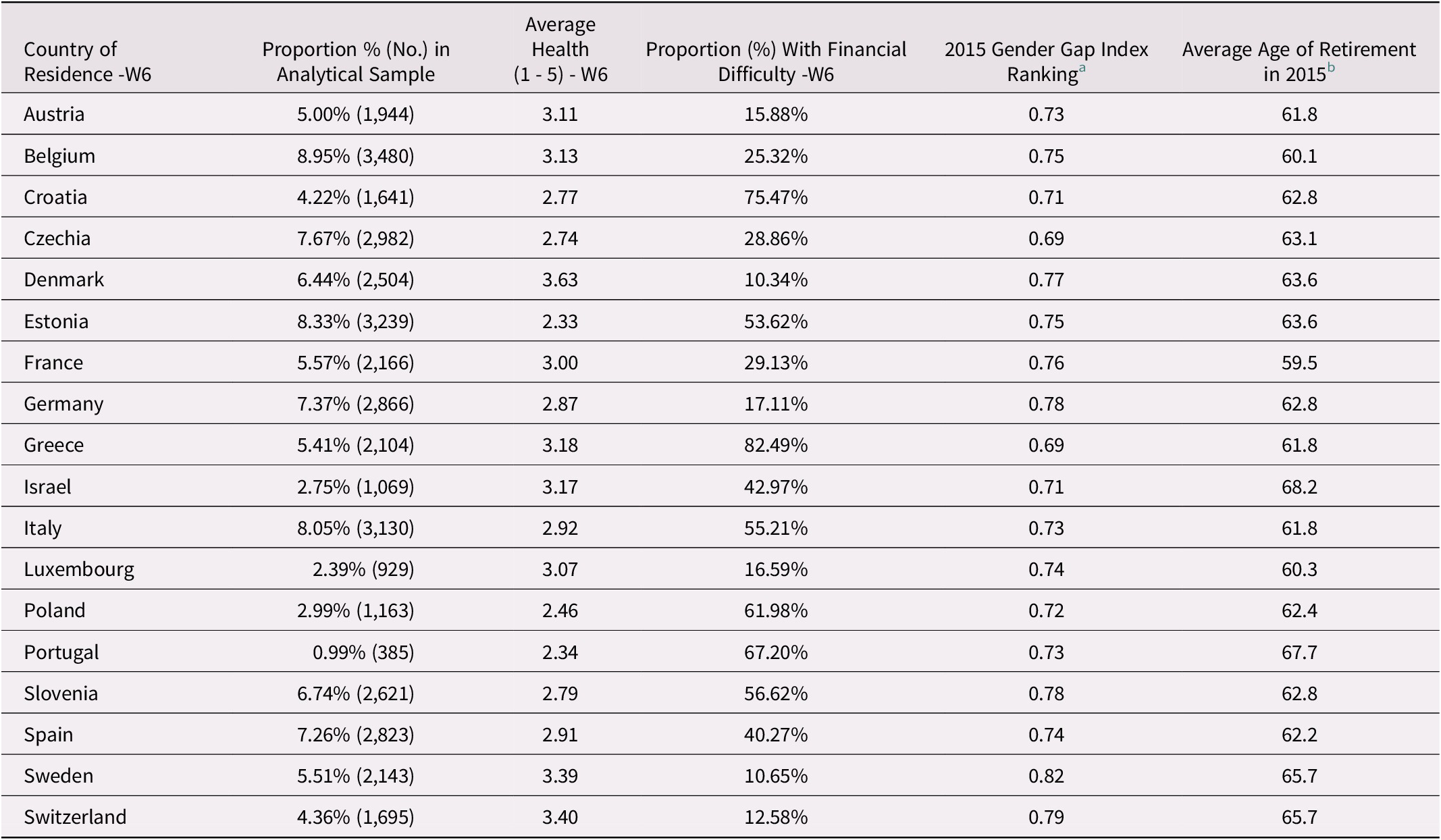
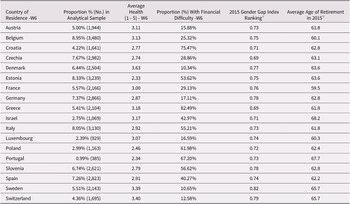
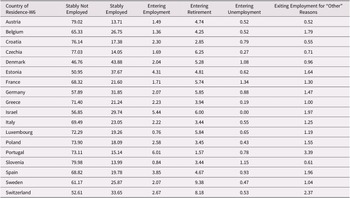
Table 1 displays the 2015 Global Gender Gap Index rankings for all 18 nations included in this study (World Economic Forum, 2020). The variability in these rankings suggests some differences in the timing and pace of these nations’ progress towards greater gender equality.
Table 1. Descriptive statistics pertaining to countries of residence at wave six within the SHARE data set (n = 38,884)
Research Questions and Hypotheses
This study presents three research questions concerning the short-term health impacts of 50–75-year-old persons’ workforce involvements/transitions. First, are employment and transition into employment beneficial for 50–75-year-old persons’ health? The mixed literature suggests two plausible hypotheses.
H1.1: Employment from 50 to 75 years of age is damaging to health because it taxes this age group’s more limited physical and mental endurance.
H1.2: Employment from 50 to 75 years of age is beneficial for health because it helps maintain salubrious amounts of physical, cognitive, and social activity.
Second, does financial difficulty increase or decrease the health benefits of employment among those 50–75 years of age? The literature presents two possible hypotheses.
H2.1: Financial difficulties among those 50–75 years of age increase the health benefits of employment as it helps improve financial circumstances.
H2.2: Lack of financial difficulties among those of 50–75 years of age increases the health benefits of employment as it is more freely chosen based on intrinsic motivations to remain active and socially engaged. Furthermore, lack of financial difficulties indicates more advantaged workforce trajectories that position adults from 50 to 75 years of age for higher quality employment that is favourable for health.
Third, is there heterogeneity by gender in how financial difficulties interact with workforce involvement/transitions in affecting the health of adults from 50 to 75 years of age? This study presents two hypotheses.
H3.1: The combined difficulties of being a person 50–75 years of age facing an ageist labour market while undergoing financial difficulties imply that any further disadvantages based on being a woman are not consequential for health.
H3.2: Intersectionality between ageism and sexism, combined with the disadvantaged workforce trajectories of many present-day women from 50 to 75 years of age, suggest that there is heterogeneity by gender in how current financial challenges interact with workforce involvement/transitions in affecting health.
Data and Methods
Data Set and Sample
In addressing these research questions, this study employed waves six (2015) and seven (2017) of the Survey of Health, Ageing and Retirement in Europe (SHARE). The SHARE is a longitudinal panel study of a sample of persons 50 years of age and older that covers many European nations and Israel. This data set’s focus is health, paid work, retirement, socio-economic status, family relationships, and social networks. For wave one (2004), more than 22,000 interviews took place in 11 European nations. Subsequent waves were approximately biennial and incorporated more European countries. Börsch-Supan et al. (Reference Börsch-Supan, Brandt, Hunkler, Kneip, Korbmacher and Malter2013) provide further details.
This study employed easySHARE (easySHARE Release 7.0.0) because it includes all of the wave seven and most of the wave six variables analyzed. easySHARE is a simplified generated data set that includes information for all respondents across all waves within one file (see Gruber, Hunkler, & Stuck, Reference Gruber, Hunkler and Stuck2014). This data set includes a more limited set of variables and it allocates couple- and household-level data to the level of the individual (Börsch-Supan & Gruber, Reference Börsch-Supan and Gruber2019). Because all of this study’s analyses were at the individual level, this limitation was not a concern. However, two control variables (the scales of social connectedness and satisfaction with one’s social network [discussed subsequently]) were obtained from the SHARE’s wave six data set (SHARE Release 7.0.0) (see Börsch-Supan, Reference Börsch-Supan2019; Malter & Börsch-Supan, Reference Malter and Börsch-Supan2017) because they are not included in easySHARE. Börsch-Supan et al. (Reference Börsch-Supan, Bristle, Andersen-Ranberg, Brugiavini, Jusot and Litwin2019) present preliminary findings from the SHARE’s waves six and seven.
This study’s sample participated in waves six and seven, and was between 50 and 75 years of age at wave six. Employing two recent consecutive waves is ideal for analyses of the current effects of specific workforce transitions. The age restriction ensured the study of older adults young enough to undergo workforce transitions. Among the 50,215 respondents who were between 50 and 75 years of age at wave six, 39,119 participated in wave seven (see Bergmann, Kneip, De Luca, & Scherpenzeel, Reference Bergmann, Kneip, De Luca and Scherpenzeel2019). Within this study’s analytical sample, 35.35 per cent were between 50 and 60 years of age, 16.45 per cent were between 61 and 64 years of age, and 48.20 per cent were between 65 and 75 years of age at wave six. All SHARE respondents meeting these sampling criteria resided in the following countries at wave six: Austria, Belgium, Croatia, Czechia, Denmark, Estonia, France, Germany, Greece, Israel, Italy, Luxembourg, Poland, Portugal, Slovenia, Spain, Sweden, and Switzerland. This study did not exclude any countries.
Variables
Dependent variable
Wave seven self-perceived health was this study’s dependent variable. In response to, “Would you say your health is…”, respondents answered “poor”, “fair”, “good”, “very good”, or “excellent”; “poor” was accorded a score of one and “excellent” received a score of five. This general measure that subsumes both physical and mental health was appropriate for this study’s focus on the broad well-being of 50–75-year-old adults.
Self-perceived overall health is an effective measure of general health and well-being (Rueda, Artazcoz, & Navarro, Reference Rueda, Artazcoz and Navarro2008; Schnittker & Bacak, Reference Schnittker and Bacak2014) that potently predicts mortality (Ferraro & Farmer, Reference Ferraro and Farmer1996; Schnittker & Bacak, Reference Schnittker and Bacak2014), especially in older samples (Mossey & Shapiro, Reference Mossey and Shapiro1982). The subjectivity of this measure might cause some concern. For example, recent life events might incline respondents to report greater or lesser overall health, depending on whether these events led to optimism or pessimism. Given this study’s focus on overall health, well-being, and quality of life, this subjectivity becomes less of a concern. Increased optimism or pessimism resulting from transitions in employment are in themselves potent influences on overall quality of life, and therefore are concordant with this study’s goals. Although this study could have employed alternative outcomes, such as overall mental health, depressive symptoms, or physician-diagnosed conditions, self-perceived overall health was particularly effective because of its breadth.
Central independent variable
The central independent variable was based on six categories of workforce involvement/transitions: employed at both waves (“employed or self-employed [including working for family business]”: reference category), not employed at both waves, entering employment, entering retirement, entering unemployment, and exiting employment for reasons other than retirement or unemployment (including because of permanent sickness or disability, to be a homemaker, and for other reasons). All respondents who performed any form of paid employment in the previous four weeks were categorized as working for pay within the SHARE (Alavinia & Burdorf, Reference Alavinia and Burdorf2008). Figure 1 displays this variable with descriptive statistics from Table 2.
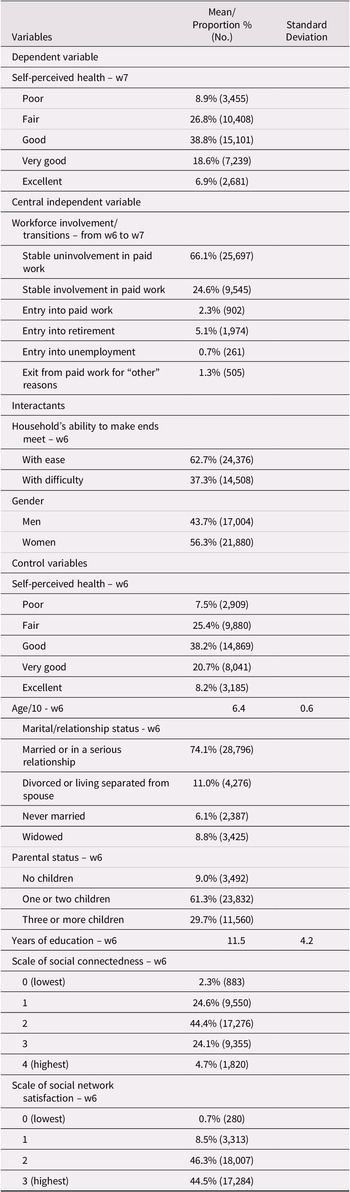
Table 2. Descriptive statistics of the analytical sample within the SHARE data set (n = 38,884)
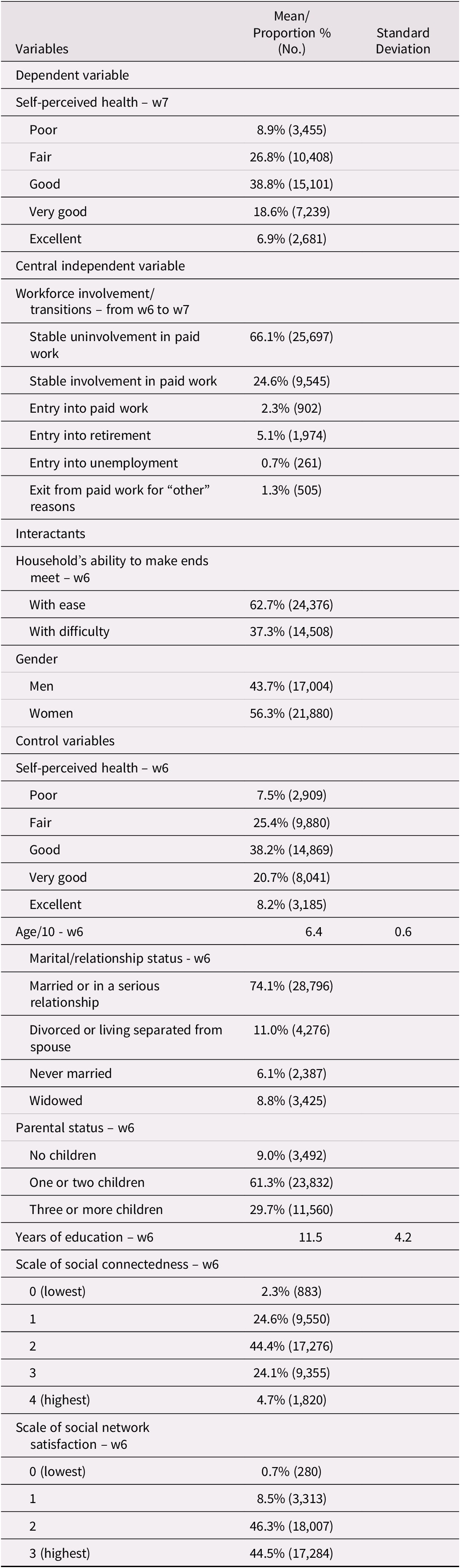
Note. SHARE = Survey of Health, Ageing and Retirement in Europe; w6 = wave 6; w7 = wave 7.
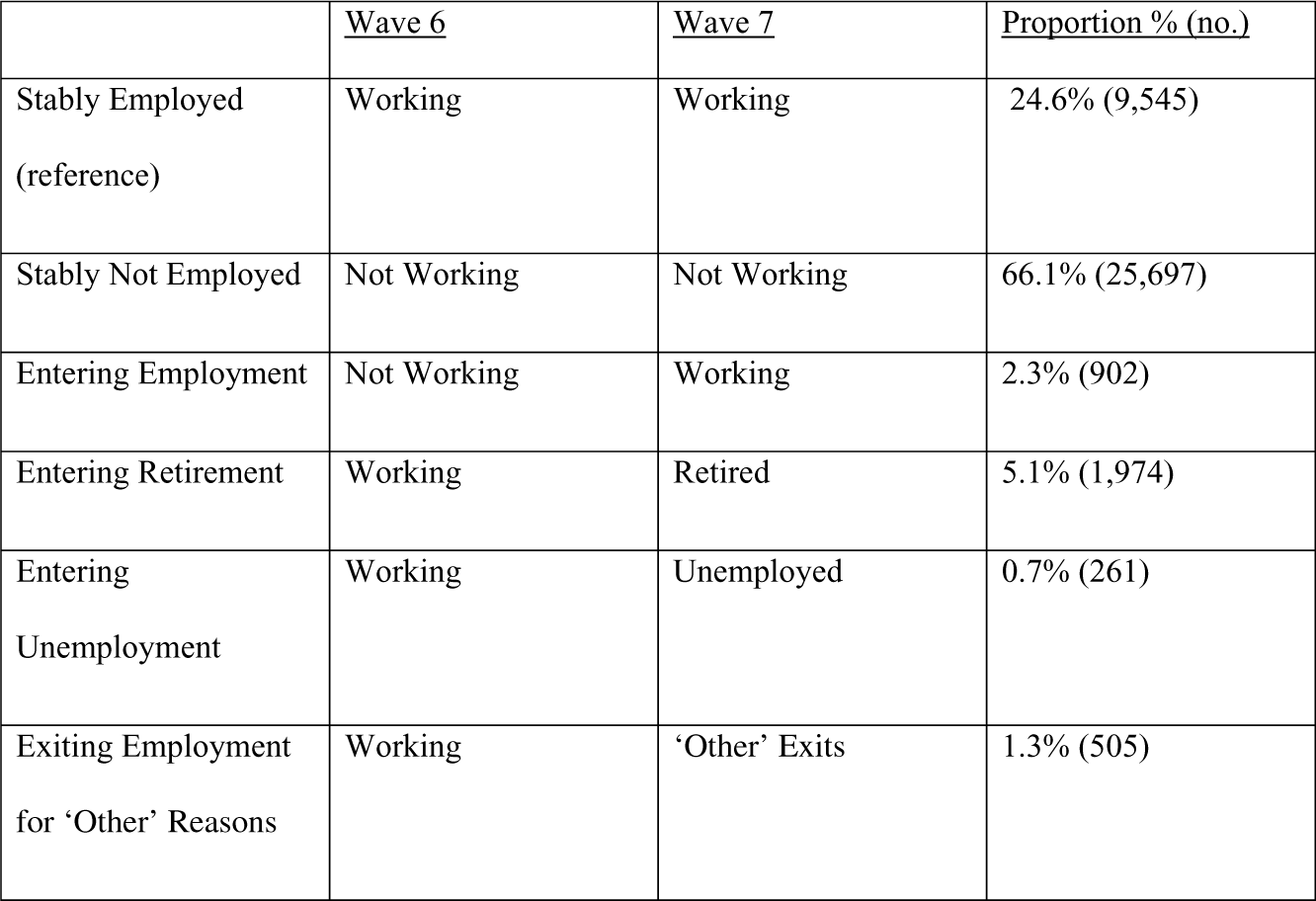
Figure 1. Schema displaying the categories of the workforce involvement/transitions central independent variable (n = 38,884)
Among those in the “stably not employed” category, 64.91 per cent were retired at wave six, 70.45 per cent were retired at wave seven, and 62.10 per cent were retired at both waves.
These categories are based on an interest in the actual and intended temporality of workforce involvements/transitions. The first two categories denote stability. Those entering employment were temporarily not employed at wave six. Those entering retirement intended some stability in their transition out of employment. Respondents entering unemployment were actively seeking work at wave seven, implying an intended temporariness in their wave seven work status. Although permitting a comprehensive analysis of workforce involvement/transitions, the final category is ambiguous concerning temporality.
This study’s focus was the following five comparisons: “stably employed” versus “stably not employed”, “entering employment” versus “stably not employed” (accomplished through post-estimation t tests), “entering retirement” versus “stably employed”, “entering unemployment” versus “stably employed”, and “exiting paid work for ‘other’ reasons” versus “stably employed”. Those undergoing each transition were compared with those with the same wave six work status who were not undergoing a transition.
Interactants
The first interactant with how workforce involvement/transitions are associated with health studied here was the ability of respondents’ households to make ends meet. In response to, “Thinking of your household’s total monthly income, would you say that your household is able to make ends meet…”, respondents could answer “with great difficulty”, “with some difficulty”, “fairly easily”, and “easily”. The former two were combined into “difficulty”, and the latter two were combined into “ease” (reference). To study how the health outcomes of workforce transitions were heterogeneous based on the financial situations within which they occurred, this variable was studied at wave six. The second interactant here studied was gender (reference = men).
Control variables
All control variables were from wave six, because controlling for wave seven variables could potentially block mechanisms between the central independent variable (and its interaction effects) and health at wave seven. First, the measure of health that served as dependent variable at wave seven was employed as a control variable at wave six (a set of dummy variable categories with “poor health” as the reference category; explained further in the Analysis section).
Next, a set of demographic variables were controlled. Because advancing age in the late middle-age and senior years often implies reduced physical and mental endurance (Wong & Tetrick, Reference Wong and Tetrick2017), age was controlled (divided by 10 to produce more substantial odds ratios [ORs]). Another control variable was marital/relationship status: married or in a serious relationship (reference), divorced or living separated from spouse, never married, and widowed. Further controlled was parental status: no children, one or two children, and three or more children (reference). Marital and parental status are relevant control variables because financial difficulties can decrease the quality of life of 50–75-year-old adults through posing obstacles to providing close family members with financial support (Cooney & Uhlenberg, Reference Cooney and Uhlenberg1992; Huang et al., Reference Huang, Perales and Western2021). Years of education were also controlled, because of their associations with likelihood of financial difficulties (Brown & Sessions, Reference Brown and Sessions1999; Muller, Reference Muller2002). These important features of respondents’ lives might confound the central relationships studied.
Moreover, two measures of respondents’ social lives were controlled. One was a scale of social connectedness, broadly measuring the extensiveness and strength of respondents’ social networks (Litwin & Stoeckel, Reference Litwin and Stoeckel2016). This scale spanned from zero (lowest) to four (highest (reference)) and was operationalized as a set of dummy variable categories. The second was a scale of respondents’ satisfaction with their close social networks. This scale spanned from zero (lowest) to ten (highest). Because few respondents reported values below five, this scale was amalgamated into four dummy variable categories: zero to four (“zero”), five to seven (“one”), eight or nine (“two”), and ten (“three” [reference]). These variables were controlled because social connectedness and networks are associated with the health (Kohli, Hank, & Kunemund, Reference Kohli, Hank and Kunemund2009) and paid work (Lancee & Radl, Reference Lancee and Radl2012) of late-middle-aged and senior persons, and might thus confound the central relationships studied.
Analysis
This investigation employed five ordinal logistic regressions to analyze how workforce involvement/transitions, difficulty making ends meet, and gender interact in their associations with 50–75-year-old adults’ health. Model 1 focused on workforce involvement/transitions. Model 2 addressed the interaction between workforce involvement/transitions and difficulty making ends meet. Model 3 focused on the interaction between workforce involvement/transitions and gender. Model 4 addressed the interaction between difficulty making ends meet and gender. The final model (Model 5) assessed a three-way interaction among workforce involvement/transitions, difficulty making ends meet, and gender. Post-estimation t tests established statistical significance scores for differences between ORs pertaining to “stably not employed” and “entering employment”.
These models included all control variables, including wave six self-perceived health. This modelling strategy is known as the “lagged dependent variable technique”, or the “conditional change panel model”, and it permitted study of how the predictors were associated with health at wave seven for fixed levels of health at wave six (Finkel, Reference Finkel1995). This study thus assessed the predictors’ associations with changes in health between the two waves. Conditional change panel models reduce the likelihood that selection effects or reverse causality are driving the associations between the predictors and the outcome. Furthermore, controlling for initial levels of health permitted adjustment for all life course influences on health up to the time of the SHARE’s sixth wave, thus allowing identification of how subsequent workforce involvements and transitions were associated with ensuing changes in health.
This investigation employed two consecutive waves of SHARE data; including more than two consecutive waves would have required analysis of workforce trajectories, which was not this study’s aim. Furthermore, employing more waves of data would have precluded conditional change panel modelling, which is crucial for studies of how workforce transitions are associated with late-middle-aged and senior persons’ health, because earlier health can select respondents in this age group into particular employment decisions (Cahill et al., Reference Cahill, Giandrea and Quinn2006).
This study drew on 39,119 respondents from 50 to 75 years of age at wave six who participated in both waves six and seven. The SHARE calibrated longitudinal individual weights for waves six to seven were employed to adjust the models for selective attrition between the two waves; there were notable statistically significant differences (established through comparison of means t tests) between those wave six respondents who participated in wave seven (“remained within the sample”) and those who did not. For example, women were more likely than men to remain in the sample. Furthermore, those who remained in the sample were slightly older, had somewhat higher self-perceived health, had slightly more years of education, had less difficulty making ends meet, tended to have more children, had higher extents of social connectedness, and were slightly less likely to be married or in a serious relationship. There were no statistically significant differences in social network satisfaction and likelihood of working for pay. The SHARE calibrated longitudinal individual weights accorded higher weights to respondents who were less likely to have remained in the sample.
Even so, this study’s findings might have underestimated how workforce involvement/transitions in interaction with difficulty making ends meet and gender are associated with health, because those with health that was more fragile and who had greater difficulty making ends meet were less likely to have remained in the sample. This underestimation might have been further accentuated because those with less education and more constrained social connectedness were less likely to have participated in wave seven; education (Goldman & Smith, Reference Goldman and Smith2011) and social connectedness (Cornwell & Waite, Reference Cornwell and Waite2009) are health-protective factors. The 121 respondents who were not associated with a weight were removed from the sample.
Missing data were dealt with through multiple imputation using chained equations. Two variables had at least 5 per cent missing data: the scales of social connectedness (15.7% missing) and social network satisfaction (12.3% missing). Respondents missing data on wave seven health were included in the multiple imputation process but excluded from the final analyses (see von Hippel, Reference Von Hippel2007), removing 114 respondents. Standard errors were adjusted for clustering at the wave six country level.
Analyses were conducted with the Stata 16 statistical software package. This study further included estimation of predicted probabilities of reporting “good”, “very good”, or “excellent” health in each of the 24 possible combinations of workforce involvement/transitions, ability to make ends meet, and gender categories, through predictive margins, as actualized by means of Stata’s “margins” command. In doing so, all covariates, including wave six health, were held at their means.
Results
The analytical sample contained 38,884 respondents, having excluded those with missing outcome information (n = 114) or missing calibrated longitudinal individual weights (n = 121). Table 2 presents all variables’ descriptive statistics for this analytical sample. Whereas relatively few respondents reported having “poor” (8.9%) or “excellent” health (6.9%) at wave seven, relatively many reported “fair” (26.8%) or “good” (38.8%) health. Wave six showed a slight tendency towards better health.
Whereas high proportions of respondents were stably employed (24.6%) or stably not employed (66.1%), relatively few entered unemployment (0.7%) or exited employment for “other” reasons (1.3%). Almost two thirds of respondents reported ease in making ends meet (62.7%). The majority of respondents were women (56.3%).
The average respondent was 63.6 years of age. Almost three quarters of respondents were married or in a serious relationship (74.1%). Whereas the majority of respondents had one or two children (61.3%), relatively few had no children (9.0%). The average respondent completed 11.5 years of education.
The scale of social connectedness had an approximately normal distribution, with 44.4 per cent of respondents having a score of 2 (midway between 0 [lowest] and 4 [highest]). Whereas relatively few respondents were in the lowest category of the scale of social network satisfaction (0.7%), many were in the second highest (46.3%) and highest (44.5%) categories.
Table 1 presents descriptive statistics for the 18 wave six countries of residence. The second column shows that the proportions of the analytical sample within each of the 18 countries ranged from 0.99 per cent (Portugal) to 8.95 per cent (Belgium). The third column displays averages in this study’s health variable at wave six. Values spanned from 2.33 (between “fair” and “good”) in Estonia to 3.63 in Denmark (between “good” and “very good”). The fourth column displays proportions experiencing financial difficulties, according to this study’s wave six variable. Proportions ranged from 10.34 per cent in Denmark to 82.49 per cent in Greece. The fifth column presents 2015 Global Gender Gap Index rankings (World Economic Forum, 2020), according to which a score of 1.00 implies full gender equality. Rankings varied from 0.69 in Czechia and Greece to 0.82 in Sweden. The final column shows average ages of retirement in 2015, according to the Organisation for Economic Co-operation and Development (2020a). Whereas the lowest was 59.5 years in France, the highest was 68.2 years in Israel. Therefore, these 18 nations show differences in health, financial circumstances, gender equality, and retirement patterns. This highlights the need to cluster standard errors by country of residence at wave six.
Table 3 displays the proportions of respondents in each country who underwent each of the six patterns of workforce involvement/transitions. Rates of stable uninvolvement in paid work ranged from 46.76 per cent in Denmark to 79.98 per cent in Slovenia. Proportions stably employed spanned from 13.71 per cent in Austria to 43.88 per cent in Denmark. Rates of entry into employment spanned from 0.76 per cent in Luxembourg to 6.01 per cent in Portugal. Entry into retirement included proportions ranging from 1.57 per cent in Portugal to 9.38 per cent in Sweden. Entry into unemployment showed rates spanning 0.00 per cent in Israel to 1.34 per cent in France. Finally, proportions exiting work for “other” reasons ranged from 0.52 per cent in Austria to 3.39 per cent in Portugal. These variations also highlight the importance of clustering standard errors by wave six nation of residence.
Table 3. Proportions (%) in each category of workforce involvement/transitions by country (n = 38,884)
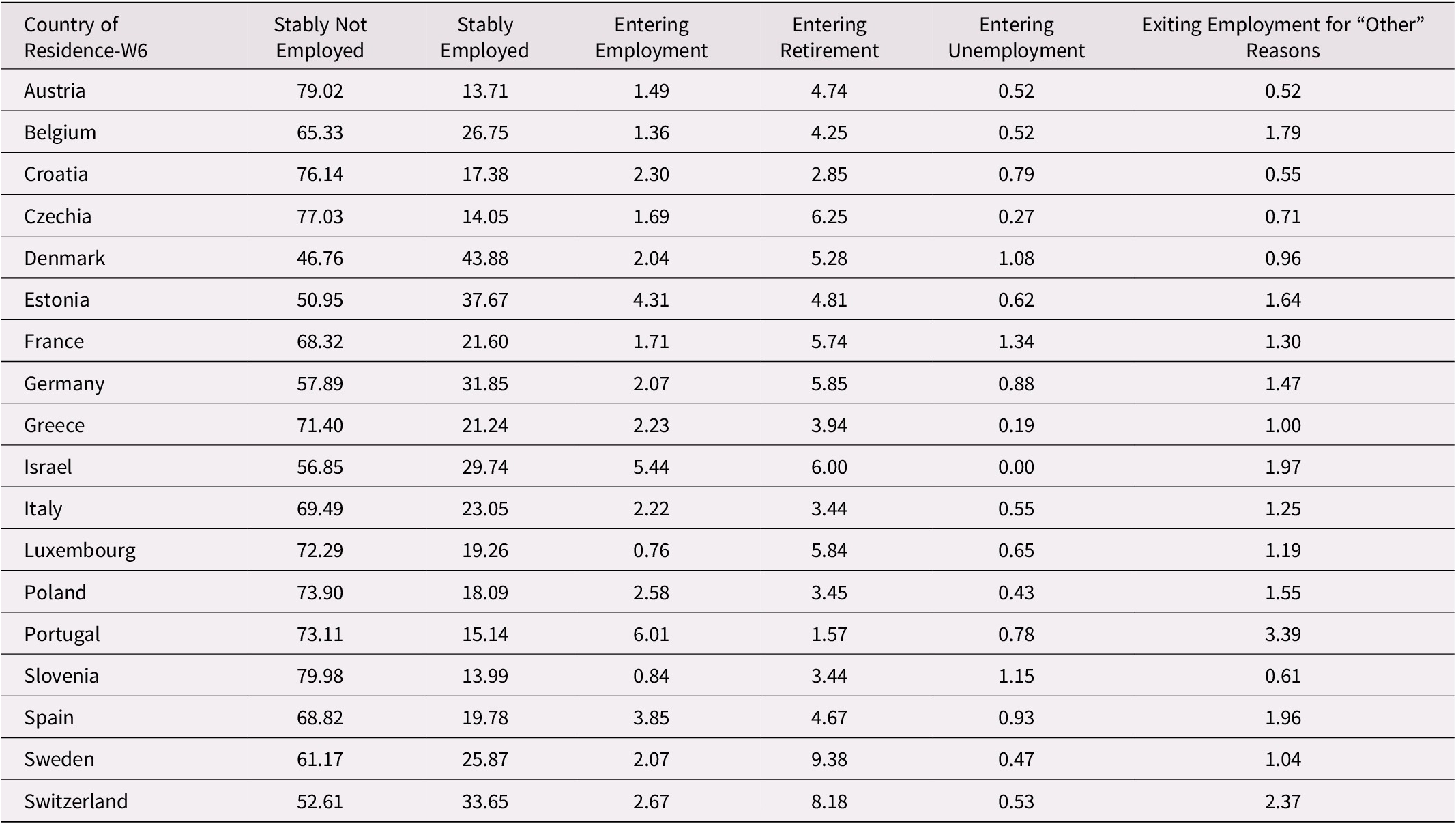
Note. W6 = wave 6.
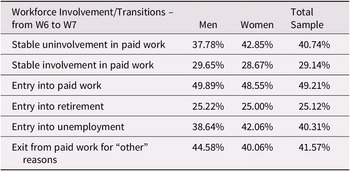
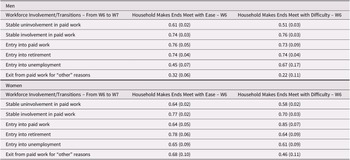
Table 4 presents the percentages reporting at wave six that their households made ends meet with difficulty for each category of workforce involvement/transition (subdivided into men, women, and the total sample). Those who entered paid work had the most difficult financial circumstances (“other” exits from paid work was a close second most difficult). Those who entered retirement had the most advantaged financial circumstances (stable involvement in paid work was a close second most advantaged). Stable uninvolvement in paid work and entry into unemployment were almost equally in the middle. For the most part, gender differences were small. Among those exiting paid work for “other” reasons, women had greater financial ease than men. Among those entering unemployment or stably uninvolved in paid work, women had greater financial difficulty than men.
Table 4. Percentages reporting at wave six that their households make ends meet with difficulty for each category of workforce involvement/transition (n = 38,884)
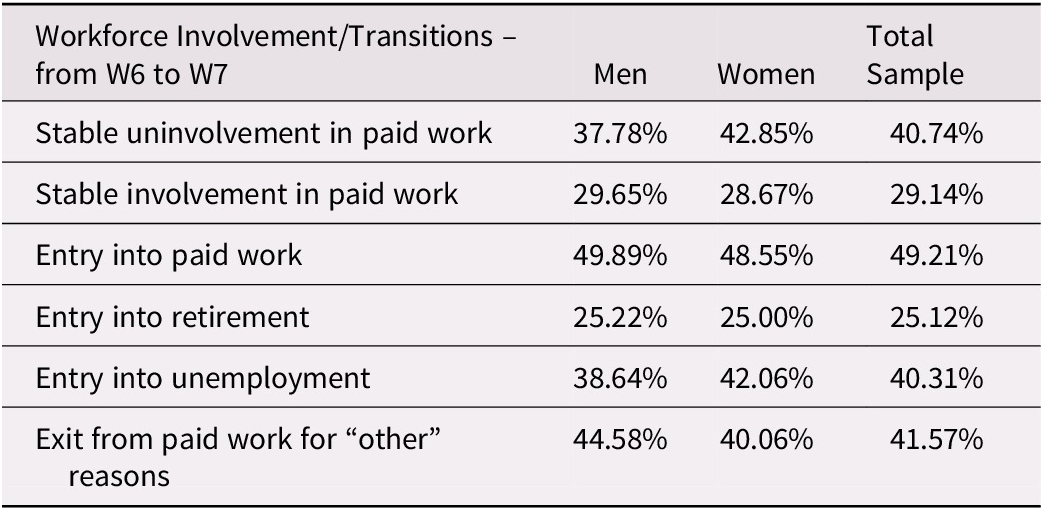
Note. W6 = wave 6; W7 = wave 7.
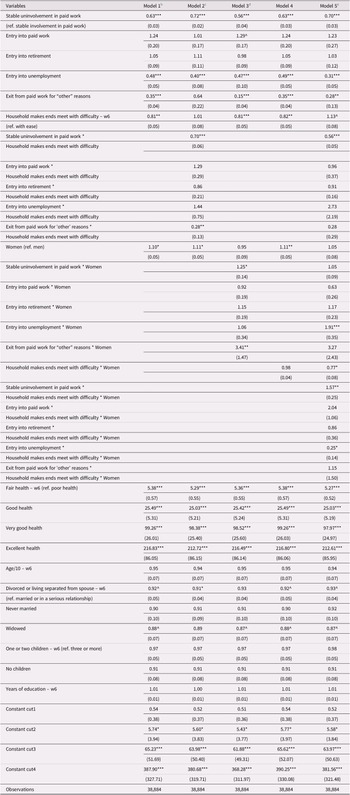
Table 5 presents this study’s central findings, displayed as ORs. Concerning Model 1, a Wald test (F-test) revealed that the workforce involvement/transitions variable made a significant contribution to model fit (p < 0.0001). Those stably not employed showed declining health compared with those stably employed (OR: 0.63, p < 0.001). Similarly, both entering unemployment (OR: 0.48, p < 0.001) and exiting employment for “other” reasons (OR: 0.35, p < 0.001) showed declining health relative to stable employment. A further Wald test (t test) revealed that those entering employment (OR: 1.24) showed improved health (p < 0.001) compared with those stably not employed (OR: 0.63). Moreover, whereas having difficulty making ends meet was associated with worse health (OR: 0.81, p < 0.01), being a woman was associated with less decline in health (OR: 1.10, p < 0.05).
Table 5. Ordinal logistic regression analyses of self-perceived health – wave seven, odds ratios a
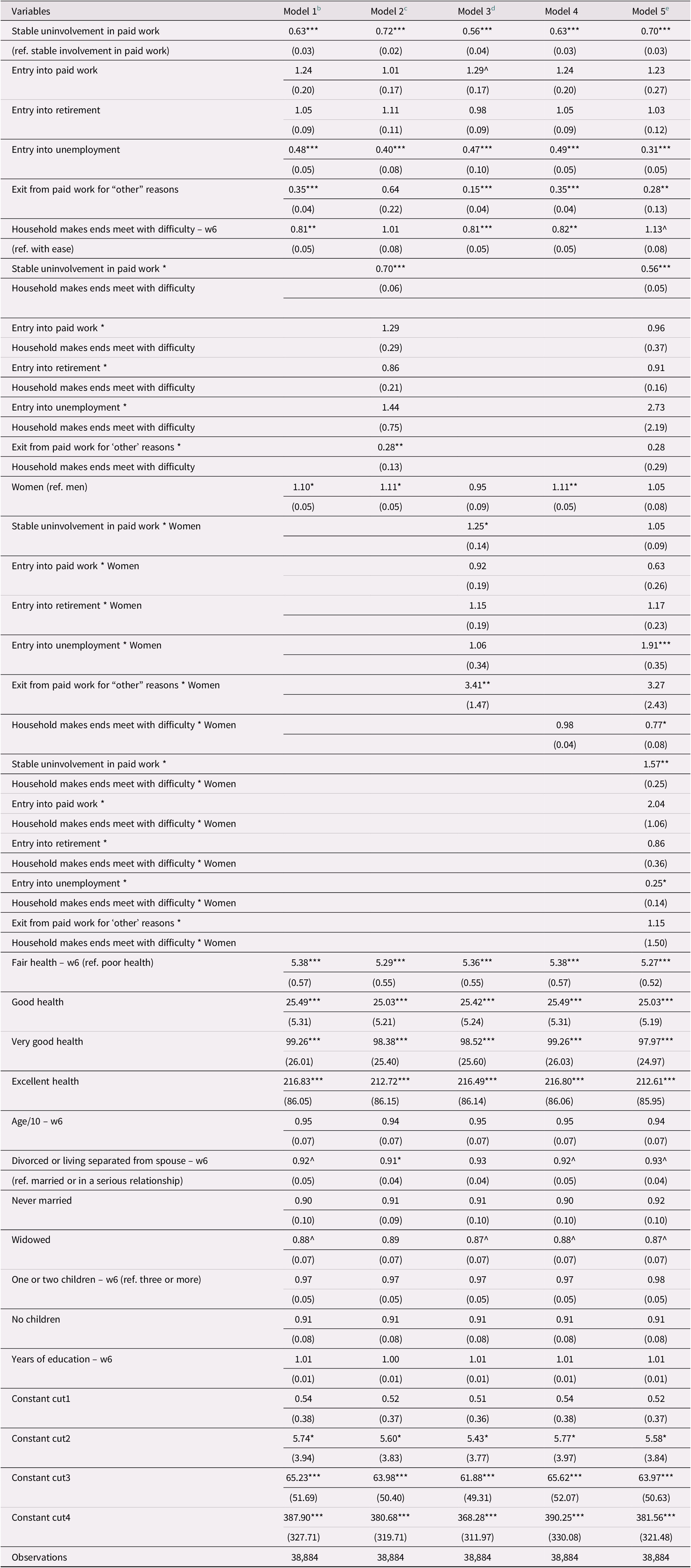
Note. Robust standard errors (exponentiated form) in parentheses. Two-tailed tests ***p < 0.001, **p < 0.01, *p < 0.05, ^p < 0.10.
a By reason of parsimony, the scales of social connectedness and social network satisfaction at w6 were controlled but are not presented; Wald tests revealed that in no models did either of these variables significantly contribute to model fit.
b Wald tests revealed that the workforce involvement/transitions variable made a significant contribution to model fit (p < 0.0001), and that those who entered into paid work showed significantly better health at w7 than those stable in their uninvolvement in paid work (p < 0.001).
c Wald tests revealed that the interaction between workforce involvement/transitions and household’s ability to make ends meet made a significant contribution to model fit (p < 0.0001), and that having difficulty making ends meet significantly accentuated the health benefits of entering into paid work compared with being stable in one’s uninvolvement in paid work (p < 0.05).
d Wald tests revealed that the interaction between workforce involvement/transitions and gender made a significant contribution to model fit (p < 0.0001), and that there was no significant difference between the interaction odds ratios pertaining to those who entered into paid work and those stable in their uninvolvement in paid work.
e Wald tests revealed that the three-way interaction among workforce involvement/transitions, household’s ability to make ends meet, and gender made a significant contribution to model fit (p < 0.001), and that there was no significant difference between the three-way interaction odds ratios pertaining to those who entered into paid work and those stable in their uninvolvement in paid work.
w6 = wave 6; w7 = wave 7.
A Wald test (F-test) revealed that the interaction between workforce involvement/transitions and difficulty making ends meet in Model 2 made a significant contribution to model fit (p < 0.0001). Compared with those stably employed, having difficulty making ends meet implied further disadvantages in health for those stably not employed (two-way interaction OR: 0.70, p < 0.001) and those exiting employment for “other” reasons (two-way interaction OR: 0.28, p < 0.01). A further Wald test (t test) suggested that having difficulty making ends meet significantly accentuated the health benefits (two-way interaction: p < 0.05) of entering employment (two-way interaction OR: 1.29) compared with being stably not employed (two-way interaction OR: 0.70). These interaction results imply that having difficulty making ends meet accentuates the value of 50–75-year-old adults’ employment.
Regarding Model 3, a Wald test (F-test) showed that the interaction between workforce involvement/transitions and gender significantly contributed to model fit (p < 0.0001). For women, compared with those stably employed, there were significant relative advantages to being stably not employed (two-way interaction OR: 1.25, p < 0.05) or exiting employment for “other” reasons (two-way interaction OR: 3.41, p < 0.01). A further Wald test (t test) showed no significant difference between the interaction ORs pertaining to those stably not employed (two-way interaction OR: 1.25) and those who entered employment (two-way interaction OR: 0.92). These results suggest that stable uninvolvement in paid work from 50 to 75 years of age is less detrimental for women than for men. Model 4 showed an insignificant interaction between ability to make ends meet and gender.
Concerning Model 5, a Wald test (F-test) revealed that the three-way interaction among workforce involvement/transitions, ability to make ends meet, and gender significantly contributed to model fit (p < 0.001). For women experiencing difficulty making ends meet, the disadvantage of being stably not employed compared with being stably employed was reduced (three-way interaction OR: 1.57, p < 0.01). Furthermore, these women showed particularly strong detriments to health when entering unemployment compared with being stably employed (three-way interaction OR: 0.25, p < 0.05). An additional Wald test (t test) showed no significant difference between the three-way interaction ORs associated with being stably not employed (three-way interaction OR: 1.57) and entering employment (three-way interaction OR: 2.04). These results revealed that for women 50–75 years of age undergoing financial troubles, stable paid work is less beneficial for health when compared with stable uninvolvement in paid work, although entry into unemployment is especially detrimental to health when compared with stable paid work.
It is further notable that better health at wave six implied better health at wave seven. As for the most part, one’s overall health declines gradually through time, this finding was expected.
The predicted probabilities of reporting “good”, “very good”, or “excellent” health for each of the 24 possible combinations of categories within the three-way interaction term, displayed in Table 6 (subdivided by gender), corroborate the findings in Table 5.
Table 6. Three-way interaction term: probabilities of reporting good, very good, or excellent self-perceived health at wave seven (n = 38,884) a
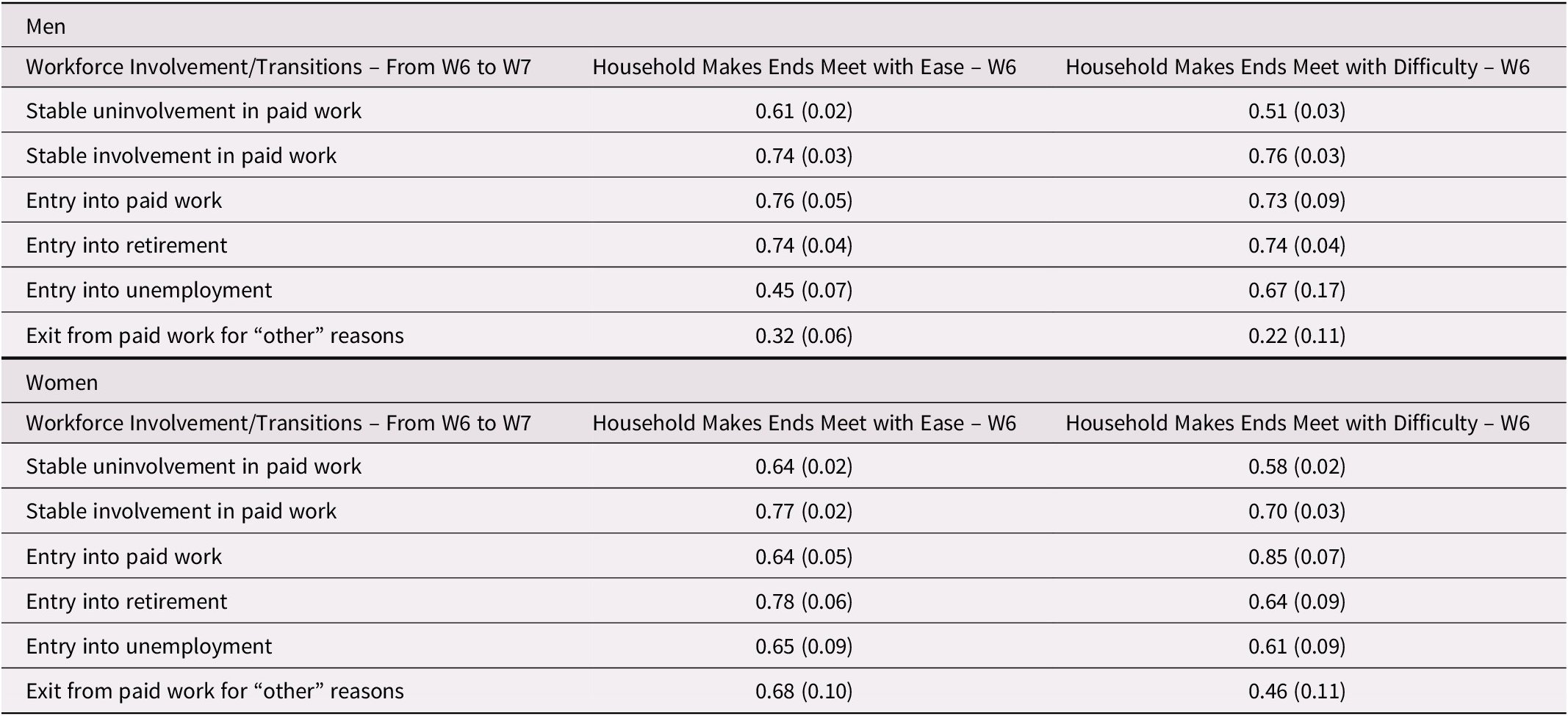
Note.
a Standard errors are in parentheses.
W6 = wave 6; W7 = wave 7.
A robustness check repeated these analyses with country of residence at wave six controlled to account for the many differences among these nations. The results were substantively the same.
Discussion
This study provides answers to all three research questions. It extends beyond most research on workforce involvement among late-middle-aged and senior persons through considering a more comprehensive set of patterns of workforce involvement/transitions. It also improves upon many earlier studies of the health outcomes of workforce involvement/transitions within this age group through use of conditional change panel modelling, which reduces concerns with reverse causation. Moreover, two important interactants are investigated.
Concerning the first question, “are employment and transition into employment beneficial for 50 to 75-year-old persons’ health?” the findings support the second hypothesis, “employment from 50 to 75 years of age is beneficial for health because it helps maintain salubrious amounts of physical, cognitive, and social activity”. In accordance with the activity theory of aging, this study finds advantages for those stably employed and those entering employment, as well as disadvantages for those entering unemployment or exiting employment for “other” reasons, with financial difficulties controlled. This implies benefits of paid work among 50–75-year-old respondents with and without financial difficulties.
Some of the motivating circumstances for early retirement, including health problems and difficult work circumstances (including regular physical strains) (de Wind et al., Reference de Wind, Geuskens, Ybema, Bongers and van der Beek2015; van den Berg et al., Reference Van Den Berg, Elders and Burdorf2010), might indicate health benefits to uninvolvement in paid work for some late-middle-aged and senior persons. This study’s results suggest that some of the benefits of the social and cognitive activity involved in employment might accrue also to those late-middle-aged and senior adults whose circumstances lead them to prefer early retirement. Nonetheless, documented motivations for early retirement encourage further study of heterogeneity in how workforce involvement/transitions affect various health and quality of life outcomes.
Regarding the second question, “does financial difficulty increase or decrease the health benefits of employment among those of 50 to 75 years of age?” the results correspond with the first hypothesis, “financial difficulties among those of 50 to 75 years of age increase the health benefits of employment as it helps improve financial circumstances”. While having difficulty making ends meet increases the disadvantages of stable uninvolvement in paid work and exit from employment for “other” reasons, it raises the advantages of entering employment. Despite the fact that 50–75-year-old persons without financial difficulties are more likely to be of higher social status and to work voluntarily in higher quality jobs (as per the theory of cumulative advantage/disadvantage), employment in this age group is especially beneficial for those desiring to improve their troubled economic conditions.
Concerning the third question, “is there heterogeneity by gender in how financial difficulties interact with workforce involvement/transitions in affecting the health of adults from 50 to 75 years of age?” the results are consonant with the second hypothesis, “intersectionality between ageism and sexism, combined with the disadvantaged workforce trajectories of many present-day women from 50 to 75 years of age, suggest that there is heterogeneity by gender in how current financial challenges interact with workforce involvement/transitions in affecting health.” Contrasted with their male counterparts, women from 50 to 75 years of age experiencing difficulty making ends meet profit less from stable employment when compared with stable uninvolvement in paid work, but suffer worse consequences when entering unemployment when compared with being stably employed. Because these women came of age when the women’s liberation movement was at an early stage, many have had fragmented work histories (Davis, Reference Davis2003; Quinn & Kozy, Reference Quinn and Kozy1996) in lower quality jobs marked by gender segregation and discrimination (Perkins, Reference Perkins1994). Their stable employment from 50 to 75 years of age is therefore likely to be of lower quality and pay, reducing its effectiveness for managing household financial difficulties. Furthermore, a 50–75-year-old woman entering unemployment while undergoing difficulty making ends meet is likely to be pessimistic about her chances of finding satisfactory employment that can alleviate her household’s financial difficulties. Therefore, the theory of cumulative advantage/disadvantage can explain these findings.
This heterogeneity by gender might seem to conflict with the main effects of gender in Models 1, 2, and 4 of Table 5 (women undergo less decline in health through time). Beyond the conceptual distinctions between main and interaction effects, this study’s conditional change panel modelling implies that the wave seven health outcome denotes changes in health between waves six and seven (Finkel, Reference Finkel1995). The main effects of gender in Models 1, 2, and 4 can therefore be interpreted through the female–male health–survival paradox, according to which women have longer life expectancies than men do while experiencing more disability across the life course (Van Oyen et al., Reference Van Oyen, Nusselder, Jagger, Kolip, Cambois and Robine2013). Whereas the former increases women’s healthy life years, the latter reduces them (Van Oyen et al., Reference Van Oyen, Nusselder, Jagger, Kolip, Cambois and Robine2013). This study largely adjusts for the latter through controlling for health at wave six. Because of their longer lifespans, women have more healthy life years than men do in most European countries (Van Oyen et al., Reference Van Oyen, Nusselder, Jagger, Kolip, Cambois and Robine2013), suggesting that aging by 2 years (from wave six [2015] to wave seven [2017]) during the late middle-age and senior years is associated with worse health declines among men than among women.
The two-way interaction between workforce involvement/transitions and gender shows women profiting less than men do from stable employment while being less negatively affected by exits from employment for “other” reasons. Especially for 50–75-year-old women who came of age during more sexist times, prevalent gender norms suggest that paid work is primarily a man’s domain, while a woman’s efforts should focus on the home and family (Blair-Loy, Reference Blair-Loy2003). Stable uninvolvement in paid work might therefore be less detrimental to 50–75-year-old women’s health. Similarly, it might be more socially acceptable for a woman in this age group to exit employment because of disability or to be a homemaker (Blair-Loy, Reference Blair-Loy2003), implying fewer negative consequences for health.
Entry into retirement did not show any significant associations with health in this study. However, a substantial majority of those stably not employed in this study reported being retired at either or both of waves six and seven. The health disadvantages for those stably not employed here revealed (main and interaction effects) thus concord with scholarship suggesting that the health detriments of retirement might only appear after a substantial amount of time (Kuhn, Reference Kuhn2018).
Through uncovering these relationships within a sample including 18 European countries, this study’s findings are broadly applicable throughout Europe. The fact that the robustness check with country of residence at wave six controlled produced substantively the same results reinforces this claim of broad applicability across Europe.
Policy Recommendations
This study’s findings of positive associations between employment from 50 to 75 years of age and health suggest that societal efforts should facilitate this age group’s employment. These efforts should include overcoming ageism in the labour market (see McMullin & Duerden Comeau, Reference McMullin, Duerden Comeau and McMullin2011) and developing retraining programs that update late-middle-aged and senior adults’ labour-market-relevant skills and knowledge. Scholars have recommended more adaptable workplace policies and practices that afford late-middle-aged and senior persons freedom in deciding the content and scheduling of their work activities (Denton & Spencer, Reference Denton and Spencer2009).
These efforts are especially important for late-middle-aged and senior persons undergoing financial difficulties. They should therefore focus on those with less education, with more fragmented employment trajectories, and in more troubled financial circumstances. Furthermore, the remuneration of this age group’s employment should safeguard their households’ ability to make ends meet.
Moreover, policies and programs should prioritize helping late-middle-aged and senior women with their paid work circumstances. The combination of ageism, sexism, and fragmented work histories imply that women in this age group in difficult financial circumstances face obstacles as they seek high quality and well-paying employment. These disadvantages are especially consequential for those, including widows, who are their households’ sole breadwinners.
The implications of the theory of cumulative advantage/disadvantage for the relationships here studied lead to further policy recommendations. Public policies should aim to achieve gender and income equity throughout the life course. This equity over the lifespan will result in more equal socio-economic and health trajectories of members of the same cohort as they age. Accordingly, future generations of late-middle-aged and senior persons will profit from fewer health inequities and disparities.
Limitations and Paths for Future Research
There are advantages and limitations to using self-assessed “household’s ability to make ends meet” as an interactant. This measure’s subjectivity is a potential concern. Adults of all ages vary in their general optimism and pessimism, as well as in their perceptions of an agreeable standard of living. These variations imply that two persons in the same objective financial circumstances might differ in their appraisals of their households’ ability to make ends meet. Nonetheless, objective financial circumstances are powerful predictors of this subjective assessment in later life (Litwin & Sapir, Reference Litwin and Sapir2009). Furthermore, this subjective self-appraisal is strongly predictive of health and quality of life (Conde-Sala, Portellano-Ortiz, Calvó-Perxas, & Garre-Olmo, Reference Conde-Sala, Portellano-Ortiz, Calvó-Perxas and Garre-Olmo2017; Hank & Schaan, Reference Hank and Schaan2008). Because this study investigates influences on a self-appraisal of overall physical and mental health, a subjective assessment that captures how respondents feel about their households’ financial circumstances is advantageous.
Because this study’s focus is the short-term associations between workforce transitions and health changes, it employs a time span of 2 years. Other scholars have found substantial health changes over a 2-year span of time (e.g., Buckley, Denton, Robb, & Spencer, Reference Buckley, Denton, Robb and Spencer2006; Stafford, Nazroo, Popay, & Whitehead, Reference Stafford, Nazroo, Popay and Whitehead2008). Scholarship connecting mental and physical health (e.g., Nabi, Kivimaki, De Vogli, Marmot, & Singh-Manoux, Reference Nabi, Kivimaki, De Vogli, Marmot and Singh-Manoux2008; Ohrnberger, Fichera, & Sutton, Reference Ohrnberger, Fichera and Sutton2017) supports the adequateness of this time span. This time span is especially sufficient for late-middle-aged and senior samples with more fragile health. However, replication of this study with a longer time span will help reveal the full associations of workforce transitions with health during the late middle-age and senior years.
One limitation is that this study does not consider specific features of respondents’ employment, such as employed versus self-employed work, which are likely to vary in their associations with health. To control for features of paid work in this study’s regression models would block potential mechanisms between the interaction terms and health outcomes. As such, effectively including features of employment in this study would require additional interaction analyses, and is therefore beyond this study’s scope. Nonetheless, studying the associations with health of specific characteristics of late-middle-aged and senior adults’ paid work is a fruitful path for future research.
More broadly, although it is beyond this study’s scope, further interaction analyses based on many aspects of late-middle-aged and senior persons’ health and well-being, as well as life, work, and financial circumstances would make valuable contributions to the literature. These analyses are encouraged by research that has identified a wide range of motivators for early retirement (de Wind et al., Reference de Wind, Geuskens, Ybema, Blatter, Burdorf and Bongers2014, Reference de Wind, Geuskens, Ybema, Bongers and van der Beek2015; Silver et al., Reference Silver, Settels, Schafer and Schieman2019; van den Berg et al., Reference Van Den Berg, Elders and Burdorf2010).
For example, although this study addresses the financial circumstances within which workforce transitions occur, future research should analyze heterogeneity based on workforce transitions’ financial consequences. Additionally, although marital/relationship status was here controlled, future scholarship should investigate interactions with marital/relationship circumstances and the employment status of one’s partner. Whether a respondent has a partner providing an additional income and/or sharing the household’s financial burdens likely influences the relationships here examined.
Another limitation of this study is that health shocks between waves six and seven could have potentially influenced workforce transitions. However, it is likely that this reverse causality pertained only to entry into retirement (no significant findings) and exits from employment for “other” reasons. Although those stably not employed (a substantial majority of whom were retired at either or both waves) did not undergo transitions, those entering unemployment were seeking out employment at wave seven, making it improbable that a health shock caused them to exit work. Those exiting employment for “other” reasons possibly showed worse health in Model 1 because a health shock caused this transition. The compounding of this health shock with financial difficulties might have intensified these health declines (Model 2). Concerning Model 3, 50–75-year-old men might be more likely than women of this age group to exit employment for “other” reasons because of a health shock. This potentially explains the stronger association between this workforce transition and health decline among men. These alternative explanations should be kept in mind.
Finally, future research might address how these associations vary across countries and welfare regimes; a comparative analysis such as this is beyond this study’s scope. Although the age span chosen, 50–75 years of age, brackets the typical retirement ages of all countries in the sample, demographic, policy, socio-economic, and labour market differences between countries might influence the associations here studied. Tables 1 and 3 depict some of these differences. Although this study’s findings are broadly applicable to the European context, future comparative research should analyze national variations.
Acknowledgment
This research was supported by the 2020 Research Block Grant Allocation Scheme-Merit Based Funding Scheme: Incentive B, Faculty of Humanities, Education and Social Sciences, University of Luxembourg. This funding source had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the article; or in the decision to submit it for publication.
No ethical approval was required as this is a secondary analysis of data gathered by a third party.
This article uses data from SHARE Wave 6 (DOI: 10.6103/SHARE.w6.700), see Börsch-Supan et al. (2013) for methodological details.
The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001–00360), FP6 (SHARE-I3: RII-CT-2006–062193, COMPARE: CIT5-CT-2005–028857, SHARELIFE: CIT4-CT-2006–028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782) and by DG Employment, Social Affairs & Inclusion though VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the United States National Institute on Aging (U01_AG09740–13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553–01, IAG_BSR06–11, OGHA_04–064, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
This article uses data from the generated easySHARE data set (DOI: 10.6103/SHARE.easy.700), see Gruber et al. (2014) for methodological details. The easySHARE release 7.0.0 is based on SHARE Waves 1, 2, 3, 4, 5, 6 and 7 (DOIs: 10.6103/SHARE.w1.700, 10.6103/SHARE.w2.700, 10.6103/SHARE.w3.700, 10.6103/SHARE.w4.700, 10.6103/SHARE.w5.700, 10.6103/SHARE.w6.700, 10.6103/SHARE.w7.700).


 Open access
Open access