



Good nutrition supports athletes’ health, performance, and recovery from training and competition(Reference Thomas, Erdman and Burke1). Adjusting dietary intake to meet sports nutrition recommendations has been found to improve outcomes such as body composition (increased muscle mass(Reference Antonio, Ellerbroek and Silver2)), competitive edge in performance (VO2 max(Reference Bailey and Hennessy3), handgrip strength(Reference Heileson, Elliott and Buzzard4) and sprint performance(Reference Rowlands and Wadsworth5–Reference Wachsmuth, Aberer and Haupt7)) and post-exercise recovery (carbohydrate improves glycogen resynthesis after endurance activities(Reference Arribalzaga, Viribay and Calleja-Gonzalez8), protein increases muscle protein synthesis and decreases muscle degradation(Reference Master and Macedo9), and adequate energy and macronutrients reduce risk of injury(Reference Vieira, Soares Nunes and Iori10)). However, athletes often do not follow consensus dietary recommendations. In this context, it is important for nutrition professionals working with athletes to understand ways in which dietary intake can be modified.
Nutrition education interventions have been used to influence athletes’ dietary behaviours(Reference Terenzio, Cassera and Gervasoni11). Nutrition interventions have included a broad range of topics, such as energy, macronutrient, micronutrient and hydration principles, as well as meal frequency and timing, and supplement use(Reference Boidin, Tam and Mitchell12). In relation, multiple interventions in athletes have included behavioural strategies, such as enablement, training, environmental restructuring, modelling and coercion(Reference Bentley, Mitchell and Backhouse13). Terenzio et al.(Reference Terenzio, Cassera and Gervasoni11) identified positive impacts on consumption of vegetables, nuts, legumes and fish (P < 0·05, P < 0·001, P < 0·001 and P < 0·05, respectively), while Boidin et al.(Reference Boidin, Tam and Mitchell12) reported inconsistent changes in dietary intake across the studies included in the review. A systematic review by Bentley et al.(Reference Bentley, Mitchell and Backhouse13) identified that the majority of interventions with a focus on behavioural strategies had a positive impact on improved dietary behaviours, made possible through several approaches.
Nutrition knowledge is one factor that is often targeted for change in nutrition education interventions(Reference Janiczak, Devlin and Forsyth14,Reference Tam, Beck and Manore15) , with a systematic review finding that nutrition education interventions are efficacious at improving nutrition knowledge(Reference Tam, Beck and Manore15). Good nutrition knowledge is one of many factors that impact dietary intake(Reference Birkenhead and Slater16–Reference Stok, Hoffmann and Volkert18). Several frameworks have been established to operationalise factors that influence diet intake. In athletes, Birkenhead and Slater(Reference Birkenhead and Slater16) identified physiological and biological; lifestyles, beliefs, and knowledge; psychological; social; and economic, and Pelly et al.(Reference Pelly, Thurecht and Slater17) identified similar factors. Likewise, in the general population DONE(Reference Stok, Hoffmann and Volkert18) noted biological, demographic, psychological, situational, social, cultural, product, micro, meso/macro, industry and government factors. In this context, it is relevant to assess other factors that may have an impact. For this review, the factors focused on are hedonic hunger, nutrition knowledge, macronutrient contribution to total energy intake, and body image and weight control. These have been identified by previous literature as factors within the Birkenhead and Slater framework(Reference Trakman19) able to be modified by nutrition professionals. By focusing on elements that may be more easily modified by nutrition professionals, this review will explore factors most suitable to modification through interventions identified.
Hedonic hunger is associated with susceptibility to environment food cues(Reference Theim, Brown and Juarascio20) or the desire to eat for the pleasure of the taste(Reference Birkenhead and Slater16). A recent study has found high risk of orthorexia and higher levels of hedonic hunger within individuals engaged in sport at any level than sedentary individuals(Reference Yildiz, Yildirim and Gündüz21).
Nutrition knowledge has been shown to have a positive relationship with improved dietary behaviours(Reference Spronk, Heaney and Prvan22). Previous research has identified that athletes with a higher level of nutrition knowledge often exhibit more positive dietary behaviours(Reference Janiczak, Devlin and Forsyth14). Studies exploring the improvement of nutrition knowledge often rely upon nutrition education interventions(Reference Coccia, Fernandes and Altiti23,Reference Nascimento, Silva and Ribeiro24) .
Macronutrient contribution to total energy intake has been shown to have an impact on total energy intake, with increased protein intake increasing satiety and therefore reducing total energy intake(Reference Westerterp-Plantenga, Lemmens and Westerterp25). Athletes’ dietary intake may modify macronutrient contribution to total energy intake for purposes of periodisation(Reference Thomas, Erdman and Burke1,Reference Stellingwerff, Bovim and Whitfield26) . Studies into macronutrient contribution to total energy intake in athletes have largely explored intake similarity to current guidelines(Reference Aerenhouts, Deriemaeker and Hebbelinck27,Reference Black, Black and Baker28) and impact on performance(Reference Anderson, Naughton and Close29–Reference Hansen, Bangsbo and Jensen32).
Body image and weight control are linked due to sports’ requirements for athletes to meet body composition goals or ideals and the methods used to meet those goals(Reference Birkenhead and Slater16,Reference Anderson and Petrie33) . Studies have found that athletes within sports which recommend weight control have a higher prevalence of dissatisfaction with body image, as well as increased risk factors for eating disorders(Reference de Oliveira, de Oliveira and Gonçalves34) and aesthetic sport athletes were found to have a higher level of body dissatisfaction than endurance, fitness and weight class athletes(Reference Kristjánsdóttir, Sigurðardóttir and Jónsdóttir35).
While nutrition education interventions are common, and the impact of these on athlete’s dietary intake(Reference Boidin, Tam and Mitchell12) and improved nutrition knowledge(Reference Tam, Beck and Manore15) have been previously reviewed, there is a dearth of studies on the impact of other modifiable factors in athletes, and results of these studies are yet to be synthesised. A systematic review by Boidin et al.(Reference Boidin, Tam and Mitchell12) found that fourteen of the twenty-two included studies reported significant change in at least one aspect of dietary intake due to a nutrition education intervention. Similarly, Tam et al.(Reference Tam, Beck and Manore15) reported a significant nutrition knowledge increase due to nutrition education interventions that were largely face-to-face delivered. The exploration of these interventions and their impact on both modifiable factors and dietary intake is necessary to inform effective design for future interventions. Therefore, the purpose of this review is to investigate the types and effectiveness of interventions used to impact the factors of hedonic hunger, nutrition knowledge, macronutrient contribution to total energy intake, and body image and weight control which influence dietary intake in athletes.
Methodology
Materials and methods
This systematic review was conducted in accordance with PRISMA guidelines(Reference Page, Moher and Bossuyt36) and prospectively registered with PROSPERO (protocol registration ID 2022 CRD42022342781).
Search method and information sources
Search strategy was developed by AJ with support from an academic librarian, which was then reviewed by GT, AF and RA. This was designed to capture information on food intake and factors assessed in our previous work(Reference Janiczak37). One reviewer (AJ) systematically searched MEDLINE, CINAHL, SPORTDiscus and Web of Science databases from database inception up to and including 18 May 2022, with initial searches conducted 29 March 2022. Search terms included subject headings of diet, eating, nutritional sciences, dietetics, sports nutritional sciences, and athletes, and keywords of ‘diet* intake’, food, ‘feeding behavio?r’, ‘eating behavio?r’, ‘energy intake’, ‘nutrition knowledge’, ‘sport* nutrition knowledge’, ‘hedonic hunger’, appetite, compensat*, ‘macronutrient balance’, ‘high protein’, ‘high carbohydrate’, ‘high fat’, ‘body composition’, ‘weight control’, ‘body image’, ‘mak* weight’, ‘nutrition science’, ‘modifiable factor’, athlete*, and sport*. Limits for English language and journal articles were used. Full MEDLINE search strategy is available in Supplementary Material.
Eligibility criteria
In order to be included in this review, studies were required to fulfil eligibility criteria as outlined in Table 1. Athletes were defined as any individual competing, participating or performing in a sport. For the purposes of this review, elite military personnel were considered athletes and were included within the review, although reserve military personnel were excluded. Recreational athletes participating in local sporting leagues were required to participate in a minimum of 2·5 h of exercise per week(Reference Debrow, Slater and Cox38–Reference Araujo40). Adolescent athletes (less than 18 years of age) were excluded from this review due to the potential for age-related confounding factors and differences in dietary intake during growth(Reference Thomas, Erdman and Burke1,Reference Berg41) . If papers included a mixed cohort that reported adolescent and adult results separate, the results from the adult group would be included.
Table 1. Inclusion and exclusion criteria
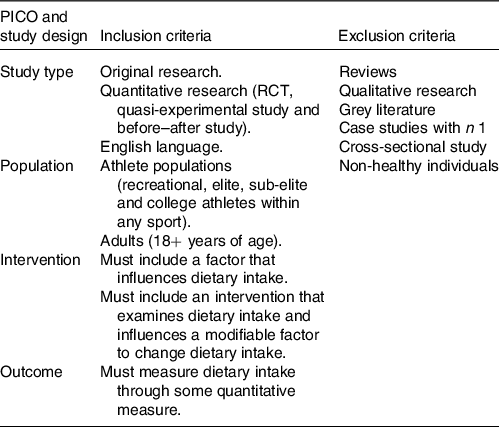
Dietary intake could include diet quality score, measure of habitual dietary intake, energy intake or nutrient intake. PICO, Population, Intervention, Comparator, and Outcome; RCT, randomised controlled trials.
Screening process
All records were imported to Covidence(42), where duplicates were removed, and screening was subsequently completed. Two reviewers (AJ and GT or AF or RA) independently screened all papers for eligibility by reviewing title and abstract. Articles were requested for retrieval through the university library, with all articles being retrieved. Eligible articles were then screened in duplicate (AJ and GT or AF or RA) for full-text review (Fig. 1). Reasons for exclusion were noted within Covidence at the time of exclusion using customised exclusion categories. Disagreements were screened by a reviewer (GT or AF or RA) that was not involved in the original screening.
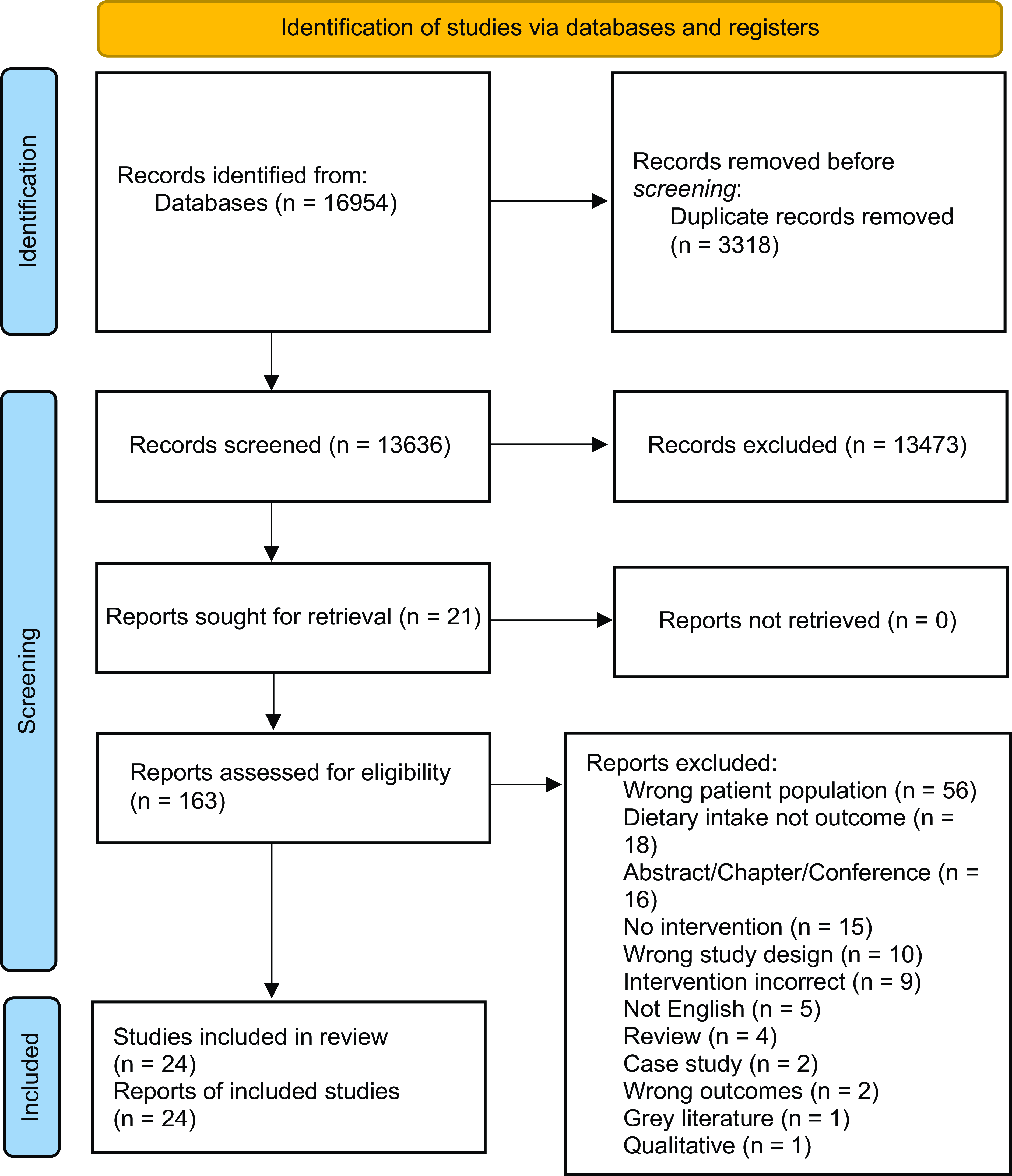
Fig. 1. PRISMA flow chart for screening process. Source: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n7.
Data extraction and data items
Covidence was used to extract data from the included studies using a pre-designed, purpose-built extraction form. Two reviewers (AJ and GT, AF, or RA) independently extracted the data from all included studies. Inconsistencies in extracted data were first discussed to attempt to reach consensus; if consensus could not be reached, a third reviewer (who was not involved in the initial extraction) was enlisted to decide. Data extracted included author and date, key study information (aim, location (country), setting (university or laboratory details), study design and recruitment methods), intervention information (intervention type and details), the factor being investigated (factor, measurement tool and results), dietary intake (measurement tool used and results), participant demographics (sample size, age and sex), and correlation measures between factor being investigated and dietary intake where available.
Quality assessment
The quality of individual studies was assessed using Quality Criteria Checklist: Primary Research(43), for the assessment of all studies. The process and guidelines for quality assessment were agreed upon among researchers prior to assessment commencement. Points were allocated for each question within the scale – ‘yes’ accounting for one point and ‘no’ or unclear receiving zero points for that question.
Analysis
Narrative synthesis was used to analyse the data collected due to the heterogeneity of methods, and outcomes measured did not support meta-analysis.
Results
Included studies
Initial data searches provided 16 954 studies that were imported into Covidence; after duplicates (n 3318) were removed, 13 636 articles remained for title/abstract screening. The title/abstract screening stage excluded a further 13 473 papers, leading to inclusion of 163 papers for full-text screening. A total of 136 papers were excluded for a variety of reasons (available in Fig. 1). Twenty-four papers were included in the final extraction for this review (see Table 2).
Table 2. Data extraction table for dietary intake and factors being investigated
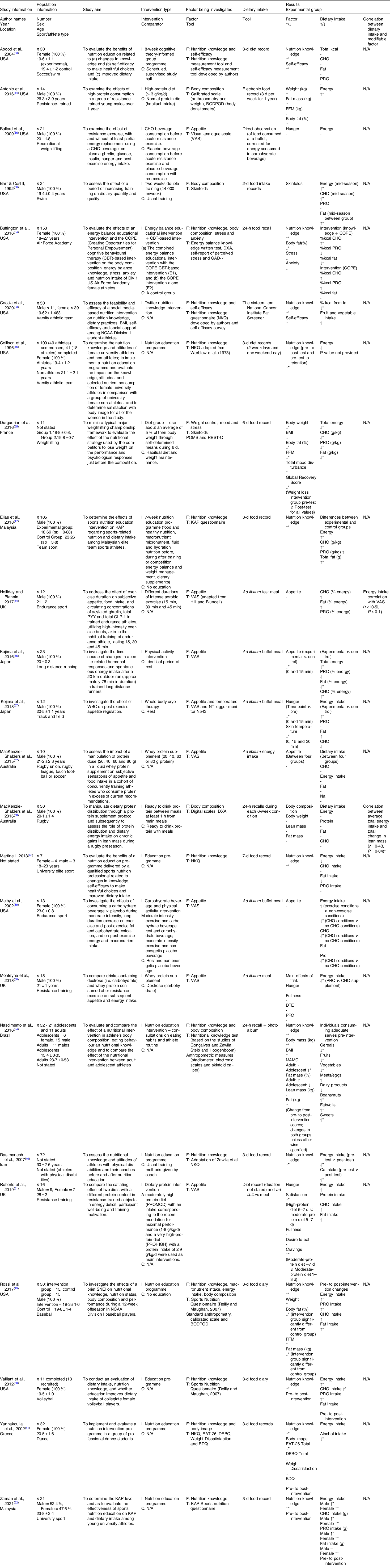
I, intervention(s); C, control; F, factor(s); T, tool(s); CHO, carbohydrate; PRO, protein; FFM, fat-free mass; %kcal, percentage of total energy intake in kilocalories; COPE, Creating Opportunities for Personal Empowerment; DXA, dual-energy X-ray absorptiometry; GAD- 7, General Anxiety Disorder-7; NCAA, National Collegiate Athletic Association; POMS, Profile of Mood States; REST-Q, Recovery-Stress Questionnaire; WBC, whole body cryotherapy; PYY, Peptide YY; GLP-1, glucagon-like peptide 1; KAP, Knowledge, Attitudes, and Practices; DTE, desire to eat; PFC, prospective food consumption; MAMC, mid-arm muscle circumference; EAT-26, Eating Attitudes test; DEBQ, Dutch Eating Behaviour Questionnaire; BDQ, Body Dissatisfaction Questionnaire; SNEI, sports nutrition education intervention.
Aims are as stated in the articles.
↑, increased in intervention group; ↓, decreased in intervention group; -, no change; N/A, not applicable.
* P-value < 0·05.
A total of 844 participants were included across all studies, with 454 male and 307 female participants (two studies did not identify sex). Six studies consisted of entirely female populations, while eleven were entirely male populations. The age of adult participants ranged between 18·69+/–0·88 and 30+/–7·6 years. Participants included were from a variety of populations, as follows: endurance athletes (n 2), university athletes (n 10), resistance-trained athletes (n 5), team sport athletes (n 2), dancers (n 1), and athletes with spinal cord injury and amputations (n 1), as well as three studies with unclear sport/exercise types. Nine countries were represented within this sample, as follows: USA (n 10), UK (n 3), Japan (n 2), Australia (n 2), Malaysia (n 2), Greece (n 1), Iran (n 1), France (n 1) and Brazil (n 1), with country unreported in one study. Six of the included studies included ethnicity information for the athletes, with four of these studies occurring within the USA (ethnicities included Caucasian, African American, Hispanic, Pacific Islander, Asian and other) and two within Malaysia (ethnicities included Malay, Indian, Chinese and Others).
The study designs included quasi-experimental (n 9), randomised crossover trial (n 7), randomised controlled trial (n 4), counter-balanced (n 1), randomised counter-balanced design (n 1), randomised double-blind trial (n 1) and randomised, double-blind, placebo-controlled trial (n 1). The types of interventions employed by researchers included nutrition education (n 10), macronutrient adjustment intervention (n 7), physical activity (n 5), cognitive theory-based intervention (n 2), weight loss (n 1) and whole-body cryotherapy (n 1). Eight factors were assessed within included papers: nutrition knowledge (n 12), hunger and appetite (n 8), body composition (n 4), macronutrient contribution to total energy intake (n 2), self-efficacy (n 2), body image (n 1), stress and anxiety (n 3), and use of weight control measures (n 1).
Intervention effectiveness
Some papers report dietary intake (e.g. absolute macronutrient intake or diet quality) and macronutrient contribution to total energy intake which has crossover in results due to the fact that dietary intake and macronutrient contribution to total energy intake are often measured with the same tools. Where adjustment to macronutrient contribution to total energy intake were the focus of the intervention (e.g. a high-protein diet), macronutrient distribution has been reported separately to absolute macronutrient and other dietary intake(Reference Antonio, Ellerbroek and Silver44,Reference Rossi, Landreth and Beam45) .
Nutrition education was the most used intervention among the included papers (n 10)(Reference Coccia, Fernandes and Altiti23,Reference Nascimento, Silva and Ribeiro24,Reference Rossi, Landreth and Beam45–Reference Zaman, Muhamad and Jusoh52) . Nutrition education interventions included twitter-based nutrition knowledge interventions, group education sessions (duration: between 2 weeks and 5 months), face-to-face education sessions and personalised individual consultations. In addition to dietary intake, all studies that employed a nutrition education intervention assessed nutrition knowledge, with body composition(Reference Nascimento, Silva and Ribeiro24,Reference Rossi, Landreth and Beam45) , body image(Reference Yannakoulia, Sitara and Matalas51) and self-efficacy(Reference Coccia, Fernandes and Altiti23) also examined in some studies. The majority of nutrition education intervention studies utilised a quasi-experimental study design (n 8)(Reference Coccia, Fernandes and Altiti23,Reference Nascimento, Silva and Ribeiro24,Reference Rossi, Landreth and Beam45,Reference Collison, Kuczmarski and Vickery46,Reference Martinelli48,Reference Valliant, Emplaincourt and Wenzel50–Reference Zaman, Muhamad and Jusoh52) , with the two remaining studies using a randomised controlled trial study design(Reference Elias, Saad and Taib47,Reference Rastmanesh, Taleban and Kimiagar49) . Dietary intake was measured using 3-d food records (n 7)(Reference Rossi, Landreth and Beam45–Reference Elias, Saad and Taib47,Reference Rastmanesh, Taleban and Kimiagar49–Reference Zaman, Muhamad and Jusoh52) , 7-d food records (n 1)(Reference Martinelli48), 24-h recall with photo album (n 1)(Reference Nascimento, Silva and Ribeiro24) and a sixteen-item National Cancer Institute Fat Screener (n 1)(Reference Coccia, Fernandes and Altiti23). These tools measured energy intake (n 8)(Reference Rossi, Landreth and Beam45–Reference Zaman, Muhamad and Jusoh52), macronutrient intake (n 5)(Reference Rossi, Landreth and Beam45,Reference Elias, Saad and Taib47,Reference Martinelli48,Reference Valliant, Emplaincourt and Wenzel50,Reference Zaman, Muhamad and Jusoh52) , Ca intake (n 1)(Reference Rastmanesh, Taleban and Kimiagar49), alcohol intake (n 1)(Reference Yannakoulia, Sitara and Matalas51), adequate intake of food groups (n 1)(Reference Nascimento, Silva and Ribeiro24), percentage of energy content from fat and fruit/vegetable intake (n 1)(Reference Coccia, Fernandes and Altiti23). Nutrition knowledge was measured using nutrition knowledge scores from various tools (n 10)(Reference Coccia, Fernandes and Altiti23,Reference Nascimento, Silva and Ribeiro24,Reference Rossi, Landreth and Beam45–Reference Zaman, Muhamad and Jusoh52) , body composition was measured using standard anthropometry, calibrated scales, and BODPOD (n 1)(Reference Rossi, Landreth and Beam45), as well as skinfold callipers(Reference Nascimento, Silva and Ribeiro24), self-efficacy was measured with a pre-validated tool to provide a composite score (n 1)(Reference Coccia, Fernandes and Altiti23), and body image scores were calculated through EAT-26, DEBQ, and Weight Dissatisfaction surveys (n 1)(Reference Yannakoulia, Sitara and Matalas51). In eight of ten studies that used a nutrition education intervention, dietary intake was positively impacted according to post-intervention testing with significant decreases in percentage of total energy content from fat(Reference Coccia, Fernandes and Altiti23), alcohol intake(Reference Yannakoulia, Sitara and Matalas51), Ca intake(Reference Rastmanesh, Taleban and Kimiagar49), total energy intake (closer to recommendations)(Reference Rastmanesh, Taleban and Kimiagar49) and sweets and oils(Reference Nascimento, Silva and Ribeiro24), as well as significant increases, closer to recommendations, in total energy intake(Reference Rossi, Landreth and Beam45,Reference Elias, Saad and Taib47,Reference Valliant, Emplaincourt and Wenzel50,Reference Zaman, Muhamad and Jusoh52) and macronutrient contribution to total energy intake(Reference Valliant, Emplaincourt and Wenzel50). Non-significant changes were also noted in deceased total energy intake(Reference Collison, Kuczmarski and Vickery46,Reference Martinelli48) , decreased % energy from fat(Reference Martinelli48), increased consumption of meat and eggs and decreased dairy products consumption(Reference Nascimento, Silva and Ribeiro24), and increased fruit and vegetable intake(Reference Coccia, Fernandes and Altiti23,Reference Elias, Saad and Taib47) . Changes in factors being investigated for nutrition education interventions were largely significant. Nutrition knowledge in athletes significantly increased in all studies post-intervention compared with baseline(Reference Coccia, Fernandes and Altiti23,Reference Nascimento, Silva and Ribeiro24,Reference Rossi, Landreth and Beam45–Reference Zaman, Muhamad and Jusoh52) . There were significant changes in body composition, with reductions in body fat (%) and fat mass (kg) for the intervention group compared with the control group, while fat-free mass (kg) increased significantly for both intervention and control group between pre- and post-intervention measures(Reference Rossi, Landreth and Beam45). Nascimento et al. reported significant increases in body mass (kg) for both adult and adolescent participants and a significant increase in mid-arm muscle circumference for adolescent participants between pre- and post-intervention measures, while other measures had non-significant changes(Reference Nascimento, Silva and Ribeiro24). Nutrition education interventions positively impacted body image scores. Yannakoulia et al. reported significant decreases in body image disturbance scores between pre- and post-intervention testing (EAT-26 total score and dieting subscale, DEBQ restraint subscale)(Reference Yannakoulia, Sitara and Matalas51); however, this study did not include a control group. Mean self-efficacy scores increased from pre-intervention testing to post-intervention testing in the Coccia et al. study, which also did not include a control group(Reference Coccia, Fernandes and Altiti23).
Two studies(Reference Abood, Black and Birnbaum53,Reference Buffington, Melnyk and Morales54) utilised a cognitive-based, theory-based intervention to influence nutrition knowledge (n 2), with Abood et al. also assessing self-efficacy(Reference Abood, Black and Birnbaum53) and Buffington et al. also assessing body composition (n 1), stress (n 1), and anxiety (n 1)(Reference Buffington, Melnyk and Morales54). These cognitive-based, theory-based interventions have an integral component of self-efficacy to provide a sense of self-control in order to modify behaviour(Reference Abood, Black and Birnbaum53) or teach participants coping mechanisms for managing stressful situations and improve emotional state and behaviours(Reference Buffington, Melnyk and Morales54). Both Abood et al.(Reference Abood, Black and Birnbaum53) and Buffington et al.(Reference Buffington, Melnyk and Morales54) utilised a randomised controlled trial study design. Abood et al.(Reference Abood, Black and Birnbaum53) used author developed surveys to measure nutrition knowledge and self-efficacy, while dietary intake was measured with an electronic food record. Buffington et al.(Reference Buffington, Melnyk and Morales54) used an energy balance knowledge written test to measure nutrition knowledge, DXA to measure body composition, self-report perceived stress and GAD-7 to measure stress and anxiety, respectively; dietary intake was measured using a 24-h food recall. Abood et al.(Reference Abood, Black and Birnbaum53) noted a significant decrease in percent of total carbohydrate intake in the control group between pre- and post-testing. The intervention group of Abood et al.(Reference Abood, Black and Birnbaum53) study demonstrated a significant increase in self-efficacy scores. Buffington et al.(Reference Buffington, Melnyk and Morales54) identified significant changes in percent of carbohydrates (increase) and percent of fat (decrease) consumed in the intervention group with an energy balance and a Creating Opportunities for Personal Empowerment (COPE) intervention each week, with significant changes not identified for the COPE intervention group, while there was a significant increase in percent of protein consumed in the control group. Significant increases in nutrition knowledge were reported for groups who participated in cognitive-based intervention groups(Reference Abood, Black and Birnbaum53,Reference Buffington, Melnyk and Morales54) ; however, Buffington et al.(Reference Buffington, Melnyk and Morales54) also found significant increases in nutrition knowledge within the control group, which participated in a supervised study session rather than the education sessions. Significant decreases in body fat percentage were noted within intervention groups, and stress scores significantly increased for control group without significant changes for intervention groups(Reference Buffington, Melnyk and Morales54). Buffington et al.(Reference Buffington, Melnyk and Morales54) found no significant changes in anxiety scores between pre- and post-intervention for any group.
A weight loss intervention was utilised to assess body composition, mood and stress in high-level weightlifters who are often required to reduce weight for competitions through a randomised counterbalanced trial(Reference Durguerian, Bougard and Drogou55). The intervention group lost about an average of 5 % of their body weight through self-determined means during a 6-d period, while the control group consumed their habitual diet and maintained their weight. Dietary intake was measured using a 6-d food record, while body composition was measured through skinfolds, mood was measured through Profile of Mood States survey and stress was measured with the Recovery-Stress Questionnaire. Dietary intake of energy and all macronutrients was found to be significantly lower than consumption during the weight loss phase. Body fat percentage, body weight and fat-free mass were found to be significantly lower in the diet group than the weight maintenance group. Total mood disturbance increased in the weight loss intervention group from pre-intervention testing to post-intervention testing, while there was a significant reduction in the global recovery score for this group from pre- to post-intervention testing.
Macronutrient adjustment interventions were used in seven of the included twenty-four studies. Macronutrient adjustment interventions involved changing intake of one or more macronutrients via supplementation (n 5)(Reference Ballard, Melby and Camus56–Reference Monteyne, Martin and Jackson60) or change in overall diet pattern (n 2)(Reference Antonio, Ellerbroek and Silver44,Reference Roberts, Zinchenko and Mahbubani61) . Macronutrient contribution to total energy intakes are considered factors to be investigated due to the possibility that throughout the course of the intervention, this factor may impact overall energy intake due to gastric emptying variation(Reference Clegg and Shafat62) or changes in hormonal appetite response(Reference Hutchison, Piscitelli and Horowitz63). A macronutrient adjustment intervention was used to impact a variety of factors being investigated: hunger and appetite (n 5)(Reference Ballard, Melby and Camus56,Reference MacKenzie-Shalders, Byrne and Slater57,Reference Melby, Osterberg and Resch59–Reference Roberts, Zinchenko and Mahbubani61) and body composition (n 2)(Reference Antonio, Ellerbroek and Silver44,Reference MacKenzie-Shalders, King and Byrne58) . Studies that included a macronutrient adjustment interventions used a variety of study designs, such as randomised crossover trial (n 4)(Reference Antonio, Ellerbroek and Silver44,Reference MacKenzie-Shalders, King and Byrne58,Reference Melby, Osterberg and Resch59,Reference Roberts, Zinchenko and Mahbubani61) , randomised double-blind trial (n 1)(Reference Monteyne, Martin and Jackson60), counterbalanced trial (n 1)(Reference MacKenzie-Shalders, Byrne and Slater57) and randomised, double-blind, placebo-controlled trial (n 1)(Reference Ballard, Melby and Camus56). Dietary intake was measured using a wide variety of tools, such as direct observation (n 1)(Reference Ballard, Melby and Camus56), 24-h recall (n 1)(Reference MacKenzie-Shalders, Byrne and Slater57), 7-d food record (n 1)(Reference MacKenzie-Shalders, King and Byrne58), ad libitum buffet meal (n 3)(Reference Melby, Osterberg and Resch59–Reference Roberts, Zinchenko and Mahbubani61), electronic food record (n 1)(Reference Antonio, Ellerbroek and Silver44) and diet record (n 1)(Reference Roberts, Zinchenko and Mahbubani61). Investigated factor outcomes were measured using a variety of tools, including visual analogue scale (VAS) for measuring appetite (n 4)(Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59–Reference Roberts, Zinchenko and Mahbubani61) , nutrition knowledge questionnaire for measuring nutrition knowledge (n 1)(Reference MacKenzie-Shalders, King and Byrne58), digital scales (n 2)(Reference Antonio, Ellerbroek and Silver44,Reference MacKenzie-Shalders, Byrne and Slater57) , DXA (n 1)(Reference MacKenzie-Shalders, Byrne and Slater57) and BODPOD (n 1)(Reference Antonio, Ellerbroek and Silver44) for measuring body composition. Total energy intake ad libitum meal was significantly lower for those who consumed carbohydrate supplements before the meal than those who did not(Reference Melby, Osterberg and Resch59), as well as those consuming protein supplementation v. carbohydrate supplementation(Reference Monteyne, Martin and Jackson60). However, Roberts et al.(Reference Roberts, Zinchenko and Mahbubani61) identified significant differences between moderate-protein and high-protein diet groups in ad libitum buffet consumption, with an increase in protein intake and decrease in carbohydrate intake in the high-protein diet intervention group. No significant differences were found in total energy intake for three of the included studies(Reference Ballard, Melby and Camus56–Reference MacKenzie-Shalders, King and Byrne58). The Ballard et al.(Reference Ballard, Melby and Camus56) study evaluated the impact of carbohydrate supplementation v. a placebo beverage prior to acute resistance exercise. MacKenzie-Shalders et al.(Reference MacKenzie-Shalders, Byrne and Slater57) explored the impact of whey protein supplement dose variation (20, 40, 60 or 80 g of protein). MacKenzie-Shalders et al.(Reference MacKenzie-Shalders, King and Byrne58) investigated the consumption of protein supplementation as a between-meal supplement v. consumption of the protein supplementation with meals. Interventions exploring appetite in relation to macronutrient adjustment had mixed results, with some studies indicating no significant difference in appetite due to the intervention(Reference Ballard, Melby and Camus56,Reference MacKenzie-Shalders, Byrne and Slater57,Reference Melby, Osterberg and Resch59–Reference Roberts, Zinchenko and Mahbubani61) and some studies having a significant difference in appetite/satiety based on time(Reference Monteyne, Martin and Jackson60,Reference Roberts, Zinchenko and Mahbubani61) . Body composition was not significantly impacted by macronutrient adjustment(Reference Antonio, Ellerbroek and Silver44,Reference MacKenzie-Shalders, King and Byrne58) in any of the studies that reported on this outcome. MacKenzie-Shalders et al. found a significant correlation between the average total energy intake and total change in lean mass in an intervention exploring protein supplementation timing(Reference MacKenzie-Shalders, King and Byrne58).
Five of the included studies evaluated the impact of physical activity on dietary intake and one or more factor that influences diet intake, such as appetite (n 4)(Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59,Reference Holliday and Blannin64,Reference Kojima, Ishibashi and Ebi65) and body composition (n 1)(Reference Barr and Costill66). Two studies also included macronutrient adjustment through supplementation as part of the intervention(Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59) . Interventions utilised included increases in exercise between groups(Reference Holliday and Blannin64,Reference Barr and Costill66) and some with a rest condition used as the control(Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59) , as well as a study utilising both increases in exercise and a rest control(Reference Kojima, Ishibashi and Ebi65). The outcomes measured across these studies were VAS to measure appetite (Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59,Reference Holliday and Blannin64,Reference Kojima, Ishibashi and Ebi65) and skinfolds to measure body composition (Reference Barr and Costill66). Dietary intake was measured through ad libitum test meals in three studies (Reference Melby, Osterberg and Resch59,Reference Holliday and Blannin64,Reference Kojima, Ishibashi and Ebi65) , one study used 2-d food intake records (Reference Barr and Costill66) and one study used direct observation of food consumed at a buffet that was subsequently corrected for energy consumed within the carbohydrate beverage that was part of the intervention (Reference Ballard, Melby and Camus56). The majority of studies using a physical activity intervention were randomised crossover trials (n 4) (Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59,Reference Holliday and Blannin64,Reference Kojima, Ishibashi and Ebi65) , with one quasi-experimental trial (Reference Barr and Costill66). Two studies identified compensatory eating occurred after exercise. A significantly higher energy intake and carbohydrate intakes were identified in groups completing a longer physical activity sessions compared with those completing shorter physical activity sessions (Reference Barr and Costill66), which was in line with increased energy and carbohydrate requirement for fuelling this increase in exercise as suggested by athlete nutrition guidelines (Reference Thomas, Erdman and Burke1). Energy, protein (g) and fat (%) intakes measured through ad libitum test meals were significantly lower in the exercise group v. the resting control group, while carbohydrate (%) intake was significantly higher (Reference Kojima, Ishibashi and Ebi65). Three studies did not identify any significant differences in total energy intake between those who exercised and those who did not (Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59) , as well those who exercised different amounts (Reference Holliday and Blannin64). Appetite was affected in all studies measured, shown to significantly differ between exercise and no exercise conditions (Reference Ballard, Melby and Camus56,Reference Melby, Osterberg and Resch59,Reference Kojima, Ishibashi and Ebi65) and a significant main effect for time, with appetite rising after exercise until the consumption of the ad libitum test meal (Reference Holliday and Blannin64). Barr and Costill found no significant differences in skinfold between groups performing longer and control training regimens (Reference Barr and Costill66). Holliday and Blannin found no significant correlations between dietary intake and measures of appetite (VAS) through a physical activity intervention with differing durations of intense aerobic exercise (Reference Holliday and Blannin64).
Kojima et al. (Reference Kojima, Kasai and Kondo67) use a whole-body cryotherapy intervention compared with a control group in a randomised crossover trial which received no whole-body cryotherapy to investigate appetite and subsequent dietary intake. Dietary intake was measured by an ad libitum buffet meal, while appetite was measured using a VAS and temperature was measured using NT logger monitor N543. Dietary intake for the intervention group was found to be significantly higher than the control group that rested post-cycling protocol. Non-significant changes in macronutrient intakes included decreased carbohydrate intake and increased fat intake, while protein intake remained steady. Hunger was found to be significantly lower in the intervention group receiving whole-body cryotherapy at 0- and 15-min intervals post-exercise and post-ad libitum meal consumption.
Quality assessment
Quality assessment scores range between 33·3 % and 90·0 % (See Table 3). One paper scored > 80 % (Reference Rossi, Landreth and Beam45), nineteen papers scored between 50 % and 80 %, and four papers scored < 50 %. The research question was mostly well defined across studies (n 21 of 24, 87·5 %). Participant selection was poorly described across the majority of studies (n 3 of 24, 12·5 %), with eligibility criteria or sampling method often not described and samples being unrepresentative of the population. Blinding was not carried out in the majority of studies (n 3 of 21, 19 %), which was largely noted as an issue due to the inability to blind participants to the type of intervention they were receiving. Withdrawals were identified within thirteen studies, a small number of studies discuss methods of handling withdrawals (n 5 of 13, 38·5). All papers within this review utilised valid measures for dietary intake.
Table 3. Quality assessment using Quality Criteria Checklist: Primary Research(43)
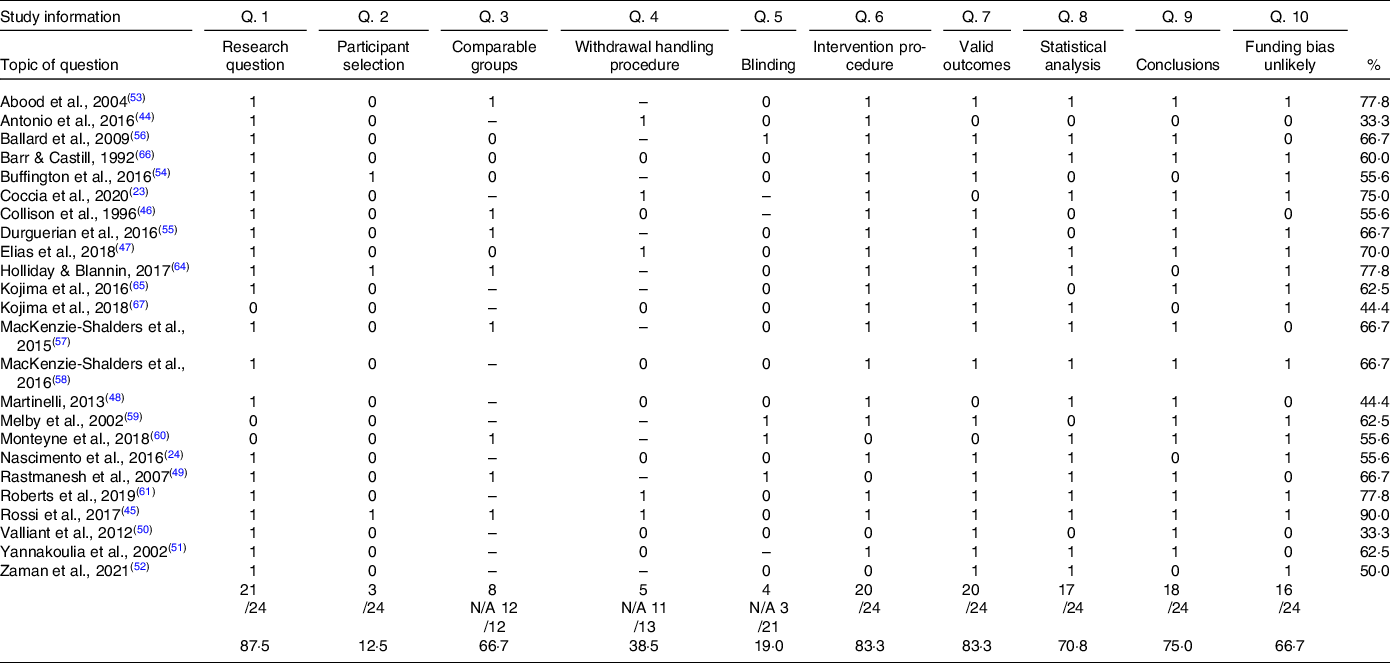
Note. 1 = yes, 0 = no/unclear, - = question is not applicable to this study.
Discussion
The purpose of this review was to investigate the types and effectiveness of interventions used to impact factors that nutrition professionals can target to influence the dietary intake of athletes. Of the twenty-four papers included within this review, it was found that more studies utilised a nutrition education intervention (n 10) than any other type of intervention. Similarly, the most common factor being investigated was nutrition knowledge (n 12), with three included studies that focused on nutrition knowledge exploring additional factors (Reference Coccia, Fernandes and Altiti23,Reference Rossi, Landreth and Beam45,Reference Yannakoulia, Sitara and Matalas51) .
Intervention impact on factor being investigated
The impact that interventions have on factors being investigated must be considered. The most common factor explored was nutrition knowledge (n 12), which was predominantly investigated using nutrition education interventions. Each study exploring nutrition knowledge (n 10) reported a significant increase in pre- and post-intervention scores (Reference Coccia, Fernandes and Altiti23,Reference Nascimento, Silva and Ribeiro24,Reference Rossi, Landreth and Beam45–Reference Valliant, Emplaincourt and Wenzel50,Reference Zaman, Muhamad and Jusoh52) . In addition to nutrition education intervention, cognitive theory-based interventions were used to impact nutrition knowledge in two of the included studies, with both studies reporting significant increases in nutrition knowledge scores in groups receiving the cognitive theory-based intervention(Reference Abood, Black and Birnbaum53,Reference Buffington, Melnyk and Morales54) . As the cognitive theory-based interventions appear to be quite closely related to nutrition education interventions, it is possible that the commonalities of these interventions account for the ability of these two intervention types to positively impact nutrition knowledge. These results somewhat concur with Tam et al. (Reference Tam, Beck and Manore15) review of the effectiveness of education interventions designed to improve nutrition knowledge in athletes where the majority (30/32 studies) reported significant improvement in nutrition knowledge within athlete populations. It is not surprising that nutrition education improves nutrition knowledge, as they often target this factor within the education programme. Nutrition education interventions should remain a mainstay of interventions for improving nutrition knowledge, as they have proven effective in the past(Reference Janiczak, Devlin and Forsyth14,Reference Trakman, Forsyth and Devlin68) . It is not possible here to comment on which aspect of nutrition education interventions is best, as the interventions included are widely varied and not well documented in research studies. It would be prudent for future research to investigate types of education interventions. It is recommended that interventions are more thoroughly described within articles. As this factor can be effectively modified, it is prudent to have nutrition knowledge be a focus or inclusion within interventions. An underexplored area is how improvements in nutrition knowledge translate to dietary intake and subsequent outcomes.
Hunger and appetite were factors explored in eight of the twenty-four included studies. Interventions related to modifying physical activity or macronutrient adjustment interventions were found to impact hunger results. This is unsurprising given that physical activity and macronutrient manipulation are thought to have a relationship with hunger levels. In contrast to the studies included in this review, a study into hunger and appetite in regularly exercising women, who did not meet the definition for athletes, found a significant reduction in hunger due to their standard exercise regimens(Reference Howe, Hand and Larson-Meyer69). It may be beneficial for future research to consider utilising programmes that are aimed at modifying athletes’ dietary intake to include components relevant to modifying macronutrient intake (through supplementation or overall diet pattern change), especially within athlete groups where hunger or appetite are concerns for meeting/exceeding energy intake requirements. A nutrition education intervention was not used within these studies to explore hunger and appetite. Further exploration of how hunger and appetite may be modified through nutrition education interventions is necessary, as these interventions have been shown to be effective in modifying nutrition knowledge and dietary intake. These education interventions may focus on methods of modifying hunger and appetite through dietary strategies. However, due to athletes participating in regular and rigorous physical activity, it may not be appropriate to explore the relationship between physical activity and hunger/appetite and subsequent dietary intake due to disruption or potential impact to the athlete’s regimen, so other strategies may be needed. A possible strategy for athletes from weight category sports experiencing increases in hunger due to exercise may be to provide strategies for high-volume, low-energy foods. Alternatively, if an athlete has high-energy needs and exercise has decreased appetite, strategies for low-volume, high-energy foods may be beneficial.
Body composition was explored within six of the twenty-four included studies(Reference Nascimento, Silva and Ribeiro24,Reference Antonio, Ellerbroek and Silver44,Reference Rossi, Landreth and Beam45,Reference Buffington, Melnyk and Morales54,Reference MacKenzie-Shalders, King and Byrne58,Reference Barr and Costill66) . The results for these studies were varied, with three studies using some form of nutrition education intervention showing significant differences in body composition outcomes(Reference Nascimento, Silva and Ribeiro24,Reference Rossi, Landreth and Beam45,Reference Buffington, Melnyk and Morales54) . These findings indicate that body composition may be effectively impacted through education interventions, which supports previous evidence of nutrition education interventions significantly improving body composition in athletes(Reference Sanchez-Diaz, Yanci and Castillo70). It is worth noting the included studies cover a wide variety of sports, which have different recommendations and requirements for body composition. For this reason, it would be beneficial for future research to include some exploration of body composition within different sports and player position for team sports. The use of specialised nutrition education programmes to empower athletes to safely make these changes would be beneficial long term, with the supervision of sports nutrition/dietetics professionals. By empowering and educating athletes, it may be possible to increase adherence to dietary recommendations and improve health outcomes after their athletic career.
Other factors that were explored within this review include macronutrient contribution to total energy intake, self-efficacy, body image, stress and anxiety, and use of weight control measures. However, these factors have an insufficient number of papers included to provide any conclusion as to the effectiveness of interventions in their modification. Further research is required for other factors that influence dietary intake to support any conclusions. As above, it may be beneficial to include these factors in investigations using a nutrition education intervention.
Intervention impact on dietary intake
As well as exploring how interventions impacted each of the factors being investigated, it was also important to consider how dietary intake was impacted by each intervention. The most common intervention utilised was the nutrition education intervention (ten out of twenty-four studies), which resulted in significant positive changes in some measure of dietary intake in five of the ten studies(Reference Coccia, Fernandes and Altiti23,Reference Rossi, Landreth and Beam45,Reference Elias, Saad and Taib47,Reference Valliant, Emplaincourt and Wenzel50,Reference Zaman, Muhamad and Jusoh52) . A previous review of the impact of nutrition education interventions on dietary intake in athletes found that about two-thirds of studies (14/22 studies) had a significant change in at least one aspect of dietary intake per study, although these results were inconsistent(Reference Boidin, Tam and Mitchell12). The Spronk et al.(Reference Spronk, Heaney and Prvan22) review identified that the majority of studies (19/29 studies) had a weak, positive relationship between higher nutrition knowledge and positive dietary behaviours in the general population. A previous study in general population children found a significant change in fruit intake, but no other variable(Reference Anderson, Porteous and Foster71). While interventions other than nutrition education have been explored within the included studies, the results of these studies indicate that there has not been such a significant impact on dietary intake through interventions other than nutrition education as through nutrition education intervention themselves or intervention types have not been utilised widely enough to draw conclusions about their effectiveness. The macronutrient adjustment intervention was included within this review based on the Birkenhead and Slater(Reference Birkenhead and Slater16) review, which noted that macronutrient intake imbalances may lead to increased total consumption. Two of the seven included studies(Reference Antonio, Ellerbroek and Silver44,Reference Monteyne, Martin and Jackson60) which utilised a macronutrient adjustment intervention reported significant change in energy intake. While there is evidence that macronutrient composition of the diet can impact health outcomes(Reference Birkenhead and Slater16,72) and body composition(Reference Castro, de Araújo and Olimpio73), this review calls into question whether alteration of macronutrient contribution to total energy intake in an ad libitum diet has a positive impact on dietary intake (energy and macronutrient intake) or has sufficient impact to be considered for intervention use. Adjustment to macronutrient intake in athletes has long been used to impact performance, with carbohydrate periodisation used for improved carbohydrate availability and performance during competition(Reference Rothschild, Kilding and Plews74,Reference Routledge, Di Michele and Graham75) , as well as protein consumption after exercise being adjusted to improve muscle protein synthesis(Reference Thomas, Erdman and Burke1). Similarly, two of the five included studies(Reference Kojima, Ishibashi and Ebi65,Reference Barr and Costill66) using a physical activity intervention reported no significant change in dietary intake in the intervention group. The Donnelly et al.(Reference Donnelly, Herrmann and Lambourne76) review in healthy adults identified that the majority of included studies showed no significant changes in energy or macronutrient contribution to total energy intake with increased physical activity.
Correlation between dietary intake and factors being investigated
Only two of the included studies(Reference MacKenzie-Shalders, King and Byrne58,Reference Holliday and Blannin64) explored the relationship between dietary intake and their respective factors being investigated of appetite and body composition. This relationship between dietary intake and nutrition knowledge has been explored in cross-sectional studies(Reference Janiczak, Devlin and Forsyth14); however, it is not possible to demonstrate causality with this study design. Based on the data gathered within this review, it is not possible to comment on how this relationship between dietary intake and investigated factors is moderated. Due to this lack of evidence, further studies exploring this relationship are needed.
Strengths and limitations
Strengths of this study include the use of multiple researchers to complete screening and data extraction processes, which reduced likelihood of reviewer bias. The use of a wide range of databases to complete searches allowed for a comprehensive view of available publications. The quality of this review was enriched by the use of previously established frameworks of factors that impact dietary intake in athletes. There have been no previous reviews that explored these factors being investigated and dietary intake in relation to the interventions used, making this a novel review. Some limitations of the methodology for this review were the exclusion of grey literature and non-English studies. In this review, we have chosen to focus on the factors identified as we were interested in factors that could be modified in interventions. However, other factors exist that could influence dietary intake in athletes (Reference Birkenhead and Slater16,Reference Pelly, Thurecht and Slater17)
Quality assessment
The majority of papers within this review (19/24 studies) had moderate scores between 50 and 80 %. Boidin et al.(Reference Boidin, Tam and Mitchell12) review found poor study quality within single-arm studies and fair study quality within double-arm studies for intervention studies exploring dietary intake and nutrition education in athletes, with a poor reporting of intervention compliance and dietary intake collection methods. A review by Sanchez-Diaz et al.(Reference Sanchez-Diaz, Yanci and Castillo70) exploring the impact of nutrition education interventions on eating habits, nutrition knowledge, body composition and physical performance found that majority of studies exploring these factors had poor-to-good methodological quality. The quality of studies within the current review may show a higher quality of papers as compared with previous reviews.
Future direction
Future directions for study may focus on factors that have been identified as having less primary research into their impact on dietary intake, such as cognitive theory-based interventions, weight loss practices and whole-body cryotherapy. The data gathered within this review could be used to develop an intervention focused on impacting multiple factors that influence dietary intake. Creation of an intervention to improve outcomes for both factors investigated here and dietary intake would allow researchers to focus on factors that athletes believe are most necessary to improve their performance and experience. Nutrition education is common and has been found to be effective in modifying targeted factors and dietary intake; therefore, it would be beneficial to explore this intervention type further with additional factors. It is not possible to say what type of nutrition education is most effective, as there is a great deal of heterogeneity within previous interventions. Therefore, it would be useful to explore the effectiveness of elements of education programmes in future studies. This review identified that no previous studies (between 1992 and 2022) have engaged the athletes or club-based stakeholders in creation of interventions (specifically nutrition education interventions) (77); by following this process of co-design, stakeholders would provide feedback to better target education interventions and increase engagement. Therefore, it would be beneficial for future athlete studies to utilise a co-design method for creation of interventions, involving a variety of shareholders from athletes, coaching teams and nutrition/dietetic professionals.
Conclusion
The aim of this review was to explore types and effectiveness of interventions used to influence factors that impact dietary intake and dietary intake in athletes. It was hypothesised that the results of this review would inform future intervention design. About half of the interventions led to improvements in dietary intake. Despite interventions having targeted factors theoretically proposed to influence dietary intake, dietary intake was unchanged in several of the studies included in this review. Nutrition education interventions are likely the most common as they are easy to implement. Future nutrition education interventions may need to focus on translating changes in dietary intake through increased nutrition knowledge. A framework around the creation and use of these interventions would be useful for consistency of delivery and replicability. It would be beneficial to incorporate practical or procedural knowledge within these interventions and to involve athletes in the development of interventions through co-design.
Acknowledgements
This review has been completed as part of a PhD project at La Trobe University, Australia, which has been supported by the Australian Government Research Training Program scholarship.
A. J. completed project conceptualisation, planning, independent screening, data extraction, and quality assessment and drafted the manuscript. G. L. T. completed project conceptualisation, independent screening, data extraction, and quality assessment, assisted with manuscript preparation, and provided primary supervision. A. F. and R. A. completed project conceptualisation, independent screening, data extraction, and quality assessment, assisted with manuscript preparation, and provided supporting supervision.
The authors declare no conflict of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114523001769







 Open access
Open access