



The COVID-19 pandemic and nationally mandated restrictions to control the virus have been anticipated to increase the incidence of population mental ill health.Reference Holmes, O'Connor, Perry, Tracey, Wessely and Arseneault1 In the UK these restrictions have varied from strict ‘lockdowns’ during peaks in disease transmission limiting time outside the home, travel, the ability to work, the delivery of education and services; to more enduring restrictions such as self-isolation, quarantine, encouraged working from home, physical distancing and mask wearing. Quarantine and physical distancing may increase feelings of isolation and loneliness that are known to be associated with an increased risk of anxiety, depression, self-harm and suicide.Reference Matthews, Danese, Caspi, Fisher, Goldman-Mellor and Kepa2 Those with pre-existing conditions may experience an exacerbation of symptoms because of fear, changing stressors or reduced access to services.Reference Yao, Chen and Xu3 In order to inform management of mental health resources as we emerge from the COVID-19 pandemic it is vitally important to understand who are most at risk.
Impact of the pandemic on mental health
However, the research to date has produced conflicting reports. UK-based surveys in the early stages of lockdown suggested no marked increase in depression or anxiety symptoms.Reference O'Connor, Wetherall, Cleare, McClelland, Melson and Niedzwiedz4 A recent wave of the Opinions and Lifestyle Survey, a weekly survey distributed to approximately 5000 households in the UK since the beginning of the pandemic in March 2020, found that well-being measures have remained stable with only anxiety increasing slightly.5 A number of studies using data from the UK Household Longitudinal Study have found higher than expected increases in 12-item General Health Questionnaire scores as the pandemic emerged in April and June 2020, especially in those aged 18–34 years.Reference Pierce, Hope, Ford, Hatch, Hotopf and John6,Reference Niedzwiedz, Green, Benzeval, Campbell, Craig and Demou7 However, the biggest rise in positive responses where to items such as ‘Less able to enjoy day-to-day activities’ and ‘Not feeling useful’, which would be expected given the extraordinary circumstance of ‘lockdown’.Reference Niedzwiedz, Green, Benzeval, Campbell, Craig and Demou7 But what is not known is the prevalence of clinically relevant symptoms in this group. The Mental Health of Children and Young People survey found that probable mental health conditions increased from 10.8% in 2017 to 16.0% in July 2020, although the mental health of the UK child population had been deteriorating in the pre-pandemic period.Reference Ford, John and Gunnell8,Reference Pierce, McManus, Jessop, John, Hotopf and Ford9 The limitations of survey-based research has been highlighted in a recent commentary in the Lancet Psychiatry,Reference Pierce, McManus, Jessop, John, Hotopf and Ford9 reiterating the call for high-quality, validated, longitudinal, whole population data-sets as stated by Holmes et al in their early COVID research position paper.Reference Holmes, O'Connor, Perry, Tracey, Wessely and Arseneault1
Impact of the pandemic impact on psychotropic medication use
A recent report of increased antidepressant prescribing associated with the lockdown in England is limited in that it was based on prescription items rather than the number of individuals in receipt of antidepressant medication and was limited to 2 years of data, thus failing to incorporate the pre-existing increasing trends in the uptake of antidepressant medication in the UK.Reference Armitage10,Reference Walker, Croker, Curtis, MacKenna and Goldacre11 Despite warnings of an impending ‘tsunami’ of mental health problems, to date there is no consistent, empirical evidence of an increase in suicide, self-harm, suicidal behaviour or suicidal thoughts associated with the pandemic.Reference John, Eyles, Webb, Okolie, Schmidt and Arensman12,Reference Jia, Ayling, Chalder, Massey, Broadbent and Coupland13
This study uses population-wide primary care data linked to prescription medication data to explore the impact of the COVID-19 pandemic on psychotropic medication uptake at an individual level. Annual trends will be explored from 2012 to 2020. It is hypothesised that the consequences of the pandemic, and related stressors, for mental health will be influenced by a range of modifiable and non-modifiable factors. Identification of the latter will be critical in determining who may be at greatest risk of mental health difficulties and should be the focus of future interventions.
Method
Study design and participants
This was a population-based, data-linkage study of prescribed psychotropic medication uptake for individuals in Northern Ireland during the lockdown period (March to October 2020) compared with the previous patterns in the pre-pandemic period (January 2012 to February 2020) within the Administrative Data Research Centre –Northern Ireland. Cohorts of individuals aged 10 years and over each month, starting 1 January 2012, were defined from the national central health card registration system (National Health Application and Infrastructure Services (NHAIS) system) which contains information on all patients registered with a primary care physician. Northern Ireland has a universal, tax-financed, free-at-the-point-of-service healthcare system so almost the entire population are registered on NHAIS. This also includes basic demographic details and address information for each patient as well as their health and care number (HCN), a unique identifier that facilitates exact matching to other health system data-sets.
The sample size varied month by month (ranging from 1 448 871 in January 2012 to 1 600 346 in October 2020) as monthly denominators were created identifying individuals who fulfilled the eligibility criteria: alive and resident in Northern Ireland, aged at least 10 years and not in an institution (for example care facility, prison). The cohort was limited to those aged 10 years and over living in the community, as psychotropic medications are less likely to be prescribed in the very young and prescribing may differ in residential care settings. NHAIS receives regular updates from the General Registrar's Office, allowing removal of patients who are deceased from analysis.
In addition to gender and age in full years at each study month, the NHAIS database was used to identify people living alone (single-person households) as this is a known risk factor for poor mental health.Reference Joutsenniemi, Martelin, Martikainen, Pirkola and Koskinen14 Patient's address in January of each year was used to categorise their area of residence into quintiles of deprivation based on the income domain of the Northern Ireland Index of Multiple Deprivation (Quintile 1 most deprived, Quintile 5 least deprived), and into ‘urban’ (Northern Ireland's two largest cities Belfast and Derry), ‘intermediate’ (all other towns/villages) and ‘rural’ (population <1000 and open countryside) areas based on an official classification of settlements.Reference Maguire, French and O'Reilly15
Choice of primary outcome measure
The primary outcome of interest was receipt of psychotropic medication, interpreted here as a proxy indicator of mental health status. Prescription medication data have been used extensively in epidemiological studies exploring population mental health.Reference Maguire, French and O'Reilly15,Reference Gardarsdottir, Heerdink, van Dijk and Egberts16 Although some medications may be used for indications other than mental ill health, most indications for psychotropic medications are mental health related and it is anticipated that the degree of misclassification would be unaffected by the pandemic.Reference Gardarsdottir, Heerdink, van Dijk and Egberts16 Prescription information was retrieved from the centralised Enhanced Prescribing Database that holds information on all medications dispensed in community pharmacies nationwide. Data were extracted for all hypnotic, anxiolytic, antipsychotic and antidepressant medications (British National Formulary (BNF) 69 categories 4.1.1, 4.1.2, 4.2.1/2, 4.3 respectively) for each month over the 106-month study period.17 Anti-epileptic drugs (BNF 4.8) were used as a counterfactual comparator to aide differentiation between specific effects of the pandemic on psychotropic medication uptake rather than more generalised effects on medications uptake, such as arising from reduced access to practitioners.Reference Bernal, Cummins and Gasparrini18 It is hypothesised that the pandemic and associated restrictions should not affect epilepsy status but may be associated with mental health status. Prescribing data were linked to population data using the unique identifier (HCN).
Statistical analysis
Data pre-processing was performed in Stata and R Statistical analyses were performed using R packages including tidyverse and forecast.Reference Wickham, Averick, Bryan, Chang, D'Agostino McGowan and Francois19,Reference Hyndman and Khandakar20 Individuals were identified as being in receipt of medication if they were dispensed one or more prescriptions that month. They were grouped according to their medication use and descriptive statistics were used to explore patterns in demographic and socioeconomic characteristics across groups.
Pre-existing trends January 2012 to February 2020
The number of patients receiving prescriptions each month was calculated, and, using the monthly denominator, expressed as a percentage of the eligible population. Line graphs were generated to visualise trends over time for each medication, and stratified by gender, age, single-person household, rurality and deprivation quintile. Individuals with missing demographic or socioeconomic data were included in the analysis with a ‘missing’ category included for each variable as required.
Impact of restrictions on uptake of medications
In the absence of widely accepted guidelines for the reporting of time-series analyses, this paper adheres to the recommendations set out by Jandoc et al (2015).Reference Jandoc, Burden, Mamdani, Levesque and Cadarette21 Data for each medication type were separated into pre-restrictions (January 2012 to February 2020) and during restrictions (March 2020 to October 2020). A central problem with scanners used to record prescriptions meant that the recorded data on prescriptions dispensed in 2017 and 2018 were artificially lowered by approximately 10% compared with previous years. To circumvent this anomaly, models were trained on both the full data and with data from 2017–2018 removed.
The following models were trained separately for all medication types: (a) seasonal naïve model trained on first-differenced data (bench-mark), (b) exponential smoothing model trained on raw monthly frequency data, and (c) the auto regressive integrated moving average (ARIMA) model. The ARIMA model was trained on monthly frequency data using the auto.arima() function (detailed in Supplementary Table 1 available at https://doi.org/10.1192/bjp.2022.112).
The algorithm was permitted to iteratively attempt to fit on differenced data (to remove trend) and first seasonal difference (to remove seasonal trend) and automatically choose the best fit. A transfer function (i.e. shape of the impact after initial introduction of intervention) was not added to the ARIMA model as restrictions over the time period studied were subject to change. The performance of all three models were compared using root mean square error and Akaike information criterion (AIC), and visual inspection of the distribution residuals and errors. The distribution of residuals for models based on the full data demonstrated a right skew (Supplementary Table 1). However, models based on data with values in 2017/18 removed demonstrated a normal distribution and are presented here. On comparison between modelling approaches, ARIMA performed best and was therefore used to model medication uptake prior to March 2020 (detailed in Supplementary Table 1). Full analysis code available on github.
The trained models were then used to forecast medication uptake in the ‘during restrictions’ time frame. The expected (i.e. forecast) monthly values and upper and lower 80% and 95% confidence limits were extracted and plotted against actual monthly values. This allowed identification of actual monthly values that lie outside of the confidence limits for the expected values. Observed to expected ratios (and 95% confidence intervals) were also calculated.
This was repeated for each medication type and stratified by gender, age, single-person household, rurality and deprivation quintile. As the models comprised ‘counts of individuals dispensed prescriptions’ as opposed to monthly counts of ‘prescriptions’ individual-level sociodemographic variation could be explored. Data linkage was performed by the Business Services Organisation's Honest Broker Service (HBS) and data were de-identified and pseudonymised prior to release to the research team. Participant consent was not required for this study. The project was approved by the HBS Governance Board and received ethical approval from the NHS REC (20/YH/0254). The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Results
The study cohort consisted of 1 801 860 community dwelling individuals aged over 10 years, who were alive and resident in Norther Ireland at any month from January 2012 to October 2020 (ranging from 1 448 871 in January 2012 to 1 600 346 in October 2020). A summary of the demographic and socioeconomic characteristics for the cohort is presented in Table 1.
Table 1 Sociodemographic characteristics and number (%) of individuals within each subgroup in receipt of medications at any time January 2012 to October 2020
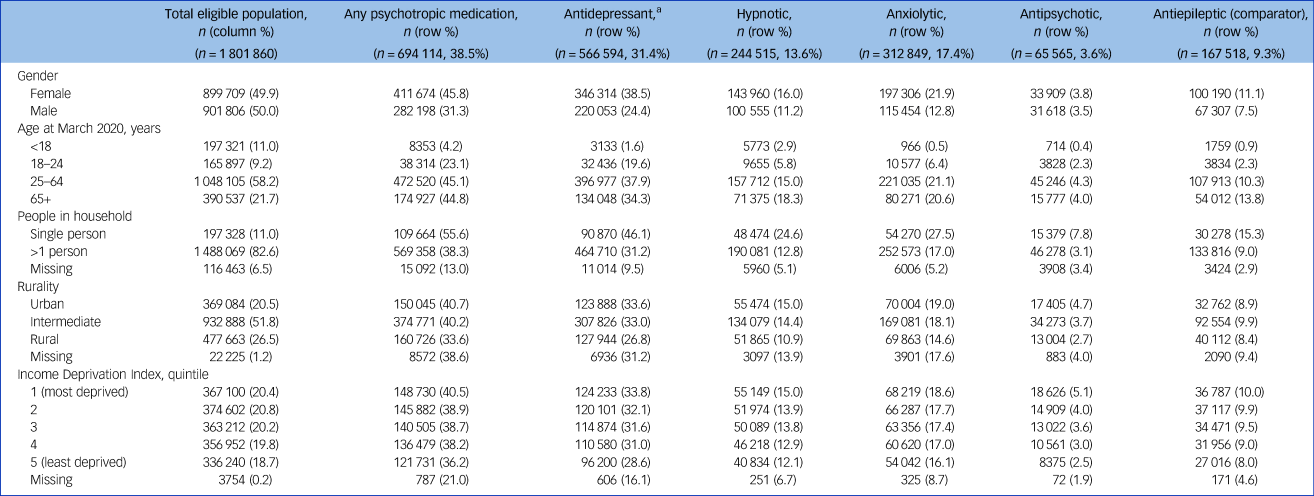
a. Individuals receiving any antidepressant (selective serotonin reuptake inhibitors or tricyclic antidepressants; monoamine oxidase inhibitors or other).
The percentage of individuals in this study cohort who were recorded as having been in receipt of psychotropic medication at any point across the study period was 38.5%: 31.4% for antidepressants, 13.6% for hypnotics, 17.4% for anxiolytics and 3.6% for antipsychotics. A higher proportion of females than males were in receipt of medications regardless of class, with over a third of females in Northern Ireland (38.5%) and almost a quarter of males (24.4%) in receipt of any antidepressant medication over the study period, and over 1 in 5 females (21.9%) and 1 in 8 males (12.8%) in receipt of anxiolytic medications.
Uptake of medication increased with age, with the peak usage for most psychotropic medications in the age group 25–64 years. The highest proportion of medication uptake was observed in urban areas, and over a half of individuals living in single-person households (55.6%) were in receipt of psychotropic medications compared with around a third for individuals who live with others (38.3%). Those living in urban areas and in the most deprived areas showed a greater percentage of medication uptake compared with those living in more rural and more affluent areas across all categories. Uptake of anti-epileptic medications followed similar patterns across these characteristics as that seen for psychotropic medications.
Trends January 2012 to October 2020
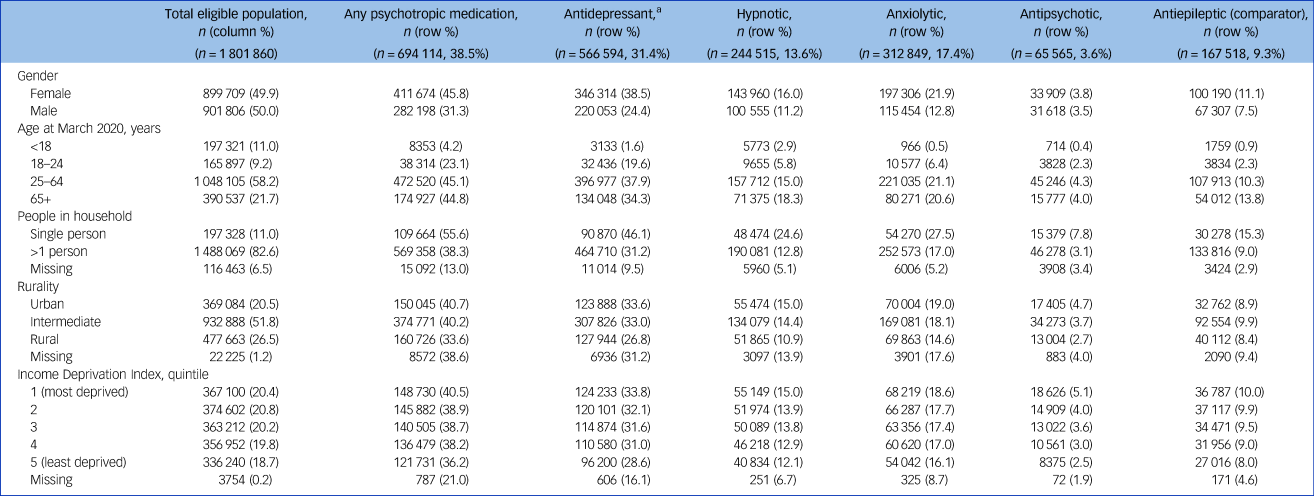
Uptake of psychotropic medications in Northern Ireland have been following a strong upward trend from January 2012 to October 2020, with steeper increases seen among those who live alone and those who live in urban or deprived areas (Fig. 1). The trend appears unaffected by the onset of the COVID-19 pandemic in March 2020. These same patterns are reflected in almost every medication subtype, with some variations (presented in Supplementary Figures 1–4). Anxiolytic medication is decreasing in those aged 65 years and over and hypnotic medication is decreasing across the entire population. The chosen comparator, anti-epileptic medications, followed similar trends to those of all psychotropic medications (Fig. 1), increasing over the study period for the full cohort (Supplementary Figure 5).

Fig. 1 Number of individuals in Northern Ireland in receipt of ‘any psychotropic’ medication each month from January 2012 to October 2020 by demographic factors (dashed vertical line depicts onset of pandemic March 2020/shaded areas 2017–2018 depict years affected by prescription scanning problem). (a) Full study cohort, (b) gender; (c) age in years; (d) household size; (e) deprivation; (f) rurality. F, female; M, male; Q, quartile.
Impact of the COVID-19 pandemic on uptake of medications
In March 2020 (when restrictions began), uptake of psychotropic medication increased beyond the confidence intervals of the ‘expected’ value in the ARIMA models, followed by a decrease in April, returning to the expected trend thereafter from May to October 2020 (Fig. 2). This is also true for antidepressant, anxiolytic and anti-epileptic medications. Antipsychotic medication uptake stayed within the expected limits throughout the entire study period. Hypnotic medication, however, was statistically significantly higher than the expected forecast values in 5 out of the 8 months follow-up (full observed/expected ratio values (95% CI) in Supplementary Table 2). Hypnotics include mostly ‘Z-drugs’ such as zaleplon, zolpidem and zopiclone; and melatonin; but also some benzodiazepines primarily indicated as hypnotics such as nitrazepam, flurazepam and temazepam.17

Fig. 2 Auto regressive integrated moving average (ARIMA) illustrating forecast versus actual values of uptake of all psychotropic medications during the first 8 months of the COVID-19 pandemic in Northern Ireland (March 2020 to October 2020). (a) all psychotropic medications, (b) antidepressants; (c) anxiolytics; (d) antipsychotics; (e) hypnotics; (f) anti-epileptics (comparator). Dark grey band denotes the 80% confidence interval and the light grey band the 95% confidence interval.
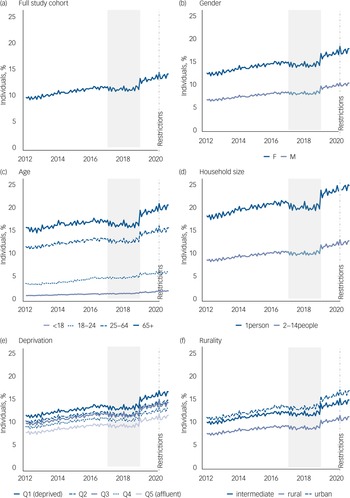
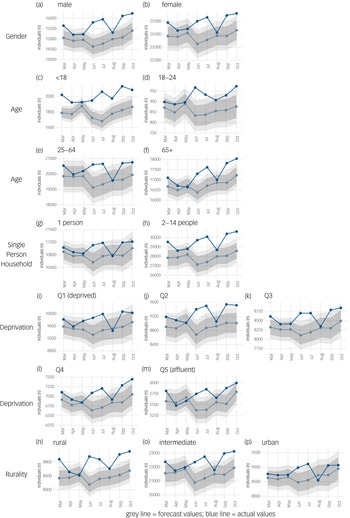
ARIMA models for trend were then trained by the range of demographic factors for each medication type separately. Fig. 3 shows the expected versus the observed uptake of antidepressant medications from March to October 2020 by gender, age, single-person household, area-level deprivation and rurality. Apart from the increase in the number of individuals in receipt of antidepressant medication observed in March 2020, medication uptake fell within the expected limits by gender, across deprivation quintiles and in urban and rural areas from April 2020 to October 2020. Slightly fewer than expected individuals under 18 years were in receipt of antidepressant medication for the first few months of the pandemic but uptake was as expected across all other age groups. Again, apart from the increase in the number of individuals in receipt of medication observed in March 2020, uptake mostly follows the expected trends across demographic subgroups for both anxiolytic medication and antipsychotic medication (Supplementary Figures 6 and 7). However, we do see statistically significantly higher than expected uptake of anxiolytic medication in those aged 65 years and over for 5 out of the 8 months of follow-up (Supplementary Figure 6), and higher than expected uptake of antipsychotic medication in the most affluent areas for 5 out of the 8 months of follow-up (Supplementary Figure 7). Although these border on significance, with the 95% CI almost crossing unity.

Fig. 3 Auto regressive integrated moving average (ARIMA) illustrating forecast versus actual values of uptake of all antidepressant medications during the first 8 months of the COVID-19 pandemic in Northern Ireland (March 2020 to October 2020). (a and b) gender; (c–f) age in years; (g and h) household size; (i–m) deprivation; (n to p) rurality. Dark grey band denotes the 80% confidence interval and the light grey band the 95% confidence interval. Q, quartile.
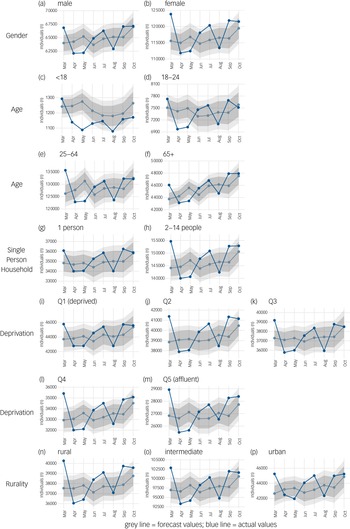
Overall hypnotic medication uptake was higher than expected in Fig. 2, and so Fig. 4 shows the expected versus the observed uptake of medications from March to October 2020 by gender, age, single-person household, area-level deprivation and rurality. Uptake of hypnotic medication was approximately 12% higher than expected in those aged under 18 years from March to October 2020 (Supplementary Table 3). Statistically significantly higher than expected uptake of hypnotic medication was observed consistently over all study months in individuals aged under 18 years, and also, for the majority of months, for males and individuals living in rural areas (see Fig. 4). Uptake was approximately 5% higher than expected in these groups (Supplementary Table 3).

Fig. 4 Auto regressive integrated moving average (ARIMA) illustrating forecast versus actual values of uptake of all hypnotic medications during the first 8 months of the COVID-19 pandemic in Northern Ireland (March 2020 to October 2020). (a and b) gender; (c–f) age in years; (g and h) household size; (i–m) deprivation; (n to p) rurality. Dark grey band denotes the 80% confidence interval and the light grey band the 95% confidence interval. Q, quartile.
Discussion
Main findings
The number of individuals in receipt of psychotropic medication during the first 8 months of the COVID-19 pandemic in Northern Ireland was generally within the expected range, as predicted from the trends in the 8 years prior to the pandemic. There was evidence suggestive of an initial ‘stockpiling’ of all medications in March 2020, with medication uptake returning to expected levels for most medications and most subgroups of the population from April 2020 through to October 2020. This initial ‘stockpiling’ phenomenon at the start of lockdown has been reported by other UK studies and is not unique to psychotropic medications as it was observed also in our counterfactual anti-epileptic medication.Reference Hayden and Parkin22
The COVID-19 pandemic, does not appear to have had a significant effect on the overall uptake of antidepressant, anxiolytic or psychotropic medications at a population level from March to October 2020. This is also largely true for population subgroups stratified by gender, age, household composition, area-level deprivation and rurality. The major exception was the uptake of hypnotic medication, which was significantly higher than expected in 5 out of the 8 months of follow-up. This increase was most significant among individuals aged <18 years, males and those living in rural areas.
Interpretation
The strong, upward, pre-existing trend observed in the uptake of psychotropic medications in Northern Ireland in the years preceding the pandemic is reflective of trends across the UK and globally.Reference Walker, Croker, Curtis, MacKenna and Goldacre11,Reference Ilyas and Moncrieff23
This study's finding that the COVID-19 pandemic and related restrictions have not had a significant impact on the uptake of antidepressant medication is in contrast with other findings based on English prescribing data by Armitage (2021), which demonstrated a 3.9% increase in the number of antidepressants prescribed in England from April to September 2020 compared with the same period in 2019.Reference Armitage10 However, as already highlighted by Walker et al (2021), Armitage's study did not take into consideration pre-COVID trends and was limited to data based on prescription item numbers not number of individuals in receipt of medication.Reference Walker, Croker, Curtis, MacKenna and Goldacre11
The absence of a change in levels of antidepressant medication uptake has two main interpretations. First, that the pandemic has had no effect on rates of depression in the population, despite expert projections. Or second, it could be argued that this reflects unmet need and that there has been a real increase in psychiatric morbidity but that this has been hidden by reduced access to care providers. There is some evidence of a decrease in emergency department presentations and psychiatric service interactions.24 Additionally, mental health referrals from primary care have reduced by 29% in the 12 months February 2020 to January 2021 compared with the same period in previous years in Northern Ireland.24 However, there is also evidence that access to health provision has not been affected as in this study medications such as hypnotics and anxiolytics did show increases, indicating that people in need were able to circumvent any difficulties in accessing services. What this study cannot ascertain is the impact of the pandemic on those already in receipt of antidepressant medication and the potential worsening of symptoms.
The most substantial increase in psychotropic medication uptake was observed among hypnotic medications, with more than expected young people, males and people living in rural areas in receipt of hypnotic medications during the first 8 months of the pandemic. Hypnotic medications are indicated for and prescribed for sleep disturbances but are rarely prescribed in children, except to aid sleep cycle synchronisation in children with sensory impairment, autistic spectrum disorder (ASD) and other neuropsychiatric/neurodevelopmental disorders including attention-deficit hyperactivity disorder (ADHD).17 A recent systematic review has suggested the COVID-19 pandemic has had a major effect on sleep quality, affecting an estimated 18% of the general population.Reference Alimoradi, Brostrom, Tsang, Griffiths, Haghayegh and Ohayon25 The fact that a significant increase in hypnotic medication was only observed among those aged <18 years in this study may be suggestive of greater sleep disturbance among children in the population with additional needs such as ASD or ADHD (which are also more commonly diagnosed in males), or reflective of the higher proportions of young people who, according to household surveys and parental reports, have reportedly demonstrated an increase in probable mental health conditions and an increase in behavioural problems during the pandemic.Reference Ford, John and Gunnell8 It is also feasible that those living in more rural areas were more prone to loneliness and isolation because of the introduction of restrictions.Reference Matthews, Danese, Caspi, Fisher, Goldman-Mellor and Kepa2
Anxiolytic medication increased among those aged 65 years and over. This is not unexpected given that older adults experience a disproportionately higher mortality rate from COVID-19 and may therefore experience greater anxiety around infection, and may also have experienced greater isolation and difficulty accessing support and services during lockdown. The observed increase in anxiolytic medication may be reflective of a tendency to prescribe medication to older people in need rather than prescribe alternate therapies. In Northern Ireland, this population are those most likely to have been affected by the trauma of the ‘Troubles’ and may have a history of anxiolytic use, especially benzodiazepine use, which may have been recommenced post introduction of COVID restrictions. Although most research to date has shown no significant impact of the pandemic on the mental health of older people, previous studies have been based on unrepresentative surveys and limited to the first few months of the pandemic.Reference Vahia, Jeste and Reynolds26 The longer-term effects are yet unknown.
Strengths and limitations
This study linked individual-level prescription data, for the whole population of Northern Ireland with other healthcare, mortality and area-level data-sets to allow for a more accurate examination of uptake of psychotropic medication during the first 8 months of the COVID-19 pandemic. The use of individual-level population and prescribing data provided the opportunity to establish accurate monthly uptake rates obviating the limitations associated with the use of population-volume data. The use of prescribing data as a proxy for mental ill health without information on indication is a recognised limitation, although we are reassured that the patterns of uptake of psychotropic medication conform to the known literature on the distribution of mental ill health within the population.Reference O'Connor, Wetherall, Cleare, McClelland, Melson and Niedzwiedz4,Reference Maguire, French and O'Reilly15,Reference Gardarsdottir, Heerdink, van Dijk and Egberts16
Using ARIMA modelling allowed this study to integrate long-term trends over the previous 8 years to forecast the expected trends for the time frame immediately after the onset of the COVID-19 pandemic. This greater adjustment for pre-existing trends enabled a clearer demonstration of the absence of an effect of COVID-19 on the uptake of most psychotropic medications. Applying ARIMA models to time-series healthcare data has the advantage of accounting for autocorrelation (or serial correlation), trends and seasonality that are known to exist in medication uptake.Reference Schaffer, Dobbins and Pearson27 The addition of the counterfactual comparator (anti-epileptic medication) adds to the robustness of the results illustrating the ‘stockpiling’ trend and return to ‘normal’ was observed outside of psychotropic medications but varied by sociodemographic factors only within psychotropic medications.
Implications
Results suggest an initial ‘stockpiling’ of medications in March 2020 with psychotropic medication uptake returning mostly to expected levels over the subsequent 7 months, with substantial increases only evident in hypnotic medication among children (age <18 years), males and those living in rural areas and increases in anxiolytic medications among older people (>65 years). The anticipated tsunami of mental ill health has not yet been manifest in significant changes in psychotropic medication uptake. There are indications that some groups of individuals have become more anxious or have had difficulties in sleeping, but these may be transient and may resolve as we emerge from the pandemic without need for psychiatric intervention. Data from this study only date to October 2020, so there is a need for more contemporaneous data and vigilance, as other sequelae from the pandemic such as financial strain or employment changes may be associated with increased mental ill health in the longer term. Exploring other population mental health indicators such as psychiatric hospital admissions, presentations with self-harm and death by suicide, in combination with psychotropic medication, over a longer period would provide a more holistic examination of the impact of the pandemic on mental ill health. However, the evidence to date based on psychotropic medication uptake suggests the pandemic has not been associated with a significant increase in psychopathology.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1192/bjp.2022.112
Data availability
The data used in this study cannot be publicly deposited. Project specific data-sets are created and destroyed in line with the Administrative Data Research Centre Northern Ireland Guidelines. Metadata for each project is available on request. Access to the data-sets used can be obtained through application to the Health and Social Care Northern Ireland Business Service Organisation's Honest Broker Service https://hscbusiness.hscni.net/services/2454.htm.
Acknowledgements
The authors would like to acknowledge the help provided by the staff of the Honest Broker Service (HBS) within the Business Services Organisation Northern Ireland (BSO). The HBS is funded by the BSO and the Department of Health, Social Services and Public Safety for Northern Ireland (DHSSPSNI). The authors alone are responsible for the interpretation of the data and any views or opinions presented are solely those of the author and do not necessarily represent those of the BSO.
Author contributions
Conceptualisation and data curation A.M. Preparation of manuscript A.M., L.K., D.O.’R. Data validation A.M. and L.K. Formal analysis L.K. and A.M. Review and editing A.M., L.K., D.O.’R., D.O.’H. and S.O.’N. Funding acquisition A.M. and D.O.’R. All authors had full access to the data and accept responsibility for this submission.
Funding
This work was supported by both the UKRI's ADRC-NI (ES/S00744X/1) and the Northern Ireland Public Health Agency's HSC RD (COM/5625/20).
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.