



Introduction
To promote young people’s health and well-being, international advocacies and discourses have been embraced by governments worldwide, affirming the importance of the social determinants of young people’s well-being (Inchley and Currie, Reference Inchley and Currie2016). Crucially, the resulting new policy paradigm has included a broad move beyond objective measures of young people’s well-being by involving them to explain issues that matter to their well-being in their own voices (Bradshaw et al. Reference Bradshaw, Keung, Rees and Goswami2011); shaping government policies based on social indicators of quality of life (Deeming, Reference Deeming2013); and embracing social determinants of health in international research and policy agendas (WHO, 2008). The emerging studies also revealed crucial variations in how adults and young people characterise well-being and the facets of well-being that are important to young people compared to adults (Statham & Chase, Reference Statham and Chase2010).
According to the WHO Commission on the Social Determinants of Health (WHO-CSDH), social determinants “are the conditions in which people are born, grow, work, live, and age’’, and the factors and systems that shape the conditions of daily life (WHO, 2008:1). This definition emphasises the role of various social contexts, including the family, in shaping young people’s health and well-being outcomes. The family has widely been found to provide the immediate social context for infants and children and suggested to provide the first exposure to various social circumstances that impact young people’s development and well-being (Bronfenbrenner, Reference Bronfenbrenner1979). The available evidence also indicates that low family socioeconomic status (SES) can have medium- and long-term deteriorating effects on children and young people’s well-being (WHO, 2008; Inchley and Currie, Reference Inchley and Currie2016).
More precisely, as a critical social determinant of health, low SES has been shown to incapacitate low-income families from providing young people with the required material and economic needs as well as from establishing required bonding social relationships (Addae, Reference Addae2020a). Low SES can affect young people’s well-being directly and indirectly by rendering parents who live in poverty at a disadvantage for providing the psychological and social needs required for their children’s well-being (Inchley and Currie, Reference Inchley and Currie2016; Ge, Reference Ge2020). It has been argued that family social capital can function as a potential complement in policy agendas targeting the well-being of young people, especially for those from low SES family backgrounds (Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012; Addae, Reference Addae2020a).
Despite growing international interest, there is relatively little comprehensive research on the social determinants of young people’s well-being in low- and middle-income countries (LMICs), including Ghana (Reavley and Sawyer, Reference Reavley and Sawyer2017). Young people are often overlooked as a population group in health statistics, being either grouped with younger children or with young adults (Inchley and Currie, Reference Inchley and Currie2016). Furthermore, young people’s well-being assessments primarily focus on objective measures relating to material and monetary poverty with little consideration for other social indicators. Although the WHO Commission on Social Determinants of Health claims that most health inequalities are preventable (WHO, 2008), young people in Ghana continue to experience health and well-being inequalities due to unfavourable family-related social circumstances (MoGCSP and UNICEF, 2015).
In this article, we examine family-related social determinants of well-being and acknowledge the role of the family in providing critical material and social resources that can function as ‘health assets’ for the well-being promotion of young people. We are especially interested in how family social capital (SC) can potentially act as a non-monetary ‘safety net’ contributing to the current child protection efforts of the Ghanaian government. We seek to provide evidence on the role of family SC in the subjective well-being, particularly life satisfaction and happiness, of young people in Ghana amidst SES’s effects. In the context of widening inequality in Ghana, our findings will prompt the need for revising existing primacies for well-being and social policies by promoting the ‘social fabric’, viz. family SC within collectivist societies, as a complement to the present emphasis on ‘economic empowerment’ within Ghana’s Child and Family Welfare Policy (CFWP) which aims to help young people build resilience against poverty.
To achieve these objectives, we first provide a brief theoretical background on the health assets approach and summarise the critical features of Ghana’s CFWP. We then elaborate on the article’s data and methodology before summarising our main empirical findings. Finally, we discuss the study’s policy implications considering the existing policy structures in Ghana.
Family social capital and young people: ‘the health assets approach’
Despite Coleman (Reference Coleman1988), Bourdieu (Reference Bourdieu1986), and Putnam (Reference Putnam2000) defining SC based on different notions, they acknowledged SC as the “interactions between members which enable the creation and preservation of valuable social resources, and the significance of positive social networks of diverse types and amounts that promote social development and health between diverse groups and societies” (Addae, Reference Addae2020b: pg2). Thus, SC is composed of the individual and collective level and categorised into cognitive (people’s acuity about interpersonal relationships, reciprocity, and enforcement of group values) and structural (number of social networks and structures of civic engagement) SC (Harpham, Reference Harpham2008). Based on the type of existing social ties, three conceptual distinctions are further classified: namely, bonding (strong ties linking family members, friends, and colleagues), bridging (the connection between individuals/groups of different structural powers), and linking (connects individuals and families to institutions to empower them to access resources) (Kim et al., Reference Kim, Subramanian and Kawachi2008).
SC can be constructed in various social contexts, including families, schools and other educational institutions, civic institutions, and local neighbourhoods. The family provides the first context of socialisation for the construction of SC for young people, and family SC has been recognised as a primary health asset in the public health literature (Morgan, Reference Morgan2010; Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012). A health asset is understood as any feature that augments the capability of individuals, societies, and populaces to preserve and support health and well-being (Morgan and Haglund, Reference Morgan and Haglund2009) and can be attained by young people from members within their social environments. This notion portrays young people as social agents who can shape their own social lives and that of others in their societies by maximising assets and minimising risks (the negative aspect of social capital) to promote well-being outcomes. The health assets approach further seeks to understand the variations in the significance of various assets, the benefit of accumulating them, and their stability across diverse social and cultural contexts (Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012).
The existing literature shows that providing opportunities for young people to access and accumulate protective health assets provides a high possibility for them to build resilience against various environmental stressors, including low SES to achieve positive health and well-being outcomes, positing SC as a protective resource amidst the direct adverse effects of low incomes and poverty (Addae, Reference Addae2020a; Morgan, Reference Morgan2010). Employing the health assets approach to inform policymaking means that young people should be provided with SC at an early age to enable them to accumulate resources needed to build their capacity to access and engage in various social networks that promote their resilience as they transition into adolescence and adulthood (Morgan, Reference Morgan2010). The health assets approach seeks active youth involvement by fostering a sense of belonging and autonomy and control over decisions that affect young people’s lives, ultimately empowering them with belief and disposition to engage in various social networks. This may eventually enhance their active community engagement, satisfying the collective perspective of SC (Putnam, Reference Putnam1995; Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012).
The health assets approach further emphasises the need to consider the context (age, gender, ethnicity, religion, culture, environment-family, school, community, etc.) in translating SC as health assets in research regarding the health and well-being of young people (Addae, Reference Addae2020b). This is because distinct associations between health, well-being, and different contexts within which social networks are formed and function have been widely established (Morgan and Haglund, Reference Morgan and Haglund2009). For instance, the home context has been found to have the strongest association with young peoples’ subjective well-being compared to the same indicators at other contexts such as the school and neighbourhood (Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012). This postulates the critical role of the family in constructing bonding SC for young people’s well-being. In view of progressing young people’s well-being, family SC should be promoted in social policies to accumulate SC at the early stage of life to optimise its benefits derived from the family contexts (Morgan, Reference Morgan2010; Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012). We, therefore, hypothesise SES and SC will independently predict well-being and that family SC will moderate the relationship between SES and well-being.
The present child and family welfare policy in Ghana
Ghana’s Child and Family Welfare Policy (CFWP) was introduced in 2014 by the Government of Ghana and the Ministry of Gender, Children and Social Protection (MoGCSP) (MoGCSP, 2014) with support from UNICEF and other local and international organisations and civil society groups (MoGCSP and UNICEF, 2015). The CFWP was devised as a component of Ghana’s Child Protection System (CPS), which as part of the Ghanaian child and family welfare system involves “laws and policies, programmes, services, practices and structures designed to promote the well-being of children by ensuring safety and protection from harm; achieving permanency and strengthening families to care for their children successfully’’ (MoGCSP, 2014:IV). CFWP recognises that a fundamental part of the family is the child and that the child’s welfare cannot be estranged from that of the family (MoGCSP and UNICEF, 2015); as such, CFWP targets the ‘formal’ component of Child and Family Welfare Services (governed by laws, policies and regulations and delivered by state institutions) and the ‘informal’ (based on community and traditional processes and resources)” (MoGCSP and UNICEF, 2015:1).
In line with the Convention on the Rights of the Child, Ghana’s 1992 constitution, and the 1988 Children’s Act, the CFWP was developed based on several fundamental guiding principles such as family and community cohesion and harmony, sense of belonging to family and community, the child’s right to survival and development, and acknowledging children’s perspectives in decisions concerning them. Accordingly, CFWP’s emphasis is on promoting the well-being of the child, the family, and the community. Therefore, CFWP reinforces a child protection system that protects and answers to children and their families when necessary and offers support to alleviate risks for vulnerable families (MoGCSP, 2014; MoGCSP and UNICEF, 2015).
Several studies revealed that despite Ghana being a collectivist society where the extended family contributes to the care and protection of children, the informal foster care provided by both the extended family and the traditional Ghanaian kinship network that has traditionally acted like a complete social ‘safety net’ for children from low-income families has weakened due to factors such as poverty and family breakdown discouraging lineage groups from caring for children (MoGCSP and UNICEF, 2015). Therefore, the CFWP aimed to create a valuable child and family welfare dimension of the CPS with three priority areas including “child protection issues stemming out of family-related challenges, including parental responsibility, domestic violence, and children deprived of adequate family care”, “child maltreatment including all forms of violence, abuse, exploitation and, neglect”, and “other protection issues […] resulting from individual risk-taking behaviour” (MoGCSP and UNICEF, 2015:9). Six policy objectives were developed to meet these critical priorities via eleven detailed policy strategies, three of which are pertinent to the discussions of this article.
First, in recognising the connection between social protection and reduced child protection outcomes and safeguarding children by reducing poverty among the extreme poor in Ghana, “Early Intervention Through Social Protection” was highlighted as part of the CFWP (Strategy 2). To promote social protection, the Department of Social Welfare sought to enhance ‘economic empowerment’ through several policy initiatives explicitly formulated to target the monetary challenges experienced by children and families (MoGCSP and UNICEF, 2015). Such initiatives included the National Health Insurance Scheme, free maternal care, the capitation grant for public schools, free school uniforms, the school-feeding programme, and the Livelihood Empowerment Against Poverty (LEAP) programme offering cash transfers to the poor (Ministry of Employment and Social Welfare, 2012; MoGCSP and UNICEF, 2015).
Second, CWFP acknowledged the need to ‘Empower Children and Young People’ (Strategy 6) in tackling child protection issues and, in so doing, recommends children’s participation in decision-making processes at the family and community levels. The recognition of children and young people as “agents of change” includes involving children’s voices in researching child protection issues. Compared to Strategy 2 on “Early Intervention Through Social Protection”, the CWFP contains less concrete policy detail on how Strategy 6 on “Empowering Children and Young People” may be achieved.
Third, as rising economic difficulties enfeebled the ‘safety nets’ offered by the extended family and kinship networks, to “establish an effective Child and Family Welfare component of the overall child protection system’’ (UNICEF and Ministry of Employment and Social Welfare, 2009; MoGCSP and UNICEF, 2015:3) is to “Empower Families Through Social Dialogue and Change” (Strategy 7) (MoGCSP and UNICEF, 2015:4). While this strategy re-affirms families’ “primary responsibility for the welfare of their children and for the provision of basic needs […] and support for the child’s socialisation and identity development”, the means of achieving this strategy mainly aimed to sensitise parents at community forums and through the sharing of relevant information about parenting and understanding of children’s physical and social development (MoGCSP and UNICEF, 2015:9). Similar to Strategy 6, the policy detail on “Empowering Families Through Social Dialogue and Change” (Strategy 7) remained relatively scarce.
Methods
Data
This article uses data from a school-based cross-sectional study carried out in 2018, which aimed to examine the role of SES and SC in the well-being of Ghanaian young people, defined as people from 10-24 years of age (WHO, 2020), and focussed its setting in the poorest region in Ghana. A total of 2,068 adolescent participants (13-18 years) were randomly selected using a multi-stage stratified sampling approach from seven districts in Ghana’s Upper West Region. Using the Ghana poverty mapping, the region was stratified into three sub-regional zones (low, medium, and high poverty zones) based on the regional poverty incidence index. To create the primary sampling units, two districts were selected from each of the low and high poverty incidence zones; and three districts were selected from the medium poverty zone because it had the largest number of districts. In all, seven districts representing the primary sampling units were employed.
This study included only male- and female-mixed public schools to ensure sample homogeneity. This is because almost all the Senior High Schools (SHS) at the time of the survey were mixed public schools. For the basic school level, Junior High Schools (JHS) were included. One JHS and one SHS were selected from each district to represent the sample units. However, for one district, two SHS were selected because most of the students in the schools exceeded the age requirement, which would have limited the sample size if only one SHS for that district was used. A total of fifteen schools comprising eight SHS and seven JHS were employed. Some classes were randomly selected in each school, and eligible students within these classes were stratified based on the class sizes and randomised proportionally. Students outside the age range (13-18 years), whose parents/guardians did not give consent, and those unwilling to participate in the study were excluded from the survey.
After a pilot study, self-administered questionnaires were distributed to eligible respondents on voluntary and anonymous bases for the data collection. The questionnaire was designed in English, the language of instruction in schools in the study area. The trained research assistant provided the interpretation of items in the region’s main dialect on an individual basis. The questionnaire administration took an average of 45 minutes in each school. Focus group discussions were completed after the questionnaires to confirm the participants’ comprehension of the survey items. Participants were compensated with pencils for their time. All ethical protocols were observed. The Committee on Human Research Publication and Ethics (CHRPE), School of Medical Sciences, Kwame Nkrumah University of Science and Technology and Komfo Anokye Teaching Hospital, Kumasi, Ghana (Ref: CHRPE/AP/542/18) provided the ethical approval for this study.
Measures
Measures of subjective assessment of one’s well-being (SWB) have been enhanced in recent years in recognition of their potential to enable monitoring of social development policy (Taylor, Reference Taylor2011) as they offer a valuable proxy and a clear yardstick for policy practitioners concerned with young peoples’ health and well-being promotion (Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012). This study focuses on two dimensions of SWB based on two theoretical components: (1) the ‘evaluative approach’ to SWB, which requires individuals to assess their overall life cognitively or on specific aspects of their life known as life satisfaction, and (2) the ‘hedonic approach’ which assesses people’s feelings and emotions, happiness which is usually employed in global cognitive assessment of well-being (Dolan and Metcalfe, Reference Dolan and Metcalfe2012; Deeming, Reference Deeming2013).
Life satisfaction (LS) was assessed using the Cantril ladder scale (Cantril, Reference Cantril1965) noted to evaluate the cognitive aspect of well-being effectively. The study participants were requested to select a step out of the 11 steps presented on an image of a ladder to represent their LS (10 - highest satisfaction and 0 - lowest satisfaction).
Happiness was evaluated using the 2010-2012WorldValue Survey’s happiness scale (Inglehart et al., Reference Inglehart, Haerpfer, Moreno, Welzel, Kizilova, Diez-Medrano, Lagos, Norris, Ponarin and Puranen2014), asking participants ‘Taking all things together, would you say you are….?’ Coded responses were 4 = ‘very happy’, 3 = ‘rather happy’, 2 = ‘not very happy’, 1 = ‘not happy at all’; all ‘don’t know’ responses were not scored. Three sub-domains of family SC, including a sense of belonging (identity and safety with their social environment), autonomy and control (perceived power to influence decisions), and social support (Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012), were employed to represent young people’s family SC. These sub-domains of SC have been thoroughly assessed among the social indicators of ‘health assets’ for promoting young people’s well-being (Morgan, Reference Morgan2010; Morgan et al., Reference Morgan, Rivera, Moreno and Haglund2012).
Family sense of belonging (FSB) was assessed using four items, including ‘how much do you feel your family understands you?’; ‘how much do you feel you and your family have fun together?’; ‘to what extent do you feel your family pays attention to you? ’and ‘how much do you feel safe at home?’ Options: 1 = very little, 2 = somewhat, 3 = neutral, 4 = quite a bit, 5 = very much (Addae, Reference Addae2020a). The FSB scale was computed by adding the scores of the four items (4-20). The reliability of the scale was α = .74.
Perceived social support from family (PSS-Fa) was measured using fifteen items adopted from the PSS-Fa scale developed by Procidano and Heller (Reference Procidano and Heller1983). This 15-item scale consists of declarative statements about socioemotional support to which the individual answered ‘1 = Yes’, ‘0 = No’, or ‘Don’t know’. The scale ranged from 0-15 with reliability of α = .770.Footnote 1
Family autonomy and control were measured separately as family autonomy support (FAS) and family control (FC) as they represent different constructs (Addae, Reference Addae2020a). FAS and FC were assessed using parental autonomy (18 items) and control scales (9 items) adopted from Marbelle (2014). The scores ranged from 18-72 (FAS) and 9-36 (FC), and the reliability of the scales was α = .87 and α = .73, respectively. Similar to the two dependent variables, all ‘don’t know’ answers for the four family SC measures, FSB, PSS-Fa, FAS, and FC, were not scored.
Family SES was assessed based on the respondents’ material affluence using the Doku et al. (Reference Doku, Koivusilta and Rimpelä2010) material affluence scale created especially for Ghana. Material affluence (MA) was measured by developing a composite score from eight items of two broad types: household assets (television, fridge, computer, radio, electricity, family car, and own room) and housing characteristics (blockhouse and non-block house). Responses to having these items in their homes were scored as ‘Yes = 1’ and ‘No = 0’, and a composite score (0-8) was created. The reliability of the scale was α = .703.
Finally, several variables accounting for the socio-demographic characteristics of adolescents were employed as covariates, including gender, ethnic group, marital status, religious affiliation, self-rated health alongside other school- and family-related characteristics. The average age for the final sample was 16.25(±1.492). All other characteristics of the original study sample are summarised in Table 1, together with the measurements of these controls.
TABLE 1. Baseline characteristics of the study sample
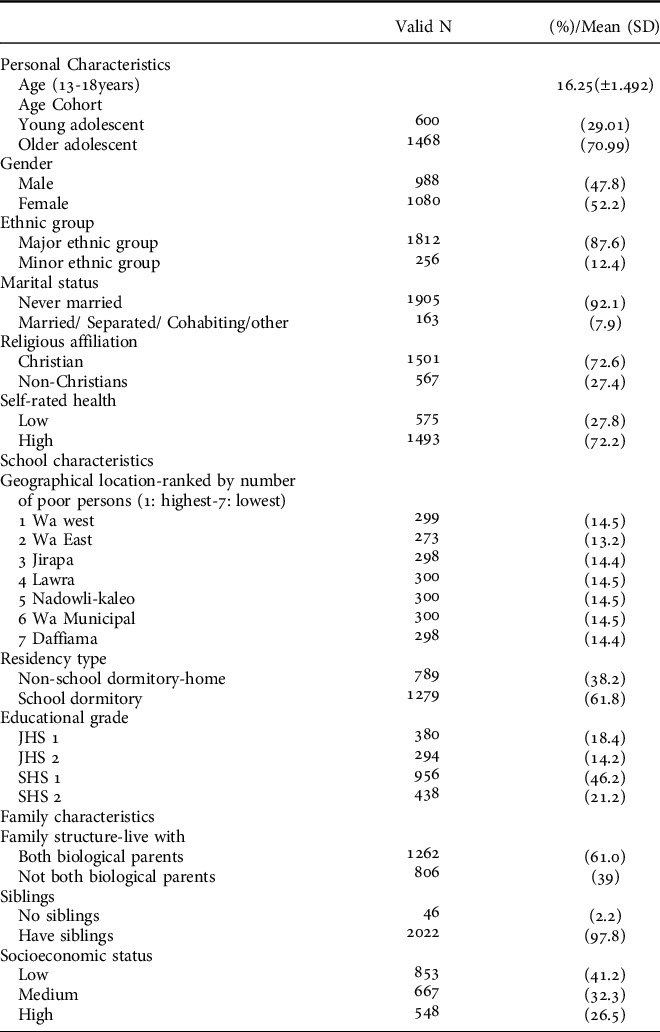
N = Sample size, % = sample percentage, SD = Standard deviation
Analytical approach
We employed descriptive statistics, which showed that a majority of the participants reported a low level of life satisfaction (LS, 55%) and happiness (59%) (Table 1). We also examined the frequency distribution of LS and happiness scores across the different social capital and socioeconomic status categories using bivariate cross-tabulation Chi-square analysis (Table 2). Using the quartile values obtained from the four composite SC variables and SES, we found statistically significant associations between SES, family sense of belonging (FSB), autonomy support (FAS), family control (FC) and perceived social support from family (PSS-Fa) and LS and happiness (Table 2).
TABLE 2. Variations in adolescents’ life satisfaction and happiness by social capital and socioeconomic status - Chi-square analysis
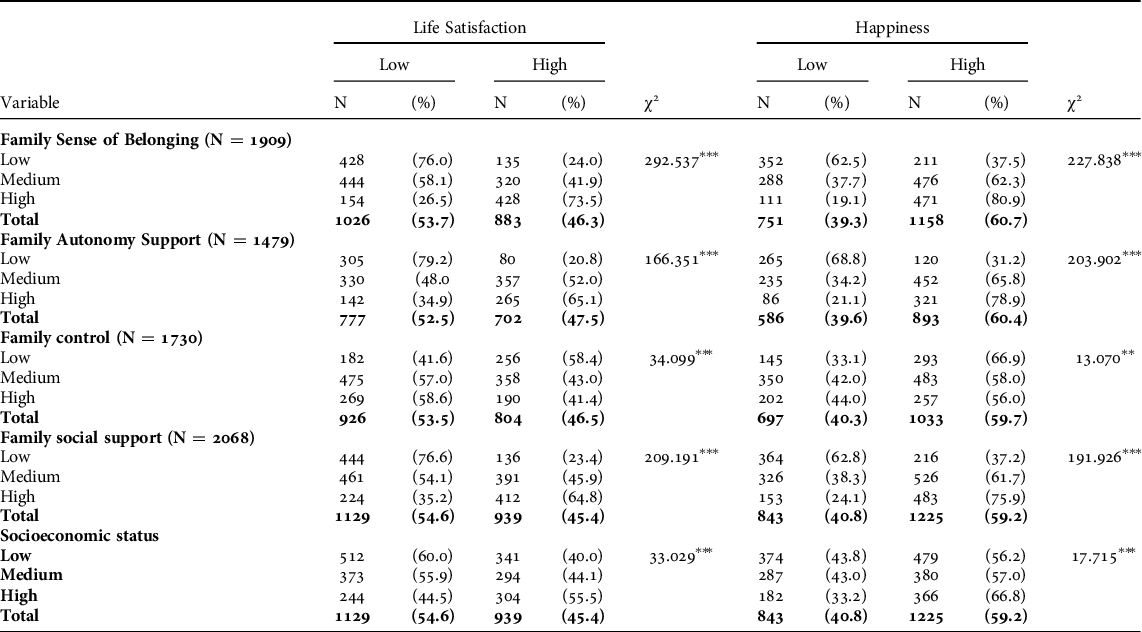
***p < 0.001; **p < 0.005. N = sample size
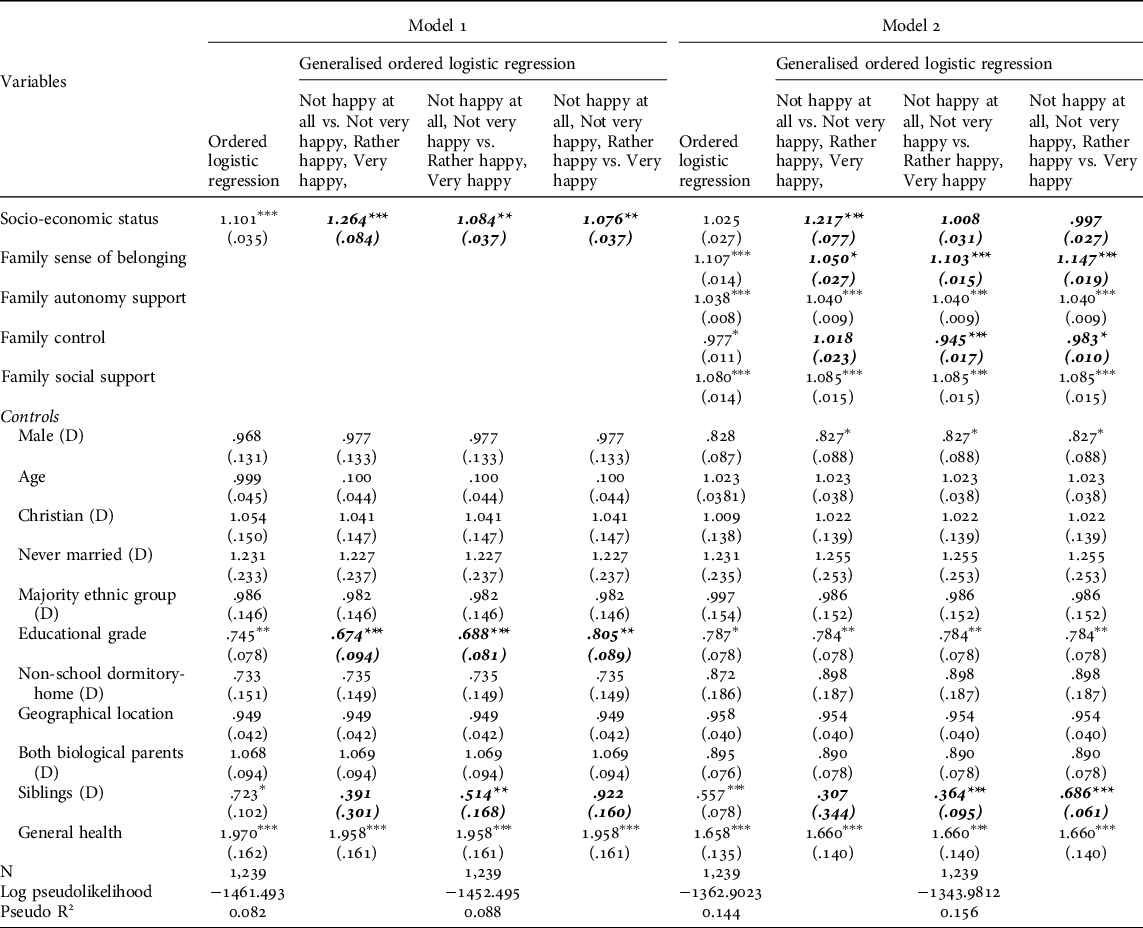
To examine the multivariate relationships between LS and happiness and the adolescents’ family SES and SC, we employed ordered logistic regression (OLM) and generalised ordered logit models (GOLM) since initial likelihood ratio test statistics suggested that OLM on LS and happiness violated the parallel lines assumption. GOLM estimates adolescents’ odds of being beyond a certain category of the dependent variable relative to being at or below that category. Unlike OLM, the outcome of GOLM is a partial proportional model, which enables researchers to empirically ascertain a model specification in which some parameter estimates differ across different categories of the dependent variable while others remain constant (Williams, Reference Williams2016). All OLM and GOLM analyses were conducted separately, involving LS and happiness as the dependent variables, respectively. First, the specified OLM and GOLM models contained only SES and all control variables to test the independent effect of SES on adolescents’ subjective well-being (Model 1). This was followed by model specifications which contained the family SC measures, SES and all control variables to test the moderation effect of family SC in the relationship between SES and adolescents’ subjective well-being (Model 2). We mainly report OLM because this is still the more common technique in the literature, but we will focus our interpretation of findings on the GOLM wherever the two deviate. Wald tests for all reported GOLM models produced an insignificant test statistic indicating that the parallel lines assumption violation no longer posed a problem.
The sample size was kept constant (n = 1,239) by removing all adolescents with missing data for any of the included independent variables and controls to enable a robust comparison of the net contributions of family SC and SES to LS and happiness. We estimated cluster robust standard errors within groups of adolescents attending the same schools, and the significance level was p < 0.05 (two-tailed). Pearson correlations between all independent variables (FSB, FAS, FC, PSS-Fa, and SES) were found to be generally below 0.5, which suggests that multicollinearity did not pose an issue for our multivariate analyses. To facilitate the GOLM analysis, the original Cantril self-anchoring striving scale was merged into a new four-category variable following a common distinction (see, e.g. Gallup World Poll) labelling adolescents as either “suffering” (original scores 0-4), “struggling”, or “neither suffering nor thriving” (5-6), “doing well” (7-8), and “thriving” (9-10).Footnote 2 The original happiness scores for all adolescents were used for estimating all GOLM models. Finally, we utilised Stata 15.1 for MAC software (Version 10.15.7) for all OLM and GOLM analyses using the “ologit” and “gologit2” ado-commands, respectively. For the latter, we relied on the ‘autofit’ option to fit partial proportional odds models (Williams, Reference Williams2006).
Results
Life satisfaction (LS)
Model 1 in Table 3 shows that the effect of SES on LS was positive and statistically significant in both the OLM and GOLM specifications after controlling for all adolescents’ sociodemographic characteristics. However, the effect of higher SES diminished across categories of LS in the GOLM. This means that adolescents with higher SES were more satisfied with their lives, ceteris paribus, with the greatest difference being that those with higher SES were less likely to put themselves in the “suffering” category. After adjusting for family SC in Model 2, the effect of SES on adolescents’ odds to attain higher LS was still predicted to be positive and statistically significant in both the OLM and GOLM. SES no longer violated the parallel lines assumption, and coefficients of SES did not vary across categories of LS (OR = 1.077, p < .001).
TABLE 3. Logistic regression estimations of adolescents’ life satisfaction by social capital and socioeconomic status

***p < 0.001; **p ≤ 0.005, *p < 0.05. Independent variables and covariates violating parallel lines assumption in Italics . Clustered standard errors in parenthesis. D = Dummy variable.
After adjusting for SES and other socio-demographic factors, most SC variables (FSB, FAS, FC) did not meet the parallel lines assumption of OLM. As such, the GOLM suggests that the effect of higher FSB on adolescents’ LS was consistently positive and statistically significant across the categories of LS, but higher FSB particularly helped “suffering” and “struggling” adolescents to escape low LS (OR = 1.139. p < .001). The effect of higher FAS was consistently positive but diminished across categories of LS, suggesting that adolescents with higher FAS were more satisfied with their lives, ceteris paribus, with the greatest difference being that those with higher FAS were less likely to put themselves in the “suffering” category (OR = 1.049, p < .001). By contrast, the effect of higher FC on LS was consistently negative, but the respective odds ratios increased across categories of LS. This finding suggests that everything else being equal, those adolescents with higher FC were more likely to put themselves in the “suffering” category (OR = .901, p < .001). Finally, PSS-Fa was the family SC variable that did not violate the parallel lines assumption. Adolescents reporting higher PSS-Fa generally tended to be more satisfied with their lives (OR = 1.084, p < .001).
Among the included covariates, it was only health status and poverty incidence that were related to LS. Adolescents reporting a higher degree of general health tended to be more satisfied with their lives, while those living in geographical locations with lower poverty rates tended to be less likely to attain high LS. Model 2, including all SC indicators, resulted in a model that overall predicted LS more accurately (Pseudo R 2 = 0.142) than Model 1, which exclusively considered SES and the sociodemographic controls.
Happiness
Models 1 and 2 in Table 4 show that our findings predicting adolescents’ happiness are similar to those predicting LS. In Model 1, the effect of SES on happiness was again positive and statistically significant after controlling for all adolescents’ sociodemographic characteristics in both the OLM and GOLM specifications; the effect of SES diminished across categories of happiness in the GOLM, suggesting again that adolescents with higher SES were happier with their lives, ceteris paribus, with the greatest difference being that those with higher SES were less likely to put themselves in the “not happy at all” category. After including family SC indicators in Model 2, our findings indicate that higher SES helped those adolescents who reported to be “not happy at all” to escape low happiness (OR = 1.217, p < .001). Unlike the OLM, which showed a statistically insignificant effect of SES on happiness, our GOLM suggests that higher SES played a statistically significant role for those adolescents at the bottom of the ‘happiness’ distribution. In contrast, the effect of higher SES on happiness was moderated and or mediated by family SC across all other categories of happiness.
TABLE 4. Logistic regression estimations of adolescents’ happiness by social capital and socioeconomic status
***p < 0.001; **p ≤ 0.005, *p < 0.05. Independent variables and covariates violating parallel lines assumption in Italics . Clustered standard errors in parenthesis. D = Dummy variable.
In addition to SES, it was the effects of FSB and FC that violated the parallel lines assumption of OLM, and parameter estimates consequently differed across categories of the happiness scale in the GOLM. The effect of higher FSB on adolescents’ happiness was consistently positive and statistically significant. Yet, the odds-ratios increased, suggesting that adolescents with higher FSB tended to be happier. The greatest difference was that adolescents with higher FSB were more likely to place themselves in the “very happy” category. Although not statistically significant, GOLM also suggested that higher FC was related with higher odds to escape low happiness among the least happy adolescents (“not happy at all”), but the effect turned negative and statistically significant for all other happiness categories. In other words, the evidence broadly confirms the findings of the OLM that higher FC is related to lower odds of adolescents attaining happiness. GOLM also confirmed the results of OLM that adolescents reporting higher FAS (OR = 1.040, p < 0.001) and PSS-Fa (OR = 1.085, p < 0.001) tended to be happier, everything else being equal.
Males, adolescents attending higher educational grades, and adolescents with siblings tended to be less “happy”, ceteris paribus, while adolescents reporting a higher degree of general health tended to be happier. Thus, for happiness, the inclusion of SC indicators in Model 2 resulted in a better model fit (Pseudo R 2 = 0.156) than Model 1, which exclusively considered SES and the sociodemographic controls.
Discussion
The notion that the measurement of SWB is key to the development of social policy has been more readily acknowledged. Indicators that encapsulate people’s overall mental health and cognitive evaluations of how they perceive their own life have been found to expound a vital aspect of the well-being concept, which can be applied to social policies when amassed at the aggregate population level (Deeming, Reference Deeming2013). Although the survey data used in this article is not at the national level, the representative sample used to represent the Upper West Region in Ghana can provide adequate evidence for social policy development in Ghana as all regions share similar socio-cultural norms relating to the family and its role in the provision of child protection and welfare. In this final section, we reflect on how our empirical insights may be utilised to reinforce and develop the present CFWP in Ghana.
Socioeconomic status (SES) and subjective well-being (SWB)
The role of material and economic factors in young people’s current and future capacity building is not in doubt. Moreover, the impact of family SES on adolescents’ well-being can be long-term as it affects young people’s current and future physical and cognitive development and overall development as they transit through the stage of growth and formation (Inchley and Currie, Reference Inchley and Currie2016). Therefore, family SES is crucial in the welfare promotion of adolescents and has rightly been identified as such in Ghana’s CFWP.
From the perspective of SWB, the “Early Intervention Strategy Through Social Protection” (Strategy 2) of the CFWP is commendable in several ways; there are obvious benefits and gains if more vulnerable families can reduce their economic burdens and support their children’s financial needs. This study found that adolescents with lower family SES stand a greater chance of achieving lower LS than those with high SES after controlling for family SC. Yet, higher family SES was not generally related to higher happiness in the presence of family SC (FSB, PSS-Fa, FAS, and FC). More precisely, our GOLM suggested that SES only plays a statistically significant role for adolescents at the bottom of the happiness scale but not for any others. This finding corroborates other studies that found that family SES is more related to LS than other measures of well-being that involve feelings or emotions, such as happiness (Diener et al., Reference Diener, Ng, Harter and Arora2010).
Rather than family SES, adolescents’ happiness appeared to be more related to feelings or emotional satisfaction derived from family SC (FSB, FAS, FC, and PSS-Fa). This finding affirms that SWB is not only dependent on material and economic measures (i.e. ‘economic empowerment’) but also rests on psychosocial measures such as family SC, which can strengthen adolescents’ resilience to shocks that arise from various environmental stresses, including poverty or low family SES (Bourdieu, Reference Bourdieu1986). More importantly, we found that family SC moderated the effect of SES on both LS and happiness. These findings reveal the protective role of family SC in the relationship between family SES and the SWB of young people in the Ghanaian context. This infers that policymakers ought to consider the family as a critical socio-economic risk absorber in Ghana. Consequently, CFWP would be well advised to address complexities regarding the effect of family SES and family SC on young people’s well-being more directly and explicitly, as is currently the case.
For instance, economic and active employment policies may improve families’ ability to meet the costs of providing basic needs and have significant positive effects on young people’s welfare. The consequences of these policies on the family role as a moderator/mediator of adolescent SWB, however, can be unpredictable as there are variations and uncertainties in the consequences of how successful inclusion of Ghanaian families in the labour market, especially in precarious employment with long working hours and unfavourable working conditions, may affect their ability to socialise with their children. This potential gap in the cost-benefit assessment of such policies, hence, fails to acknowledge that adolescence is a period of biological and social growth that requires adolescents to be both economically and socially capable and that developmental losses in adolescence cannot be regained. Thus, policies that trade short-term economic benefits for short- and long-term social costs are not sufficient to assess the genuine inter-generational consequences of Ghana’s current policy mix (Harper and Marcus, Reference Harper and Marcus1999).
Therefore, family and child welfare policies that seek to alter parents’ activities with their children within or outside the home can be introduced through policies targeting child support and positive parent-child relationships. In developing the CFWP for the future, policymakers in Ghana should focus their attention on social investment policies that facilitate increased employment rates together with social benefits for the poor and that, therefore, do not destabilise the social capacity of families to provide the adolescent child with the required non-monetary health assets (FSB, FAS, PSS-Fa) needed to boost their well-being.
Family social capital and subjective well-being
Similar to the CFWP, several studies have acknowledged that children are social agents in their own right that are capable of making decisions, holding social and economic power, and actively shaping society (Morgan, Reference Morgan2010; MoGCSP and UNICEF, 2015). Nevertheless, children, especially in LMICs, are still too often recognised as ‘incapable socialised future beings’, and this perception has been argued to drive specific socioeconomic, cultural, and political strategies for children and adolescents, cementing their dependent status within the policy arena (Clark & Eisenhuth, Reference Clark and Eisenhuth2009). As a result, adolescents are subsumed in and controlled by their families and state institutions, including schools. This situation is at odds with the CWFP’s acknowledgement of the need to ‘Empower Children and Young People’ (Strategy 6).
Recognising adolescents as social agents means acknowledging adolescents as builders and beneficiaries of SC. But equally, CWFP in Ghana has a vital role in the empowerment of families to build SC for their children, especially at the early stage of their lives. This study found that some adolescents are socially deprived due to the inability of their families to provide them with the required SC in the home context. Such adolescents are identified by having low levels of FSB, FAS, PSS-Fa and high FC, which harms their ‘social empowerment’ and poses a risk of social exclusion.
Ghana is a highly embedded collectivist society providing a ‘social fabric’ where extended family members share mutually valuable relationships through collaborative childcare and socioemotional support (MoGCSP and UNICEF, 2015). The traditional extended family system holds an in-built safety net for children from low-income families, and customarily the Ghanaian kinship network functions as an informal social welfare system. While traditionally, there should be guaranteed distribution of resources across the various levels of the family for promoting everyone’s well-being and strengthening kinship bonds (MoGCSP and UNICEF, 2015), our findings corroborated that the family context is failing some adolescents in Ghana by depriving them of the needed social resources expected from socialisation at the family level. In contrast to the guiding principles of the CWFP, we found that several Ghanaian adolescents lack a sense of belonging to the family and the right to participation.
Parenting at the early stage of life is very important for the building of family SC for adolescent’s well-being promotion. Our findings suggested that adolescents with low FSB and PSS-Fa were less likely to attain high LS and happiness, respectively. Furthermore, research indicates that collectivist societies mostly use implicit social support approaches to obtain emotional comfort from social networks (Kim et al., Reference Kim, Subramanian and Kawachi2008). High FSB and PSS-Fa can hence potentially help adolescents build resilience against the effects of low SES, prevent social isolation and exclusion at the family level, and enhance the ability of adolescents to accrue appropriate material and emotional resources for their well-being.
Moreover, we found that FAS and FC are instrumental for the well-being of Ghanaian adolescents (Marbelle & Glorlick, Reference Marbelle and Glorlick2013). The CFWP expressly acknowledges “Empowering Children and Young People” (Strategy 6) in tackling child protection issues and recommends children’s participation in decision making processes at the family level. However, we found that adolescents in Ghana still lack the empowerment to participate in the decision-making process at the family level, posing a direct threat to their SWB. After controlling for all other variables, including SES, adolescents with lower FAS were less likely to achieve higher LS and happiness. Those with higher FC also showed higher odds of attaining low well-being (Suldo & Huebner, Reference Suldo and Huebner2004). Furthermore, higher levels of parental control have been associated with more anxiety due to decreased self-efficacy in adolescents (Wood et al., Reference Wood, McLeod, Sigman, Hwang and Chu2003), consequently resulting in negative impacts on adolescents’ socioemotional achievement.
Collectively, this article has shown that the vulnerable status of adolescents in Ghana within families and the unavoidable affairs of control, authority, and dependence requires acknowledgement and solution as they obstruct adolescents’ capability to accrue social and health assets from their families and consequently dictate the direction of adolescents’ well-being. In the light of these solid empirical findings, and in referring to Strategy 7 of the CWFP to “Empower Families Through Social Dialogue and Change”, the current focus on information sharing and community discussions and forums with parents presents a practical first step, but may ultimately not go far enough if children and adolescents are not included in the information sharing/dialogue as they form an integral part of the family and hold vital perspectives about their well-being.
Conclusions
According to Dean (Reference Dean2012), it is a fundamental responsibility of mainstream social policy analysis to ensure research into the subjective dimension of human development. Here, we used a representative sample of Ghanaian adolescents to provide evidence on the significance of family SC and SES for their SWB to suggest reinforcement and development of the present CWFP. To our knowledge, this is the first study in Ghana to do so. While our findings are robust, the use of cross-sectional data did not allow for causal relationships to be established. Also, the study focused only on one region, the poorest region in Ghana, inferring a lack of national-level representation of the findings. Future studies should consider the use of nationwide and longitudinal survey data, resources permitting.
The findings from this study support the claim that economic measures and GDP are on their own not adequate to measure the well-being of different societal groups, including young people (Deeming, Reference Deeming2013). Furthermore, we showed that the SWB of adolescents in Ghana is not solely dependent on their family SES but also on family SC. Indeed, our findings suggest that family SC is an essential building block for the healthy development of adolescent well-being. It is, therefore, necessary for policymakers to fully recognise and promote the family as a potential enabler and capability builder for young people’s empowerment – particularly as they continue to be tasked with the primary responsibility of influencing the social determinants of adolescent well-being in the collectivist Ghanaian context.
Recognising adolescents’ social capital in future policy development means recognising the level of their social, economic, and political contributions to society. Together with designing appropriate policies, this would eventually promote new policy exposition on multidimensional well-being. Families have a crucial responsibility to care for their children and prepare them for healthy, happy, and fruitful lives as active contributors to society; however, the capacity of parents to offer optimum care for their children – both economically and psycho-socially – is key (McNeill, Reference McNeill2010). As such, loving care, understanding, a secure attachment, socio-emotional support, non-coercive parenting styles, and an overall safe family environment are among the factors needed to raise happy adolescents that are satisfied with their lives. Notwithstanding, decisions of governments and other stakeholders shape the social environment, including but not limited to the distribution of material goods in which families live to nurture the next generation (McNeill, Reference McNeill2010). Governments can create opportunity structures that enhance the family’s capacity to provide protective social resources to young people while minimising risk factors introduced by the family in the home environment. As such, social policies should be shaped by a focus on health assets by addressing chronic poverty and material deprivation while promoting or at the very least not destabilising society’s social fabric (social capital), especially within the family context of young people. A government that enhances young people’s family social capital protects their right to social well-being and freedom of participation (a sense of belonging, social support, and support for autonomy and control) and invests in helping them reach their full economic potential.
Acknowledgements
We are thankful to the participating schools and adolescents without whose collaboration the data collection would not have been possible. We are grateful for the helpful comments from the two anonymous reviewers of the journal and to Satoshi Araki of Lingnan University for advising us on the use of the generalised ordinal regression models. All remaining errors remain our own.
Competing interests
The author(s) declare none.





 Open access
Open access