



Over 2010–2011, Canterbury experienced four major earthquakes (moment magnitude scale >6.0) and thousands of aftershocks, resulting in major property and infrastructure damage throughout the city, 185 deaths and thousands of injuries.Reference Ardagh, Richardson, Robinson, Than, Gee and Henderson1 A large number of people were exposed to the earthquakes, creating a unique opportunity to examine the cognitive and emotional effects of trauma exposure.
Epidemiological studies have shown that exposure to potentially traumatic events is common, with 70–80% of people experiencing one or more such events over their lifetime.Reference Benjet, Bromet, Karam, Kessler, McLaughlin and Ruscio2 Although there is increased risk of developing a mental health disorder after such exposure,Reference Beaglehole, Mulder, Frampton, Boden, Newton-Howes and Bell3 this occurs in only a minority.Reference Fergusson, Horwood, Boden and Mulder4 Most people follow a trajectory of recovery or resilience, with relatively short-lived distress that settles over time.Reference Galatzer-Levy, Huang and Bonanno5 Although extensive literature reports on the impact of trauma on brain functioning in post-traumatic stress disorder (PTSD), an increasing number of studies have examined outcomes in trauma-exposed but resilient participants, who constitute most of the population. These studies have provided insights into the impact of exposure to trauma on neurocircuitry, cognitive functioning and resilient responses.
Brain functioning and resilience
Neuroimaging studies comparing groups with and without PTSD after trauma exposure have shown greater prefrontal–amygdala activation or connectivity in resilient (without PTSD) groups,Reference Stark, Parsons, Van Hartevelt, Charquero-Ballester, McManners and Ehlers6 which, it is hypothesised, reflects greater top-down regulation of emotion and a resilient response.Reference Shin and Liberzon7 Studies specifically examining the effects of exposure in individuals without PTSD have reported long-term changes, with greater grey matter density in the prefrontal–limbic systems compared with non-exposed controls.Reference Li, Hou, Wei, Du, Zhang and Liu8
Studies of cognitive functioning in PTSD report that differences are significantly less when the comparison group includes trauma-exposed rather than non-trauma-exposed controls.Reference Brewin, Kleiner, Vasterling and Field9,Reference Johnsen and Asbjørnsen10 This suggests that trauma itself may have detrimental effects on cognitive performance not only in people with PTSD, but also in exposed but psychiatrically well people. This would provide support for reports in the general population of ‘earthquake brain’ or ‘flood-brain’ after trauma exposure.Reference Crowe11 Studies specifically addressing this issue have had inconsistent findings. For example, Stein et al. showed that women exposed to intimate partner violence, regardless of PTSD status, had impairment in tasks of attention, working memory, and response inhibition, compared with non-exposed controls.Reference Stein, Kennedy and Twamley12 After exposure to the Canterbury earthquake sequence, no difference was found in performance on cognitive tasks between individuals with PTSD and resilient trauma-exposed individuals. However, both of these earthquake-exposed groups had poorer performance on a test of visuospatial learning and memory compared with non-exposed control groups.Reference Bell, Frampton, Colhoun, Douglas, McIntosh and Carter13 In individuals exposed to urban violence, Flaks et al found no differences in attention and executive functioning between an exposed but psychiatrically well group and a non-exposed control group.Reference Flaks, Malta, Almeida, Bueno, Pupo and Andreoli14 These inconsistent findings may be explained by factors such as age at the time of exposure, type (e.g. natural disaster or sexual assault) and duration of trauma (e.g. single incident such as a motor vehicle accident or chronic repeated events such as intimate partner violence).
Facial emotion processing is a specific aspect of cognitive functioning that has received less attention in relation to trauma exposure. A systematic review of studies of social cognition in PTSD reported mixed findings in the processing of threatening expressions (anger, fear, sadness).Reference Couette, Mouchabac, Bourla, Nuss and Ferreri15 Studies in people with PTSD found decreased accuracy and sensitivity in interpreting facial expressions of fear, sadness,Reference MacNamara, Post, Kennedy, Rabinak and Phan16,Reference Poljac, Montagne and de Haan17 and anger,Reference MacNamara, Post, Kennedy, Rabinak and Phan16 compared with combat-exposed controls. Studies, including our own work following the Canterbury earthquakes, have found that when compared with non-exposed controls, exposed individuals (including those without PTSD) had increased sensitivity for cues of potential threats, including emotional facial expressions, which could help interpret potentially harmful situations rapidly and may therefore, in the short term, be a useful adaptive response.Reference Bell, Colhoun, Frampton, Douglas, McIntosh and Carter18–Reference Pistoia, Conson, Quarantelli, Panebianco, Carolei and Curcio20
We previously assessed cognitive functioning and emotion processing approximately 2–3 years after the Canterbury earthquake sequence in 89 individuals who were exposed to these events but did not develop psychological difficulties, and identified as resilient.Reference Bell, Frampton, Colhoun, Douglas, McIntosh and Carter13,Reference Bell, Colhoun, Frampton, Douglas, McIntosh and Carter18 Similar to those with PTSD, resilient individuals showed clinically significant impairment in visuospatial learning and memory and facial emotion processing compared with a non-exposed group who had completed cognitive testing in other studies before the earthquakes. These findings highlight the importance of understanding cognitive functioning in resilient groups in addition to those with mental health disorders. This may be particularly important after disasters because of the population-wide effects and a resilient response being the most prevalent. If there are persisting impairments in threat sensitivity and cognitive functioning, this may affect people's productivity and could potentially be a target for intervention.
The aim of the current study was to focus on the earthquake-exposed resilient group from our previous work to examine the longer-term cognitive effects of the Canterbury earthquake sequence (approximately 8–9 years after exposure) in a context of reduced ongoing seismic threat (in contrast to the ongoing risk of further earthquakes at the time of the original study). The design was improved from the original study by recruiting a matched non-earthquake exposed control group and expanding the cognitive testing battery. In accord with our previous findings, the hypothesis was that participants in the earthquake-exposed resilient group, compared with non-exposed controls, would perform less well on tests of spatial memory, have increased accuracy for the identification of all facial emotions and exhibit a bias in the misclassification of neutral facial expressions to threat-related emotions.
Method
Participants
Earthquake-exposed resilient participants
This group comprised Canterbury residents who had self-identified as resilient, i.e., coping well, despite moderate-to-high exposure to earthquake-related events (such as physical injury or illness, death of a loved one, witnessing falling buildings, seeing bodies, property loss, income loss or problems with housing caused by earthquake-related events). They were recruited in response to articles, opinion pieces and community notices in local newspapers, and via word of mouth over the course of 13 months, from January 2013 to February 2014. They all had a face-to-face assessment and completed diagnostic and self-report questionnaires, to confirm that they had no earthquake-related psychiatric diagnoses and had not received any earthquake-related counselling. In this current study, this group were retested between July 2018 and March 2020 (approximately 8–9 years after the Canterbury earthquakes in 2010 to 2011). They were recruited from the 101 people who participated in the original studies approximately 2–3 after the Canterbury earthquakes and had consented to be contacted for future research.Reference Bell, Frampton, Colhoun, Douglas, McIntosh and Carter13,Reference Bell, Colhoun, Frampton, Douglas, McIntosh and Carter18 Reasons for exclusion from both the original and current study were current alcohol dependence, lifetime psychotic or bipolar disorder, comorbid neurological or medical conditions, pregnancy, previous serious head injury or taking medications likely to interfere with cognitive testing. All participants were fluent in English.
Non-earthquake-exposed controls
Non-earthquake-exposed control participants, recruited through advertising (using similar methods) between September 2019 and June 2021 in Dunedin, New Zealand (approximately 300 km south of Canterbury), had not been exposed to the earthquakes and had not lived in Canterbury since the earthquakes. Control participants were subject to the same exclusion criteria as earthquake-exposed participants. They were matched with the earthquake-exposed resilient group for age, gender and years of education.
Procedure
Assessments were conducted by research assistants at university research units in Christchurch (earthquake-exposed resilient participants) and Dunedin (non-exposed controls). Each assessment was part of a battery of tests (total duration approximately 180 min), which included diagnostic and psychometric measures, cognitive assessment and a narrative of earthquake experiences (earthquake-exposed group only, reported separately). Research assistants received training in administration of cognitive testing by a clinical psychologist (K.D.).
Cognitive testing
Cognitive testing included a battery of tasks designed to test visuospatial learning and memory, verbal learning and memory, executive functioning, psychomotor speed, sustained attention and social cognition. Pencil-and-paper tasks were administered according to standardised instructions, and computerised tasks according to corresponding manual protocols (E-Prime 2.0 software (Psychology Software Tools, Inc, Sharpsburg PA, USA; see https://pstnet.com/products/e-prime/) and CogState software (CogState Inc, Fitzroy, Melbourne, Australia; see https://www.cogstate.com/academic-research/)) on a PC laptop. The following tasks were administered.
Verbal learning and memory
For the Rey Auditory-Verbal Learning Task (RAVLT),Reference Schmidt21 participants recalled words from a list presented five times (trials 1–5), after a distractor list (trial 6) and after 20 min (trial 7, delay). Number of words recalled in each of the trials from 1 to 7 was recorded, as well as distractor list recall and total learning (sum of trials 1–5).
Visuospatial learning and memory
For the Groton Maze Learning Test (GMLT; CogState), participants navigated a 28-step hidden pathway within a 10-by-10 grid of squares on a computer screen. The process was repeated for four successive learning trials (total of five learning trials) and a delay trial after 20 min. The number of errors for each trial, and over all learning trials, was recorded.
Executive functioning
For the Digit Span Forward and Backward test, participants were read a sequence of numbers and asked to repeat the sequence in order (forward) or in reverse order (backward). Total score (number of sequences correctly recalled) and span length (highest number of digits recalled) were recorded for forward and backward, as well as a total score (forward + backward score).
For the Controlled Oral Word Association Test, a task of verbal fluency, participants generated words starting with a particular letter (C-F-L), for a period of 90 s. The number of words generated for each letter was recorded and summed across the three letters, giving a total score.
The Delis–Kaplan Executive Function System – Fluency BatteryReference Delis, Kaplan and Kramer22 involved two measures of verbal fluency: category fluency, which required participants to generate as many words as possible from designated semantic categories (animals, boys names), and category switching, in which participants alternated between generating words from two different categories (fruit, furniture). Total words generated in both conditions, and total correct switches in the latter condition, were recorded.
Psychomotor speed
The Timed Chase Test (TCT, CogState) served as a control task for the GMLT and involved participants chasing a moving tile around a grid of squares on a computer screen for 30 s. Number of correct moves per second was recorded.
The Digit Symbol Coding Test (DSCT) assessed participants’ ability to correctly draw symbols that corresponded with specific digits under time pressure (90 s). Number of correct responses was recorded.
Sustained attention
In the computerised Vigil Continuous Performance Test,Reference Cegalis and Bowlin23 single randomised letters were presented sequentially on a computer screen for 85 ms, with a 900 ms inter-stimulus interval. Letters were presented in white on a black background. Participants responded when they viewed target ‘K’, only when cued by an earlier ‘A’ stimulus (‘AK’ target sequence). Over the course of 480 stimuli, 100 target sequences are presented in 8 min. These targets were pseudo-randomised, so that 25 target sequences were presented in four blocks (with no breaks between blocks). The number of omissions and commissions were recorded.
Social cognition
The Reading the Mind in the Eyes Test (RMET)Reference Baron-Cohen, Wheelwright, Hill, Raste and Plumb24 is a 36-item task in which participants indicated which emotion best matched the mental state that different eye images were displaying. The task used a pen-and-paper format with black and white images. Forced-choice responding was used, with participants choosing one of four adjectives for each item (e.g. jealous, hateful). There was no time limit to complete the task; however, participants were asked to answer as quickly and accurately as possible. A total score out of 36 was calculated, with higher scores indicating more accurate performance.
Facial expression emotion recognition test
For the Facial Expression Recognition (FER) Test, participants completed a modified version of the FER taskReference Harmer, Bhagwagar, Perrett, Völlm, Cowen and Goodwino25 presented on a computer, using E-Prime software (E-Prime 2.0). Faces displaying five basic emotions (happy, sad, angry, fearful and disgusted) were randomly presented on a screen for 500 ms, followed immediately by a blank screen. Faces had been morphed into varying intensities of each emotion from 50 to 100%, in 10% steps. Neutral facial expressions (0% emotion) were also presented. Participants were instructed to identify the emotions displayed in a forced-choice format as quickly and accurately as possible. Reaction times, recognition accuracy and neutral misinterpretation bias (percentage of neutral expressions misclassified as an emotion) were recorded (for more detailed description, see Douglas and PorterReference Douglas and Porter26).
The RAVLT, GMLT, TCT and DSCT were used in the original study 2–3 years after the start of the earthquake sequence. To prevent practice effects in the earthquake-exposed resilient group, alternative versions were used in the current study.
Diagnostic and psychometric measures
All participants had a diagnostic interview to screen for Axis I mental disorders (Mini-International Neuropsychiatric Interview; MINI), completed the National Adult Reading Test (NART) and the following self-report psychometric measures.
PTSD Checklist-Specific
The PTSD Checklist-SpecificReference Weathers, Litz, Herman, Huska and Keane27 assesses 17 current (past month) symptoms of PTSD in relation to the Canterbury earthquakes (completed only by the earthquake-exposed group). Total symptom scores range from 17 to 85, with scores >44 being in the clinical range.
Depression, Anxiety and Stress Scale
The Depression, Anxiety and Stress Scale (DASS-21)Reference Ng, Trauer, Dodd, Callaly, Campbell and Berk28 assesses 21 symptoms (seven items for depression, anxiety and stress) over the past week. Subscale scores of >14 for depression, >10 for anxiety and >19 for stress are defined as moderate-extreme.
Dissociative Experiences Scale
The Dissociative Experiences Scale (DES)Reference Bernstein and Putnam29 assesses amount of time participant experiences 28 symptoms of dissociation, with higher scores indicating higher dissociation.
Posttraumatic Growth Inventory
The Posttraumatic Growth InventoryReference Tedeschi and Calhoun30 assesses 21 positive outcomes from the earthquakes (earthquake-exposed resilient group only). Scores are summed and range from 0 to 105, with higher scores reflecting greater post-traumatic growth.
Connor–Davidson Resilience Scale
The Connor–Davidson Resilience Scale (CDRS)Reference Connor and Davidson31 assesses 25 resilience items over the past month. Scores are summed and range from 0 to 100, with higher scores reflecting greater resilience.
Social Adjustment Scale
The Social Adjustment Scale (SAS)Reference Weissman and Bothwell32 assesses 45 items of social functioning over the past 2 weeks. Scores are summed and divided by the number of items, and range from 1 to 5.
Traumatic Exposure Severity Scale
The Traumatic Exposure Severity ScaleReference Elal and Slade33 assesses the occurrence of 39 earthquake-related stressors and the distress experienced in relation to these (earthquake-exposed resilient group only).The number of exposures and distress scores are summed.
Life Events Scale
The Life Events Scale (LES) was adapted from the Crisis in Family Systems–Revised Questionnaire,Reference Shalowitz, Berry, Rasinski and Dannhausen-Brun34 and assesses 66 stressful life events (not specifically related to earthquake exposure) in the previous 5 years and the past 6 months. Number of exposures and distress scores are summed.
Childhood Trauma Questionnaire
The Childhood Trauma Questionnaire (CTQ)Reference Bernstein, Fink, Handelsman, Foote, Lovejoy and Wenzel35 retrospectively measures childhood abuse and neglect, rating frequencies of experiences from 1 to 5. Five subscale (emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect) and total scores are produced from summing scores.
State-Trait Anxiety Inventory
The State-Trait Anxiety Inventory (STAI) assesses state (current) and trait (lifetime) symptoms of anxiety, with higher scores indicating greater anxiety.
Ethics
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human patients were approved by the University of Otago, New Zealand Human Ethics Committee (approval number H18/042). All participants provided informed written consent.
Statistical analysis
Statistical analyses were conducted with the Statistical Package for Social Sciences version 26 for Windows. Demographic and clinical data were summarised with standard descriptive statistics, including means, s.d., ranges, frequencies and percentages, as appropriate. Comparison of demographic and clinical variables between the earthquake-exposed and non-exposed controls used ANOVA and chi-squared tests. Comparisons of cognitive data were conducted with ANCOVA, with group as the between-participant factor and age, gender, years of education, anxiety from STAI-state and depression from DASS-21 depression subscale score as covariates to adjust for clinical features known to affect cognitive functioning. Ethnicity, CTQ score and NART score were also used as covariates to adjust for differences between groups. Where tasks had more than one level, an additional within-participants factor of level was added and analysed by repeated measures ANOVA, within a general linear mixed model. A supplementary analysis was completed of performance at 2–3 years (time point 1) and 8–9 years after the earthquakes (time point 2) in the resilient earthquake-exposed controls who had completed cognitive testing at the two time points, using repeated measures ANCOVA, but with an additional within-participants factor of time (time point 1 versus time point 2). A two-tailed P<0.05 was taken to indicate statistical significance.
Results
From the 101 earthquake-exposed resilient participants identified in the original studies, 59 participated in the current study (15 unable to be contacted, seven not interested, four too busy, four unwell, four no longer in Canterbury and eight were members of the University department who, at the time of the current study, had considerable knowledge of the study design and testing). Two participants were excluded because of alcohol dependence when assessed (see Supplementary Figure 1 available at https://doi.org/10.1192/bjo.2022.512). The only statistically significant difference in psychometric and cognitive tests at time point 1, between those who participated in the current study and those who did not, was higher alcohol use before and after the earthquakes, and greater accuracy for neutral expressions from the FER, in the group who did not participate in the current study. Sixty non-exposed controls were recruited..
Table 1 shows that although groups were well-matched on gender, age and years of education, the earthquake-exposed resilient group scored significantly higher on the NART and included a greater proportion of people of New Zealand European origin. Three participants (5%) in the earthquake-exposed resilient group had a current diagnosis of generalised anxiety disorder. Both groups reported functioning well (from the SAS), had negligible rates of mental disorder (from the MINI) and low use of antidepressants. Both groups had low scores on measures of depression (from the DASS-21), anxiety (from the anxiety subscale of the DASS-21 and STAI) and dissociative experiences (from the DES), and high scores on measures of resilience (from the CDRS). Compared with the non-exposed group, the earthquake-exposed resilient group rated significantly higher stress (from the DASS-21 stress subscale), and reported exposure to a greater number of stressful life events and greater difficulty from these over the past 5 years (from the LES). The non-exposed control group scored significantly higher than the earthquake-exposed resilient group on total childhood trauma (from the CTQ emotional abuse and emotional neglect subscales), although all scores were in the categories of none or low abuse.
Table 1 Comparison of demographic and clinical variables between earthquake-exposed and non-exposed groups
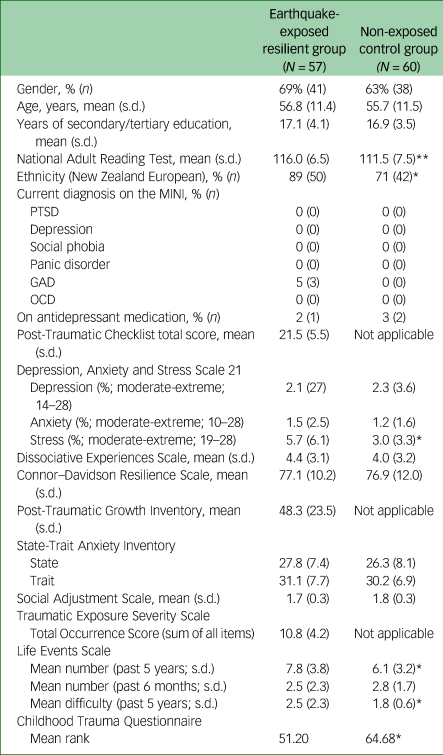
MINI, Mini-International Neuropsychiatric Interview; PTSD, post-traumatic stress disorder; GAD, generalised anxiety disorder; OCD, obsessive–compulsive disorder.
*P < 0.05, **P < 0.001.
Between-group cognitive comparisons
After controlling for demographic and clinical variables (age, gender, years of education, anxiety level from STAI-state, depression symptoms (depression subscale score of the DASS-21), ethnicity, CTQ score and NART scores), the earthquake-exposed group performed significantly better than the non-exposed group on the Total Digit Forward test (F(1,97) = 7.2, P = 0.026) (Table 2). No significant between-group differences on any other cognitive measures were found.
Table 2 Mean scores on cognitive test variables (non-social measures) in earthquake-exposed and non-exposed groups
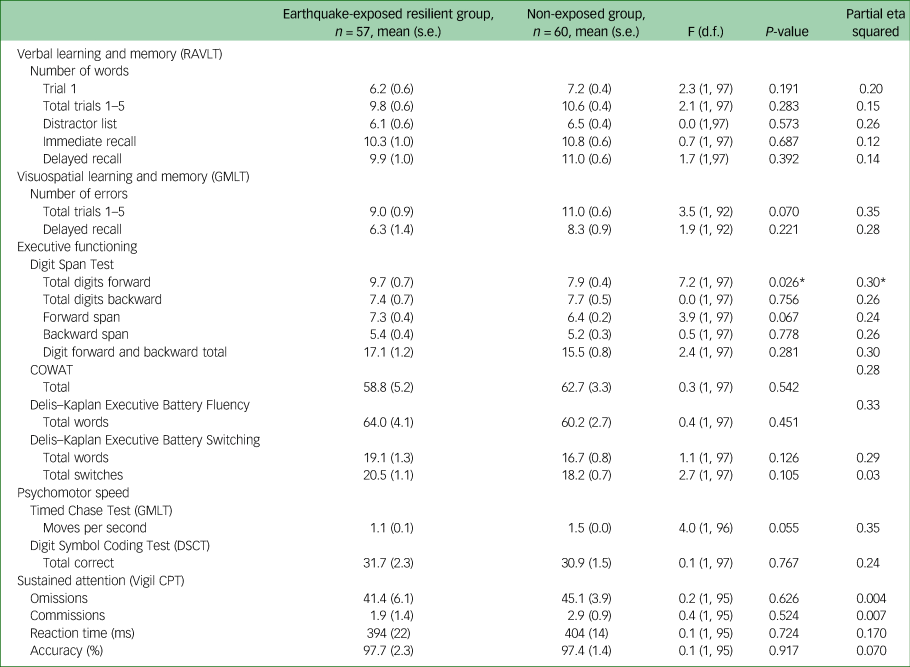
Means are estimated means with age, gender, years of education, ethnicity, CTQ and NART scores as covariates. RAVLT, Rey Auditory Verbal Learning Test; GMLT, Groton Maze Learning Test; COWAT, Controlled Oral Word Association Test; DSCT, Digit Symbol Coding Test; Vigil CPT, Vigil Continuous Performance Test.
*P < 0.05.
On measures of social cognition, no significant between-group differences were found in total RMET score (F(1,94) = 0.7, P = 0.38, partial eta squared 0.23), or any of the FER test variables, including overall reaction time and accuracy, or reaction time or accuracy in identifying specific facial expressions (neutral, angry, happy, sad, fearful and disgusted, all P > 0.05, partial eta squared 0.000–0.039; see Fig. 1). No significant between-group differences were found in tendency to misinterpret neutral expressions as particular emotions (see Fig. 2; all P > 0.1, partial eta squared 0.002–0.018).
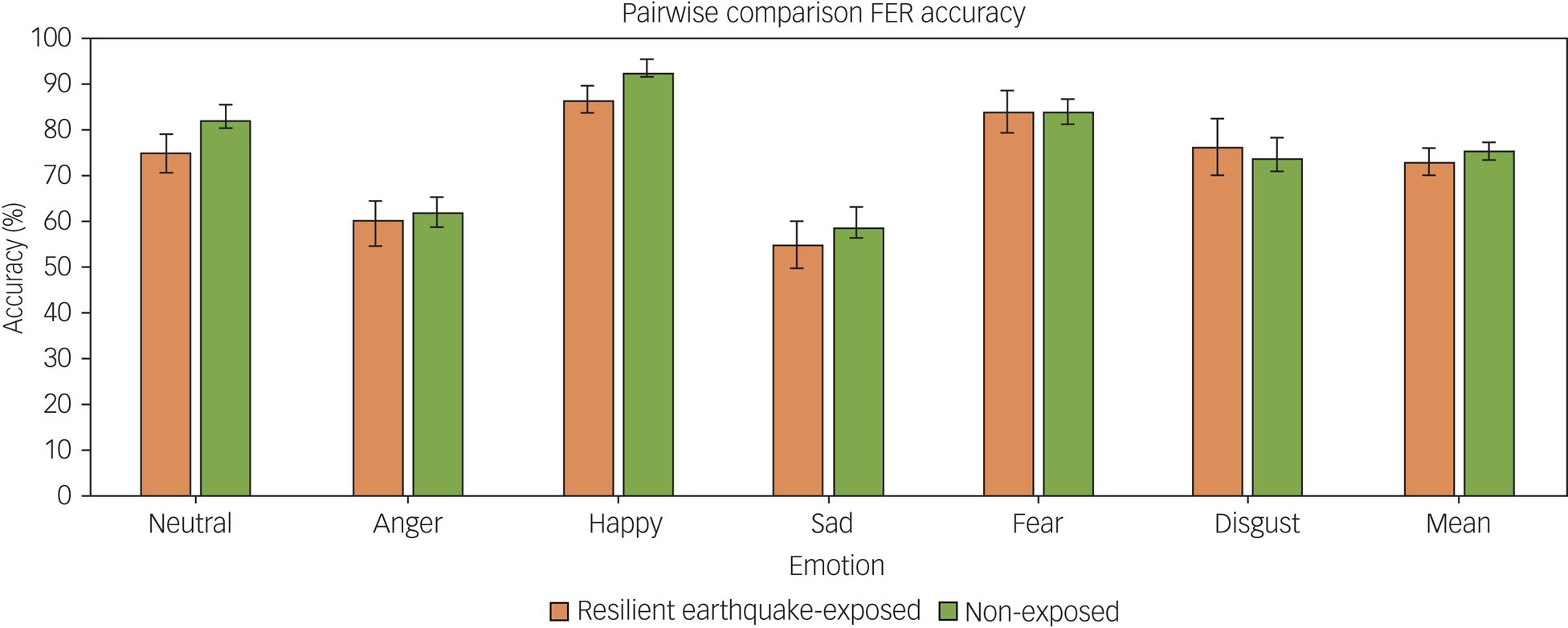
Fig. 1 Recognition accuracy (mean and s.e.m.) for the five facial expressions of emotion and neutral expressions on the Facial Expression Recognition Task (FER), in the earthquake-exposed resilient group (n = 57) and the non-exposed control group (n = 60).
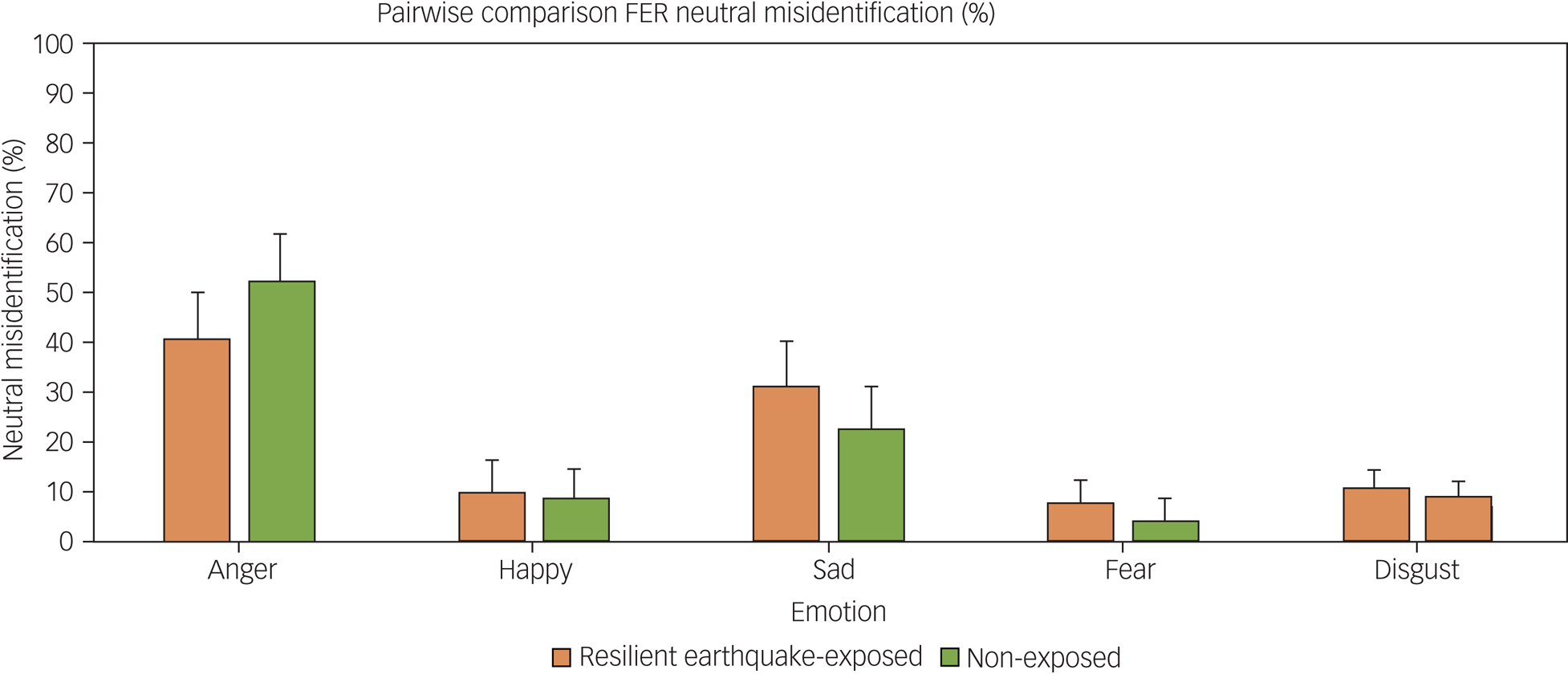
Fig. 2 Misclassification (mean and s.e.m.) of neutral expressions to the five facial expressions of emotions on the Facial Expression Recognition Task (FER), in the earthquake-exposed resilient group (n = 57) and the non-exposed control group (n = 60).
Within-group cognitive comparisons over time
Of the 57 earthquake-exposed resilient participants in the current study, 50 had completed cognitive testing in the original study 2–3 years after the earthquakes (time point 1), which therefore allowed comparison of these participants over time (see Supplementary Figure 1). Of these 50, one completed FER, but not cognitive testing, meaning 50 participants were included in the FER and 49 in the cognitive analysis. A smaller battery of cognitive tests were completed at time point 1 (RAVLT, GMLT, TCT and DSCT), with comparisons limited to these.
As shown in Table 3, in comparing the earthquake-exposed group at time points 1 and 2, poorer performance on the RAVLT (all variables except distractor list recall) and the TCT, and better performance on one GMLT variable (delay trial, total errors), were found at time point 2 compared with time point 1.
Table 3 Means of cognitive test variables in earthquake-exposed resilient group over time
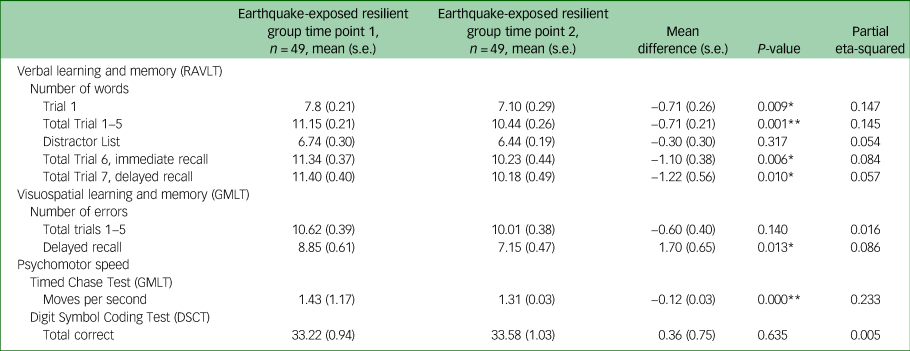
Time point 1: approximately 2–3 years after the beginning of the earthquake sequence; time point 2: approximately 8–9 years after the beginning of the earthquake sequence. RAVLT, Rey Auditory Verbal Learning Test; GMLT, Groton Maze Learning Test; DSCT, Digit Symbol Coding Test.
*P < 0.05, **P < 0.001.
On the FER task, the earthquake-exposed group at time point 2 had slower reaction times for expressions of anger (F(1,42) = 10, P = 0.003), sadness (F(1,42) = 9.3, P = 0.004) and disgust (F(1,42) = 5.4, P = 0.025), compared with time point 1. No differences for the other emotions were found (neutral: F(1,42) = 1.2, P = 0.274; happy: F(1,42) = 1.3, P = 0.267; and fearful: F(1,42) = 3.7, P = 0.061)). The earthquake-exposed group were also more accurate in identifying neutral expressions (neutral: F(1,42) = 6.1, P = 0.018), but not other emotions (angry: F(1,42) = 0.2, P = 0.696; happy: F(1,42) = 1.4, P = 0.246; sad: F(1,42) = 1.4, P = 0.963; fearful: F(1,42) = 0.1, P = 0.760; and disgust: F(1,42) = 0.0, P = 0.969)) at time point 2 compared with time point 1. No differences in performance across time points were found in neutral misinterpretation scores.
Discussion
The aim of the current study was to examine the long-term cognitive effects of exposure to the Canterbury earthquake sequence (8–9 years post-earthquake sequence) in a group of people who had previously identified as resilient, by comparing them with a non-exposed control group. Contrary to our findings at 2–3 years post-earthquake, with the exception of a measure of working memory (Digit Span Forward), no significant differences were found in performance between the earthquake-exposed resilient and non-exposed groups in this longer-term comparison.
These findings may be explained by a combination of factors, including the passage of time since the earthquakes and the context in which the studies were conducted. At the time the original studies were conducted, people were living in an environment of ongoing seismic activity where, over a 2-year period, Canterbury experienced over 10 000 aftershocks. This may have resulted in biological changes, such as in the amygdala, with residents being in a chronically hyper-aroused state. At that time, attentional biases to threat, as shown by the facial expression recognition data,Reference Bell, Colhoun, Frampton, Douglas, McIntosh and Carter18 may have been adaptive, with advantage in attending to potential threat rather than underestimating it. By the time of the current study, there was no seismic activity and the sense of threat had abated. Maintaining a constant state of hypervigilance in this context would provide less advantage and may potentially be maladaptive (i.e. playing a role in promoting or maintaining anxiety). In support of this interpretation, facial emotion recognition studies from Italy post-earthquakes reported similar findings, with evidence of hypervigilance in the context of seismic activity,Reference Pistoia, Conson, Carolei, Dema, Splendiani and Curcio19,Reference Pistoia, Conson, Quarantelli, Panebianco, Carolei and Curcio20 but not in the longer term.Reference Sagliano, Conson, Saporito, Carolei, Sacco and Pistoia36 Similarly, a previous study that reported poorer cognitive performance in women with and without PTSD after exposure to intimate partner violence compared with healthy controls, included participants where exposure was relatively recent (between 4 weeks and 2 years previously).Reference Stein, Kennedy and Twamley12 A study four years after an earthquake in Turkey, found impaired performance on a test of immediate verbal recall in those with PTSD, but not in earthquake-exposed controls.Reference Eren-Koçak, Kiliç, Aydin and Hizli37 Studies examining even longer-term outcomes, including holocaust survivors with and without PTSD compared with non-exposed controls, reported no difference between non-PTSD and non-exposed participants.Reference Golier, Yehuda, De Santi, Segal, Dolan and de Leon38 These findings provide early support for the hypothesis that changes in cognitive and emotion processing in trauma-exposed resilient people may be state-dependent, and related to exposure to continued threat in the environment that reverses when threat resolves.
A further explanation for our findings of no difference in cognitive function 8–9 years after the earthquakes between earthquake-exposed resilient and non-exposed groups may relate to the improved design of the current study, which included a concurrently recruited, non-exposed control group. In our earlier studies, the non-exposed comparison was conducted as a supplementary analysis, and included data from historical control groups recruited for two studies conducted before the start of the earthquake sequence. These were therefore not matched to the earthquake-exposed groups, were younger than the non-exposed control group of the current study, and were different from the current non-exposed group in having no past or family history of mental disorder. These historical studies had also utilised slightly different cognitive test batteries so that differences in the length and timing of the batteries between the exposed groups and controls may have resulted in differences in performance.
Further analysis of a subset of the original earthquake-exposed resilient group allowed examination of changes in cognitive functioning over time, comparing time point 1 (approximately 2–3 years after the start of the earthquake sequence) with time point 2 from the current study (approximately 8–9 years after the earthquakes). In the current study, the group performed less well on tests of verbal memory and learning, and were slower on a test of psychomotor speed. These findings may be explained by a deterioration in functioning as a result of ageing of the cohort, with the studies being conducted 6–7 years apart.Reference Gray, Douglas and Porter39 Performance on one of the tests of spatial learning and memory, however, was better in the current study (at time point 2) than in the original (at time point 1). Interestingly, in the original study, performance on this test had been impaired compared with the non-exposed control sample. Findings from the FER task included slower reaction times for expressions of emotions of anger, sadness, fear and disgust in the current study compared with the original study. In our original study, we had reported faster responses to anger, fear and disgust (but slower response to sadness) in the earthquake-exposed resilient group compared with the historical non-exposed group. It is possible that improvement in visuospatial performance and slowing of reaction times to negative emotions suggests normalisation of these outcomes over time, when the threat has abated.
These conclusions are, however, speculative, being hampered by the study design, which unfortunately did not allow examination of changes over time in the non-exposed group. Comparisons were also only able to be conducted on 55% of the original sample of earthquake-exposed resilient participants. Although there were very few differences between those who did and did not participate at time point 2, it is possible that those in the current study were more resilient. For example, although there were no differences on measures of resilience, anxiety or depression, those who did not take part in the current study had higher rates of alcohol use, poorer visuospatial performance (P = 0.015) and slower reaction times to sad emotions (P = 0.015) at time point 1.
Regarding explicit aspects of psychological functioning, the exposed group reported functioning well, had low scores on measures of depression and anxiety, high ratings of resilience and very low rates of mental disorder. This suggests that those identifying as resilient at time point 1, approximately 2–3 years after the earthquakes, maintained this trajectory despite exposure to a significantly higher number of stressful life events and experiencing greater difficulty from these, compared with the non-exposed controls. It is well-established that exposure to adverse childhood experiences increases risk for worse mental health in adulthood,Reference Hughes, Bellis, Hardcastle, Sethi, Butchart and Mikton40 and it is of note that the earthquake-exposed resilient group had less exposure to childhood trauma than the average population represented by the non-exposed group.
Study findings should be interpreted in the context of the following limitations. Although the groups were well-matched on gender, age and years of education, the earthquake-exposed resilient group scored significantly higher on the NART estimate of premorbid IQ and included a greater proportion of New Zealand European participants. These differences were, however, adjusted for statistically. There was also no measure of affective temperament, which has also been shown to be associated with mental health outcomes.Reference Baldessarini, Innamorati, Erbuto, Serafini, Fiorillo and Amore41 The earthquake-exposed resilient group comprised 57 of the original 101 participants identified in the studies at time point 1, 2–3 years after the earthquakes.Reference Bell, Frampton, Colhoun, Douglas, McIntosh and Carter13,Reference Bell, Colhoun, Frampton, Douglas, McIntosh and Carter18 Although the study design was improved by utilising a concurrently recruited, non-exposed control group rather than historical controls, this did not allow for examination of changes in functioning over the 6–7 years between studies in the non-exposed group, which limits the strength of the findings. Although uniformity of earthquake exposure was a strength, it may limit the generalisability of the findings to those exposed to other trauma types in light of previous reports of more prolonged effects after exposure to interpersonal trauma. Results should also be considered in light of the 2 years of extensive seismic activity. This constitutes a particular type of stress, in which there were ongoing aftershocks with potential for them to become serious and life-threatening. About 50% of the non-exposed group were recruited after the start of the COVID-19 pandemic. Although this could have resulted in additional stressors, there was no difference in psychometric measures (DASS-21 scores) between these participants and those recruited before the pandemic (perhaps reflecting the positive COVID-19 response in New Zealand at the time). Subanalyses of cognitive outcomes were not possible because of the size of the groups. A final issue is that of limited statistical power related to the size of the groups, which may have resulted in type 2 errors.
The study has considerable strengths related to the study design. These include all of the earthquake-exposed participants having been exposed to the same type of trauma at the same time, whereas most other studies have included participants exposed to a wide variety of types of trauma. All exposed participants were resilient and therefore did not have comorbidities such as depression, which complicate interpretation of cognitive findings in many previous studies.
In conclusion, the key finding from the current study was that no differences were found in performance on any of the cognitive tasks in individuals who had been exposed to earthquakes 8–9 years previously but identified as resilient, compared with matched non-exposed controls. There are some limitations in the strength of these findings related to study design and because we were not able to robustly examine changes in cognitive functioning over time. However, if replicated, they suggest that changes in cognitive functioning in trauma-exposed resilient people may be state-dependent and related to exposure to continued threat in the environment, which improves as the threat reduces. The findings increase our understanding of the effects of trauma exposure in resilient populations, and highlight the importance of examining longer-term outcomes.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2022.512
Data availability
The data that support the findings of this study are available from the corresponding author, C.B., upon reasonable request.
Acknowledgements
The authors thank the participants, Emily Douglas for administration of cognitive testing, and Andrea Bartram for data management.
Author contributions
C.B., K.D. and R.P. conceptualised and designed the study. Recruitment to study and acquisition of data was by C.B., K.D., M.P., V.M. and R.S. Analysis of data was conducted by W.M., C.F., C.B and R.P. The paper was drafted by C.B. All authors revised the paper and gave final approval for the version to be published.
Funding
This research was funded through a grant to K.D., from the University of Otago Research Committee (grant number: UORG 3008).
Declaration of interest
The authors, C.B., R.P. and K.D. are on the Editorial Board of BJPsych Open. There are no other potential conflicts of interest with respect to the research, authorship and/or publication of this article.








 Open access
Open access
eLetters
No eLetters have been published for this article.