


Obsessions and compulsions commonly occur in the post-streptococcal movement disorders Sydenham's chorea and paediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (Reference Swedo, Leonard and GarveySwedo et al, 1998; Reference Mercadante, Busatto and LombrosoMercadante et al, 2000). These disorders are thought to be autoimmune in origin, in that antibodies raised in response to streptococcus cross-react with the basal ganglia. We have recently described serum anti-brain antibodies that bind to basal ganglia proteins in patients with post-streptococcal brain syndromes (Church et al, Reference Church, Cardoso and Dale2002, Reference Church, Dale and Cardoso2003a ; Reference Dale, Church and SurteesDale et al, 2004). The recognition that obsessions and compulsions may occur after streptococcal infection has led to the hypothesis that a subgroup of obsessive–compulsive disorder might be secondary to post-streptococcal autoimmunity. We tested this hypothesis by measuring antibasal ganglia antibodies in a cohort of unselected individuals with obsessive–compulsive disorder, and comparing the findings with paediatric control groups.
METHOD
Patients
Fifty children and adolescents with obsessive–compulsive disorder were recruited from a specialist clinic between August 2001 and August 2002. Ethics approval was granted by the local committee. Consecutive patients were screened for probable obsessive–compulsive disorder before attending the clinic, and all underwent a detailed clinical assessment by child psychiatrists and psychologists. All those meeting DSM–IV criteria for the disorder (American Psychiatric Association, 1994) were invited to participate in the study. All patients were assessed with a structured diagnostic interview, the Children's Yale–Brown Obsessive Compulsive Scale (CY–BOCS; Reference Scahill, Riddle and McSwiggin-HardinScahill et al, 1997), at the time of serological examination (mean score 19.5, range 5–33). The symptom characteristics of the total cohort are presented in Table 1, including medication status (56% of the sample). Patients were taking paroxetine (n=9), fluoxetine (n=7), sertraline (n=9) or clomipramine (n= 3) at the time of sampling. The mean age at symptom onset (retrospectively) was 8.9 years and the mean age at the time of assessment was 13.0 years (range 6–16). After complete description of the study to the participants, written informed consent was obtained from the family.
Table 1 Clinical characteristics of our sample of children with obsessive–compulsive disorder: comparison of groups testing positive or negative for anti-basal ganglia antibodies on western immunoblotting

| Characteristic | Total OCD cohort | ABGA positive | ABGA negative | P 1 |
|---|---|---|---|---|
| Number of patients | 50 | 21 | 29 | |
| Age at onset, years: mean | 8.9 | 9.2 | 8.6 | NS |
| Age at assessment, years: mean | 13.0 | 12.4 | 13.7 | NS |
| Male, % | 60 | 62 | 57 | NS |
| CY—BOCS score: mean | 19.5 | 16.4 | 21.6 | <0.001 |
| Obsessions, % | ||||
| Contamination | 64 | 62 | 66 | NS |
| Aggressive | 64 | 48 | 76 | NS |
| Sexual | 18 | 14 | 21 | NS |
| Hoarding/saving | 16 | 0 | 28 | <0.05 |
| Magical thoughts/superstitions | 30 | 24 | 35 | NS |
| Somatic | 26 | 24 | 28 | NS |
| Religious | 22 | 14 | 28 | NS |
| Miscellaneous | 48 | 38 | 55 | NS |
| Compulsions, % | ||||
| Washing/cleaning | 68 | 71 | 66 | NS |
| Checking | 70 | 57 | 79 | NS |
| Repeating | 70 | 76 | 66 | NS |
| Counting | 56 | 62 | 52 | NS |
| Ordering/arranging | 50 | 33 | 62 | NS |
| Hoarding/saving | 32 | 24 | 38 | NS |
| Excessive games/superstitions | 26 | 24 | 28 | NS |
| Rituals involving other people | 38 | 29 | 45 | NS |
| Miscellaneous | 64 | 67 | 62 | NS |
| Other clinical characteristics, % | ||||
| Tics | 32 | 43 | 24 | NS |
| Tourette syndrome | 16 | 29 | 7 | <0.05 |
| Major depression | 8 | 10 | 7 | NS |
| Separation anxiety | 2 | 5 | 0 | NS |
| Generalised anxiety | 8 | 10 | 7 | NS |
| Phobia | 6 | 14 | 0 | NS |
| ADHD | 18 | 19 | 17 | NS |
| ODD | 4 | 0 | 7 | NS |
| Family history of obsessions/compulsions2 | 36 | 38 | 35 | NS |
| Family history of tics2 | 4 | 5 | 3 | NS |
| Anti-streptolysin O titre >200 IU/ml, % | 44 | 62 | 31 | <0.05 |
| Drug treatment at assessment | 56 | 48 | 62 | NS |
Controls
For comparison in the serological study, we recruited paediatric control groups: a neurological control group with stroke, metabolic movement disorders and encephalitis (n=100, mean age 8.2 years, range 1–16 years, 50 males); a group with uncomplicated streptococcal infections, defined as laboratory-confirmed streptococcal pharyngitis without autoimmune or invasive complications (n=40, mean age 9.8 years, range 2–15 years, 25 males); and a third group of children with autoimmune disorders without neurological involvement, including rheumatic carditis and post-streptococcal glomerulonephritis (n=50, mean age 9.2 years, range 2–16 years, 25 males). Some of these control groups had been previously reported (Reference Church, Dale and LeesChurch et al, 2003b ). The control groups were recruited during the same period as the obsessive–compulsive disorder cohort (between August 2001 and August 2002).
Serology
All serum samples were coded and stored at –80 °C prior to streptococcal serological investigation, in which anti-streptolysin O titres were measured using the Dade Behring BN II nephelometer (http://www.dadebehring.com). All control group levels were within acceptable parameters. Titres greater than 200 IU/ml were considered significant according to World Health Organization guidelines (Reference Spaun, Bentzon and Olesen LarsenSpaun et al, 1961). Streptococcal serological measurements took place in a different laboratory from the other tests, with investigators masked to the anti-basal ganglia antibody results.
The methods for assaying anti-basal ganglia antibodies have been described by Church et al (Reference Church, Cardoso and Dale2002). All participants in the patient and control groups had their antibody levels measured using both enzyme-linked immunosorbent assay (ELISA) and western blotting (all assays were performed by A.J.C.). The former technique gives a semi-quantitative measurement of antibody binding to antigens, whereas western blotting can define specific antibody–antigen interactions. For both assays, the antigen was homogenised delipidated human basal ganglia (caudate and putamen). Human immunoglobulin G (IgG) was first removed from the homogenised antigen using Protein A. Samples from patients and controls were coded and assayed at the same time on the same ELISA plates and western blots. A 96-well ELISA plate was incubated with basal ganglia homogenate overnight. The plate was then blocked with 2% bovine specific albumin, and washed with normal saline (0.9% sodium chloride) with 0.2% milk proteins and 0.025% Tween. Duplicate serum samples were diluted 1:300 and incubated for 1 h. After washing, 1:1000 rabbit anti-human IgG conjugated with horseradish peroxidase (Dako, Glostrup, Denmark) was incubated for a further hour. After washing, the plate was developed with the reagent o-phenylenediamine for 15 min and stopped with 1 mol/l hydrochloric acid. A known positive and negative control was used on all ELISA plates. For western blotting, the basal ganglia homogenate was mixed with lithium dodecyl sulphate and 0.05 mol/l dithiothreitol and heated at 65 °C for 15 min; 30 μg of protein was loaded onto a 4–12% Bis–Tris gel and subjected to electrophoresis. The gel was transferred to nitrocellulose (BioRad, Hemel Hempstead, UK) and the proteins blocked with 2% milk proteins. The blot was loaded onto a manifold and serum samples diluted 1:300 were incubated overnight. Samples were washed with normal saline with 0.2% milk proteins and 0.025% Tween. The secondary antibody (rabbit anti-human IgG conjugated with horse-radish peroxidase) was diluted 1:1000 and incubated for 2 h. The blot was then washed again and developed with substrate 4-chloro-1-naphthol for 15 min. A positive western blot result was reported when there was discrete antibody–antigen binding demonstrated on colorimetric detection. Positive antibody binding was compared with the previously reported findings in Sydenham's chorea (Reference Church, Cardoso and DaleChurch et al, 2002).
Statistics
All statistical tests were performed using the Statistical Package for the Social Sciences version 12. The distribution of the ELISA data was positively skewed, therefore the planned comparisons between the obsessive–compulsive disorder patient cohort and the control cohorts were made with Mann–Whitney tests. Western blotting antibody positivity was compared using the chi-squared test. Clinical characteristics of patients testing positive and negative for anti-basal ganglia antibodies were compared using chi-squared tests.
RESULTS
A summary of results is presented in Table 2. The mean anti-basal ganglia antibody ELISA absorbance in the obsessive–compulsive disorder cohort was elevated compared with the control groups (P<0.005 in all comparisons). Likewise, the presence of anti-basal ganglia antibodies on western immunoblotting was significantly more common in the patient cohort compared with all controls (P<0.001 in all comparisons). Almost two-thirds (64%) of the patient cohort with positive findings on western blotting had an ELISA level above 0.33 – the previously proposed cut-off level (Reference Church, Cardoso and DaleChurch et al, 2002) – compared with 7% of the patient group with negative western blotting. In the patient cohort, rather than polyspecific binding using western blotting, there was antibody binding to discrete basal ganglia antigens of molecular weight 40 (n=12), 45 (n=9) and 60 (n=9). An example of a patient and a control western blot is presented in Fig. 1. Fourteen of the 21 samples testing positive for anti-basal ganglia antibodies had binding to one of these basal ganglia antigens, whereas the other seven had binding to two or three of these autoantigens. These antibody–antigen binding patterns are similar to those previously reported in Sydenham's chorea (Reference Church, Cardoso and DaleChurch et al, 2002). There was other binding in the patient cohort samples to antigens of unclear significance: 30 kDa, 35 kDa, 42 kDa and 67 kDa (all n=1), and 95 kDa and 98 kDa (n=2). The clinical characteristics of the patients who tested positive for anti-basal anti-basal ganglia antibodies were compared with those who were negative for these antibodies (see Table 1). The antibody-positive patients were more likely to have comorbid Tourette syndrome and raised anti-streptolysin O titres. The antibody-negative patients had a higher mean CY–BOCS score and hoarding/saving obsessions. There was no other statistically significant difference.
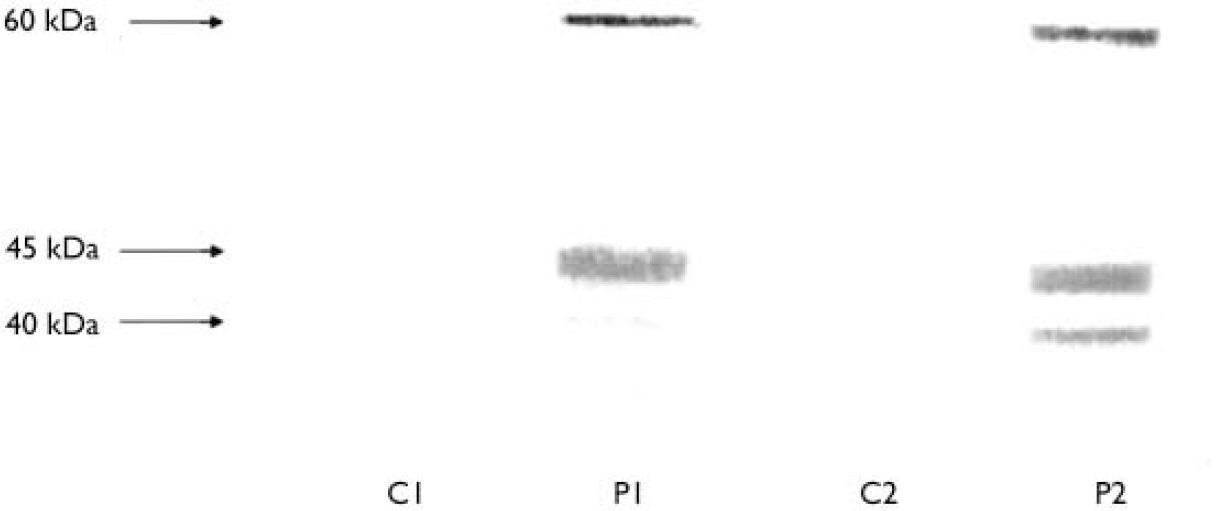
Fig. 1 A representative western blot of two patients with obsessive–compulsive disorder positive for anti-basal ganglia antibody (P1 and P2) and two controls (C1 and C2).
Table 2 Immunological findings in the obsessive–compulsive cohort compared with control groups

| Assay | OCD patients (n=50) | Neurology controls (n=100) | Streptococcal controls (n=40) | Autoimmune controls (n=50) |
|---|---|---|---|---|
| ELISA | ||||
| Mean ABGA binding (95% CI) | 0.3051 (0.284-0.326) | 0.229 (0.207-0.251) | 0.189 (0.171-0.207) | 0.251 (0.2-0.302) |
| Western blotting | ||||
| Positive for ABGA (%) | 422 | 4 | 2 | 10 |
DISCUSSION
Neurobiology of obsessive–compulsive disorder
Obsessive–compulsive disorder is characterised by intrusive, repetitive and distressing thoughts or images (obsessions), and repetitive or ritualistic actions (compulsions) (Reference SteinStein, 2002). Over the past few decades, convergent evidence from genetics, neuroimaging and pharmacology points towards a neuropsychiatric basis for this disorder, involving specific brain regions – particularly the orbitofrontal cortex and basal ganglia. The association of obsessive–compulsive disorder with extrapyramidal movement disorders such as Tourette syndrome, Huntington's disease, Parkinson's disease and Sydenham's chorea further strengthens the neuroanatomical association with the basal ganglia (Reference SteinStein, 2002). A genetic vulnerability seems important in disease expression of obsessive–compulsive disorder, given the high incidence of the condition and of tic disorders in family members (Reference Pauls, Alsobrook and GoodmanPauls et al, 1995). Although a number of genetic polymorphisms involved in neurotransmission have been implicated in some study cohorts, there is no unifying genetic locus. It is therefore proposed that disease expression is multifactorial, requiring both a genetic predisposition and an environmental trigger. It is also possible that there are subgroups within ‘idiopathic’ disorder cohorts with differing neurological or psychological factors resulting in the syndrome termed ‘obsessive–compulsive disorder’.
Obsessive–compulsive disorder after infectious disease
Further evidence for specific brain mechanisms in obsessive–compulsive disorder is the long-recognised association between this disorder and infection or immunemediated central nervous system disease. For example, obsessive–compulsive behaviours were reported in patients with encephalitis lethargica during the 1916–1927 epidemic, although parkinsonism was the most striking clinical feature (Reference Von Economo and NewmanVon Economo, 1931). The pathological abnormalities of encephalitis lethargica were inflammatory infiltrates that were relatively localised to the basal ganglia, leading to early speculation that obsessive–compulsive disorder could occur secondary to basal ganglia dysfunction (Reference Von Economo and NewmanVon Economo, 1931).
Another infection-mediated cause of secondary obsessive–compulsive disorder is Sydenham's chorea, a latent manifestation of group A streptococcal infection. Psychiatric studies using operationalised criteria have revealed that obsessive–compulsive symptoms are common in Sydenham's chorea (Reference Mercadante, Busatto and LombrosoMercadante et al, 2000) and are even more evident in chronic or relapsing disease (Reference Asbahr, Ramos and NegraoAsbahr et al, 1999). Like encephalitis lethargica, Sydenham's chorea is characterised by an inflammatory infiltrate, predominantly of the basal ganglia (Reference Von Economo and NewmanVon Economo, 1931). Furthermore, recent magnetic resonance volumetric measurement of brain regions demonstrated specific volumetric enlargement of the basal ganglia in patients with Sydenham's chorea, although conventional magnetic resonance images are normal (Reference Giedd, Rapoport and KruesiGiedd et al, 1995).
In the late 1980s an apparently new post-streptococcal neuropsychiatric phenotype was recognised: motor tics and/or obsessive–compulsive disorder (Reference Swedo, Leonard and GarveySwedo et al, 1998). The syndrome was named ‘paediatric autoimmune neuropsychiatric disorders associated with streptococcal infections’ (PANDAS), and was characterised by an abrupt onset of symptoms after streptococcal infection, with a relapsing course associated with further infections (Reference Swedo, Leonard and GarveySwedo et al, 1998). The recognition of the PANDAS phenotype has led to speculation that post-streptococcal autoimmunity might play a contributory part in a subgroup of ‘idiopathic’ tic disorders and obsessive–compulsive disorder. The PANDAS concept and the role of autoimmunity in movement and psychiatric disorders (including Tourette syndrome) remain controversial (Reference Kurlan and KaplanKurlan & Kaplan, 2004; Reference Swedo, Leonard and RapoportSwedo et al, 2004).
Immunopathogenesis of post-streptococcal brain disease
The favoured hypothesis regarding Sydenham's chorea and PANDAS pathogenesis states that an immune response raised against group A streptococcus cross-reacts with brain proteins owing to similarity in the antigens, a concept called molecular mimicry. To date, most investigators have focused on cross-reactive anti-neuronal antibodies as possible mediators of disease, although T cells may also be involved (Reference Husby, van de Rijn and ZabriskieHusby et al, 1976; Reference Kiessling, Marcotte and CulpepperKiessling et al, 1993; Reference Church, Cardoso and DaleChurch et al, 2002). Antibodies against human basal ganglia and brain antigens are more common in Sydenham's chorea (Reference Husby, van de Rijn and ZabriskieHusby et al, 1976; Church et al, Reference Church, Cardoso and Dale2002, Reference Church, Dale and Cardoso2003a ) and other post-streptococcal movement disorders compared with controls (Reference Dale, Church and SurteesDale et al, 2004). Using western immunoblotting in two cohorts with Sydenham's chorea and post-streptococcal parkin-sonism respectively, we have previously proposed that a conserved group of neuronal antigens are involved in antibody binding, of molecular weights 40, 45 and 60 (Church et al, Reference Church, Cardoso and Dale2002, Reference Church, Dale and Cardoso2003a ; Reference Dale, Church and SurteesDale et al, 2004). We have demonstrated that the 45 kDa protein exists as a doublet. The 40 kDa, 60 kDa and one of the 45 kDa bands are brain-specific (Reference Dale, Church and SurteesDale et al, 2004). Limitations of western blotting and ELISA include the fact that both techniques alter the conformation of the antigens and could therefore affect antibody–antigen interaction. It would be preferable to use the specific autoantigens in their physiological state. We are currently attempting to identify these antigens. A separate group have found similar antibody findings (using immunofluorescence rather than western immunoblotting) in individuals with motor tics in association with streptococcal infection (Reference Kiessling, Marcotte and CulpepperKiessling et al, 1993). Pathogenic effect of the antibodies in Sydenham's chorea and PANDAS has been inferred by the induction of disease in animals after PANDAS antibody (IgG) infusion (Reference Hallett, Harling-Berg and KnopfHallett et al, 2000) and symptom reduction after immunotherapies that remove IgG (Reference Perlmutter, Leitman and GarveyPerlmutter et al, 1999).
An interesting recent development is the demonstration of an antibody in people with Sydenham's chorea that cross-reacts with lysoganglioside (a neuronal cell surface molecule), resulting in altered neuronal cell signalling (Reference Kirvan, Swedo and HeuserKirvan et al, 2003). Identifying the 40 kDa, 45 kDa and 60 kDa autoantigens to see whether they are related to lysoganglioside or represent other neuronal markers will further our understanding of the possible role of autoimmunity in movement and neuropsychiatric disorders. Possible mechanisms of antibody action could include upregulation (Reference Kirvan, Swedo and HeuserKirvan et al, 2003) or downregulation of neuronal metabolism or cell signalling.
Role of post-streptococcal autoimmunity in obsessive–compulsive disorder
We report here that 42% of patients with obsessive–compulsive disorder (a consecutive cohort of children and adolescents attending a specialist clinic) had circulating anti-basal antibodies. This is a highly significant finding, as these antibodies are uncommonly found in the control groups studied. In contrast, patients with the neurological disorder most robustly established as a post-streptococcal autoimmune disorder – Sydenham's chorea – almost always test positive for these antibodies using the same assays (Reference Church, Cardoso and DaleChurch et al, 2002). These findings demonstrate that a subgroup of people with obsessive–compulsive disorder have antibody findings similar to those seen in Sydenham's chorea, suggesting that autoimmunity many have a role in the genesis and/or maintenance of the former disorder. Only a few other studies have looked for anti-neuronal antibodies in obsessive–compulsive disorder. An indirect immunofluorescence method has been used in one small study of idiopathic disease, and did demonstrate increased brain antibody binding in the group with the disorder (Reference Kiessling, Marcotte and CulpepperKiessling et al, 1994). Two other studies found no evidence of anti-neuronal autoantibodies in people with the disorder (Reference Murphy, Goodman and FudgeMurphy et al, 1997; Reference Hoekstra, Horst and LimburgHoekstra et al, 2003). These discre-pancies in autoantibody findings in different study cohorts could be due to different methods of antigen preparation (e.g. delipidation, used in methods described here) or antibody detection (colorimetric v. enhanced chemiluminescence). The detection method is particularly important, as sensitive techniques such as enhanced chemiluminescence can pick up low titres of clinically insignificant antibodies in healthy people. We use colorimetric detection, which we believe has reduced sensitivity but improved specificity. Although the presence of anti-neuronal antibodies is important in establishing a possible autoimmune aetiology in obsessive–compulsive disorder, it is also essential to demonstrate that immune factors are pathogenic (rather than simply markers). It could be argued that antibodies are produced as a result of neuronal damage or are a non-specific response to recent streptococcal infection, therefore representing an epiphenomenon. However, the low prevalence of these antibodies in the neurological and streptococcal control groups makes this less likely.
The presence of anti-basal ganglia antibodies in some of the patients with obsessive–compulsive disorder raises the possibility that these cases may differ from those in which these antibodies are absent. We therefore compared the two groups to define any possible clinical differences. In support of the role of streptococcal infection, antibody-positive patients were more likely to have positive results on streptococcal serological testing. However, titres of anti-streptolysin O were elevated in 31% of antibody-negative patients. Streptococcal infection is common in children and therefore cannot be used as a marker of post-streptococcal neuropsychiatric disorder alone. The antibody-positive patients were also more likely to have tics or Tourette syndrome, further supporting a link between post-streptococcal autoimmunity and movement disorders. Other than these findings, there was no clear difference between the antibody-positive and antibody-negative patients in terms of obsessive–compulsive symptoms, comorbidity and family history. Importantly, the mean CY–BOCS score in the antibody-negative patients was higher than in the antibody-positive patients. This suggests that the absence of these antibodies was not due to remission of disease: rather it suggests that there are discrete subgroups of obsessive–compulsive disorder with a differing pathogenesis.
The patients recruited to this study attended a specialist clinic for children with obsessive–compulsive disorder, so it is conceivable that our cohort contained children whose disorder was complicated, atypical or therapy-resistant. Whether the autoimmune subgroup in our study had disorders with a different natural history (perhaps more spontaneous remission, or better long-term outcome) or differential treatment responsiveness requires longitudinal studies. However, all 50 patients had obsessive–compulsive disorder using internationally defined criteria (DSM–IV) and exhibited the range of obsessions, compulsions (and comorbidities) previously described in the idiopathic condition. It would be important to compare these findings with epidemiological samples of childhood- and adult-onset disorder, and also with other psychiatric disorders. Further examination of this autoimmune subgroup might provide insight into the neurobiology of obsessive–compulsive disorder and offer alternative therapies to patients with refractory illness in the future.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ Some cases of obsessive–compulsive disorder in children may be secondary to post-infection autoimmunity.
-
▪ If proved, this hypothesis might alter treatment strategies in the future (including antibiotic prophylaxis).
-
▪ Patients presenting with acute obsessive–compulsive disorder after pharyngeal infections should be investigated for streptococcal infection or carriage.
LIMITATIONS
-
▪ The study did not demonstrate whether the anti-neuronal antibodies were pathogenic or merely an epiphenomenon.
-
▪ The antibody detection methods used might have altered the brain proteins, resulting in altered antibody–antigen interaction.
-
▪ Our method used a brain homogenate rather than specific proteins. Identifying the autoantigens would help to determine whether the autoantibodies are specific.
Acknowledgements
R.C.D. has a training fellowship awarded by Action Research UK and the Barnwood House Trust. A.J.C. is funded by the University College London central research fund.




eLetters
No eLetters have been published for this article.