



Currently estimated to occur in 1 in 54 children in the United States (Maenner et al., Reference Maenner, Shaw, Baio, Washington, Patrick, Dirienzo and Dietz2020), autism spectrum disorder (ASD) is a lifelong neurodevelopmental condition characterized by challenges in social communication and restricted and repetitive behaviors that interfere with everyday life functioning (American Psychological Association, 2020). Children and adolescents with ASD also have an increased risk for emotional problems such as anxious and depressed affect (Bos, Diamantopoulou, Stockmann, Begeer, & Rieffe, Reference Bos, Diamantopoulou, Stockmann, Begeer and Rieffe2018; Centers for Disease Control and Prevention, 2019a) and behavior problems such as rule-breaking and disruptive behavior (Bauminger, Solomon, & Rogers, Reference Bauminger, Solomon and Rogers2010; Centers for Disease Control and Prevention, 2019b). It has been estimated that 70–90% of children and adolescents with ASD experience clinically significant emotional and behavioral problems (EBPs) (Bos et al., Reference Bos, Diamantopoulou, Stockmann, Begeer and Rieffe2018; Salazar et al., Reference Salazar, Baird, Chandler, Tseng, O'sullivan, Howlin and Simonoff2015; Simonoff et al., Reference Simonoff, Pickles, Charman, Chandler, Loucas and Baird2008).
Family is one of the most influential and enduring environmental psychosocial contexts in a youth's life and thereby thought to play a central role in shaping his/her emotional and behavioral development (Cummings, Davies, & Campbell, Reference Cummings, Davies and Campbell2000). Family system theories (e.g., Cox & Paley, Reference Cox and Paley1997) posit that youth actively shape, and in turn are shaped by, their family system in a transactional process. One aspect of the family environment shown to be intertwined with youth emotional and behavioral development across time in non-ASD samples is the parent couple relationship (i.e., marital or romantic partner relationship) and, in particular, parent couple conflict (PCC) defined as parents disagreeing or not seeing eye-to-eye on topics (e.g., Buehler et al., Reference Buehler, Anthony, Krishnakumar, Stone, Gerard and Pemberton1997; Davies & Cummings, Reference Davies and Cummings1994). The goal of the current study was to provide the first longitudinal examination of the bidirectional associations between PCC and EBPs of children and adolescents with ASD.
A growing body of research suggests that parents of children/adolescents with ASD are at risk for maladaptive couple outcomes, including lower marital satisfaction (Gau et al., Reference Gau, Chou, Chiang, Lee, Wong, Chou and Wu2012; Lee, Reference Lee2009), lower partner affection and support (Brobst, Clopton, & Hendrick, Reference Brobst, Clopton and Hendrick2009), and higher rates of separation/divorce (Berg, Shiu, Acharya, Stolbach, & Msall, Reference Berg, Shiu, Acharya, Stolbach and Msall2016; Hartley et al., Reference Hartley, Barker, Seltzer, Floyd, Greenberg, Orsmond and Bolt2010) than parents of children without developmental disabilities. However, the findings are mixed with one study showing a similar rate of separation/divorce in families of children with versus without ASD (Freedman, Kalb, Zablotsky, & Stuart, Reference Freedman, Kalb, Zablotsky and Stuart2012) and other studies reporting that some parents report feeling more connected to their partner because of shared parenting joys and challenges of raising a child with ASD (Hock, Timm, & Ramisch, Reference Hock, Timm and Ramisch2012). Researchers have speculated that the increased risk for maladaptive parent couple relationship outcomes reported by many parents of children with ASD may, in part, be driven by the high parenting stress reported by mothers and fathers of children and adolescents with ASD relative to their peers who have children and adolescents without ASD (Giovagnoli et al., Reference Giovagnoli, Postorino, Fatta, Sanges, De Peppo, Vassena and Mazzone2015). Within family systems theories (Cox & Paley, Reference Cox and Paley1997), the spillover hypothesis (Almeida, Wethington, & Chandler, Reference Almeida, Wethington and Chandler1999) asserts that parents transfer mood, feelings, and behaviors that originate in one family context (e.g., parenting) into other family subsystems (e.g., parent couple relationships) (Almeida et al., Reference Almeida, Wethington and Chandler1999; Kouros, Papp, Goeke-Morey, & Cummings, Reference Kouros, Papp, Goeke-Morey and Cummings2014). It is thus possible that parenting stress stemming from youth EBPs contributes to increased negative mood, fatigue, and negative interpersonal behaviors in the parent couple relationship in families of youth with ASD. In cross-sectional studies, a negative association between parent couple relationship quality and EBPs in youth with ASD has been reported (Brobst et al., Reference Brobst, Clopton and Hendrick2009; Robinson & Neece, Reference Robinson and Neece2014). Moreover, at a daily level, using data from the same sample reported on in the current study (Hartley et al., Reference Hartley, Papp, Mihaila, Bussanich, Goetz and Hickey2017), parents of youth with ASD reported a relatively lower number of daily positive couple interactions following a day with a higher level of parenting stress. Given these findings, it is possible that a high level of EBPs in youth with ASD leads to an increased level of PCC across time.
In a transactional process, it is also likely that PCC contributes to increased EBPs in children and adolescents with ASD. Within family systems theories, PCC is posited to lead to poor parent psychological wellbeing, which detracts from adaptive parenting (e.g., engaged, positive, and consistent parenting) (Gao, Du, Davies, & Cummings, Reference Gao, Du, Davies and Cummings2018; Kiecolt-Glaser & Wilson, Reference Kiecolt-Glaser and Wilson2017; McCoy, George, Cummings, & Davies, Reference McCoy, George, Cummings and Davies2013). Moreover, youth who are present for PCC have themselves been shown to feel anxious, upset, and emotionally insecure by these interactions (Cummings et al., Reference Cummings, Davies and Campbell2000). There is a large body of empirical research demonstrating the negative effects of PCC on youth emotional and behavioral development in non-ASD populations (e.g., Cummings, Cheung, Koss, & Davies, Reference Cummings, Cheung, Koss and Davies2014; Pendry, Carr, Papp, & Antles, Reference Pendry, Carr, Papp and Antles2013; Stutzman et al., Reference Stutzman, Bean, Miller, Day, Feinauer, Porter and Moore2011). For example, in school-age youth without ASD, destructive (e.g., hostile, disrespectful) PCC was found to predict later increases in youth emotional problems, including feelings of sadness or fear, and increases in behavior problems, such as aggressive and disruptive behaviors (e.g., Knopp et al., Reference Knopp, Rhoades, Allen, Parsons, Ritchie, Markman and Stanley2017; Pendry et al., Reference Pendry, Carr, Papp and Antles2013; Stutzman et al., Reference Stutzman, Bean, Miller, Day, Feinauer, Porter and Moore2011). In addition, in a general population sample, Papp (Reference Papp2012) found that mother-reports of a higher level of PCC were associated with a higher level of youth depressive symptoms across time, and this effect was strongest during early adolescence.
To date, there is no research examining the potential bidirectional pathways between PCC and youth EBPs in families of children and adolescents with ASD. However, there is growing longitudinal evidence of bidirectional associations between parent factors and child EBPs in families of youth with ASD and/or developmental delay (e.g., Baker et al., Reference Baker, McIntyre, Blacher, Crnic, Edelbrock and Low2003; Neece, Green, & Baker, Reference Neece, Green and Baker2012; Woodman, Mawdsley, & Hauser-Cram, Reference Woodman, Mawdsley and Hauser-Cram2015; Zaidman-Zait et al., Reference Zaidman-Zait, Mirenda, Duku, Szatmari, Georgiades and Volden2014), including in the sample reported on in the current study (Rodriguez, Hartley, & Bolt, Reference Rodriguez, Hartley and Bolt2019). For example, Baker et al. (Reference Baker, McIntyre, Blacher, Crnic, Edelbrock and Low2003) found a bidirectional association between child EBPs and self-reported parenting stress in families of young children with development disabilities, while Zaidman-Zait et al. (Reference Zaidman-Zait, Mirenda, Duku, Szatmari, Georgiades and Volden2014) reported bidirectional associations between self-reported parenting distress and both internalizing and externalizing behavior problems in children with ASD. Given reports of heightened PCC (Hartley et al., Reference Hartley, Papp, Mihaila, Bussanich, Goetz and Hickey2017) and elevated youth EBPs (e.g., Bos et al., Reference Bos, Diamantopoulou, Stockmann, Begeer and Rieffe2018), understanding the directional longitudinal pathways between PCC and youth EBPs is particularly relevant for families of youth with ASD. Elucidating these pathways can drive family-wide interventions to both support parent couple relationships and reduce the EBPs of youth with ASD.
Although less studied, there is evidence of parent gender differences in spillover between the couple and parenting domains. In what has been termed the father vulnerability hypothesis (Cummings, Merrilees, & George, Reference Cummings, Merrilees, George and Lamb2010), in general population samples, fathers have been found to have greater difficulty than mothers containing negative emotions generated in the couple domain from spilling into parenting (e.g., Belsky, Youngblade, Rovine, & Volling, Reference Belsky, Youngblade, Rovine and Volling1991; Davies, Sturge-Apple, Woitach, & Cummings, Reference Davies, Sturge-Apple, Woitach and Cummings2009; Kouros et al., Reference Kouros, Papp, Goeke-Morey and Cummings2014; Stroud, Meyers, Wilson, & Durbin, Reference Stroud, Meyers, Wilson and Durbin2015). For example, in a daily diary study using a general population sample, Kouros et al. (Reference Kouros, Papp, Goeke-Morey and Cummings2014) found longer-lasting spillover between marital and parent–child quality in fathers than in mothers, and this spillover was particularly strong if the fathers were also experiencing other stressors. Less is known about potential parent gender differences in the opposite direction of spillover – in other words, research to date has not assessed whether fathers are also more prone than mothers to having stressful parenting spill over into the couple domain.
Current Study
The goal of the current study was to examine the bidirectional associations between PCC and youth EBPs in a sample of 188 families of youth with ASD (originally aged 5–12 years), drawing on four time points of data collection, each spaced 12 months apart. Both mother-reports and father-reports of PCC and of youth EBPs were collected at each time point. Guided by family systems theories (Cox & Paley, Reference Cox and Paley1997, Reference Cox and Paley2003; Cummings et al., Reference Cummings, Davies and Campbell2000) and based on previous research on general population samples (e.g., Brobst et al., Reference Brobst, Clopton and Hendrick2009; Giovagnoli et al., Reference Giovagnoli, Postorino, Fatta, Sanges, De Peppo, Vassena and Mazzone2015; Knopp et al., Reference Knopp, Rhoades, Allen, Parsons, Ritchie, Markman and Stanley2017), we hypothesized a bidirectional relation between PCC and the EBPs of youth with ASD. Specifically, we hypothesized a higher level of youth EBPs would predict increased PCC 12 months later and, in the opposite direction, a higher level of PCC would predict increased youth EBPs 12 months later. Based on evidence supporting the father vulnerability hypothesis (Cummings et al., Reference Cummings, Merrilees, George and Lamb2010), PCC was predicted to have more robust associations with youth EBPs 12 months later in fathers than mothers.
Method
Participants
The participants were part of an ongoing longitudinal study examining family outcomes in relation to ASD. At the time of recruitment, couples had a child with ASD aged 5–12 years. Of the sample, 14 parent couples had more than one child with ASD; in these families, the eldest child with ASD was selected as the target child (i.e., the focus of study) to capture when parenting a child with ASD began. The inclusion criteria included the following: (a) the child had a documented medical or educational diagnosis of ASD and the diagnostic evaluation included the Autism Diagnostic Observation Schedule, second edition (Lord et al., Reference Lord, Rutter, DiLavore, Risi, Gotham and Bishop2012); (b) the parents were aged 21 years or older; (c) the parents had been in a committed cohabiting couple relationship for at least 3 years; (d) both parents in the couple agreed to participate. Recruitment occurred through fliers posted in community locations (e.g., grocery stores), research registries, and fliers mailed to schools and ASD clinics. In total, 188 couples who had a child with ASD enrolled in the study between 2013 and 2014. Parents completed the Social Responsiveness Scale (SRS-2) (Constantino & Gruber, Reference Constantino and Gruber2012) in order to assess the target child's current ASD symptom severity. Five children with ASD received an SRS-2 total t score below or equal to 60; however, after reviewing all information (e.g., medical or educational records, Autism Diagnostic Observation Schedule, and teacher-reported SRS-2), these children were included in analyses as they were deemed to meet ASD criteria. Of the parents, 15 (8%) parent couples included one biological parent and one step parent, 5 (3%) included two adoptive parents, and 13 (7%) were not married.
The present study examined data from four time points (T1, T2, T3, T4), each spaced approximately 12 months apart (M = 11.66, SD = 3.70). At T1, the child with ASD had an average age of 7.90 years (SD = 2.25) and most (86%) were male. Child ethnic/racial categories comprised White, non-Hispanic (83%), Latino (7%), Asian (4%), Black (3%), Native American (0.5%), and multiple racial/ethnic groups (3%). Approximately one third (34%) of children with ASD had intellectual disability (ID). Mothers and fathers had an average age of 38.69 years (SD = 5.62) and 40.76 years (SD = 6.19), respectively, and 69% had at least an Associate's degree. Parents had been in their current couple relationship for an average of 14.55 years (SD = 5.59). Based on the Couples Satisfaction Index (Funk & Rogge, Reference Funk and Rogge2007), 41% of mothers and 35% of fathers scored less than 104.5, placing them in the couple relationship distressed range.
Procedure
The study was approved by the Institutional Review Board at the University of Wisconsin-Madison. At each time point, mothers and fathers jointly reported on the family sociodemographics and then independently completed questionnaires about PCC and the EBPs of the youth with ASD. Parents were each paid $50 for this portion of the study at each time point.
Measures
Family sociodemographics
Family sociodemographics were reported on by parents or obtained via medical or educational records. Youth age was coded in years. Youth ID status was coded as 0 = no ID or 1 = ID, assessed via medical or educational records and based on the presence of a diagnosis of ID and/or IQ and adaptive behavior testing indicating that the child met criteria for ID. Parent education was coded from 1 = less than high school to 10 = doctoral or law degree. Parent couple relationship length was coded in years, based on when the partners started dating.
Parent couple conflict (PCC)
The Couple Conflict and Problem-Solving Scale (CCPSS) (Kerig, Reference Kerig1996) is a self-reported measure of couple conflicts. The frequency score is the number of times parents experience minor conflicts (scored as 1 = once a year to 6 = just about every day) or major conflicts (scored as 2 = once a year to 12 = just about every day). The scores for minor and major conflicts are then summed, giving a possible total score range from 3 to 18. The severity subscale is composed of 22 items, each rated to reflect the degree in which partners disagree about various topics (possible range from 0–100 per item). The frequency × severity total was used in the present study. The CCPSS has been shown to be reliable and valid in general population samples (Kerig, Reference Kerig1996). In the current sample, the severity score had good internal consistency across all time points in mothers (Cronbach's α = .86 to .89) and fathers (Cronbach's α = .89 to .90). The frequency score had acceptable internal consistency across time in mothers (Cronbach's α = .62 to .79) and fathers (Cronbach's α = .67 to .82). The means and standard deviations for mother- and father-reported couple conflict frequency and severity across the four time points are listed in Table 1.
Table 1. Mother- and father-reported means (M) and standard deviations (SD) for main variables
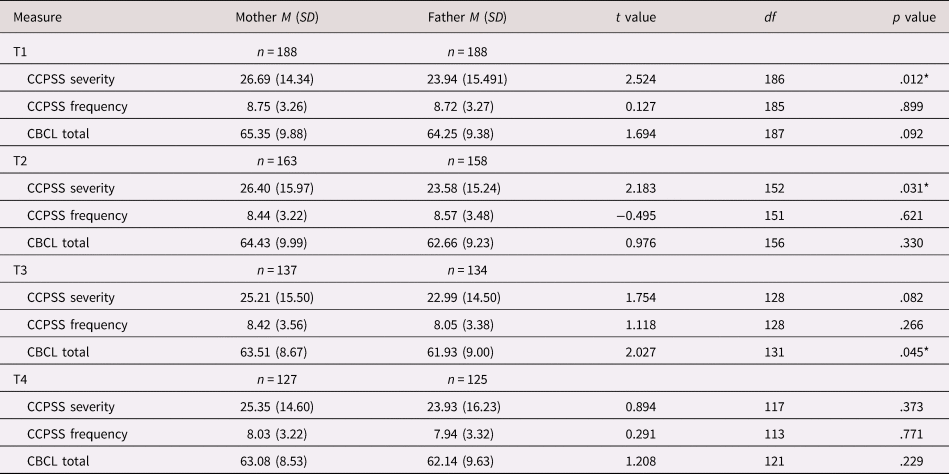
Note: t value = value for paired-samples t test; df = degrees of freedom; CCPSS = Couple Conflict and Problem-Solving Scale (Kerig, Reference Kerig1996); CBCL total = Child Behavior Checklist total t score (Achenbach & Rescorla, Reference Achenbach and Rescorla2001); *p < .05
Youth emotional and behavioral problems (EBPs)
Youth EBPs were assessed using the Child Behavior Checklist (CBCL) for ages 1.5–5 years (preschool form) and ages 6–18 years (school-age form) (Achenbach & Rescorla, Reference Achenbach and Rescorla2000, Reference Achenbach and Rescorla2001). The CBCL consists of 113 items that are summed into a total problems score, which was used in the present study. The total problem score encompasses eight syndrome scales: anxious/depressed, withdrawn/depressed, somatic complaints, social problems, thought problems, attention problems, rule-breaking behavior, and aggressive behavior. The current study focused on the total problems t score but also used the internalizing and externalizing t scores in follow-up analyses. The CBCL has strong reliability and good concurrent validity in the ASD population (Pandolfi, Magyar, & Norris, Reference Pandolfi, Magyar and Norris2014). In the current sample, the CBCL total problems t score had a high internal consistency across time in mothers (Cronbach's α = .94) and fathers (Cronbach's α = .94 to .95). This was also true for the internalizing scale (mothers, Cronbach's α = .84 to .85; fathers, Cronbach's α = .82 to .85) and externalizing scale (mothers, Cronbach's α = .89 to.90; fathers, Cronbach's α = .88 to .89) across time.
Data analysis plan
Descriptive statistics and boxplots were used to examine the distribution of study variables. Pearson correlations between PCC and youth EBPs were examined. In addition, Pearson correlations examining the association between sociodemographic variables (youth age, youth ID status, parent education, and parent couple relationship length) and the main variables of interest (i.e., PCC and youth EBPs) were also conducted to determine relevant covariates to include in subsequent models.
A cross-lagged panel model (CLPM), using maximum likelihood parameter estimators, was conducted in structural equation modeling (SEM) to examine the bidirectional effects between PCC and youth EBPs (CBCL total score). Analyses were conducted using Mplus7 statistical software (Muthén & Muthén, Reference Muthén and Muthén2012). To account for missing data, the full information maximum likelihood method was used (Little, Reference Little2013). Research indicates that this method is a robust estimator in SEM and typically a better estimation method compared with other deletion or imputation methods (Schlomer, Bauman, & Card, Reference Schlomer, Bauman and Card2010). CLPMs are useful when examining longitudinal data because they test directional associations across various time points simultaneously in both directions (Kearney, Reference Kearney and Allen2016). The CLPM also estimates and controls for the stability of variables across time. Additional lagged paths between T1 and T3, as well as between T2 and T4, were added for stability. In a multi-group model, mothers and fathers were entered as a dichotomous grouping variable (e.g., mothers = 0, fathers = 1). PCC and youth EBPs were entered as continuous variables. The root mean squared error of approximation (RMSEA), comparative fit index (CFI), and the Tucker–Lewis index (TLI) were examined in addition to the chi-square (χ2) statistic in order to assess model fit in line with recommendations (Little, Reference Little2013). A small χ2, TLI and CFI scores greater than .90, and RMSEA values between .05 and 08 are considered to represent good model fit (Hu & Bentler, Reference Hu and Bentler1999; Little, Reference Little2013). Figure 1 shows a conceptual model.
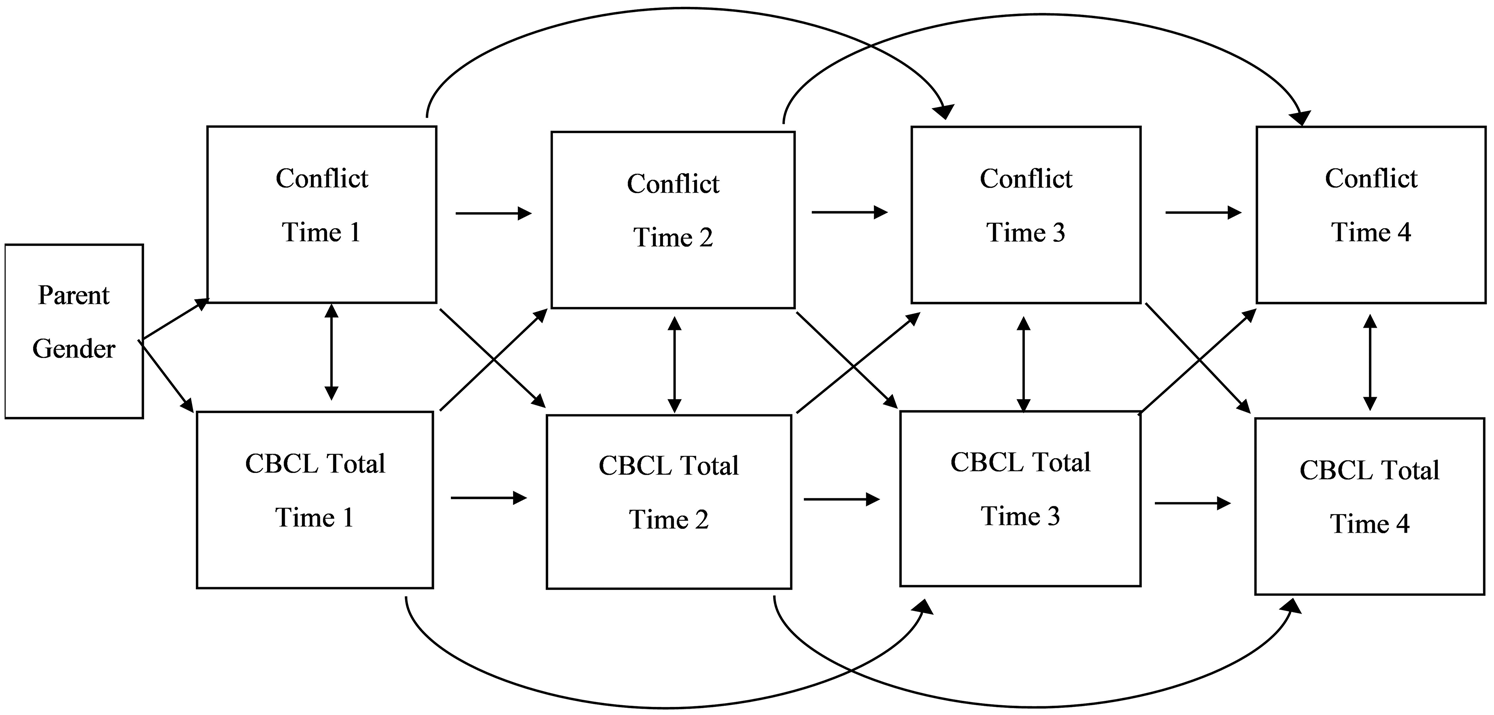
Figure 1. Hypothesized conceptual model representing the bidirectional effects between couple conflict and youth emotional and behavioral problems in families of youth with ASD.
Follow-up exploratory CLPMs were analyzed to examine youth internalizing (CBCL internalizing t score) and externalizing (CBCL externalizing t score) problems separately. In addition, exploratory cross-reporter models were ran to examine the associations between mother-report of PCC and father-report of youth EBPs and vice versa. Like the original model described above, these follow-up models also controlled for parent education, parent couple relationship length, youth age, and youth ID status.
Results
Preliminary analyses
The main study variables (CBCL and CCPSS) had a normal distribution without skew (kurtosis range = −.660 to .145 for CBCL, −.275 to .905 for conflict severity, and −.723 to −.284 for conflict frequency). Missing completely at random tests revealed that data were missing at random on the main study variables (χ2 = 21.19–27.76, p values > .05). Of the 188 families who completed at T1, 61 did not complete one or more of the subsequent time points (completion: T1 = 188; T2 = 163; T3 = 137; T4 = 127). The reasons for study attrition included being too busy, not being able to be reached, and no longer interested in participating. Attrition analyses were conducted to test whether the families who completed all time points differed from those who did not regarding the main study variables. Participants who had missing data on one or more time points for either of the main variables were coded as incomplete. Independent t tests indicated no significant differences between these groups in PCC severity (mother, t (187) = −1.346, p = .180; father, t (185) = −0.990, p = .324), conflict frequency (mother, t (185) = −1.025, p = .307; father, t (184) = −0.467, p = .641), or in youth EBPs (mother, t (185) = −0.504, p = .615; father, t (185) = 0.104, p = .918). Additional independent t tests were run to compare sociodemographic variables (parent age, parent ethnicity, parent education, parent relationship length, and parent couple satisfaction) between those who completed the study at all four time points and those who did not. There were no significant differences between the two groups.
Table 1 shows the means and standard deviations for PCC and youth EBPs (CBCL total score) across the four time points, as well as paired sample t values examining within-couple differences between mother-reports and father-reports. Associations between mother- and father-reports of PCC and youth EBPs across time were small to moderate (r = .33 to .58). Table 2 presents the associations between sociodemographic variables (youth age, youth ID status, parent education, and parent couple relationship length) and the main study variables of interest (PCC and youth EBPs). Pearson correlations for mother-reports indicated a significant negative association between youth age and severity of PCC at T1 (r = −.153, p = .035) and T3 (r = −.204, p = .018). In terms of father-reports, youth age was not significantly correlated with the severity or frequency of PCC or youth EBPs. The presence of youth ID status was significantly positively correlated with mother-report of severity of PCC at T3 (r = .178, p = .039), mother-report of conflict frequency at T1 (r = .210, p = .004), T3 (r = .287, p = .001), and T4 (r = .264, p = .004), and mother-report of youth EBPs at T1 (r = .163, p = .026) and T3 (r = .173, p = .043). In addition, youth ID status was significantly positively correlated with father-report of couple conflict frequency at T4 (r = .186, p = .047) and youth EBPs at T1 (r = .183, p = .012), T2 (r = .186, p = .019), and T4 (r = .201, p = .025). Parent relationship length was significantly positively associated with mother-report of youth EBPs at T1 (r = .165, p = .024). Parent couple relationship length was not significantly associated with father-reports of PCC or youth EBPs. Parent education was significantly positively associated with mother-report of PCC severity at T3 (r = .276, p = .001) and conflict frequency at T1 (r = .158, p = .030) and T3 (r = .258, p = .003), but was not significantly associated with father-reports. Given the significant correlations between youth age, youth ID, parent education, and parent couple relationship length and the main study variables, these four sociodemographic variables were controlled for in the CLPM. Specifically, we regressed PCC and scores of youth EBPs on these sociodemographic variables (i.e., parent education, parent couple relationship length, youth age, and youth ID status) at each time point. The resulting unstandardized residual scores were then saved and entered into the CLPM to account for the influence of these variables across time points.
Table 2. Pearson correlations among study variables for mothers (shaded and above the diagonal) and fathers (unshaded and below the diagonal)
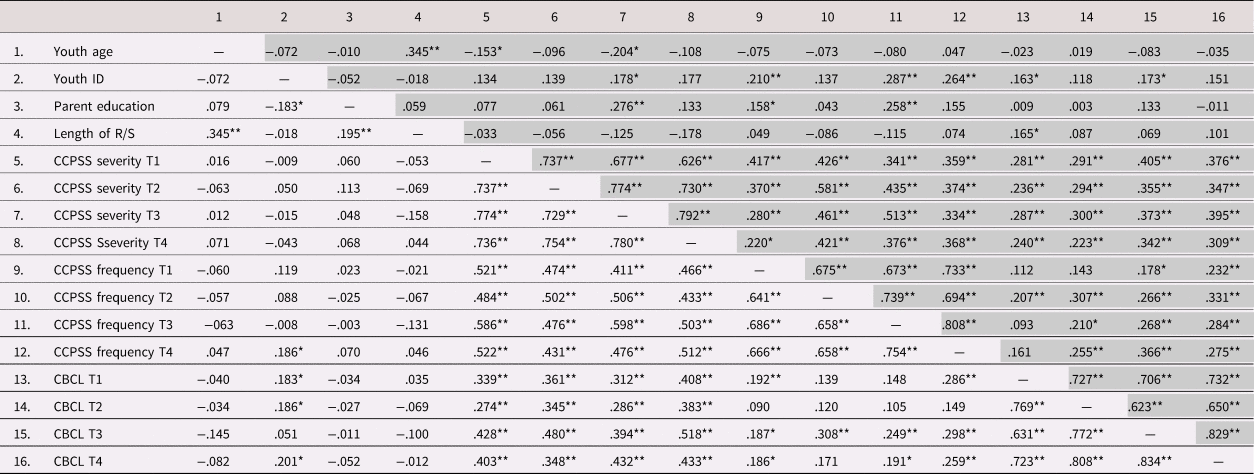
Note: Length of R/S = parent couple relationship length; CBCL = Child Behavior Checklist total t score; *p < .05, **p < .01.
Cross-lagged panel model (CLPM)
Path coefficients for the CLPM are displayed in Table 3. The model indicated good fit (χ2 (16) = 34.050, p = .005; TLI = .961; CFI = .988; RMSEA = .078). The cross-lagged panel analysis for mother-reported youth EBPs and PCC revealed stability effects in variables across time points (EBPs, T1→T2: β = .713, p = .000; T2→T3: β = .228, p = .006; T3→T4: β = .694, p = .000; PCC, T1→T2: β = .694, p = .000; T2→T3: β = .646, p = .000; T3→T4: β = .506, p = .000). Across the time points, there were also stability effects in the model of father-reported youth EBPs (T1→T2: β = .412, p = .000; T2→T3: β = .749, p = .000; T3→T4: β = .829, p = .000) as well as PCC (T1→T2: β = .791, p = .000; T2→T3: β = .247, p = .026; T3→T4: β = .664, p = .000). Equality constraints were also tested for each direction of effects, and differences between mothers and fathers were significantly different (youth EBPs → PCC: χ2 = 18.03, df = 5, p < .05; PCC → youth EBPs: χ2 = 22.40, df = 5, p < .05).
Table 3. Path coefficients and standard errors (SE) for mother- and father-reports of parent couple conflict and youth emotional and behavioral problems
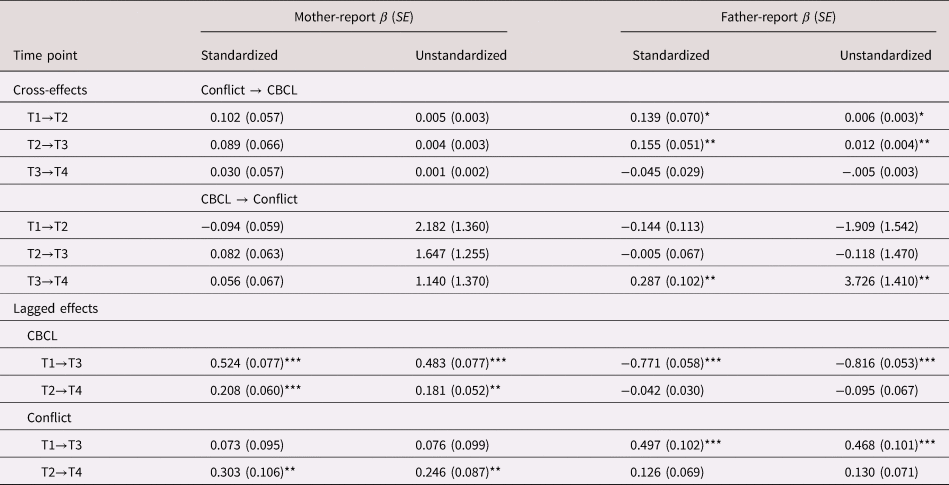
Note. *p < .05; **p < .01; ***p < .001. CBCL = Child Behavior Checklist (Achenbach & Rescorla, Reference Achenbach and Rescorla2001).
After controlling for youth age, youth ID, parent education, and parent couple relationship length, father-report of PCC at T1 significantly predicted increased youth EBPs at T2 (β = .139, p = .046), and PCC at T2 significantly predicted youth EBPs at T3 (β = .155, p = .002). Moreover, father-report of youth EBPs at T3 significantly predicted increased PCC at T4 (β = .287, p = .005). Mother-reports did not reveal significant cross-lagged effects. Figures 2a and 2b display the significant pathways in the CLPM for mothers and fathers, respectively.
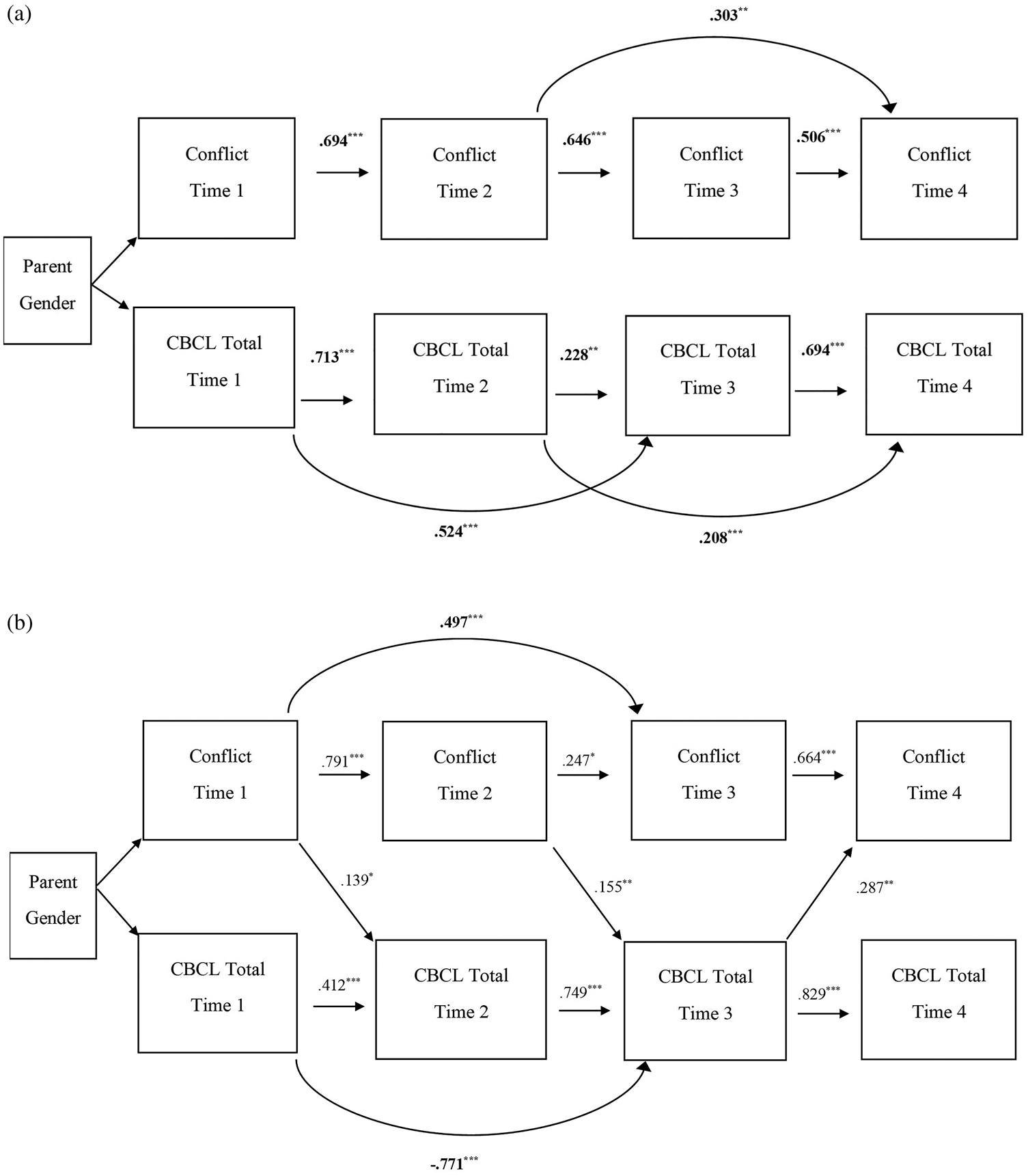
Figure 2. (a) Results of cross-lagged panel model (CLPM) for mother-report of parent couple conflict (PCC) (severity × frequency) and youth emotional and behavioral problems (EBPs). Only significant paths are shown. Values are standardized path estimates. *p < .05, **p < .01, ***p < .001. (b) Results of the CLPM for father-report of PCC (severity × frequency) and youth EBPs. Only significant paths are shown. Values are standardized path estimates. *p < .05, **p < .01, ***p < .001.
Follow-up analyses were conducted using the above described CLPMs, but instead of CBCL total t scores we examined internalizing (CBCL internalizing t score) and externalizing (CBCL externalizing t score) problems separately. Similar to the original model, no mother effects were found. In the internalizing problem model (model fit: χ2 (16) = 44.865, p = .0001; TLI = .926; CFI = .978; RMSEA = .098), father-report of PCC at T1 predicted youth internalizing behavior problems at T2 (β = .163, p = .024). In the opposite direction, father-report of youth internalizing behavior problems at T3 predicted PCC at T4 (β = .256, p = .037). Results for the externalizing model (model fit: χ2 (16) = 58.123, p = .0000; TLI = .909; CFI = .973; RMSEA = .119) indicated that father-report of PCC at T2 predicted youth externalizing behavior problems at T3 (β = .117, p = .030) and, in the other direction, father-report of youth externalizing behavior problems at T3 predicted PCC at T4 (β = .231, p = .010). Finally, we also conducted follow-up exploratory analyses to examine the original models described above but using cross-reporter scores of youth behavioral and emotional problems (CBCL total t score). In one model (model fit: χ2 (8) = 24.333, p = .002; TLI = .922; CFI = .977; RMSEA = .104), mother-reported PCC at T2 predicted father-reported youth EBPs at T3 (β = .126, p = .031) but there were no other significant pathways. In the second model (model fit: χ2 (8) = 16.672, p = .0337; TLI = .965; CFI = .990; RMSEA = .076), mother-reported youth EBPs at T3 predicted father-reported PCC at T4 (β = .131, p = .023).
Discussion
Youth with ASD are at elevated risk for EBPs, with an estimated 70–90% having clinically significant EBPs (Salazar et al., Reference Salazar, Baird, Chandler, Tseng, O'sullivan, Howlin and Simonoff2015; Simonoff et al., Reference Simonoff, Pickles, Charman, Chandler, Loucas and Baird2008). One domain of the family environment shown to have important associations with youth emotional and behavioral development in non-ASD populations is the parent couple relationship, and specifically couple conflict (Buehler et al., Reference Buehler, Anthony, Krishnakumar, Stone, Gerard and Pemberton1997; Davies & Cummings, Reference Davies and Cummings1994). To our knowledge, the current study is the first longitudinal examination of the bidirectional associations between PCC and youth EBPs in families of children and adolescents with ASD.
In one direction, our findings highlight that PCC may influence the emotional and behavioral functioning of youth with ASD. Specifically, from T1 to T2 and T2 to T3, higher levels of father-reported PCC predicted increased EBPs 12 months later in the child or adolescent with ASD. A similar pathway of effects has been reported for youth without neurodevelopmental disabilities (Cummings et al., Reference Cummings, Cheung, Koss and Davies2014; Davies & Cummings, Reference Davies and Cummings1994; Stutzman et al., Reference Stutzman, Bean, Miller, Day, Feinauer, Porter and Moore2011), highlighting that the family environment remains an important and potentially modifiable factor that affects youth behaviors in the presence of ASD. It is also possible that PCC leads to poor parent psychological wellbeing (Kiecolt-Glaser & Wilson, Reference Kiecolt-Glaser and Wilson2017), which reduces effective parenting (e.g., warmth, responsiveness, and consistency) (Gao et al., Reference Gao, Du, Davies and Cummings2018; McCoy et al., Reference McCoy, George, Cummings and Davies2013) and thereby contributes to EBPs in children and adolescents with ASD (Hickey, Bolt, Rodriguez, & Hartley, Reference Hickey, Bolt, Rodriguez and Hartley2020). Within family system theories, the emotional security theory may highlight an alternative explanation for the direction of these effects. This theory posits that exposure to chronic PCC reduces children's and adolescents’ sense of emotional security (i.e., confidence that parents will be available in times of need) (Davies & Cummings, Reference Davies and Cummings1994), in turn hindering the development of emotion regulation skills and leading to increases in EBPs such as depressed and anxious mood (Davies, Martin, Sturge-Apple, Ripple, & Cicchetti, Reference Davies, Martin, Sturge-Apple, Ripple and Cicchetti2016). The cumulative effects of unresponsive and unpredictable parenting behaviors may increase youths’ emotional distress and ability to regulate challenging behaviors in the presence of parental conflict. Future research is needed to explore the mechanism through which the couple relationship exerts effects on youth with ASD.
In the other direction, from T3 to T4, the EBPs of youth with ASD predicted increased PCC 12 months later for father-reported measures. Previous research on parents of youth with ASD found that comorbid EBPs accounted for greater variability in parenting stress than the youth's ID status or ASD symptoms (Lecavalier, Leone, & Wiltz, Reference Lecavalier, Leone and Wiltz2006). Thus, the stress generated from EBPs evidenced by youth with ASD may be a critical pathway of spillover from the parenting domain into the parent couple domain in the context of ASD.
The current study revealed cross-effects for associations between father-reported PCC and youth EBPs, but a similar pattern was not found for mother-reports. The father vulnerability hypothesis (Cummings et al., Reference Cummings, Merrilees, George and Lamb2010) may explain these parent gender differences. This hypothesis posits that fathers have more difficulty than mothers containing stress generated within one domain (e.g., couple disagreement) from spilling over into other domains (e.g., negative parent–child interaction). Previous studies on a general population sample found that fathers evidenced greater stress from the couple domain to the parenting domain than mothers (e.g., Belsky et al., Reference Belsky, Youngblade, Rovine and Volling1991; Davies et al., Reference Davies, Sturge-Apple, Woitach and Cummings2009; Kouros et al., Reference Kouros, Papp, Goeke-Morey and Cummings2014; Stroud et al., Reference Stroud, Meyers, Wilson and Durbin2015). This spillover of stress and negative emotions and behaviors from the parent couple domain may negatively influence fathers’ parent–child interactions in ways that increase the EBPs of the son/daughter with ASD. In the other direction, we also found that father-report, but not mother-report, of youth EBPs predicted increased PCC. Thus, in both directions, fathers may be less able than mothers to compartmentalize stress within the couple or parenting domain to avoid spillover.
It is also not clear why youth EBPs predicted increased father-reported PCC from T3 to T4 but not at earlier time points. It is possible that a child's EBPs become more taxing and/or spillover of stress from these interactions is more common for fathers as the child with ASD grows older. In part, this could be because the presentation of problems shifts with age (e.g., Harrop et al., Reference Harrop, McConachie, Emsley, Leadbitter, Green and Consortium2014; McCauley, Elias, & Lord, Reference McCauley, Elias and Lord2020) and may be more difficult to manage. Moreover, there is evidence that the EBPs of youth with ASD are experienced more negatively and perceived as more discouraging across time by fathers, as they are viewed as being more atypical, permanent, and more difficult to treat (e.g., Rivard, Terroux, Parent-Boursier, & Mercier, Reference Rivard, Terroux, Parent-Boursier and Mercier2014) as the child grows older. As a result, negative emotions generated from youth EBPs may be more likely to spill over into the parent couple relationship and create opportunities for couple conflict as the son/daughter ages. It is important to note that the current study included a relatively wide age range of youth with ASD at T1 (aged 5–12 years). Thus, it is not clear if these changes are due to time or are related to specific developmental periods (e.g., entry into or through adolescence). Future research should thus explore whether there are developmental periods of heightened risk and susceptibility for effects. It is also possible that fathers themselves have more difficulty preventing parenting stress from contributing to PCC across time. In other words, fathers’ ability to cope with and/or compartmentalize stress within a domain may worsen across time. This possibility should also be examined in future studies.
We ran follow-up exploratory analyses to begin to understand if the bidirectional links between PCC had unique associations with youth internalizing versus externalizing problems. The findings indicated that youth internalizing (T3) positively predicted father-reported couple conflict 12 months later. In the other direction, higher father-reported couple conflict at T1 and T2 predicted higher youth internalizing and externalizing behavior problems 12 months later. Thus, in fathers, the spillover effects of high couple conflict appear to contribute to both internalizing (e.g., anxious and depressed affect) and externalizing (e.g., disruptive behaviors and aggression) problems in youth with ASD. In contrast, for fathers, youth internalizing problems (more so than externalizing behavior problems) may play a particularly salient role in leading to increased couple conflict, and this may be most true as the youth with ASD grows older and internalizing behavior problems often become more prominent (e.g., Boya, Bos, Stockmann, & Rieffe, Reference Boya, Bos, Stockmann and Rieffe2020).
Study Strengths, Limitations, and Future Directions
The present study has both strengths and limitations. In terms of strengths, bidirectional pathways of effects between PCC and EBPs in children and adolescents with ASD were examined in a model that controlled for relevant youth and family sociodemographics. In addition, the model included both mother-reported and father-reported measures, allowing us to capture family processes and mental health processes from multiple perspectives and explore unique effects for mothers and fathers.
In terms of limitations, our sample size was modest for SEM and predominately consisted of White, non-Hispanic parents. Future research is needed to determine if the pattern of findings is replicated in larger and more diverse samples. It should be noted that families with missing data did not differ significantly at T1 from those with complete data; however, it is possible that these families could have differed in characteristics that were not assessed (e.g., parenting stress). The present study relied on parent-reported measures of couple conflict and youth EBPs. We focused on associations from a single reporter because it was thought to better capture PCC (e.g., parents may perceive disagreement severity differently) and youth EBPs as experienced by that parent (e.g., youth may behave differently with different parents). However, this approach could have inflated associations. To reduce these concerns, we conducted a follow-up exploratory analysis using cross-reporter measures (e.g., father-report of PCC predicting mother-report of youth EBPs 12 months later and vice versa). The overall pattern of associations remained, with the exception of the pathway from father-reported PCC at T1 to youth EBPs at T2. In addition, mother-report of PCC at T2 predicted youth EBPs at T3 (as reported by fathers), and mother-report of youth EBPs at T3 predicted father-report of PCC at T4. Thus, the important links between PCC and youth EBPs remain outside of single-reporter methods.
In our SEM, mother- and father-reports of PCC and youth EBPs were separately entered into the model because the associations between mother- and father-report were modest. Future studies should examine models that use alternative approaches to account for potential confounds of potential dependence issues that arise with nested couple data (e.g., Deng & Yuan, Reference Deng and Yuan2015). It will also be important for future studies to incorporate youth-report of EBPs from youth with ASD. Future research should also examine other domains of the parent couple relationship such as intimacy, relationship satisfaction, dyadic coping, and conflict resolution strategies in order to better understand the specific underlying mechanisms that drive a connection between PCC and youth outcomes (e.g., couple conflict specifically or marital quality more broadly) in the context of child ASD. Moreover, in the present study, we examined associations between PCC and youth emotional and behavioral functioning from one year to the next; however, bidirectional effects may be stronger across a shorter time frame and/or better captured day-to-day, week-to-week, or month-to-month.
Study Implications
According to the Interagency Autism Coordinating Committee (2016), in 2016, more than US$364 million was allotted to ASD research, with only 16% of these funds allocated to studies on ASD interventions. Our research highlights the importance of research on family-wide interventions, given the intertwined nature of the EBPs of youth with ASD and parent couple functioning. Efforts to foster positive youth emotional and behavioral functioning and efforts to support positive parent couple relationships appear to go hand-in-hand. Thus, family-wide intervention approaches that offer both psychoeducation aimed at helping parents navigate PCCs constructively (e.g., communication coaching) and strategies aimed at teaching youth with ASD how to regulate their emotions and behaviors (e.g., applied behavior analysis) are recommended. In addition, it may also be important to teach fathers ways of preventing negative affect and behaviors generated from partner disagreements from spilling over into parenting behaviors and parent–child interactions. Mindfulness trainings offer one potential strategy for fathers to learn how to avoid “holding on” to stress or projecting negative feelings generated elsewhere into parent–child interactions and instead to focus on present emotions and experiences. As children with ASD age into older childhood and adolescence, it may also be important for fathers to learn new behavior management strategies, especially for internalizing problems, and to recognize and deal with any of their own negative feelings that may trigger over time.
Acknowledgment
We thank the families who gave their time to participate in the study.
Funding Statement
This research was supported by the National Institute of Mental Health (R01MH099190, Hartley) and the National Institute of Child Health and Human Development (U54HD090256, Chang; T32HD07489, Hartley)
Conflicts of Interest
None.






 Open access
Open access