



Childhood maltreatment
There is an increasing interest in understanding the effects of early adverse developmental experiences. Childhood maltreatment, which includes physical, sexual and emotional abuse and neglect, is common worldwide, with paediatric prevalence rates of 13–36%.1 It has been associated with a host of adverse consequences, including abnormal error processingReference Lim, Hart, Mehta, Simmons, Mirza and Rubia2 and impaired attention, inhibition, emotion and reward processing.Reference Hart, Lim, Mehta, Simmons, Mirza and Rubia3,Reference Lim, Hart, Mehta, Simmons, Mirza and Rubia4 Large-scale epidemiological studies found that childhood maltreatment is significantly associated with first onsets of various psychiatric disorders, including mood, anxiety and substance use disorders.Reference Green, McLaughlin, Berglund, Gruber, Sampson and Zaslavsky5 The psychopathological outcomes associated with childhood maltreatment may be mediated by the disruption of neural underpinnings.Reference Bremner and Vermetten6
Several structural magnetic resonance imaging (MRI) studies found that childhood maltreatment is associated with grey matter volume (GMV) abnormalities, particularly in the inferior frontal gyrus (IFG)Reference Mackes, Golm, Sarkar, Kumsta, Rutter and Fairchild7 and limbic regions,Reference Kirsch, Tretyak, Radpour, Weber, Nemeroff and Fromme8 as well as the somatosensory and visual regions.Reference Tomoda, Navalta, Polcari, Sadato and Teicher9,Reference Tomoda, Polcari, Anderson and Teicher10 Meta-analytical studies showed that childhood maltreatment is associated with GMV reductions in prefrontal cortex (PFC)-limbicReference Paquola, Bennett and Lagopoulos11 and ventrolateral PFC-limbic-temporal and somatosensory regions that are known to mediate cognitive control, emotion and sensory processing, which are typically compromised in this population.Reference Lim, Radua and Rubia12 Furthermore, recent large-scale transdiagnostic studies have found that childhood maltreatment is linked to inferior frontal GMV reductions,Reference Begemann, Schutte, van Dellen, Abramovic, Boks and van Haren13 whereas emotional childhood trauma is associated with GMV alterations in the PFC-limbic and sensory networks.Reference Popovic, Ruef, Dwyer, Antonucci, Eder and Sanfelici14
Maltreated young people also had reduced cortical thickness in the frontal-limbic and sensoryReference Lim, Hart, Mehta, Worker, Simmons and Mirza15,Reference McLaughlin, Sheridan, Winter, Fox, Zeanah and Nelson16 regions. In adults, reduced left somatosensory cortical thickness was associated with childhood sexual and emotional abuse,Reference Heim, Mayberg, Mletzko, Nemeroff and Pruessner17 whereas individuals exposed to domestic violence during childhood had reduced cortical thickness in bilateral lingual gyri.Reference Tomoda, Polcari, Anderson and Teicher10
Peer victimisation
Peers are important for a child's social development, but they can also be a substantial source of interpersonal stress during childhood. Peer victimisation is characterised by repetitive aggressive behaviour engaged in by an individual or peer group, with the intension to cause harm to the victim.Reference Olweus and Hart18 It can take several forms, including overt confrontation between the perpetrator and the victim, as well as relational aggression, reputational aggression and ostracism. peer victimisation is a serious global issue, with paediatric prevalence rate of 30%.Reference Currie and Morgan19 Several large-scale prospective studies reported that peer victimisation has deleterious developmental and mental health outcomes, including poor school performance and development of psychiatric disorders such as anxiety and depression.Reference Takizawa, Maughan and Arseneault20 Cohort studies in the UK and USA even found that peer victimisation in childhood had worse long-term adverse effects on young adults’ mental health than childhood maltreatment.Reference Lereya, Copeland, Costello and Wolke21
The field of early-life stress has made much progress in documenting the neurobiological effects of childhood maltreatment, but research investigating neural alterations in peer victimisation is relatively limited. peer victimisation has been associated with decreased medial orbitofrontal cortex (OFC)Reference Vargas, Damme and Mittal22 GMV and increased fusiform cortical thickness.Reference Muetzel, Mulder, Lamballais, Cortes Hidalgo, Jansen and Guroğlu23 However, it remains unclear if the structural abnormalities observed were specifically associated with peer victimisation, given that childhood maltreatment and peer victimisation have additive effects on mental health outcomes and maltreated children are at increased risk of subsequent victimisation by peers, possibly via altered neurocognitive functioning.Reference Goemans, Viding and McCrory24 Therefore, it is imperative that studies examine peer victimisation in the absence of prior exposure to childhood maltreatment from carers.
MAOA gene
Although childhood trauma is an important risk factor for several psychiatric disorders, it does not invariably lead to dysfunction. It is recognised that genetic differences influence the likelihood that trauma exposure will result in psychopathology. The monoamine oxidase type A (MAOA) gene, which selectively metabolises serotonin, norepinephrine and dopamine,Reference Shih, Chen and Ridd25 has emerged as an important genetic factor in relation to psychopathology. The MAOA influences the regulation of the hypothalamic-pituitary-adrenal axis response to stress, which may occur through the hippocampus and other limbic areas. Corticosteroids have a profound effect on cells in the hippocampus through hippocampal glucocorticoid receptors, where chronic stress can cause hippocampal atrophy.Reference McEwen, Nasca and Gray26 Furthermore, stress interacts with the MAOA gene, resulting in differences in hippocampal activation and functional connectivity with other limbic regions during emotional tasks.Reference Sun, Ming, Zhong, Dong, Li and Xiong27
Therefore, the aim of this study was to examine the common and specific neural effects of childhood interpersonal stress from carers (childhood maltreatment) and peers (peer victimisation), by conducting both region-of-interest (ROI) and whole-brain structural (GMV, cortical thickness) analyses on a community sample of healthy youths free from psychopathology, drug misuse and medications. Given that childhood maltreatment is associated with GMV deficits in inferior frontal-limbic and sensory regions,Reference Paquola, Bennett and Lagopoulos11,Reference Lim, Radua and Rubia12 we hypothesised that the childhood maltreatment group, and the peer victimisation group to a lesser extent, would have structural abnormalities particularly in the IFG, insula, postcentral and lingual regions. We also explored the interactional effects of exposure to childhood interpersonal stress (childhood maltreatment and peer victimisation) and MAOA genotype on the hippocampus, the most stress-sensitive structure in the brain.
Method
Participants
Potential participants were recruited from the community via advertisement in social clubs and organisations and on social media. Exclusion criteria were childhood sexual abuse, drug abuse, psychotropic medications, neurological abnormalities, brain injuries, intellectual disabilities and a history of or current psychiatric disorders. We first conducted a thorough pre-screening interview via phone to assess the inclusion/exclusion criteria and severity of the early-life stressful experiences by using the Childhood Trauma Questionnaire (CTQ),Reference Bernstein and Fink28 Revised-Peer Experiences Questionnaire (RPEQ)Reference Prinstein, Boergers and Vernberg29 and European Cyberbullying Intervention Project Questionnaire (ECIPQ).Reference Del Rey, Casas, Ortega-Ruiz, Schultze-Krumbholz, Scheithauer and Smith30 Inclusion criteria for the childhood maltreatment group were non-sexual maltreatment from carers before the age of 13 years, scoring above the cut-off for moderate severity on at least one of the CTQ subscales, but no experience of peer bullying. Inclusion criteria for the peer victimisation group were frequently bullied by peers before the age of 13 years, scoring at least ‘a few times’/‘once a month’ on the RPEQ and ECIPQ, but no history of maltreatment from carers (scoring below the cut-offs for none/low severity on all the CTQ subscales). The control group should not have any experience of maltreatment from carers and victimisation from peers (scoring below the same cut-offs as above). Interested volunteers that were deemed suitable were next invited to participate in the study, and those who were unsuitable were notified and their information deleted immediately during this stage. A total of 108 youths (35 in the childhood maltreatment group, 35 in the peer victimisation group and 38 controls; age range: 17–21 years) participated in the study.
All participants and their guardians provided written informed consent and were reimbursed. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human participants were approved by the Nanyang Technological University (NTU)'s Institutional Review Board (approval number IRB-2018–01–025) and all MRI scans were reviewed by a neuroradiologist.
Study design and procedure
The study consisted of a face-to-face interview and an MRI session that took place either on the same day or on different days within a 1-week period. During the interview session, all participants completed the following: DSM-5 Level-1 Cross-Cutting Symptom Measure and the KSADS-PL (Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime Version) interviews for psychopathology, Strengths and Difficulties Questionnaires (SDQ),Reference Goodman31 Beck Depression Inventory (BDI),Reference Beck, Steer and Carbin32 Beck Anxiety Inventory (BAI)Reference Beck, Epstein, Brown and Steer33 and the Negative and Positive Affect Scale (NAPAS).Reference Mroczek and Kolarz34 The Childhood Experience of Care and Abuse (CECA) interviewReference Bifulco, Brown and Harris35 was used to corroborate the CTQ. IQ was assessed with the Wechsler Abbreviated Scale of Intelligence.Reference Wechsler36 Socioeconomic status was measured with six items (on parental educational level, housing size and type) from the Family Affluence Scale.Reference Currie, Elton, Todd and Platt37 Lastly, recent stressful life events (RSLEs) was assessed with common stressors adapted from the Life Event Questionnaire for Adolescents,Reference Masten, Neemann and Andenas38 where participants rated the 12-month incidence and distress level of each stressor. A total RSLE score was calculated by summing the number of items that were rated as quite or very stressful. In the present study, the internal consistency of the questionnaires ranged from 0.88 to 0.93.
Imaging acquisition and processing
All participants underwent high-resolution T1-weighted MRI on a 3T Siemens MAGNETOM Prisma (Siemens Healthcare GmbH, Germany) at NTU, with a 64-channel head coil and a MPRAGE sequence (repetition time 2200 ms, echo time 2.28 ms, T1 = 994 ms, 208 slices, isotropic voxel size 1 mm3, flip angle 8° and field of view 260 mm).
Images were first visually inspected for artefacts and structural abnormalities. Next, GMV and cortical thickness analyses were conducted with voxel-based morphometry and surface-based morphometry, respectively, using the standard fully automated processing pipelines with default parameters in the Computational Anatomy Toolbox (CAT12.8 for Windows; www.neuro.uni-jena.de/cat/) implemented in SPM12 version 7771 (Statistical Parametric Mapping for Windows; Wellcome Centre for Human Neuroimaging, London, UK; https://www.fil.ion.ucl.ac.uk/spm). After pre-processing, all scans were passed through the automated image quality check protocol in the CAT12 toolbox, and only participants with a minimum weighted average score of B+ in the quality reports were included.Reference Gaser, Reuter and Montag39 Finally, the scans were smoothed with a smoothing Gaussian kernel of 8 mm full width at half maximum (FWHM) for GMV data and 15 mm FWHM for cortical thickness data. The Neuromorphometrics (GMV) and DK40 (cortical thickness) atlases in CAT12 were used for anatomical labelling and ROI extraction. Prior research confirmed that CAT12 accurately measures cortical thickness and can be considered a fast and reliable alternative to FreeSurfer.Reference Seiger, Ganger, Kranz, Hahn and Lanzenberger40
A general linear model was computed for each morphometric measure (GMV and cortical thickness), with group as a between-participant factor, controlling for RSLE (and total intracranial volume (TIV) for GMV analysis). A cluster threshold of P < 0.05 family-wise error (FWE) correction for multiple comparisons was used for the analyses.
Statistical analysis
Statistical analyses were carried out with Statistical Package for the Social Sciences (SPSS) version 26 (for Windows; SPSS Inc., Chicago, IL, USA). Demographic and clinical data were analysed with ANOVA and post hoc t-tests adjusted for multiple comparisons, whereas χ2-test and Fisher's exact test were used for categorical demographic variables. Pearson correlations were used to explore associations between brain metrices and psychological measures within each group. As the ROIs examined were defined a priori and identified independently based on earlier studies, no adjustment for multiple comparisons was made.
MAOA genotyping
DNA was extracted from buccal samples, using the routinely available QIAamp Fast DNA Tissue Kit. After laboratory quality control procedures to evaluate DNA integrity and concentration, all samples were genotyped with the Sequenom Mass ARRAY® primer extension assay. All single nucleotide polymorphism genotyping assays were designed with the Sequenom MassARRAY® genotyping platform, as previously described.Reference Khor, Davila, Breunis, Lee, Shimizu and Wright41
Individuals were stratified and compared based on homozygous major allele carriers for the ten common assayable MAOA single nucleotide polymorphisms (rs2235186, rs3788862, rs3027407, rs1465107, rs5953210, rs2072743, rs1137070, rs979606, rs6323, rs3027400). Exploratory gene×environment analysis was conducted on the bilateral hippocampal GMV, using ANOVA with group (childhood stress: childhood maltreatment and peer victimisation versus controls) and MAOA genotype as between-participant factors, in SPSS version 26.
Results
Participant characteristics
All participants self-reported no history of or current psychiatric disorders, and the information was further corroborated with the DSM-5 Level-1 Cross-Cutting Symptom Measure and the SADS interviews. They also reported no head trauma injuries or loss of consciousness, and had not committed any bullying acts currently or in the past. One participant from the childhood maltreatment group and two participants from the control group had to be excluded because of MRI motion artefacts; they were hence excluded from all analyses. The final sample consisted of 105 participants (34 in the childhood maltreatment group, 35 in the peer victimisation group and 36 controls).
The three groups did not differ significantly in age, gender, IQ, ethnicity and socioeconomic status (Table 1). As expected, the childhood maltreatment and peer victimisation groups scored significantly higher than controls on the BDI, BAI, NAPAS negative affect scale, RSLEs and SDQ emotional and total difficulties (P < 0.01), but lower than controls on the NAPAS positive affect scale (P < 0.001); nevertheless, their depression and anxiety scores were still within normative range below the cut-offs for moderate severity on the BDI and BAI, respectively. The childhood maltreatment and peer victimisation groups did not differ from each other, except on SDQ peer problems, where the peer victimisation group had the highest score (Table 1). RSLE score was used as a covariate in all subsequent analyses to avoid confounding the effects of early-life stress with recent stressors.
Table 1 Demographic characteristics of 34 youths exposed to childhood maltreatment, 35 youths exposed to peer victimisation and 36 controls

a. Tests adjusted for multiple comparisons.
b. The values in parentheses are marginally statistically significant.
c. The age range is 17–21 years.
d. The socioeconomic status total score ranges from 6 to 26, with higher values indicating higher status.
e. The total score is the sum of the physical abuse, emotional abuse, physical neglect and emotional neglect scores.
f. The Fisher's exact test was used.
ROI analysis
GMV
Relative to controls, the childhood maltreatment group had significantly reduced GMV in left postcentral (F(1,66) = 6.72, P = 0.012), IFG (F(1,66) = 4.09, P = 0.047), anterior insula (F(1,66) = 4.05, P = 0.048) and bilateral lingual (left: F(1,66) = 4.07, P = 0.048; right: F(1,66) = 3.95, P = 0.049) regions, as well as marginally smaller GMV in right anterior insula (F(1,66) = 3.53, P = 0.065) and postcentral (F(1,66) = 3.70, P = 0.059) regions (Table 2).
Table 2 Group differences in grey matter volume and cortical thickness of the regions of interest

GMV, grey matter volume.
a. Group differences in GMV were conducted with total intracranial volume and recent stressful life events (RSLE) score as covariates. Group differences in cortical thickness were conducted with RSLE score as a covariate.
b. The values in parentheses are marginally statistically significant.
c. Cortical thickness of the whole insula.
Compared with controls, the peer victimisation group exhibited significantly smaller left lingual GMV (F(1,67) = 4.48, P = 0.038) and marginally smaller right IFG (F(1,67) = 3.63, P = 0.061) and left postcentral (F(1,67) = 3.68 P = 0.059) GMV. The peer victimisation group had marginally larger bilateral (right: F(1,65) = 3.89, P = 0.050; left: F(1,65) = 3.63, P = 0.061) anterior insula GMV than the childhood maltreatment group, thereby suggesting that the reduced anterior insula GMV may be abuse-related whereas the reduced left lingual and postcentral GMV may be related to exposure to early-life interpersonal stress from carers or peers (Table 2).
Cortical thickness
Relative to controls, the childhood maltreatment group had significantly reduced left lingual cortical thickness (F(1,67) = 6.07, P = 0.016), whereas the peer victimisation group had significantly increased cortical thickness in right insula (F(1,68) = 5.20, P = 0.026) and marginally increased in the left IFG (F(1,68) = 3.87, P = 0.050) (Table 2).
Whole-brain analysis
GMV
The childhood maltreatment group had significantly reduced GMV in a cluster comprising left post/precentral, IFG, insula, superior parietal and supramarginal gyri relative to controls (P = 0.018, FWE-corrected) (Table 3, Fig. 1). Mean GMV values of the significant cluster were next extracted for comparison with the peer victimisation group, using analysis of covariance with RSLEs and TIV as covariates. The peer victimisation group also had significantly reduced GMV relative to controls (F(1,67) = 12.3, P = 0.001) only, which was furthermore related to higher ECIPQ cyberbullying score (r = −0.36, P = 0.036, 95% CI −0.67 to −0.03) within the peer victimisation group.
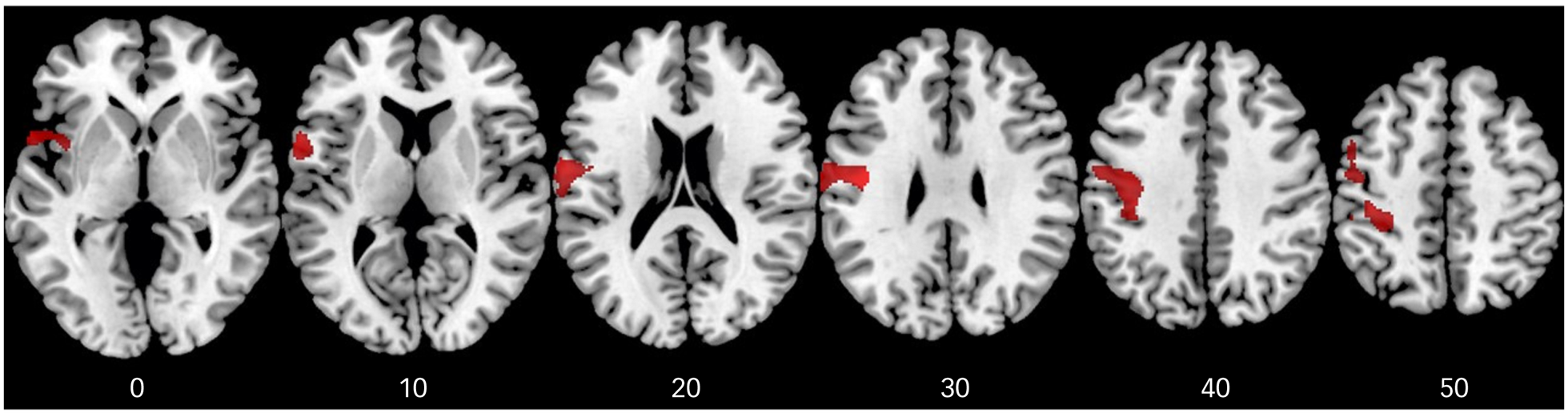
Fig. 1 Axial sections of grey matter volume reduction in the childhood maltreatment group compared with the control group (shown in red), as revealed by F-test (P < 0.05), family-wise error-corrected at the cluster level. The cluster was also significantly reduced in the peer victimisation group relative to the control group only. Axial slices are marked with the z-coordinate as distance in millimetres from the anterior–posterior commissure. The right side of the image corresponds to the right side of the brain.
Table 3 Group differences in grey matter volume in the whole-brain analysis

MNI, Montreal Neurological Institute, FWE, family-wise error.
a. Group differences in grey matter volume were conducted with total intracranial volume and recent stressful life events score as covariates.
b. The cluster was also found to be significantly reduced in the peer victimisation group relative to the control group only.
Cortical thickness
The peer victimisation group had significantly increased cortical thickness in a cluster comprising the left superior frontal, (rostral) anterior cingulate (ACC) and medial OFC relative to the childhood maltreatment group (P = 0.011, FWE-corrected) (Table 4, Fig. 2). This significant medial PFC (mPFC)-ACC cluster was next extracted for comparison with controls, using analysis of covariance with RSLEs as a covariate. The peer victimisation group also had significantly increased cortical thickness relative to controls (F(1,68) = 10.1, P = 0.002), which was furthermore related to higher ECIPQ cyberbullying score (r = 0.34, P = 0.045, 95% CI 0.08–0.66) within the peer victimisation group. There were no significant differences between childhood maltreatment and control groups. Hence, the observed atypical increased cortical thickness of the mPFC-ACC cluster may be related to exposure to peer bullying.

Fig. 2 Significant vertex-wise cortical thickness cluster superimposed on a template reconstruction of brain surface in Montreal Neurological Institute (MNI) space. The significant cluster shows reduced cortical thickness in the childhood maltreatment group compared with the peer victimisation group, as revealed by F-test (P < 0.05), family-wise error-corrected. The cluster was also significantly reduced in the control group relative to the peer victimisation group only. The colour bar represents T statistics.
Table 4 Group differences in cortical thickness in the whole-brain analysis

MNI, Montreal Neurological Institute; few, family-wise error.
a. Group differences in cortical thickness were conducted with recent stressful life events score as a covariate.
b. The cluster was also found to be significantly reduced in the control group relative to the peer victimisation group only.
Exploratory correlational analysis
For the childhood maltreatment group, higher CTQ emotional abuse score was significantly associated with reduced GMV in the bilateral insula (left: r = −0.37, P = 0.034, 95% CI −0.70 to −0.03; right: r = −0.51, P = 0.002, 95% CI −0.81 to −0.20), lingual (left: r = −0.43, P = 0.011, 95% CI −0.75 to −0.10; right: r = −0.52, P = 0.002, 95% CI −0.82 to −0.21), left IFG (r = −0.40, P = 0.018, 95% CI −0.73 to −0.07) and right postcentral (r = −0.36, P = 0.037, 95% CI −0.69 to −0.03) regions. Reduced right lingual GMV was also associated with higher CTQ emotional neglect (r = −0.39, P = 0.024, 95% CI −0.71 to −0.06) and total CTQ (r = −0.37, P = 0.031, 95% CI −0.70 to −0.04) scores.
Exploratory gene×environment analysis
There was a significant stress×MAOA effect on the bilateral hippocampal GMV (left: P < 0.01; right: P < 0.05), resulting from childhood stress-exposed youths without the homozygous major alleles having significantly smaller hippocampal GMV than childhood stress-exposed homozygous major allele carriers and childhood stress-unexposed controls without the homozygous major alleles (Table 5, Fig. 3).

Fig. 3 Significant gene×environment interaction effects between group (childhood stress exposed versus unexposed controls) and MAOA genotype on grey matter volume of (a) left hippocampus and (b) right hippocampus, P < 0.05. GMV, grey matter volume; MAOA, monoamine oxidase type A.
Table 5 Significant group by MAOA genotype on hippocampal grey matter volume

MAOA, monoamine oxidase type A; GMV, grey matter volume.
a. Tests were not adjusted for multiple comparisons.
Discussion
Both parent and peer relationships have been proposed to have an impact on the brain development of young people, yet little research has examined the common and specific neural effects associated with being maltreated by carers and bullied by peers. Moreover, given that childhood maltreatment and peer victimisation have additive effects on mental health outcomes,Reference Shih, Chen and Ridd25 it is imperative for studies to examine peer victimisation in the absence of exposure to adverse caregiving, and to examine childhood maltreatment in the absence of exposure to peer bullying. To our knowledge, this is the first MRI study to do so in a sizable community youth sample free from psychopathology, medications and drug abuse and controlled for the number of RSLEs. This is crucial to elucidate the effects of early-life stress independently from confounding effects associated with recent stressors, psychiatric diagnosis, medications and drug abuse.Reference Lim, Radua and Rubia12
For the ROI analysis, the childhood maltreatment group had reduced left IFG, bilateral anterior insula, postcentral and lingual GMV and left lingual cortical thickness relative to controls, as well as reduced bilateral anterior insula GMV relative to the peer victimisation group. The reduced GMV in bilateral anterior insula, lingual, left IFG and right postcentral regions were furthermore associated with higher emotional abuse, whereas the reduced right lingual GMV was associated with higher emotion neglect and total CTQ scores, within the childhood maltreatment group. The peer victimisation group exhibited reduced GMV in left lingual and postcentral regions, along with increased cortical thickness in left IFG and right insula relative to controls.
At the whole-brain level, both the childhood maltreatment and peer victimisation groups had smaller GMV than controls in a cluster comprising left post/precentral, IFG, insula, superior parietal and supramarginal gyri, which was furthermore related to greater cyberbullying within the peer victimisation group. Furthermore, the peer victimisation group had increased cortical thickness in a cluster comprising the left superior frontal, ACC and medial OFC relative to both childhood maltreatment and control groups, which was also related to greater cyberbullying. Hence, our findings suggest that the reduced anterior insula GMV and increased mPFC-ACC cortical thickness may be related to being maltreated by carers and bullied by peers, respectively, whereas the relatively widespread compromised GMV in inferior frontal-limbic, somatosensory and lingual regions may be related to exposure to early-life interpersonal stress. Finally, our exploratory childhood stress×MAOA analysis on the bilateral hippocampal GMV suggests a protective effect of having homozygous major alleles, particularly in the presence of early-life interpersonal stress.
The IFG is a key area of cognitive control, mediating saliency detection, action selection, inhibition and sustained attention.Reference Rubia, Lim, Ecker, Halari, Giampietro and Simmons42 It is also involved in interpersonal emotion regulation and implementing reappraisal strategies,Reference Grecucci, Giorgetta, Bonini and Sanfey43 along with linguistic processing in the Broca's area, including processing emotional content of speech.Reference Frühholz and Grandjean44 The IFG has been proposed as part of the trauma-disrupted network, where the left IFG, in particular, is implicated in processing aversive and trauma-related information.Reference Lee, Choi, Lee, Yoo, Kim and Kim45,Reference Landre, Destrieux, Andersson, Barantin, Quide and Tapia46 Adolescents exposed to verbal abuse showed hypersensitivity of left IFG to swear words,Reference Landre, Destrieux, Andersson, Barantin, Quide and Tapia45 whereas women with sexual abuse-related post-traumatic stress disorder exhibited left IFG overactivation to trauma-related words.Reference Landre, Destrieux, Andersson, Barantin, Quide and Tapia46 A meta-analysis further found that anger stimuli exhibited a greater association with left IFG activation compared with other emotions.Reference Vytal and Hamann47 The current finding of reduced left IFG GMV is consistent with our meta-analysisReference Lim, Radua and Rubia12 and previous studies in childhood maltreatment.Reference Mackes, Golm, Sarkar, Kumsta, Rutter and Fairchild7 The association of reduced left IFG with adverse caregiving experiences is further underpinned by the observed correlation with emotional abuse, which has a strong linguistic component.
The insula plays a key role in interoceptive awareness and emotion regulation, where the anterior insula, in particular, is involved in the processing of specific negative emotions including fear and disgust,Reference Calder, Lawrence and Young48 which are common in emotional abuse. Studies often implicate the insula in emotion regulation abnormalities in childhood maltreatment. Insula hyperresponsiveness to negative facial expressions has been observed in individuals exposed to childhood maltreatment relative to controls,Reference Hart, Lim, Mehta, Simmons, Mirza and Rubia3 whereas childhood maltreatment scores strongly correlated with insula responsiveness to fearful/angry faces in healthy adults.Reference Dannlowski, Kugel, Huber, Stuhrmann, Redlich and Grotegerd49 The present finding of a possibly abuse-related reduced insula GMV is further supported by the significant corelation with emotional abuse within the childhood maltreatment group, and corroborates earlier findings of insula GMV deficit in childhood maltreatment.Reference Kirsch, Tretyak, Radpour, Weber, Nemeroff and Fromme8 Recent large-scale transdiagnostic studies also underscore the involvement of left (anterior) insula abnormalities in childhood trauma, particularly emotional trauma.Reference Popovic, Ruef, Dwyer, Antonucci, Eder and Sanfelici14
Childhood maltreatment has been associated with abnormal development of the sensory systems that relay adverse sensory experiences. Studies reported reduced lingual GMV in women who experienced childhood sexual and physical abuseReference Tomoda, Navalta, Polcari, Sadato and Teicher9 and in adolescents exposed to severe childhood maltreatment,Reference Lim, Hart, Mehta, Worker, Simmons and Mirza15 as well as reduced lingual cortical thickness in children who experienced psychosocial deprivationReference McLaughlin, Sheridan, Winter, Fox, Zeanah and Nelson16 and in young adults who witnessed domestic violence during childhood.Reference Tomoda, Polcari, Anderson and Teicher10 Reduced left somatosensory GMV in childhood maltreatment has also been reported in meta-analysisReference Lim, Radua and Rubia12 and recent large-scale transdiagnostic studies.Reference Begemann, Schutte, van Dellen, Abramovic, Boks and van Haren13 Thus, the current findings of reduced lingual and somatosensory GMV in maltreated individuals relative to controls, which were furthermore correlated with higher emotional abuse with the childhood maltreatment group, are consistent with earlier studies. Importantly, the peer victimisation group also exhibited similar deficits in left lingual (albeit at a marginal level in left somatosensory) GMV relative to controls. Thus, our findings underscore the detrimental effects of peer victimisation and suggest that the sensory systems that process and interpret adverse sensory inputs may be altered by early traumatic interpersonal experiences from carers or peers.
Our exploratory stress×MAOA analysis on the bilateral hippocampal GMV suggests a ‘protective’ effect of having homozygous major alleles, particularly in the presence of early-life interpersonal stress. Childhood stress, moderated by genetic vulnerability, is associated with reduced hippocampal GMV and increased vulnerability to depression.Reference Masten, Eisenberger, Borofsky, Pfeifer, McNealy and Mazziotta51 Additionally, stress interacts with the MAOA gene, resulting in differences in hippocampal activation and functional connectivity with other limbic regions during emotional tasks,Reference Sun, Ming, Zhong, Dong, Li and Xiong27 where hippocampal deactivation may lead to disinhibition of the hypothalamic-pituitary-adrenal axis and the initiation of stress hormone release under stress. Together, this novel but preliminary evidence suggests that in healthy adolescents, vulnerability to hippocampus alterations may be driven by reduced ‘genetic protection’ in the presence of childhood trauma, which could have implications for targeted prevention of mood disorders.
Finally, although the childhood maltreatment and peer victimisation groups had comparable levels of depression, anxiety, negative affect and SDQ difficulties scores (which were still within normative ranges), they exhibited common and distinct structural abnormalities. Both the childhood maltreatment and peer victimisation groups exhibited early-life stress related reduced GMV in inferior frontal-limbic, somatosensory and lingual regions, whereas abnormalities in anterior insula GMV are likely to be abuse-related. The peer victimisation group had increased cortical thickness in mPFC-ACC regions relative to the childhood maltreatment and control groups, which may possibly reflect a delayed maturation of the regions and the associated emotion processing capabilities. Only one study had investigated whole-brain cortical thickness abnormalities in peer victimisation, and found that children who were frequently victimised by peers had thicker left fusiform gyrus, which could be related to the development of social anxiety disorder, given the role of the fusiform in processing threatening faces.Reference Muetzel, Mulder, Lamballais, Cortes Hidalgo, Jansen and Guroğlu23 Furthermore, studies observed increased activity in the rostral and dorsal ACC in chronically peer-victimised and rejection-sensitive adolescents in response to online peer rejection, which was associated with higher levels of internalising symptoms and distress,Reference Masten, Eisenberger, Borofsky, Pfeifer, McNealy and Mazziotta51,Reference Rudolph, Miernicki, Troop-Gordon, Davis and Telzer52 whereas spending more time with friends reduced ACC response to social exclusion.Reference Masten, Telzer, Fuligni, Lieberman and Eisenberger53 Being rejected based on one's profile pictures also resulted in increased activity in the mPFC.Reference Achterberg, van Duijvenvoorde, van der Meulen, Euser, Bakermans-Kranenburg and Crone54 Adolescents are particularly sensitive to peer rejection, and this is further exacerbated by social media. Cyberbullying has more detrimental effects on adolescent mental health than traditional bullying, and it may be more dangerous as it has an increased potential for a large audience (i.e. the entire virtual world), anonymity and it is not limited to a specific location/time (e.g. during school hours). Given the involvement of the mPFC and ACC regions in appraisal and expression of fear or anxiety, we speculate that the observed thicker mPFC-ACC cluster, which was furthermore correlated with greater cyberbullying, may reflect a delayed maturation of the regions linked to the adolescents’ heightened emotional sensitivity to online peer rejection/bullying, and the ensuing immature emotion processing capabilities may increase their risk of developing psychopathology later on.
Strengths and limitations
Among the strengths of this study are that all participants were free from psychopathology, medications and drug abuse; their current stressors were assessed and controlled for; and the early adverse experiences were carefully corroborated by interviews (e.g. CECA). The generalisability of the results may be restricted to the ‘more resilient’ portion of community youths who did not have any psychiatric disorders despite been exposed to harsh treatment by carers or peers during childhood. Nonetheless, the current findings underscore that early-stress exposed individuals do show neural alterations compared with the early-stress-unexposed controls, even in the absence of psychopathology. Future studies with larger samples should build on the current findings and examine the neural effects of peer victimisation, particularly cyberbullying, in youths. The study is cross-sectional and the findings are still correlational. The gene×environment analysis was exploratory given the sample size and should be interpreted with caution. It is also unclear to what extent malnutrition, levels of social support and duration of early-life stress may have influenced the findings. Finally, the differences in MRI measurements observed may possibly be related to, rather than as direct evidence of, underlying brain structural abnormalities.
In conclusion, early-life interpersonal stress from carers and peers is commonly associated with structural alterations of the inferior frontal-limbic, somatosensory and visual regions that are known to mediate cognitive control, emotion and sensory processing. In addition, childhood maltreatment and peer victimisation may be specifically associated with reduced anterior insula GMV and increased mPFC-ACC cortical thickness, respectively. The peer-victimisation-related thicker mPFC-ACC cluster, which was furthermore correlated with greater cyberbullying, may suggest a delayed maturation of the regions linked to the adolescents’ heightened emotional sensitivity, particularly to online peer rejection/bullying. Our findings underscore the negative effects of being bullied by peers, which is no less detrimental than being maltreated by carers, and the need for future studies to explicitly examine how cyberbullying may affect brain development and increase risk of developing psychopathology in young people.
Data availability
The data that support the findings of this study are available from the corresponding author, L.L., upon reasonable request.
Acknowledgements
We thank all of the individuals and their families who participated in this study.
Author contributions
L.L. conceived and designed the study, recruited the participants and acquired the data. L.L. and C.C.K. analysed the data. L.L. wrote the manuscript, and both authors reviewed the manuscript.
Funding
This study was supported by the Lee Kong Chian School of Medicine, Nanyang Technological University Singapore (NTU) Fellowship Grant, awarded to L.L.
Declaration of interest
None.









 Open access
Open access
eLetters
No eLetters have been published for this article.