



Understanding the factors that lead people to experience suicidal thoughts is crucial for the development of psychological interventions. However, little research has examined the acute, proximal factors which precede an increase in such suicidal experiences. Only during the past few years have studies using intensive longitudinal designs examined temporal associations between suicidal ideation and risk factors such as affect, stress, hopelessness and sleep.Reference Sedano-Capdevila, Porras-Segovia, Bello, Baca-Garcia and Barrigon1
Clinicians, from a pragmatic perspective, are likely to be more concerned with assessing acute suicide risk over hours, days or weeks rather than across time periods spanning months and years. Similarly, for people with suicidal thoughts, it may feel more urgent and relevant to explore the most recent antecedents to those experiences. Identification of factors that predict and reflect suicidal experiences over a time span of hours or days rather than weeks, months or years would greatly help clinicians to effectively evaluate and organise care to address an individual's immediate needs with respect to suicidal thoughts and behaviours and to address acute risk. Such an approach has the potential to offer increased understanding of psychological factors that ‘trigger’ or lead to suicidal experiences, and the interactions between those psychological factors, which may amplify suicidal thoughts and acts on an hour-by-hour, day-to-day basis.
Theoretical accounts and empirical evidence suggest that feeling defeated and trapped is central in the pathways to suicidal thoughts and acts.Reference Johnson, Gooding and Tarrier2–Reference O'Connor and Kirtley6 Although it has been suggested that defeat and entrapment represent overlapping constructs,Reference Johnson, Gooding and Tarrier2,Reference Taylor, Wood, Gooding, Johnson and Tarrier7 temporal pathways have been proposed from defeat to entrapment, then to suicidal ideation.Reference O'Connor and Kirtley6 Of course, it should be acknowledged that when an individual has already made a suicide attempt, it is unlikely that the process of ideation and intention formation for a repeat suicide attempt will begin anew. However, research examining these constructs has often investigated these experiences cross-sectionally.
Ecological momentary assessment
An increasing body of literature has examined suicidal experiences using in-the-moment, real world assessments over hours and days.Reference Sedano-Capdevila, Porras-Segovia, Bello, Baca-Garcia and Barrigon1 Suicidal thoughts can fluctuate throughout the day.Reference Ben-Zeev, Young and Depp8,Reference Kleiman, Turner, Fedor, Beale, Huffman and Nock9 Real-time examination of the dynamic nature of suicidal experiences has been made more accessible by the development of diary-based technology which asks people about their experiences over minutes, hours and days.Reference Kleiman and Nock10 Typically, these types of ecological momentary assessment (EMA) or experience sampling methods ask people how they are feeling ‘right now’ using cues such as ‘right now I am feeling sad’ or ‘right now I am feeling hopeless’. They are especially suited to sampling experiences of individuals in their ‘real-world’, day-to-day lives.Reference Trull and Ebner-Priemer11
Findings from suicide-focused EMA studies indicate that previously identified risk factors may not predict proximal changes in suicidal thoughts across time scales spanning a few hours.Reference Ben-Zeev, Young and Depp8,Reference Kleiman, Turner, Fedor, Beale, Huffman and Nock9,Reference Hallensleben, Glaesmer, Forkmann, Rath, Strauss and Kersting12 Furthermore, studies employing EMA methodologies in this area have reported inconsistent patterns of results. For example, one study showed that sadness, tension and boredom were significantly associated with subsequent suicidal ideation,Reference Ben-Zeev, Young and Depp8 whereas another study showed that hopelessness and perceived burdensomeness were related to suicidal ideation at the next assessment, while depression and thwarted belongingness were not significant.Reference Hallensleben, Glaesmer, Forkmann, Rath, Strauss and Kersting12,Reference Rath, de Beurs, Hallensleben, Spangenberg, Glaesmer and Forkmann13 In addition, Kleiman et alReference Kleiman, Turner, Fedor, Beale, Huffman and Nock9 found that hopelessness, loneliness and perceived burdensomeness were concurrently associated with suicidal ideation, but none of these variables significantly predicted a subsequent change in suicidal ideation over time.Reference Kleiman, Turner, Fedor, Beale, Huffman and Nock9 Low connectedness combined with either high burdensomeness or high hopelessness were reliably associated with more severe same- and next-day suicidal ideation.Reference Czyz, Horwitz, Arango and King14 The most consistent finding of these studies is that suicidal ideation in-the-moment is related to previous suicidal ideation, i.e. an auto-regressive effect. One study used an EMA design to examine fluctuations in defeat and entrapment in a healthy sample.Reference Stenzel, Holler, Rath, Hallensleben, Spangenberg and Glaesmer15 Whereas defeat and entrapment were associated cross-sectionally, i.e. at the same measurement time point, they were not associated micro-longitudinally when a time lag of approximately 2 hours was used.
To date, EMA studies have made novel advances in the field by simultaneously examining multiple predictors of suicidal thoughts at a micro-longitudinal level across hours and days.Reference Sedano-Capdevila, Porras-Segovia, Bello, Baca-Garcia and Barrigon1 Furthermore, they have investigated complex pathways to suicidal experiences as reflected by multi-composite theories of suicide. However, defeat and entrapment were not included in these EMA studies. In addition, they did not take into account that the time interval between the predictor and the outcome variable is likely to affect the strength of associations between key variables, assuming time intervals of 2 h,Reference Ben-Zeev, Young and Depp8 30 to 120 minReference Hallensleben, Glaesmer, Forkmann, Rath, Strauss and Kersting12 and 4 to 8 h.Reference Kleiman, Turner, Fedor, Beale, Huffman and Nock9
Present study
Therefore, the main aim of the current study was to explore whether previously hypothesised causal relationships between defeat, entrapment and suicidal ideation accounted for temporal associations between these important psychological variables at time intervals of 3, 6, 9 and 12 h in a sample of people with major depression who also had experiences of suicidal thoughts, plans and attempts.
Method
Study design
An exploratory EMA design was used to collect in-the-moment ratings of defeat, entrapment and suicidal ideation. Participants were asked to complete ratings of these experiences six times per day across a week, using a touch-screen watch (CamNtech, Cambridge, UK).
Participants
Participants were recruited via three avenues: (a) referral from UK National Health Service (NHS) mental health services; (b) referral from UK mental health charities; and (c) self-referral in response to online advertisements on social media websites or posters placed in local community settings. Data were collected as part of a wider project which aimed to assess bi-directional associations between sleep disturbance and daily ratings of suicidal ideation.Reference Littlewood, Kyle, Carter, Peters, Pratt and Gooding16 The primary inclusion criteria for this study were: self-reported suicidal ideation and/or behaviours in the past month, experience of at least one major depressive episode according to the DSM-IV and confirmed by the Structured Clinical Interview for DSM Disorders,Reference First, Spitzer, Gibbon and Williams17 and age 18 to 65 yearsFootnote a. Written informed consent was obtained from all participants.
Ethics statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the local NHS research ethics committee (reference number:16/NW/0226).
EMA measure development
The full repeated diary assessments consisted of 24 items measuring 12 different types of experiences. For the current study, we used only the variables of suicidal ideation, defeat and entrapment, because we sought to focus on the proposed central relationship between these key components in the pathways to suicidal thoughts and acts. In addition, it is still unknown how many observations are required in a multivariate time-lagged model, where adding one variable multiplies the number of parameters that have to be estimated.Reference Jordan, Winer and Salem19 Hence, there was a need for caution. The four items used to assess these variables are provided in Table 1. Currently there is a lack of psychometrically validated EMA items suitable to meet the aims of the current study.Reference Myin-Germeys, Kasanova, Vaessen, Vachon, Kirtley and Viechtbauer20 Consequently, an initial item pool was developed from relevant pre-existing questionnaire measures and variable descriptions. This item pool was then discussed with members of a lived experience research advisory panel. This led to the revision of items to better reflect the terminology preferences of experts by experience. Items were then piloted with different members of the lived experience panel in order to establish the face validity and acceptability of the revised items. We used both entrapment items that were developed for this study, because ‘I want to escape my emotional pain’ reflects internal entrapment, while ‘I feel trapped’ can reflect external entrapment.
Table 1 Overview of the items used to assess study variables

a. Developed with lived experience research advisory panel.
Procedure
Recruitment and data collection were completed between May 2016 and March 2017. Repeated assessments of psychological variables and suicidal ideation were collected via the PRO-Diary watch (CamNtech, Cambridge, UK) across a 7 day period. Participants completed a maximum of six assessments at quasi-random time points each day. In line with best practice guidance, the daily assessment windows were customised based on a participant's habitual sleep and wake patterns in order to minimise the likelihood that the watch alerts would disrupt their sleep. The waking hours were then split into six sampling windows, with an assessment solicited at a random time within each period. The watch emitted an alert at the start of an assessment period, and participants were then asked to complete assessments of the variables using the watch touch panel. This resulted in short time intervals between measurements of 2 to 4 h and just under 3 h on average. All items were scored using a seven-point Likert scale from 1 = ‘not at all’ to 7 = ‘very much so’. Participants received £30 compensation for their involvement in the study, irrespective of whether they completed the full 7 day study.
Statistical analysis
Entrapment was assessed by two items, so the mean value was calculated and used in analyses. Means and standard deviations were obtained for all variables.
To assess temporal associations between variables, we used multilevel vector autoregression (MLVAR).Reference Bringmann, Vissers, Wichers, Geschwind, Kuppens and Peeters21,Reference Epskamp, Waldorp, Mõttus and Borsboom22 MLVAR is a multivariate explorative analysis for longitudinal data without a priori defined predictor and outcome variables, so we assumed that suicidal ideation could predict defeat and entrapment. This is important, because there is no reason to assume that an earlier episode of suicidal ideation cannot be associated with future feelings of defeat and entrapment, which in turn can lead to a new episode of suicidal ideation. All variables were regressed on all other variables included in the analysis at previous time points. Relations between variables were controlled for all other variables, because all regressions were in the same model. Therefore, relations could be interpreted as partial correlations. The analysis was multilevel, because every individual was assumed to have their own statistical model. Variables were person-mean centred and assumed to be stationary, i.e. they could fluctuate but there was no general upward or downward trend. First, the temporal network was estimated. In the temporal network graph, arrows indicate variables ‘predicted’ by lagged variables, i.e. they correlate with lagged variables and can therefore be assumed to be preceded by these variables in time. Second, the residuals of this first analysis were used to construct another network of partial correlations, which represented the relationships between the variables that could not be explained by the previously estimated time-lagged correlations. This network included both contemporaneous correlations and temporal correlations that occurred in time frames different from the time interval the temporal network was based on and contained within-subject effects, as with the temporal network.Reference Bringmann, Vissers, Wichers, Geschwind, Kuppens and Peeters21,Reference Epskamp, Waldorp, Mõttus and Borsboom22 In the graphs of the temporal and contemporaneous networks, thicker edges represented stronger relationships. We assumed that the temporal and contemporaneous effects were correlatedReference Jordan, Winer and Salem19,Reference Epskamp, Waldorp, Mõttus and Borsboom22 and used a significance level of 0.05 to decide whether variables were related, without correcting for multiple testing. Missing data were not imputed or estimated.
We explored the temporal associations between variables using four time lags, namely, lag 1 (2–4 h), lag 2 (5–7 h), lag 3 (8–10 h) and lag 4 (11–13 h). We only considered time lags that occurred within a day. This meant that every night counted as a reset, so the last measurement of day 1 did not predict the first measurement on day 2. Considering that we had six observations per item per day, this resulted in two observations per day for a lag 4 effect, i.e. from time point 1 to time point 5 and from time point 2 to time point 6. Note that in the lag 4 MLVAR model, lags 1, 2 and 3 were also included.
Although it was possible to estimate which variable would take the most central or important place in the networks (i.e. by using centrality measures), we omitted these analyses, because it has been argued that centrality measures are misleading when used in vector autoregressive modelsReference Epskamp, Waldorp, Mõttus and Borsboom22 and in networks of psychological constructs in general.Reference Bringmann, Elmer, Epskamp, Krause, Schoch and Wichers23
We used the R packages mlVARReference Epskamp, Deserno and Bringmann24 for the analyses and qgraphReference Epskamp, Cramer, Waldorp, Schmittmann and Borsboom25 for the visualisations.
Results
Sample
The sample comprised 51 individuals, of which 34 were women (67%). The mean age was 35.47 years (s.d. = 12.81, range 18–65 years). Most participants reported having attempted suicide at least once (n = 36, 71%) and were taking antidepressant medication (n = 34, 67%). Only one participant did not report any suicidal ideation during the 7 day EMA sampling period (see Littlewood et al (2019)Reference Littlewood, Kyle, Carter, Peters, Pratt and Gooding16 for a further description of the sample).
Descriptive statistics
These 51 respondents completed a total of 1852 assessments (Table 2). The response rate per participant ranged from 52.4% to 100%, with a mean of 86.7%. The highest response rates were on days 1 and 4 (87.6% each), while the lowest response rate (79.1%) was on day 7. Missing assessments were approximately evenly distributed throughout the day, because the response rate per time of the day ranged from 84.0% (time points 1 and 2) to 87.1% (time point 4). Means and standard deviations of the EMA items are shown in Table 2.
Table 2 Overview of descriptive statistics for the study variables of suicidal ideation, defeat and entrapment
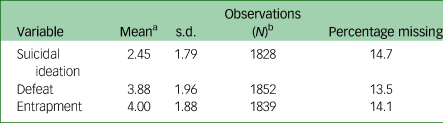
a. Range 1–7.
b. Out of a maximum of 2142.
MLVAR
Figures 1 and 2 show the significant temporal associations between variables, as well as their strengths. Full results including non-significant associations and standard errors can be found in Supplementary Appendix 1 available at https://doi.org/10.1192/bjo.2022.68. The lag 1 (3 h) network showed significant auto-correlations for each variable. In addition, entrapment had two-way temporal associations with defeat in addition to suicidal ideation, meaning that entrapment predicted and was predicted by defeat and suicidal ideation. The lag 2 (6 h) network also showed significant auto-correlations of the variables entrapment and suicidal ideation, but the auto-correlation of defeat was not significant. In addition, there were bidirectional associations between entrapment and suicidal ideation but no association with defeat. The lag 3 (9 h) associations were similar in terms of auto-correlations. There was a temporal association between entrapment and suicidal ideation, where entrapment predicted later suicidal ideation, but there was no effect from suicidal ideation to entrapment. In the final lag 4 (12 h) network, there was only one significant effect from entrapment to suicidal ideation. The residual and contemporaneous effects (estimated based on the residuals of the lag 1 effects) are shown in Fig. 3. There were significant contemporaneous effects between all variables, of which the association between defeat and entrapment was the strongest and the association between defeat and suicidal ideation was the weakest.

Fig. 1 Temporal effects for lag 1 (approximately 3 h) and lag 2 (6 h). Arrows indicate variables ‘predicted’ by lagged variables, meaning that there is a temporal association. Numbers are multivariate regression coefficients. Only statistically significant coefficients are shown.

Fig. 2 Temporal effects for lag 3 (9 h) and lag 4 (12 h). Arrows indicate variables ‘predicted’ by lagged variables, meaning that there is a temporal association. Numbers are multivariate regression coefficients. Only statistically significant coefficients are shown.

Fig. 3 Residual and contemporaneous effects based on the residuals of the lag 1 model. A thicker edge represents a stronger relationship. Numbers are multivariate coefficients estimated from the residuals of the lag 1 temporal effects. All associations were statistically significant.
Discussion
In this study we used EMA data to explore temporal relationships at small time intervals (3 to 12 h) between defeat, entrapment and suicidal ideation, derived from contemporary theories of psychological pathways to suicidal thoughts and acts.Reference Johnson, Gooding and Tarrier2,Reference O'Connor3,Reference Williams5,Reference O'Connor and Kirtley6 Whereas previous research showed that entrapment is key mechanistically in pathways to suicidal ideation, our results suggest that entrapment may also account for the emergence of suicidal thoughts across time periods of 3 to 12 h.
The results can be broken down into three main findings. First, suicidal ideation predicts itself over short time intervals, and entrapment also predicts itself over short time intervals, as indicated by significant auto-correlations for time windows of 3, 6 and 9 h. The auto-correlation of defeat was significant only for a time interval of approximately 3 h. Second, the temporal effect of entrapment predicting suicidal ideation was significant for all time intervals, whereas we found no significant temporal association between defeat and suicidal ideation for any time interval. Entrapment had two-way temporal associations with defeat and suicidal ideation for a time interval of 3 h and could therefore constitute a bridge between defeat and suicidal ideation at this time interval. Third, the network of residuals indicated that defeat, entrapment and suicidal ideation were correlated contemporaneously and/or that there may be temporal effects that occur in time frames different from the time interval the temporal network was based on (i.e. approximately 2–4 h).
Many theories of suicide centre on a two-stage pathway from defeat to entrapment to suicidal ideation.Reference Johnson, Gooding and Tarrier2,Reference O'Connor3,Reference Williams5,Reference O'Connor and Kirtley6 Empirically, findings from a meta-analysisReference Siddaway, Taylor, Wood and Schulz26 and systematic reviewReference Taylor, Gooding, Wood and Tarrier4 support this pathway, albeit with the caveat that investigations have largely used cross-sectional designs. More broadly, two recent longitudinal studies found entrapment to mediate the association between defeat and suicidal ideation.Reference Branley-Bell, O'Connor, Green, Ferguson, O'Carroll and O'Connor27,Reference Owen, Dempsey, Jones and Gooding28 Our intensive micro-longitudinal study suggests that these pathways may also explain some of the daily fluctuations in suicidal ideation, supporting the hypothesis that entrapment is a driver for the emergence of suicidal ideation, and that entrapment could be considered a bridge variable between defeat and suicidal ideation. However, we also found support for a converse temporal pathway, i.e. from suicidal ideation to entrapment to defeat. A recent EMA study found that defeat was contemporaneously associated with entrapment but not approximately 2 h later.Reference Stenzel, Holler, Rath, Hallensleben, Spangenberg and Glaesmer15 Apart from methodological differences, a potential explanation for this finding is that the sample of Stenzel et al consisted of individuals without mental health problems, whose psychological mechanisms relating to suicidal thoughts are probably different.
Psychological models of the pathways to suicidal ideation and behavioursReference Johnson, Gooding and Tarrier2,Reference O'Connor and Kirtley6 would benefit from considering fluctuations in and temporal relationships between defeat, entrapment and suicidal experiences over time spans of hours, in addition to the follow-up time points of months often used in recent prospectively designed studies.Reference Owen, Dempsey, Jones and Gooding28,Reference Panagioti, Gooding and Tarrier29 Alternative theoretical accounts may be needed to understand the mechanisms that lead to short-term proximal changes in suicidal ideation over the course of hours. It has been posited that the association between entrapment and suicidal ideation is moderated by variables such as interpersonal factors, future thoughts and resilience.Reference O'Connor and Kirtley6 Future research will need to determine whether these moderating effects also apply to short-term changes in suicidal ideation.
We should also be mindful about debates concerning the conceptual similarities and differences between defeat and entrapment,Reference Taylor, Wood, Gooding, Johnson and Tarrier7 together with hopelessness,Reference Johnson, Gooding and Tarrier2,Reference Taylor, Gooding, Wood and Tarrier4 and ways in which these perceptions may be context dependent. For example, relationships between feeling trapped and having suicidal thoughts or plans may differ in people who are incarceratedReference Gooding, Tarrier, Dunn, Shaw, Awenat and Ulph30 or on in-patient psychiatric wardsReference Haddock, Pratt, Gooding, Peters, Emsley and Evans31 compared with those in the community. Similarly, people with severe mental health problems including the challenges of hallucinatory voices may feel particularly trapped by these voices throughout their day.Reference Taylor, Gooding, Wood, Johnson, Pratt and Tarrier32
Clinical implications
Research that combines in-the-moment, repeated assessments with network analyses offers great potential clinical and practical utility. For instance, identifying bridging variables can be used to better target interventions aimed at key mechanistic pathways, at clinically important time points.Reference Kelly, Gooding, Pratt, Ainsworth, Welford and Tarrier33 To illustrate, in the current study, entrapment had bidirectional temporal associations with defeat and suicidal ideation at approximately 3 h time intervals. Consequently, it may prove clinically important to develop interventions directed at perceptions of entrapment, as a means of influencing not only entrapment but also defeat and suicidal ideation together and interactively. If emerging entrapment can be considered a warning sign for the rapid emergence of suicidal ideation, mobile technologiesReference Berry, Machin, Ainsworth, Berry, Edge and Haddock34 could be developed to contact a client when entrapment feels overwhelming or uncontrollable for them, in order to prevent further escalation.
The high response rate we found indicates that the EMA schedule used in this study might be feasible in clinical practice among a comparable group of patients. There might be selection bias in our sample, because some patients were included by self-referral. It should also be noted that participants were offered incentives, which may limit the generalisability of results,Reference Porras-Segovia, Molina-Madueno, Berrouiguet, Lopez-Castroman, Barrigon and Perez-Rodriguez35 although the incentives were not response contingent. To enhance the translational impact of work in this area, the views of clinicians and of people with lived experience of suicidal thoughts and acts should both be incorporated in order to understand how EMA designs can be best utilised for acceptable and feasible clinical interventions in ways which maximise co-production by numerous stakeholders.Reference Realpe, Elahi, Bucci, Birchwood, Vlaev and Taylor36
Limitations
There were several limitations to this study. First, the validity and reliability of the repeated diary items could be challenged on the basis that they were not been subjected to rigorous psychometric assessment. However, the observed associations were consistent with those previously reported in the literature, suggesting that the items provide some degree of valid assessment. The lack of available psychometrically validated items has been acknowledged as a broad limitation of current EMA work in this area.Reference Myin-Germeys, Kasanova, Vaessen, Vachon, Kirtley and Viechtbauer20 This is currently being addressed by Kirtley et al,Reference Kirtley, Hiekkaranta, Kunkels, Eisele, Verhoeven and Van Nierop37 who are encouraging EMA researchers to deposit their existing items into an open repository, which can then be subjected to psychometric evaluation. In lieu of this work, the items used in the current study were developed in conjunction with a lived experience research advisory panel, with the goal of producing items that were deemed to possess face validity.
Second, the results of the lag 3 and lag 4 models have to be interpreted with caution because of low statistical power, meaning that some ‘true’ temporal effects may have been undetected. Owing to missing values, the numbers of observations per individual may have been relatively small. This issue of within-subject power could be addressed in the design phase of subsequent research, which should seek to extend the EMA sampling period from 1 to multiple weeks or even a number of months.Reference Nuij, van Ballegooijen, Ruwaard, De Beurs, Mokkenstorm and van Duijn38 Consultation with patient and public involvement advisory panels may help to identify a ‘sweet spot’ which balances participant burden and research benefit.
Third, we included only defeat, entrapment and suicidal ideation in our analyses, because the relationships between these variables have been clearly hypothesised in the literature; however, there might be equally important proximal psychological predictors of suicidal ideation.Reference Hawton, Casanas i Comabella, Haw and Saunders39,Reference Van Orden, Witte, Cukrowicz, Braithwaite, Selby and Joiner40
Fourth, the sample consisted of participants who had primarily experienced major depressive episodes. Hence, the results may not be generalisable to other groups that are vulnerable to suicidal ideation or behaviours, such as those who experience personality disorders and/or non-affective psychosis.
Fifth, the statistical model used in our analyses assumed discrete time intervals between measurements, whereas the actual time intervals in this study were 2 to 4 h. This might have biased our results. However, discrete time intervals may also lead to biased data, because participants could learn when to expect the measurements, and also because discrete time intervals may lead to data being missing not-at-random (e.g. if a participant always misses a measurement at 08:00 h in the morning).
Sixth, we did not have sufficient power to perform subgroup analyses or moderator analyses. It is possible that the effects we found were linked to a specific factor, such as history of suicide attempts or mood.
To conclude, theoretical models describe the development of suicidal ideation and behaviour, although they are based largely on cross-sectional designs. Previous research showed that entrapment is a key mechanistic component in the emergence of suicidal ideation. Our results suggest that entrapment may also account for the emergence of suicidal thoughts across time periods of 3 to 12 h. In addition, entrapment was found to be a bridge variable between defeat and suicidal ideation at a time interval of 3 h. Clinically, the identification of variables that predict and reflect suicidal experiences over acute time frames of hours or days could be used to inform effective suicide prevention interventions.
Supplementary material
Supplementary material is available online at http://doi.org/10.1192/bjo.2022.68.
Data availability
The data that support the findings of this study are available from the corresponding author, W.v.B., upon reasonable request.
Acknowledgements
We thank the people who took part in this study for sharing their personal experiences. In addition, we acknowledge and thank the members of the lived experience research advisory panel for their support in developing and piloting the study.
Author contributions
W.v.B. and D.L.L. drafted the manuscript. W.v.B. conducted the analyses. All authors critically revised the manuscript. All authors approved the final article.
Funding
W.v.B. contributed to this study as part of the Continuous Assessment for Suicide Prevention and Research (CASPAR) project, funded by ZonMw (Netherlands Organisation for Health Research and Development), project number 537001008. D.L.L. conducted this research during her doctoral studentship, funded by the Medical Research Council and The University of Manchester Presidential Scholar Award.
Declaration of interest
None.








 Open access
Open access
eLetters
No eLetters have been published for this article.