



Hurricanes have devastating impacts on infrastructure including hospitals and health centers and cause a surge in acute and emergency care. Reference Stephens, Wilt and Lehnert1–Reference Mitsova, Esnard and Sapat4 However, the effect of a hurricane on routine care after the immediate danger has passed is less well known. Studies have found that health-care access following natural disasters has been linked with decreased access to health care. Reference Cortés, Lassalle and Perreira5–Reference Flores, Collins and Grineski8 Most of the research has examined the effect of 1 disaster on 1 specific region, but there is limited evidence comparing the effects of hurricanes on access to care for different regions. Therefore, this study compared the effect of hurricanes on routine checkup by states that had a major hurricane (category 3-5) make landfall versus states that were impacted by a category 1-2 hurricane.
Methods
In this cross-sectional study, we analyzed the Behavioral Risk Factor Surveillance Survey (BRFSS). 9 We compared Puerto Rico (2017 Hurricane Irma, Hurricane Maria), Texas (2017 Hurricane Harvey), and Florida (2017 Hurricane Irma, Hurricane 2018 Michael) with states that had a category 1-2 hurricane make landfall from 2014 to 2019: Georgia, Louisiana, Mississippi, North Carolina, and South Carolina. The sample consisted of 323,319 respondents aged 18 and older. We excluded states that did not have a hurricane make landfall during the study period.
The outcome was a binary indicator of getting a routine checkup within the past year. The predictor variable of interst was living in a state that had a Hurricane category 1 or greater make landfall during the study period. Control variables included age (18-24, 25-34, 35-44, 45-54, 55-64, 65 and older), female or male sex, race/ethnicity (White non-Hispanic, Black non-Hispanic, Hispanic, American Indian or Alaskan Native non-Hispanic, Asian, Native Hawaiian or other Pacific Islander non-Hispanic, other/multiracial), marital status (married/cohabiting, formerly married, never married), presence of children in the household, education (Less than High School, High School Graduate, More than High School), employed or not, income ($75,000+ vs <$75,000), having any health insurance or not, and general health (Good or Better Health vs Fair or Poor Health).
We present trends with 95% confidence intervals for getting a routine checkup within the past year that account for survey weights, strata, and population sampling units. The predicted probabilities were calculated from logistic regression by creating an interaction term for year and state. BRFSS is publicly available with deidentified observations, therefore, the Drexel University human research protection program deemed it exempt from institutional review board approval. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.
Results
Figure 1 shows the unadjusted trend in routine checkup within the past year. Respondents in Puerto Rico reported a higher probability of routine checkup within the past year compared with the other states until 2017. There was no difference in routine checkup between Puerto Rico and Florida from 2017 to 2019 but Puerto Rico continued to have a greater likelihood of routine checkup compared with the control states. Florida residents had a significantly higher probability of routine checkup compared with the control states in 2016. Respondents in Texas reported the lowest probability of getting a routine checkup in the past year compared with the other states.
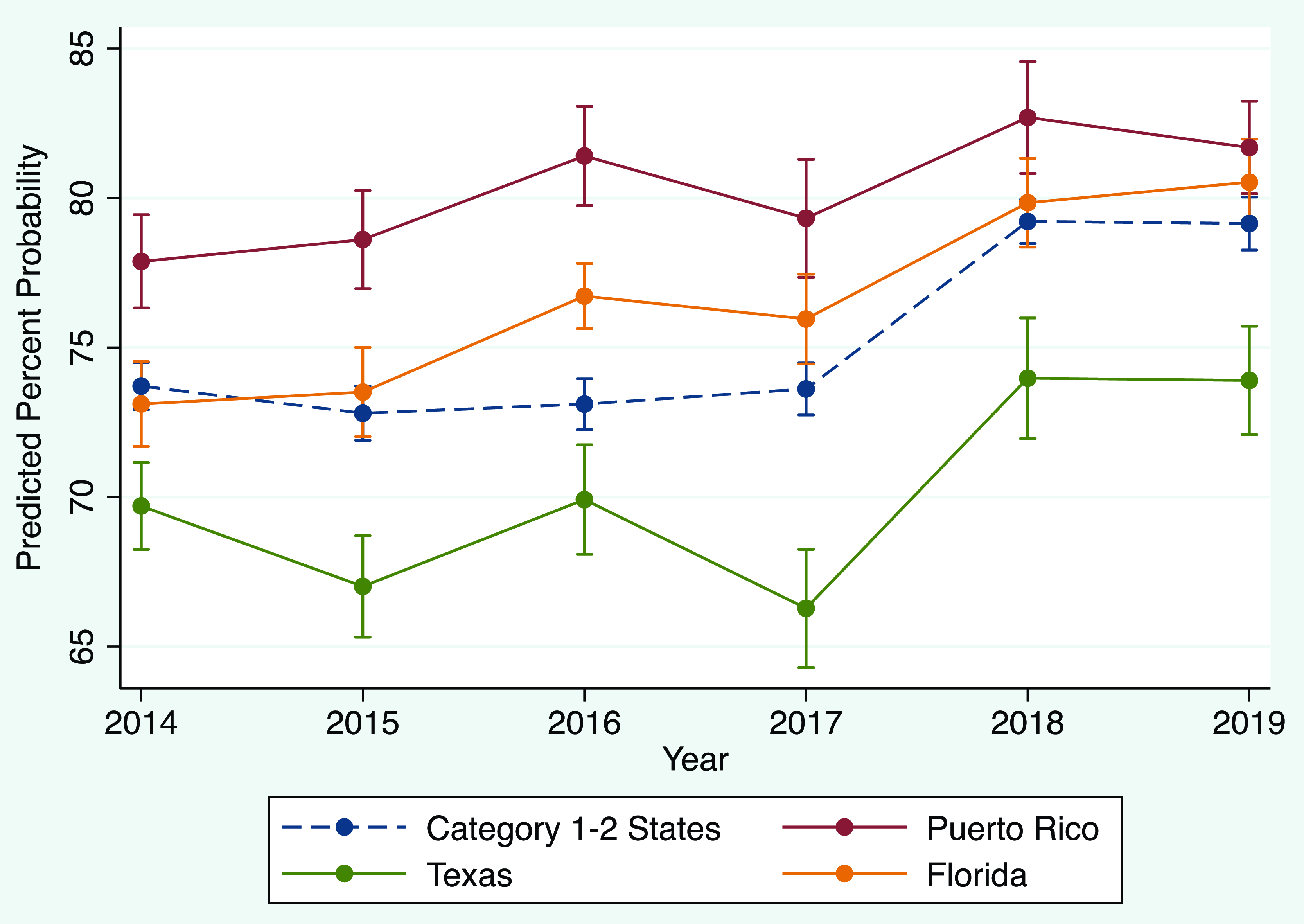
Figure 1. Weighted unadjusted trend in routine checkup within the past year among adults. Note: Data from the 2014-2019 Behavioral Risk Factor Surveillance Survey (BRFSS). BRFSS survey weights, strata, and population sampling units were applied. Hurricane category 1-2 states include Georgia, Mississippi, Louisiana, North Carolina, South Carolina.
Table 1 shows that, in 2016, the year before the 2017 hurricane season, the probability of routine checkup in Puerto Rico and Florida were similar and both were higher than Texas and the control states. In 2017, there was a decrease in routine checkup compared with the prior year for the major hurricane states (Puerto Rico -4%, Texas -3%, Florida -1%) and no change in 2017 for the control states. Texas had statistically significant drop in routine checkup in 2017 compared with the other hurricane states. By 2018, the estimate for routine checkup significantly increased to the highest level in the study period for all states: Puerto Rico (78%), Texas (76%), Florida (79%), control states (78%). The smallest increase in 2018 for routine checkup was in Florida (4%), which had another major hurricane make landfall that year. In 2019, there was no significant change in reporting routine checkup in any of the states. Moreover, there was no difference in the probability of routine checkup across states in 2018 and 2019.
Table 1. Multivariate adjusted marginal effects for routine checkup within the past year among adults

Note: Data from the 2014-2019 Behavioral Risk Factor Surveillance Survey (BRFSS). BRFSS survey weights, strata, and population sampling units were applied. Hurricane category 1-2 states include Georgia, Mississippi, Louisiana, North Carolina, South Carolina. Marginal effects estimated from multivariate logistic regression controlling for age, sex, race/ethnicity, marital status, presence of children in the household, education, employment status, income, health insurance, and general health.
Discussion
Our study compared the trend in routine checkup for states that were exposed to a hurricane. Our study makes a unique contribution by comparing the impact of a hurricane on routine care across multiple states and over time. However, our results should be interpreted as conservative especially for Texas where the bulk of the hurricane impact was in the southeast area of the state. Second, we were unable to conduct a difference in difference study design because the data violated the parallel trends assumption.
We found that states impacted by a major hurricane in 2017 had a drop in routine checkup while the states that experienced a category 1-2 landfall did have a change in that year. By the following year, all states reported an increase in routine checkup suggesting that the disruption in routine checkup was temporary. The effect may have been most pronounced in Texas, which is a state that has the highest uninsurance rate in the United States. 10 Our findings are consistent with studies that have examined specific hurricanes or areas and documented disruptions in access to care. Reference Cortés, Lassalle and Perreira5–Reference Flores, Collins and Grineski8 The long-term impact on disruptions to routine care associated with disasters, such as delayed diagnosis and treatment of chronic disease, warrant further investigation.
Author contribution
Concept and design: A.N.O., J.P.S.; Acquisition, analysis, or interpretation of data: J.P.S., A.N.O., D.L.M., A.C.R.-G.; Drafting of the manuscript: J.P.S., D.L.M., A.N.O., A.C.R.-G.; Critical revision of the manuscript for important intellectual content: A.N.O., D.L.M., A.C.R.-G.; Statistical analysis: J.P.S.; Obtained funding: A.N.O.; Administrative, technical, or material support: A.N.O.; Supervision: A.N.O.
Funding
This research was supported by the National Institute on Minority Health and Health Disparities (NIMHD) under award numbers R01MD013866 and R01MD016426. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIMHD. The funders had no role in study design, data analysis, decision to publish, or preparation of the manuscript.
Competing interests
The authors have declared that no competing interests exist.



 Open access
Open access