


In 1994, the Norwegian government called for a proposal of a research project in the area of resilience among youth. The project named ‘Resilient Future’ won the competition. The aim of the project was to study the causes and consequences of resilience in youth. To study the developmental process of resilience and its interaction with adversities, behavioral adjustment and mental disorders, one has to include the role of genes. For this task, a genetically informative sample was needed. By means of behavior genetic models, one may be able to figure out the basis of the association between all these variables, especially regarding the disentanglement of apparently environmental causation from gene–environment correlations.
Consequently, the work started out by collecting a twin sample of adolescents. The intention was to follow the sample at least through youth and early adulthood to figure out causal relationships.
Sample Recruitment
After a year of obtaining the necessary permissions, a list of more than 5374 twin pairs were assembled from the countrywide Norwegian Birth Register. The twins were born in the years 1988–1994, seven cohorts who were between 12 and 18 years in 2006 when the start of data collection was planned. The planned procedure was to administer questionnaires in three waves, 2 years apart, and a face-to-face interview when the twins reached 18 years. At the time of the interview, the twins also received a self-report questionnaire of the Big Five, together with a questionnaire about affective, cognitive and behavioral reactions to sensitive interpersonal situations.
It transpired that one or both twins had died in 475 twin pairs (see Figure 1). Furthermore, 131 families had moved abroad. The address was unknown for 100 families, reducing the total number of actual twin families to 4668. The families were contacted by mail, informed about the study’s goals and procedures and invited to participate. In 2486 families, either one or both of the parents or one or both of the twins consented to participate, corresponding to 50.8% of the 5374 families with living twins retrieved from the Birth Registry, and 53.3% of the 4668 families living in Norway with a known address. In 1976 families, both parents and both twins consented to participate. (The reason for incomplete consent from family members was death of the father in 98 families, death of the mother in three families, and death of both parents in one family. Moreover, 360 fathers, 40 mothers, and one or both twins from eight families declined to participate.)
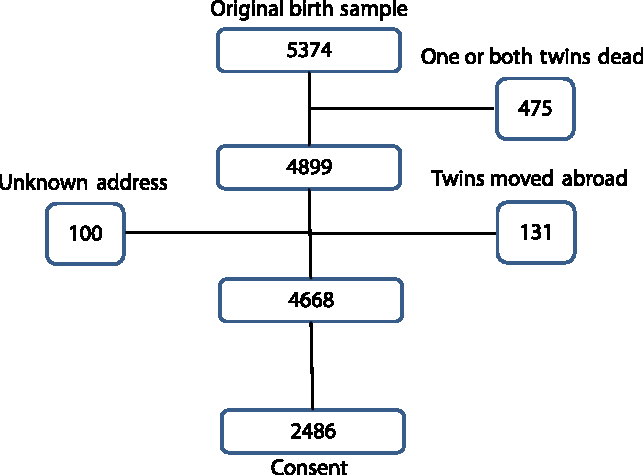
Fig. 1. Attrition of twin pairs from birth to consent.
In the original twin cohorts, 51.0% were boys. After excluding families because of twin death, the percentage of boys was reduced to 50.6, to 50.5% after excluding families that had moved abroad and to 50.3% because of unknown address. Lack of consent further reduced the boys’ percentage to 46.7.
Research Design
The research plan required that both mothers and fathers completed separate questionnaires about each twin. In addition, the twins themselves were asked to fill in questionnaires three times, at ages 12–18, 14–20 and 16–22. The twins only gave a face-to-face interview at around age 18, or later if they were hard to locate. The first wave of the questionnaire data collection was supposed to take place in 2006, the second in 2008 and the third in 2010. The interviews had started already in 2006 when the first cohort (1988) was 18 years old. In 2012, the interviews with the youngest (1994) cohort, who then turned 18 years, could finally begin.
Questionnaires
The questionnaires were almost completely identical for all informants at all waves. The exception was questions about demographics from the parents and questions about sexual topics for the twins. In order to maximize the number of scales, only a few items were included for each. These were retrieved from the results of a pilot study that had been performed previously with the complete scales. From the complete scales, items producing similarly high item-to-trait correlations in both sexes and across all age groups were selected. As the project’s original focus was reactions to adversities, the questionnaire included a number of common, more or less stressful life events, and also a few positive events; (Masten, Neemann, & Andenas, Reference Masten, Neemann and Andenas1994). The parenting style was included, focusing on liberal, authoritarian and laissez-faire styles, as seen from the parental as well as the twin’s point of view (Reitman et al., Reference Reitman, Currier, Hupp, Rhode, Murphy and O’Callaghan2001). Central in the questionnaire were two resilience trait scales, a so-called ‘ego-resilience’ scale (Block & Kremen, Reference Block and Kremen1996), and another scale simply called ‘Resilience scale’ (RS; Wagnild & Young Reference Wagnild and Young1993). In addition, several other personality scales were included: a Big Five scale for children and youth, named the Hierarchical Inventory for Personality in Children (HiPiC; Mervielde & De Fruyt, Reference Mervielde, De Fruyt, Mervielde, Deary, Fruyt and Ostendorf1999) and other scales covering a broad array of personality traits, namely, self-efficacy, including social aptitudes, good school work habits and law-abiding behavior (Pastorelli et al., Reference Pastorelli, Caprara, Barbanelli, Rola, Rozsa and Bandura2001). Internalizing (or internalizing-reversed) scales used were Sense of Coherence (Antonovsky, Reference Antonovsky1987; Mehlum, Reference Mehlum1998), loneliness (Russel, Peplau, & Cutrona, Reference Russel, Peplau and Cutrona1980) and happiness (Cantril’s Ladder; Cantril, Reference Cantril1965). Externalizing scales were delinquency (LeBlanc & Tremblay, Reference LeBlanc and Tremblay1988; Tremblay et al., Reference Tremblay, Phil, Vitaro and Dobkin1994), which comprised truancy, vandalism, violence and antisociality; the Externalizing scale of the Strength and Difficulties questionnaire (SDQ; Goodman, Reference Goodman1997, Reference Goodman2001); and Impulsivity (Patrick, Curtin, & Tellegen, Reference Patrick, Curtin and Tellegen2002). Internalizing and externalizing scales covering DSM-IV-oriented mental disorders were also included: for internalizing problems, the Depression Scale (Fendrich, Weissmann, & Warner, Reference Fendrich, Weissmann and Warner1990; Radloff, Reference Radloff1977); for anxiety, the Screen for Child Anxiety Related Emotional Disorders (SCARED; Birmaher et al., Reference Birmaher, Khetarpal, Brent, Cully, Balach, Kaufman and Neer1997); a scale for somatoform traits (Garber, Walker, & Zeman, Reference Garber, Walker and Zeman1991) and the Eating Disorder Inventory (EDI; Garner & Olmstedt, Reference Garner and Olmstedt1984). On the externalizing side were substance problems, smoking, alcohol and drugs (Johnston et al., Reference Johnston, O’Malley, Bachman and Schulenberg2005; Knight et al., Reference Knight, Sherritt, Shrier, Harris and Chang2002). In addition, there was a coping scale (Spirito et al., Reference Spirito, Stark and Williams1988) and questions about puberty development and sexuality (Petersen et al., Reference Petersen, Crockett, Richards and Boxer1988). Further questions addressed feelings of being integrated in society, school and the family (California Department of Education, 2003), as well as religious affiliation, the ‘Religious Attitudes scale’ (Donovan & Jessor, Reference Donovan and Jessor1985; Heath et al., Reference Heath, Madden, Grant, McLaughlin, Todorov and Bucholz1999).
Interview
The interview — our outcome measure — comprised the International Neuropsychiatric Interview (MINI), an assessment of the most common Axis I disorders in the DSM-IV (Lecruiber et al., Reference Lecruiber, Sheehan, Weiller, Amorim, Bonora, Harnett Sheehan and Dunbar1997; Sheehan et al., Reference Sheehan, Lecruiber, Sheehan, Janavs, Weiller, Keskiner and Dunbar1997, Reference Sheehan, Lecruiber, Sheehan, Amorim, Janavs, Weiller and Dunbar1998). Furthermore, personality disorders were assessed by means of the Structured Interview for DSM-IV Personality Disorders (SIDP-IV; Helgeland, Kjelsberg, & Torgersen, Reference Helgeland, Kjelsberg and Torgersen2005; Helgeland & Torgersen, Reference Helgeland and Torgersen2004; Pfohl, Blum, & Zimmerman, Reference Pfohl, Blum and Zimmerman1997; Torgersen, Kringlen, & Cramer, Reference Torgersen, Kringlen and Cramer2001). In addition, a retrospective trauma interview was included (Fink et al., Reference Fink, Bernstein, Handelsman, Foote and Lovejoy1995). Moreover, questions addressing zygosity again, as well as general wellbeing, were posed. Moreover, the twins received two questionnaires and were asked to return them by mail: The Big Five questionnaire, NEO-PI-R (Costa & McCrae, Reference Costa and McCrae1992; Martinsen, Nordvik, & Østbø, Reference Martinsen, Nordvik and Østbø2005) and the Situational Signature Questionnaire (SiSiQ) for the assessment of affective, cognitive and behavioral reactions to difficult interpersonal situations (Lenswelt-Mulders & Hettema, Reference Lenswelt-Mulders and Hettema2001).
Determination of Zygosity
Determination of zygosity is important in all twin studies. A zygosity scale was included in the questionnaires for twins and parents (Torgersen, Reference Torgersen1979), together with questions about how much the twins were together. To validate the assessment, a subgroup of same-sex twin pairs was asked to provide a salivary sample, which was analyzed for 17 gene markers. These 17 gene markers have a likelihood of misclassifying a dizygotic (DZ) twin pair as monozygotic (MZ) of only p < .0001. Twin pairs with zygosity scores in the middle between those supposed to be either MZ or DZ were oversampled. The same-sex twin pairs who were not gene tested were classified as MZ or DZ twins based on discriminant analysis of the zygosity scores.
Attrition of Waves
Twins as well as parents were asked to fill out questionnaires at each wave. However, if the twins passed the age of 18, parents no longer received questionnaires because most young adults leave home at this age. This means that for the youngest 1992–1994 cohorts, questionnaires were sent to both twins and parents at all three waves. However, for the cohorts 1990–1991, the parents’ questionnaires were not included at Wave 3, and for the cohorts 1988–1989, the parents’ questionnaires were not included at Waves 2 and 3.
When one or both, almost always both, twins returned questionnaires to us, 97.3% of the mothers and 69.6% of the fathers also filled out the questionnaires.
Figure 2 shows the reduction in participation from Wave 1 to Wave 2 and from Wave 2 to Wave 3. Participation was counted if at least one person from each family returned the questionnaire.
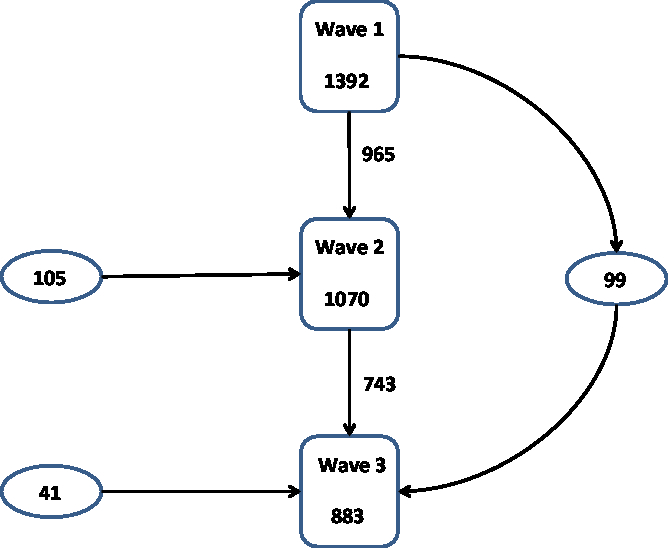
Fig. 2. Attrition through the waves.
Thirty-one percent of twin pairs did not transit directly from one wave to the next, which was the same from Wave 1 to Wave 2 as from Wave 2 to Wave 3. Furthermore, 105 twin pairs appeared for the first time in Wave 2 and 41 pairs appeared for the first time in Wave 3. Finally, 99 pairs who participated in Wave 1, but not Wave 2, reappeared in Wave 3.
Table 1 gives a more complete picture of the combinations of participation in the different waves. In total, 1538 pairs participated in any wave, a little more than one-fourth participated in only one wave (428 pairs), or in two waves (413 pairs), and a little less than half in all three waves (697).
Table 1. Number of twin pairs in different wave participation combinations

Understandably, few twins appeared for the first time in Wave 2 (59 + 46 pairs), and even fewer for the first time in Wave 3 (41 pairs). The practice of inviting families that had consented, but not participated in a preceding wave, increased the number of pair/wave participations by 291.
Table 2 shows the distribution of sex–zygosity combinations in the three waves and among those who participated in one, two or three waves. No differences between the various waves and between the numbers of participants at each wave were statistically significant in cross-tabulations. Generally, more female than male pairs participated, especially from MZ pairs, and slightly more same-sex DZ pairs than opposite-sex pairs participated. The percentages of males declined from 45.0 in Wave 1, through 43.3 in Wave 2 and 41.7 in Wave 3. The percentages of males were 45.0 among those who only participated in one wave, 43.3 among those who participated in two waves and 42.0 among those who participated in all three waves. We observed a tendency of females being more inclined to stay in the project. It was mentioned that in the consenting sample, the percentage of boys was 46.7. In comparison, the percentage of boys that actually participated in at least one wave was 44.5.
Table 2. Number (%) of twin pairs participated in different data collection waves and those participated in one, two or three waves by sex and zygosity
Note: MMZ = male monozygotic, FMZ = female monozygotic, MDZ = male dizygotic, FDZ = female dizygotic, ODZ = opposite-sex dizygotic.
The percentages of MZ twins who participated were around 36–40 in different waves and among those that participated in one, two or three waves, without any difference from first to last wave or from participating in one or three waves. The total MZ percentage was 37.3%.
As mentioned earlier, the plan was to carry out a wave every second year and an interview when the twins turned 18 years. This meant that the twins would be 12–18 years old at Wave 1, 14–20 years at Wave 2 and 16–22 years old at Wave 3. The average ages of the twins in Table 3 show that slightly less than 2 years passed between Waves 1 and 2 and somewhat more than 2 years passed between Waves 2 and 3. There were up to 3 years’ variation in age in the same cohort and wave, as some twins were born earlier in the cohort year, some had moved and time passed in finding the new address, and some twin families delayed for a long time before they returned the questionnaire, after being reminded the permitted number of times.
Table 3. Mean (SD) age of twins in each birth cohort by wave

Note: First wave = 2006–2007, second wave = 2008–2009, third wave = 2010–2011.
Personality differences between the twins who participated only once versus two or three times were analyzed. To investigate this, we constructed personality factors that comprised all personality scales described earlier, completed in all waves and by all informants. A three-factor solution displayed a Shyness factor with neuroticism, introversion and loneliness first and foremost; a Conduct Problems factor consisting of nonagreeableness, delinquency and antisociality; and a Structure factor that included conscientiousness, good school habits, openness and resilience. The Shyness factor was not related to the frequency of the participation in the data collection waves. The scores on the Conduct Problems factor were weakly related to the frequency of wave participation. However, the factor that was very strongly, positively related to the frequency of wave participation was the Structure factor.
The best way of testing attrition bias in twin studies is to see whether heritability is expected to be related to the tendency to participate. A calculation of the average twin correlations over the Big Five HIPIC scales for all informants showed a MZ/DZ ratio of .55/.20 for those participating in one wave, .59/.12 for those participating in two waves and .59/.18 for those participating in three waves. Attrition does not seem to have much influence on the expected heritability estimates.
Attrition from Waves to Interview
All twins were invited to a face-to-face interview at age 18, and 1210 pairs who had participated in any wave accepted the invitation, whereas 328 pairs declined. In addition, 215 pairs who had never participated in any waves accepted to be interviewed. Table 4 shows the sex–zygosity combinations among those who declined to be interviewed in spite of participation in at least one wave, those who participated in both wave and interview and those who only participated in the interview. There were small and nonsignificant differences between those who were interviewed plus wave and those who were interviewed only. However, there were strikingly different sex–zygosity combinations (χ2 = 14.350, df = 5, p = .014) among pairs participating in wave plus interview compared to those participating in wave but declining the interview. Those refusing the interview were more often male, irrespective of zygosity, and more often from opposite-sex twin pairs.
Table 4. Number (%) of twin pairs participated in the waves of questionnaire data collection and/or interview by sex and zygosity

Note: MMZ = male monozygotic, FMZ = female monozygotic, MDZ = male dizygotic, FDZ = female dizygotic, ODZ = opposite-sex dizygotic.
The twins’ average age at the time of the interview was 19.1 years, ranging from 17.5 to 23.3 years. Sixty-two percent of the interviewees were 18 years, 18% were 19 years, 9% were 20 years, 7% were 21 years and finally, 4% were 22–23 years.
Consent to the interview was related to the personality factors mentioned above. The Structure factor, consisting of the HIPIC Big Five conscientiousness and openness (imagination) scales, good school habits and resilience, predicted participation in the interview, whereas the Shyness and the Conduct Problems factors did not.
To see the total picture of predictors of participation in the interview, a stepwise logistic regression analysis was conducted. In addition to the personality factor, birth year (cohort), zygosity, sex and number of times the twins had participated in the study were included. It turned out that zygosity did not predict consenting to the interview. Female sex (Wald = 29.06, p =.000), cohort (later cohort implied shorter time in the project before the interview; Wald = 48.01, p = .000) and participation in higher number of waves before or after the interview (Wald = 176.96, p = .000) predicted consent to the interview. Including all these variables, the Structure factor still predicted participation (Wald = 4.03, p = .045).
As mentioned earlier, the most important test of attrition bias is to compare the available twin correlations for participation and nonparticipation in specific parts of the study. Regarding participation versus nonparticipation in the interview among those participating in any wave, the MZ/DZ correlations of the Big Five HIPIC scales across waves and informants were .59/.17 versus .61/.26. Thus, there does not seem to be any difference in expected personality heritability between those consenting and those not consenting to the interview.
Regarding the twins who had not responded to the waves but came to the interview, they were more often from the younger cohorts and thus consented to the project and interview at a younger age. It may be that they were too young to follow through when they received the questionnaires or that an interview was more attractive. They had slightly higher scores on borderline, antisocial, paranoid and dependent personality disorder traits. Logistic stepwise regression analysis showed that only borderline traits (Wald 14.546, p = .000), in addition to younger age at consent (Wald 21.143, p = .000), independently significantly predicted participation.
Conclusion
The Oslo University Twin sample presented in this article was developed with the aim of investigating the causes and consequences of resilience in youth and adolescence. Because of the combination of informants (parents and twins), the combination of questionnaires and face-to-face diagnostic interview, the high number of assessments repeated biannually and the broad coverage of personality, vulnerability, mental disorders, traumas and other environmental factors, there is a vast number of varied research questions that can be addressed.
Representativeness was also good. In this small country with good registries, it was possible to trace almost all twins from younger cohorts (12–18 years old). More than half of the traced twins (53.3%) consented to participate in the study. Furthermore, 61.9% of these actually participated in at least one of the three biannual waves. In the interview, 57.3% of those who consented to the project participated. Of these, 85.1% had also participated in any waves. The likelihood to participate in a higher number of waves as well as interview was related to structured personality, female sex, but not to zygosity. Most importantly, however, attrition did not bias the heritability estimates.






