


Adolescence is a crucial period for physical and mental development, and the diet and eating behaviours which develop during these years tend to persist throughout the individual's life(Reference Wahl1–Reference Mikkila, Rasanen and Raitakari3). The eating habits and behaviours established during adolescence may be difficult to change later in life(Reference Kelder, Perry and Klepp4). Establishing healthy food consumption behaviours leads to nutritional adequacy, and eating behaviours influence morbidity and mortality in adolescence and in adulthood(Reference Guo, Wu and Chumlea5).
Breakfast skipping is reported to be one of the bad eating habits, and affects an individual's health status. For example, breakfast skipping was reported to be associated with weight gain(Reference Song, Chun and Obayashi6,Reference van der Heijden, Hu and Rimm7) and increase of BMI(Reference Watanabe, Saito and Henmi8,Reference Sakurai, Yoshita and Nakamura9) . Moreover, breakfast skipping was also reported to be associated with a higher prevalence of obesity(Reference van der Heijden, Hu and Rimm7), hypertension(Reference Stote, Baer and Spears10,Reference Shafiee, Kelishadi and Qorbani11) , hyperlipidaemia(Reference Shafiee, Kelishadi and Qorbani11,Reference Farshchi, Taylor and Macdonald12) , insulin insensitivity and type 2 diabetes(Reference van der Heijden, Hu and Rimm7) and CVD(Reference Shafiee, Kelishadi and Qorbani11,Reference Cahill, Chiuve and Mekary13) . Such reports might partly explain findings from previous cross-sectional and intervention studies which show that eating breakfast may be a predictor of healthy eating behaviour, and implies a high intake of dietary fibre, thiamine or folate, and a low intake of fat(Reference Deshmukh-Taskar, Radcliffe and Liu14–Reference Zhang, Cordeiro and Liu16). A systematic review of studies about breakfast skipping reported that one of the main factors for breakfast skipping was habituation(Reference Pendergast, Livingstone and Worsley17). The rate of breakfast skipping among Japanese adolescents has not decreased over the past 10 years and is slightly less than that of adults(18,19) . Thus, it is highly likely that breakfast skipping continues as a habit from adolescence to adulthood. Similarly, breakfast skipping has been reported as a public health issue worldwide, including in the USA(Reference Deshmukh-Taskar, Nicklas and O'Neil20) and the UK(Reference Coulthard, Palla and Pot21). Therefore, breakfast skipping in adolescence is accepted as one of the important public nutritional problems in the world.
There are a few reports about the association between breakfast consumption and the adequacy of nutrient intake among adolescents. For example, a UK study has reported that the intakes of folate, vitamin C, Ca and iodine for breakfast consumers were higher than those of breakfast skippers among children and adolescents aged 4–18 years; in addition, the proportion of breakfast consumers aged 4–18 years having adequacy of folate, vitamin C, Ca, Fe and iodine was higher among breakfast consumers(Reference Coulthard, Palla and Pot21). However, only specific nutrients were selected for comparison with reference values in this previous study. Additionally, a Belgium study reported that the consumers of a good-quality breakfast rich in cereals, dairy products and fruits/vegetables had higher intakes of protein, Fe, Ca, Mg, vitamin B1, vitamin B2 and vitamin C than did those who consumed breakfast of a lower quality such as only drinking a beverage with energy or those of less than 1674 kJ/meal (400 kcal/meal) among adolescents aged 13–18 years(Reference Matthys, De Henauw and Bellemans22). Positive associations have also been reported between breakfast skipping and vitamin and mineral intakes among Japanese adolescents(Reference Murakami, Livingstone and Fujiwara23). However, in this paper, the relationship between breakfast skipping and diet by sex was not studied because male and female participants were analysed as a single group. Additionally, the intakes were not compared with the Japanese dietary reference intake (DRI) values. It has been reported that growth in adolescence differs by sex(Reference Duncan Cance and Ennett24), and that the influence of breakfast skipping on diet is different between adolescent boys and girls (Belgian study)(Reference Matthys, De Henauw and Bellemans22). In girls, a focus on body image is thought to lead to breakfast skipping(Reference Bibiloni Mdel, Pich and Pons25). Therefore, it is necessary to examine the influence of breakfast skipping on nutrient intake adequacy by sex, and girls need special attention in this regard. Furthermore, previous reports have been limited to the relationship between breakfast skipping and nutrient intake of a few select nutrients or of nutrients in general; there are no reports on the association between breakfast skipping and the overall adequacy of habitual nutrient intake. Therefore, we aimed to examine the relationship between breakfast skipping and adequacy of total habitual nutrient intake among junior high school female students.
Methods
Study design and participants
A set of two self-administered questionnaires (i.e. a diet history questionnaire and lifestyle questionnaire) were distributed by teachers to 742 junior high school female students belonging to three schools in Kanto, Japan in June 2016. Students were asked to answer the questionnaires on their own, or in cooperation with their parents, if necessary. The completed questionnaires were examined by the research staff, and those with missing information were returned to the students for completion. Both questionnaires were completed by 575 female students.
We excluded students with missing data (n 17), with milk allergies (n 8), and those with a reported energy intake less than half the energy requirement for the lowest physical activity category, according to the Japanese DRI or that equal to or more than 1·5 times the energy requirement for the highest physical activity category (<4498 kJ/d or ≥16 945 kJ/d; n 34)(Reference Murakami, Miyake and Sasaki26). Thus, the final participants consisted of 516 junior high school female students. Written informed consent was obtained from all participants and their parents. This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Ethics Committee of Seitoku University, Japan (approval no. H27U056).
Frequency of meals and snacks
Participants reported the frequency of breakfast eating per week in the lifestyle questionnaire, by answering the question: ‘How many times per week do you have breakfast?’. The definition of breakfast was the first meal of the day, eaten before or at the start of daily activities (e.g. errands, travel and work), within 2 h of waking, typically no later than 10.00 hours, and of an energy level between 20 and 35 % of total daily energy needs, which has been defined by Timlin & Pereira(Reference Timlin and Pereira27). In the present study, we classified participants into two groups according to the frequency of breakfast eating: breakfast consumers group (seven times/week) and breakfast skippers group (0–6 times/week).
Using the lifestyle questionnaire, participants were also queried about the weekly frequency of lunch, dinner and snack consumption before and after dinner by means of the question ‘How many times per week do you have lunch, dinner, snacks before dinner and snacks after dinner?’. Due to the lack of any standard definition of lunch and dinner time in the literature, we defined lunch and dinner as meals eaten from 12.00 to 14.00 hours and from 16.00 to 20.00 hours, respectively.
Dietary assessment
Habitual dietary intake during the preceding month was assessed using a brief self-administered diet history questionnaire for Japanese children and adolescents (BDHQ15y)(Reference Okuda, Sasaki and Bando28). The BDHQ15y was developed based on the adult version of the validated brief self-administered diet history questionnaire for Japanese adults (BDHQ) that enquires about dietary history during the preceding month(Reference Kobayashi, Murakami and Sasaki29,Reference Kobayashi, Honda and Murakami30) . The BDHQ15y is a four-page structured questionnaire comprising sixty-seven questions on the frequency of intake of food items commonly cooked and consumed in Japan. Daily food, energy and selected nutrient intakes were calculated using an ad hoc computer algorithm for the BDHQ15y based on the Standard Tables of Food Composition in Japan(31). Validity of the BDHQ15y was verified by a study on the relationship between selected food intake and blood biomarker levels(Reference Okuda, Sasaki and Bando28). Food groups were categorised as per previous studies(Reference Kobayashi, Murakami and Sasaki29,Reference Asakura, Haga and Sasaki32) .
Any self-estimated dietary assessment cannot avoid under- or over-reporting of dietary intake(Reference Murakami, Miyake and Sasaki33,Reference Murakami, Livingstone and Okubo34) . Therefore, we adjusted the reported dietary intakes based on the assumption that each participant reported the estimated energy requirement (EER) when the physical activity level was at the second level to render the comparison between the reported nutrient intake and the Japanese DRI values practically possible. The following formula was used: dietary intake (unit/d) = reported dietary intake (unit/d)/reported energy intake (kJ/d) × EER (kJ/d). The percentage of daily energy intake was calculated using the crude value for total fat and carbohydrate intake. Additionally, food intake values were energy-adjusted using the density method (i.e. the percentage of energy for energy-providing nutrients and their amounts per 4184 kJ for food groups and other nutrients) to minimise the influence of dietary misreporting.
Determination of habitual nutrient intake inadequacy
Inadequacy of intake for each nutrient was determined by comparing nutrient levels with each dietary reference value according to the Japanese DRI using a previously reported method(Reference Okubo, Sasaki and Murakami35–Reference Kohri, Kaba and Itoh37). Different types of dietary reference values comprising the Japanese DRI were established according to their purpose. The estimated average requirement (EAR) is set to avoid insufficient intake of nutrients, whereas the tentative dietary goal to prevent lifestyle-related diseases (DG) is set to prevent non-communicable diseases.
An intake level below the EAR was considered as inadequate, and a cut-point method was used for the following fourteen nutrients with known EAR: protein, vitamin A expressed as retinol activity equivalents, vitamin B1, vitamin B2, niacin expressed as niacin equivalents, vitamin B6, vitamin B12, folate, vitamin C, Ca, Mg, Fe (EAR reference values for during menstruation because 87·7 % female adolescents aged 12–15 years have experienced their first menstruation(Reference Tamura, Saito and Asada38)), Zn and Cu. For the following five nutrients, the intake level outside the range of DG values was considered as not meeting the standard DG: total fat, carbohydrate, total dietary fibre, Na expressed as salt-equivalents, and K.
Other variables
Using the BDHQ15y, participants were asked about their body weight and height. The BMI was calculated as weight (kg) divided by the square of height (m). In the BDHQ15y, participants also reported the weekly frequency of performing exercises such as sports club activities for the past month (every day, 4–6 d/week, 2–3 d/week, 1 d/week, or never). Additionally, participants reported on the following variables by completing a self-administered lifestyle questionnaire: employment status of father (full-time, part-time, housekeeping, or other), and employment status of mother (full-time, part-time, housekeeping, or other).
Statistical analysis
All statistical analyses were performed using the IBM SPSS statistics software package (version 22.0; SPSS Inc.). All reported P values were two-tailed, and a P value of 0·05 was considered as statistically significant. The differences in characteristics between breakfast consumers and breakfast skippers were compared using the χ2 test for categorical variables and the independent t test for continuous variables. Potential confounding factors considered in the adjusted model were school type (public or private), frequency of lunch skipping (0 d/week or 1–7 d/week), dinner skipping (0 d/week or 1–7 d/week), and snack eating before dinner (0 d/week or 1–7 d/week) which were found to be substantially different (P < 0·05) between groups categorised by the frequency of breakfast consumption, and snack eating after dinner (0 d/week or 1–7 d/week) observed in associations with nutrient or food intake. The difference in the mean nutrient intake between the two groups was compared using an independent t test in the crude model, while a covariate analysis (ANCOVA) was performed to adjust for confounding variables (such as school type, frequency of lunch skipping, dinner skipping, snack eating before dinner, and snack eating after dinner) in the adjusted model. The nutritional inadequacy of each nutrient intake was represented as the proportion of participants whose intake was below the EAR or outside the range of the DG in each group. The χ2 test for the crude model and the logistic regression analysis adjusted for school type, frequency of lunch skipping, dinner skipping, snack eating before dinner, and snack eating after dinner for the adjusted model were used to examine the difference in the prevalence of not meeting DRI between breakfast consumers and skippers.
The overall nutritional inadequacy of participants was determined based on the number of nutrients that did not meet the DRI values of the fourteen nutrients with EAR and five nutrients with DG. Differences in the number of nutrients that did not meet DRI between the breakfast consumers and skippers groups were assessed by the independent t test in the crude model and a covariate analysis to adjust for school type, frequency of lunch skipping, dinner skipping, snack eating before dinner, and snack eating after dinner in the adjusted model.
Results
The basic characteristics of the participants are shown in Table 1. The incidence of breakfast skipping was significantly lower in students attending public junior high school than in those attending private junior high school (44·9 v. 55·1 %; P = 0·002). Students having breakfast every day were likely to have lunch and dinner every day in comparison with those who did not necessarily eat breakfast every day (both P < 0·001). Additionally, the proportion of students eating snacks before dinner every day was significantly higher in breakfast consumers than in breakfast skippers (P = 0·003). The proportion of students skipping breakfast 1–2 d/week was approximately 60 % among breakfast skippers. There were no significant differences in grade, BMI, the number of participants who engaged in habitual exercise, energy intake, working status of the father and mother, and the proportion of eating snacks after dinner every day, between breakfast consumers and skippers.
Table 1. Characteristics of study participants categorised into breakfast consumers and skippers (n 516)
(Numbers and percentages; mean values and standard deviations)
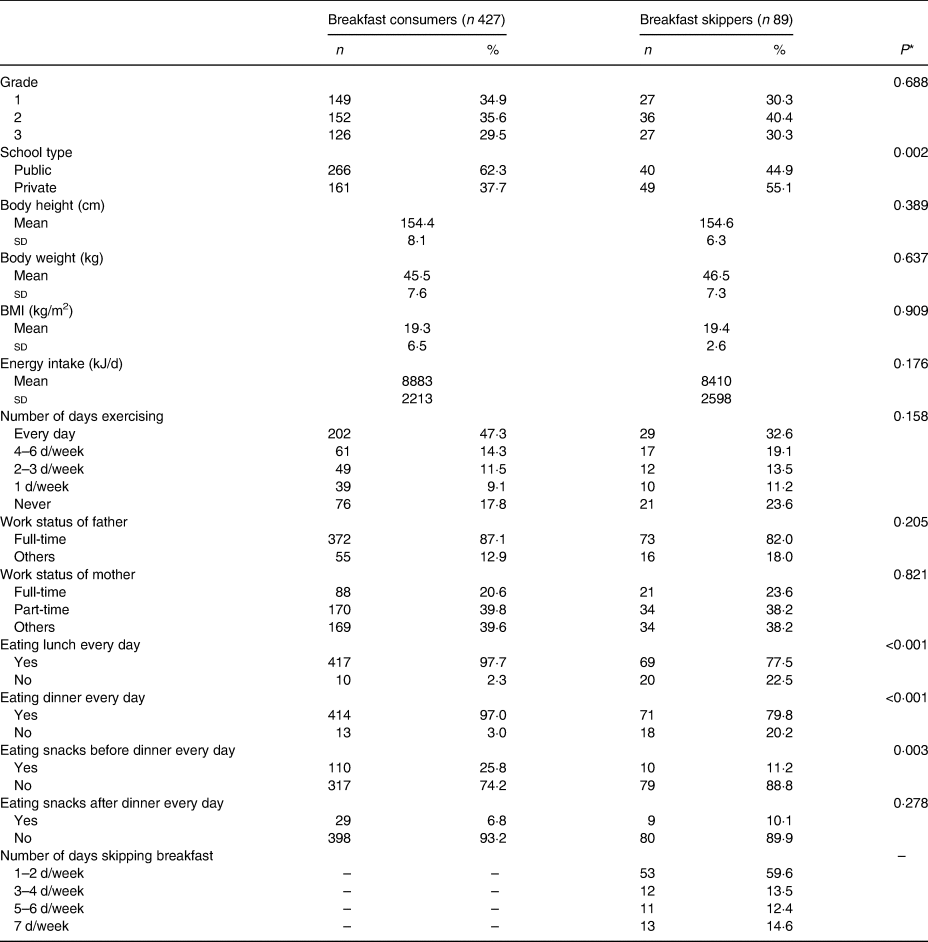
* The P values are shown for the χ2 test for categorical variables and for the independent t test for continuous variables and pertain to comparisons between breakfast consumers and skippers.
The daily nutrient intake and nutrient intake inadequacy among 516 junior high school female students are shown in Table 2. In the crude model, most nutrient intakes except those of fat, carbohydrate, total dietary fibre, vitamin A, niacin, vitamin B12 and Na were significantly higher in breakfast consumers than in breakfast skippers. In the adjusted model, the carbohydrate intake of breakfast skippers was higher than that of breakfast consumers. The proportion of students having inadequacy of vitamin B1, vitamin B2, vitamin C, Ca, Zn and K was significantly lower in breakfast consumers than in breakfast skippers in the crude model, while the significant difference in vitamin A and Fe intake inadequacy was additionally found in the adjusted model. With reference to Na intake inadequacy alone, the proportion of participants showing inadequacy was higher in breakfast consumers group compared with that in the breakfast skippers group.
Table 2. Daily nutrient intakes and prevalence of not meeting estimated average requirement (EAR) and tentative dietary goal to prevent lifestyle-related disease (DG) among 516 female junior high school students categorised into breakfast consumers and skippers*
(Mean values and standard deviations)
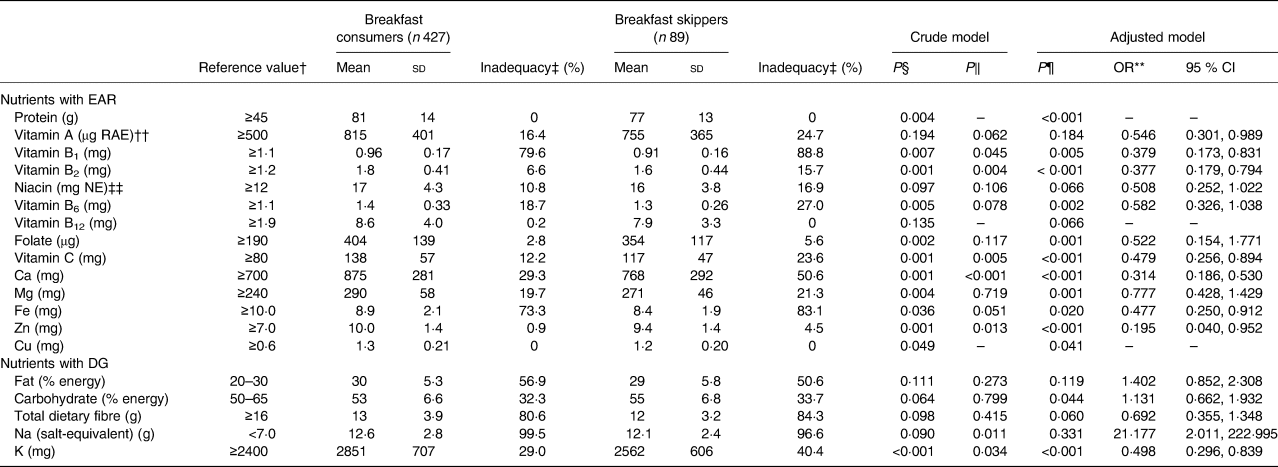
RAE, retinol activity equivalents; NE, niacin equivalents; DRI, dietary reference intake.
* Adjustment of reporting error was performed according to the following: nutrient intake = reported nutrient intake/reported energy intake × estimated energy requirement.
† DRI for 12- to 14-year-old Japanese girls. The estimated energy requirement of physical activity level II is 10 042 kJ/d.
‡ Percentage of participants whose nutrient intake did not meet DG or EAR of DRI. Each nutrient intake was compared with the appropriate DRI value using the cut-point method.
§ P values are shown for independent t test to analyse differences of nutrient intake between breakfast consumers and skippers.
ǁ P values are shown for the χ2 test to analyse differences in the prevalence of participants with inadequate nutrient intake between breakfast consumers and skippers.
¶ P values are shown for covariate analysis to analyse difference of nutrient intake between breakfast consumers and skippers adjusted for confounding variables of school type (public or private), frequency of lunch skipping (0 d/week or 1–7 d/week), dinner skipping (0 d/week or 1–7 d/week), and snack eating before dinner (0 d/week or 1–7 d/week).
** Multivariate adjusted OR about nutrient intake inadequacy of breakfast skipper with reference to breakfast consumers were calculated by adjusting for frequency of school type (public or private), lunch skipping (0 d/week or 1–7 d/week), dinner skipping (0 d/week or 1–7 d/week), snack eating before dinner (0 d/week or 1–7 d/week) and snack eating after dinner (0 d/week or 1–7 d/week).
†† Sum of retinol, β-carotene/12, α-carotene/24, and cryptoxanthin/24.
‡‡ Sum of niacin and protein/6000.
Table 3 shows the overall nutritional inadequacy among female junior high school students in the breakfast consumers and skippers groups. The total number of nutrients not meeting EAR among breakfast consumers was lower than that among breakfast skippers in the adjusted model, while the total number of nutrients not meeting DG did not differ significantly between the two groups.
Table 3. Number of nutrients not meeting tentative dietary goal (DG) and estimated average requirement (EAR) among 516 female junior high school students categorised into breakfast consumers and skippers
(Mean values and standard deviations)

* P values are shown for the independent t test to analyse differences between breakfast consumers and skippers.
† P values are shown for covariate analysis to analyse differences between breakfast consumers and skippers adjusted for confounding variables of school type (public or private), frequency of lunch skipping (0 d/week or 1–7 d/week), dinner skipping (0 d/week or 1–7 d/week), snack eating before dinner (0 d/week or 1–7 d/week) and snack eating after dinner (0 d/week or 1–7 d/week).
The habitual food groups intake among female junior high school students is shown in Table 4. In the crude model, the daily intakes of total vegetables, green and yellow vegetables, other vegetables, green tea and dairy products were significantly higher among breakfast consumers than among breakfast skippers, while noodle and soft drink intakes were significantly lower among breakfast consumers than among breakfast skippers. In addition to the above-mentioned differences found with the crude model, higher fruit intake among breakfast consumers was found with the use of the adjusted model.
Table 4. Daily food group intakes among 516 female junior high school categorised into breakfast consumers and skippers (g/4184 kJ)*
(Mean values and standard deviations)

* Adjustment of reporting error was performed according to the following: food group intake = reported food group intake/reported energy intake × 4184 (kJ).
† P values are shown for the independent t test to analyse differences between breakfast consumers and skippers.
‡ P values are shown for covariate analysis to analyse differences between breakfast consumers and skippers adjusted for confounding variables of school type (public or private), frequency of lunch skipping (0 d/week or 1–7 d/week), dinner skipping (0 d/week or 1–7 d/week), eating a snack before dinner (0 d/week or 1–7 d/week) and snack eating after dinner (0 d/week or 1–7 d/week).
Discussion
The present study examined the association of breakfast skipping with nutrient adequacy in female junior high school students. We found that junior high school female students who ate breakfast every day had higher intakes of most nutrients and lower inadequacy of nutrient intakes than those who skipped breakfast. To the best of our knowledge, the present study is the first to examine the relationship between breakfast skipping and overall nutrient intake adequacy among female junior high school students in Asia including Japan.
In the present study, the rate of breakfast skipping among female students was 17·2 %; this result is in agreement with those published from other countries including the USA (18·0 %)(Reference Drewnowski, Rehm and Vieux39), UK (19·9 %)(Reference Coulthard, Palla and Pot21) and Belgium (16·9 %)(Reference Matthys, De Henauw and Bellemans22). However, the rate of breakfast skipping in the present study was inconsistent with the rate previously reported for Japanese adolescents (2·3 %)(Reference Murakami, Livingstone and Fujiwara23). The possible reasons for this could be differences in participant characteristics and in the definition of breakfast skipping between studies. The participants in the previous study included both girls and boys(Reference Murakami, Livingstone and Fujiwara23). Another previous study has reported that the proportion of breakfast skippers among adolescents was higher in girls than in boys(Reference Coulthard, Palla and Pot21,Reference Matthys, De Henauw and Bellemans22) . Thus, the higher breakfast skipping rate observed in the present study may have been because this study only included girls. Additionally, breakfast skippers in the previous study were defined as individuals who reported that they did not consume any foods or beverages at breakfast in the 1-d dietary records(Reference Murakami, Livingstone and Fujiwara23); however, in this study, individuals whose frequency of breakfast consumption was 0–6 times/week were defined as breakfast skippers. The difference in the definition of breakfast skipping between studies may have produced the differences in results.
The rate of breakfast skipping was significantly higher among students from private schools than among those from public schools. It has been reported that the proportion of private/public junior high school students is directly proportional to the commute time(40,41) . Additionally, one of the reasons for breakfast skipping was lack of time (for eating breakfast) in the morning(Reference Pendergast, Livingstone and Worsley17). This may explain the difference in the rate of breakfast skipping between public and private school students; however, further studies are needed to examine the influence of the school type on breakfast skipping. It was observed that the rate of lunch or dinner skipping was higher among breakfast skippers than among breakfast consumers in the present study. A study of Japanese adults reported that breakfast skippers were likely to have the unhealthy lifestyle habit such as irregular time of eating dinner(Reference Yokoyama, Onishi and Hosoda42). This result was consistent with that of the present study. However, the proportion of students eating snacks before dinner every day was higher in the breakfast consumers than in the skippers group, which was not similar to the finding from the previous study which reported a lower proportion of people having snacks every day among breakfast consumers among Japanese adults(Reference Yokoyama, Onishi and Hosoda42). The difference in results between the two studies might be due to the fact that the energy requirement was different for adults and junior high school students(43). However, the content of the snack was not explained, and, thus, further studies are needed.
A Japanese study has reported that the intakes of vitamins and minerals were higher among breakfast consumers than among breakfast skippers(Reference Murakami, Livingstone and Fujiwara23). Additionally, a UK study reported that the intakes of folate, vitamin C, Ca and Fe were higher in breakfast consumers than in breakfast skippers(Reference Coulthard, Palla and Pot21). These results are consistent with the results of the present study. In the present study, it was observed that the intakes of most nutrients excluding fat, carbohydrate, total dietary fibre, vitamin A, niacin, vitamin B12 and Na were higher among breakfast consumers than among skippers in crude model analysis. In the present study, habitual vitamin A, niacin, vitamin B12, fat, total dietary fibre and Na intake were the only six parameters which were not significantly different between the two groups both in the crude and the adjusted model. Regarding vitamin A intake, one reason for the lack of significant difference between groups may be that the intake was highly varied between individuals and well as in a single individual over time(Reference Fukumoto, Asakura and Murakami44). Thus, it is possible that the results were influenced by characteristics of food intake pattern, and not necessarily by the meal itself. Therefore, further study will be needed to reveal the food sources and intake levels as per each of the food sources for vitamin A among Japanese adolescents. However, in the adjusted model, the proportion of participants in our study who showed vitamin A intake adequacy was higher in breakfast consumers than in breakfast skippers. This result was similar to that from a previous study which suggested a difference of vitamin A intake adequacy based on breakfast consumption, among Canadian girls aged 4–18 years(Reference Barr, DiFrancesco and Fulgoni45). Therefore, evidence suggests that vitamin A nutrient inadequacy is affected by the frequency of breakfast consumption.
On the one hand, no differences were observed in the habitual niacin, vitamin B12, fat and total dietary fibre intake adequacy. The results of niacin and vitamin B12 intakes in the present study were consistent with those of a previous study which observed no differences in niacin and vitamin B12 intakes between breakfast consumers and skippers among adolescents(Reference Murakami, Livingstone and Fujiwara23). Regarding fat intake, the result of no difference between breakfast consumers and skippers in the present study is consistent with a UK adolescents study(Reference Coulthard, Palla and Pot21) and Japanese study(Reference Murakami, Livingstone and Fujiwara23) which assessed fat as macronutrient balance (% energy). Thus, the fat intakes in terms of macronutrient balance (% energy) may not be associated with breakfast skipping among Japanese female adolescences. Additionally, for total dietary fibre, the proportion of people who meet total dietary fibre value of DRI was low. This may partly explain the deficiency in total dietary fibre which was reported among many Japanese adolescent girls and young women(Reference Kobayashi, Asakura and Suga36,Reference Asakura and Sasaki46) . Therefore, total dietary fibre intake may be deficient regardless of breakfast consumption, and breakfast skipping is unlikely to be the most significant factor to influence this outcome. However, Na inadequacy was higher among breakfast consumers than among breakfast skippers. In the present study, breakfast consumers had a higher vegetable intake than did breakfast skippers. Vegetables are cooked with salt seasoning like miso soup served with rice in the traditional Japanese dietary pattern(Reference Okubo, Sasaki and Murakami47), which was reported as the main source of Na in the Japanese diet(Reference Asakura, Uechi and Masayasu48). This may partly explain the present result that the inadequacy of Na intake may be higher among breakfast consumers.
A higher intake of carbohydrates was observed among breakfast skippers than in consumers in adjusted model analysis. This may be partly explained by the higher intakes of noodles and soft drinks among breakfast skippers in the present study. This result was consistent with a previous study which reported that young Japanese women aged 18–20 years who sleep late are more likely to skip breakfast and tend to eat noodles(Reference Sato-Mito, Sasaki and Murakami49). Moreover, sleep restriction has been reported to be associated with a carbohydrate intake preference(Reference Broussard, Kilkus and Delebecque50). Breakfast skippers may have a short sleep time(Reference Sato-Mito, Sasaki and Murakami49), which may have increased carbohydrate intake. Further study is needed to explain the higher carbohydrate intake among breakfast skippers in consideration of bedtime and wake-up time.
There was little to no nutrient inadequacy of protein, vitamin B12 and Cu among the entire study population (incidence: 0 %). The proportion of Japanese adolescent girls(Reference Asakura and Sasaki46) and young women(Reference Kobayashi, Asakura and Suga36) with insufficient intakes of these nutrients was reported to be very small, and thus these reports are consistent with our present findings. In other words, protein, vitamin B12 and Cu might be nutrients which are sufficiently consumed by Japanese people, and the adequacy of these nutrients may not be related to breakfast skipping.
The habitual intakes of vitamin B6, folate and Mg were higher among breakfast consumers than among breakfast skippers, which was consistent with the result that the contribution of vitamin B6, folate and Mg intakes at breakfast was reported to be approximately 20 % of total intake of these nutrients(Reference Drewnowski, Rehm and Vieux39). However, the nutrient intake adequacy of vitamin B6, folate and Mg intakes was not different between the two groups both in crude model and adjusted model analyses. A previous study in Japanese adolescents reported that there only a few people who did not meet the EAR of vitamin B6, folate and Mg(Reference Asakura and Sasaki46). The nutrient intakes in the previous study were assessed by dietary records, while our study used a diet history questionnaire. It is possible that this difference in dietary survey methods may have affected the results. Additionally, the nutrient adequacy of vitamin B6, folate and Mg differs considerably based on dietary patterns among Japanese young women(Reference Okubo, Sasaki and Murakami35). Therefore, further study will be needed to reveal the food sources for vitamin B6, folate and Mg among Japanese adolescents; additionally, the influence of type of dietary pattern on intake levels of those nutrients among adolescent girls also needs to be evaluated.
Regarding vitamin B1, vitamin B2, vitamin C, Ca, Fe, Zn and K, both the habitual nutrient intakes and nutrient adequacy were observed to be different between breakfast consumers and skippers. These results were consistent with those from a previous study(Reference Coulthard, Palla and Pot21–Reference Murakami, Livingstone and Fujiwara23,Reference Fukumoto, Asakura and Murakami44) . Therefore, the intakes and deficiency of many vitamins and minerals may be affected by breakfast skipping.
The overall nutritional inadequacy was observed in the difference of the total number of nutrients not meeting EAR between breakfast consumers and skippers, but not those not meeting DG. A difference in energy intake between breakfast consumers and skippers was not observed. About half of the nutrients for which DG is set are energy-providing nutrients such as carbohydrate and fat. On the other hand, most nutrients for which EAR is set are vitamins and minerals. For a majority of these, there was observed a difference of nutritional inadequacy for each nutrient between breakfast consumers and skippers in the present study. Additionally, these results that were observed in the difference of vitamins and minerals intake adequacy were similar to the previous study results that showed the difference of vitamins and minerals intake adequacy such as vitamin C, Ca and Fe with or without breakfast(Reference Coulthard, Palla and Pot21). These may partly explain the present result of overall nutritional inadequacy.
Higher intakes of fruit, vegetables, green tea and dairy products and lower intakes of noodles and soft drinks were observed among breakfast consumers than among breakfast skippers. The results of the present study were consistent with those from previous studies which reported higher intakes of fruits, vegetables and dairy products(Reference Murakami, Livingstone and Fujiwara23,Reference Drewnowski, Rehm and Vieux39,Reference Min, Noh and Kang51) , and lower intakes of soft drinks(Reference Murakami, Livingstone and Fujiwara23), among breakfast consumers. It has also been reported that Japanese tend to consume green tea during meals(52). However, breakfast skippers have been reported to be higher consumers of soft drinks(Reference Smith and Richards53). These may partly explain the present study results that there was no difference of beverage consumption between breakfast consumers and skippers, while breakfast consumers had higher green tea consumption and lower soft drink consumption than breakfast skippers in the present study. Moreover, a dietary pattern including higher vegetable intake was reported to be a healthy dietary pattern, while that consisting of higher noodle intake was reported to be an unhealthy dietary pattern(Reference Okada, Takahashi and Takimoto54). Consequently, the consumption of breakfast every day may lead to a healthier dietary pattern among female junior high school students.
Several limitations of this study need to be mentioned. First, the participants in the study were not sampled randomly from the general population, and the survey area was restricted to a single region in Japan. The participants were therefore probably not representative of Japanese adolescents. Second, we used the BDHQ15y to assess dietary intake, although its ability to estimate dietary intakes has been validated on a limited number of foods and nutrients. Third, we could not include intake from dietary supplements in the analysis because reliable composition tables of dietary supplements were lacking in Japan. Fourth, household income, education, sleep duration, wake-up time, bedtime and nutritional habits of participants' parents were not investigated. These factors have been reported to influence children's diets(Reference Sato-Mito, Sasaki and Murakami49,Reference Serra-Majem, Ribas and Ngo55–Reference Al-Shookri, Al-Shukaily and Hassan57) . Although the employment status of participants’ parents was examined in this study, this information is not necessarily equivalent to data on household income. Finally, we did not examine whether the participants had experienced their first menstruation, although the EAR for Fe changes depending on menstruation. A previous study reported that 585 out of 4769 female students (12·3 %) aged 12–15 years had not experienced their first menstruation, and the majority of these girls were 12 years old(Reference Tamura, Saito and Asada38). Because junior high school female students are likely to have their first menstruation shortly, they would need higher Fe intake. Thus, we considered that the EAR for Fe for menstruating women was a more appropriate reference value to assess nutritional adequacy in this study.
Conclusions
This cross-sectional study showed that breakfast skipping was related to the deficiency of many vitamins and minerals such as that of vitamin A, vitamin B1, vitamin B2, vitamin C, Ca, Fe, Zn and K among Japanese female junior high school students. Additionally, breakfast consumption was likely to lead to a healthier dietary pattern. Therefore, further studies are needed to clarify the factors related to skipping breakfast to devise a strategy for improving dietary behaviour among adolescent girls.
Acknowledgements
The authors would like to express their thanks to R. Tanaka, F. Tanaka, A. Niwayama and M. Yamaguchi who prepared the questionnaire distribution.
This study was supported by the Milk Education Research Council and Japan Dairy Association 2016. The Milk Education Research Council and Japan Dairy Association had no role in the design, analysis or writing of this article.
Author contributions were as follows: all authors contributed to the concept and design of the survey, and to data collection. M. M., A. S. and A. M. contributed to data management. M. M., Y. H. and A. S. conducted the statistical analysis. M. M. drafted the paper. Y. H., A. S., A. M. and S. I. provided input for the final draft of the manuscript. All authors read and approved the final manuscript.
There were no conflicts of interest.





 Open access
Open access