


Acute onset, transient psychotic disorders with a good outcome are recognised in both ICD–10 (World Health Organization, 1992a ) and DSM–IV (American Psychiatric Association, 1994) as distinct from schizophrenia and affective psychoses. In ICD–10 acuteness of onset is considered to be their defining characteristic, whereas in DSM–III–R and DSM–IV duration of psychosis of less than 6 months is their distinguishing feature. There is little information about family history, premorbid functioning or course and outcome to validate the independent diagnostic status of these disorders although some studies have suggested that the ICD–10 criteria identify a diagnostically unstable group of disorders with a relatively good outcome (Reference Jorgensen, Bennedsen and HyllestedJørgensen et al, 1997; Reference Amin, Singh and BrewinAmin et al, 1999; Reference Sajith, Chandrasekaran and Sadanandan UnniSajith et al, 2002; Reference Marneros, Pillman and HaringMarneros et al, 2003). There is also little empirical evidence to justify the duration of onset and remission criteria used to delineate acute non-affective psychoses in the two classification systems. The ICD–10 criterion of a 2-week period of onset in acute and transient psychotic disorders (ATPDs; F23) is based on ‘clinical reports and authorities’ (World Health Organization, 1992a : p. 10). The validity of duration criteria for schizophreniform disorders has also been questioned (Reference StrakowskiStrakowski, 1994), since no particular cut-off point of duration criterion seems to identify distinct subgroups of non-affective psychoses (Reference Keith and MatthewsKeith & Matthews, 1991).
In this study we aimed to:
-
(a) determine the age- and gender-standardised incidence rates, gender ratio, 3-year diagnostic stability, course and outcome of ICD–10 ATPDs;
-
(b) determine whether, on the basis of premorbid functioning, family history and 3-year outcome, ATPDs are similar to schizophrenia or to affective psychosis;
-
(c) explore the association between acute onset, early remission and favourable outcome in first-episode non-affective psychotic disorders, when other predictors of outcome such as gender, life events, premorbid functioning and family history are controlled.
METHOD
The Academic Department of Psychiatry in Nottingham University collected a cohort of all people with first-onset psychosis in which the first contact with mental health services was made between June 1992 and May 1994 in a defined geographical area. All the patients concerned received an indepth assessment using established and standardised instruments, along with an extensive collateral history and were assigned an ICD–10 diagnosis. The cohort was followed up 3 years later and assessed using standardised measures. The study reported here was part of this 3-year follow-up. Details of the intake and follow-up studies, the instruments used and their reliability have been described by Brewin et al (Reference Brewin, Cantwell and Dalkin1977) and Singh et al (Reference Singh, Croudace and Amin2000).
Sample
The study sample was an intake cohort comprising all instances of first-onset psychosis in patients aged 16–64 years identified in Nottingham between 1 June 1992 and 31 May 1994. The total population of Nottingham in this age band in 1991 was 397 048 (Office of Population Censuses and Surveys, 1992). The cohort was identified by screening all people making their first-ever contact with psychiatric services for potential psychosis. Patients with an organic mental illness or with severe learning disabilities were excluded.
Follow-up study
The follow-up assessments were conducted between 1 June 1995 and 31 May 1997 and occurred in chronological order of the patient's initial contact with psychiatric services, as close as possible to 3 years after the initial contact. The following measures were used; see Singh et al (Reference Singh, Croudace and Amin2000) for details:
-
(a) Schedules for Clinical Assessment in Neuropsychiatry (World Health Organization, 1992b );
-
(b) Disability Assessment Schedule (Reference Jablensky, Sartorius and EmbergJablensky et al, 1992);
-
(c) Scale for Assessment of Negative Symptoms (Reference AndreasenAndreasen, 1982);
-
(d) Global Assessment Scale (Reference Endicott, Spitzer and FleissEndicott et al, 1979);
-
(e) McGlashan and Strauss–Carpenter scales (Reference McGlashanMcGlashan, 1984; Reference Strauss and CarpenterStrauss & Carpenter, 1974);
-
(f) OCCPI/OPCRIT system (Reference McGuffin, Farmer and HarveyMcGuffin et al, 1991);
-
(g) family history and premorbid functioning (see below);
-
(h) life events (see below).
Family history and premorbid functioning
The patients' family histories and premorbid functioning were rated on OPCRIT and Family History–Research Diagnostic Criteria (Reference Endicott, Andreasen and SpitzerEndicott et al, 1975) using all available sources of information, including case-note scrutiny and direct interviews with carers. Family history of mental illness was recorded for first-degree relatives of the patients, including parents, siblings and children. OPCRIT categories were used for categorising premorbid dysfunction.
Life events
At follow-up, life events information was collected for the 3 months preceding the onset of the psychotic illness from all available sources, including direct patient interview, information from family and carers, and medical records on stressful life events. Events were categorised as bereavement, major loss or separation, trauma or hospitalisation for a non-psychiatric condition, social change including major changes in employment, housing, marital status, migration, and post-partum events.
Definitions
Onset. Onset was defined as the period between the first reported symptom or noticeable behavioural change and the emergence of psychotic symptoms.
Duration of initial psychotic episode. Duration of initial psychotic episode was defined as the period between the emergence of clear psychotic symptoms and remission.
Remission. Remission was defined as the point in time when ‘the patient is virtually symptom free and shows his or her usual premorbid personality’ (Reference Jablensky, Sartorius and EmbergJablensky et al, 1992).
Relapse. Relapse was defined as emergence of symptoms after a 4-week period of return to premorbid functioning.
Outcome. Favourable cross-sectional outcome was defined as no or minimal symptoms in the previous 4 weeks. Favourable longitudinal outcome (i.e. episodic rather than chronic course) was defined as a single psychotic episode with complete remission, or multiple episodes with inter-episodic remission.
Data collection
Information on onset, remission and relapse was gathered from all sources of information, including psychiatric notes, general practitioner's notes, patient interview and carer interview. In patients who had continuing residual symptoms (negative or non-psychotic) following cessation of positive psychotic symptoms, a judgement was made whether these symptoms were part of the initial psychotic episode or represented a new or distinct episode. Where no complete remission and return to premorbid status had been attained, the residual symptoms were considered to be part of the initial episode. This allowed fewer false-positive ratings of remission and also ensured that duration of episode was not restricted to positive psychotic symptoms only.
Diagnostic process
The authors S.P.S. and S.A. presented the follow-up data and assessments to a senior member of the research team (a consultant psychiatrist), with everyone involved in the diagnostic process masked to the original consensus diagnosis. All clinical information available over the 3-year follow-up period was used to determine a longitudinal diagnosis based on ICD–10 criteria for all participants, including those who were ‘currently well’, i.e. whose psychotic episode had ended before the follow-up assessment.
Diagnostic decision tree
A diagnostic decision tree was created as follows.
-
(a) In cases in which no new information emerged subsequent to that used to establish the onset diagnosis, the original diagnosis remained. This ensured that a consensus diagnosis was not made on a reinterpretation of the original data 3 years later.
-
(b) In cases in which the ATPD-diagnosed patient subsequently developed an episode fulfilling ICD–10 criteria for another illness category, such as schizophrenia, affective psychosis or substance-related psychosis, the longitudinal diagnosis changed from ATPD to the subsequent diagnosis. However, cases with a non-ATPD diagnosis at onset were not recorded as ATPD on follow-up even if the patient had experienced a subsequent episode fulfilling the criteria for ATPD. The direction of any change in diagnosis was therefore always away from ATPD.
RESULTS
Characteristics of the intake sample
Between June 1992 and May 1994 a total of 209 patients with first-episode psychosis were referred to the study team. Of these, 71 were excluded because of a subsequently identified previous history of psychosis or an organic cause for the episode. A leakage study identified another 30 patients for inclusion, giving an inception cohort of 168 persons with first-episode psychosis.
Follow-up
Over the follow-up period, one patient was found to have an organic psychosis and was excluded, and another refused to participate in the study, leaving 166 individuals to be followed up. We traced 164 individuals (99%) to their residence, obtained face-to-face interviews with 135 (81%) and another 8 (5%) were interviewed by telephone. Two people had died, one by suicide. For 139 participants (97% of those interviewed), assessments were conducted 35–37 months from inclusion, thus ensuring homogeneity of time elapsed since contact with services. We collected collateral information (from treating psychiatry teams, carers known to the service and general practitioners) on all cases, including those in which the person was not interviewed. We therefore had complete follow-up data for 86% of participants and partial data for the others, including all those who had not been directly interviewed.
The socio-demographic profile of the total cohort and the ATPD subgroup, subdivided by gender, is presented in Table 1. Diagnoses in the 166 cases were 112 (67.5%) non-affective psychosis (F20–29), 56 (33.7%) schizophrenia (F20), 41 (24.7%) affective psychosis (F30–33), 13 (7.8%) substance-induced psychosis (F1x) and 32 (19%) acute and transient psychotic disorder (F23). In the ATPD group, 12 patients (37.5%) had acute delusional disorder (F23.3), 10 (31%) had acute polymorphic disorder without symptoms of schizophrenia (F23.0), 7 (22%) had acute schizophrenia-like psychosis (F23.2) and 3 (9%) had acute polymorphic disorder with symptoms of schizophrenia (F23.1). Although there was no statistically significant difference between men and women in this group in mean age at first contact with psychiatric services (t=0.416, P=0.68), there was a trend for women to be older than men; the means were skewed by two outlying cases of men who had an age at first contact of over 50 years. Dichotomising data into those below and above age 30 years still did not lead to a statistical difference between the genders on age at onset (χ2=1.347, P=0.28). Men with ATPDs were significantly more likely to have been unemployed than women (χ2= 5.45, P=0.03). There was no excess of ethnic minority patients in the ATPD group.
Table 1 Socio-demographic characteristics of the study cohort
| Variable | Total cohort (n=166) | Acute and transient psychotic disorders (n=32) | ||
|---|---|---|---|---|
| Men (n=98) n (%) | Women (n=68) n (%) | Men (n=21) n (%) | Women (n=11) n (%) | |
| Age, years1 | ||||
| 15–30 | 70 (71) | 33 (49) | 14 (67) | 5 (46) |
| 31–50 | 22 (22) | 26 (38) | 5 (24) | 6 (54) |
| > 51 | 6 (6) | 9 (13) | 2 (9) | 0 |
| Marital status | ||||
| Single | 66 (67) | 30 (44) | 11 (52) | 8 (73) |
| Married/cohabiting | 21 (21) | 27 (40) | 6 (28) | 1 (9) |
| Separated/divorced | 9 (10) | 9 (13) | 2 (10) | 2 (18) |
| Widowed | 2 (2) | 2 (3) | 2 (10) | 0 |
| Ethnic status | ||||
| White | 68 (70) | 53 (78) | 14 (67) | 7 (64) |
| African–Caribbean | 20 (20) | 14 (20) | 4 (19) | 3 (27) |
| Asian/other | 10 (10) | 1 (2) | 3 (14) | 1 (9) |
| Accommodation | ||||
| Owner occupied | 13 (13) | 28 (41) | 4 (19) | 4 (36) |
| Rented/council property | 39 (41) | 27 (40) | 9 (43) | 6 (55) |
| Living with relative/carer | 39 (41) | 13 (19) | 7 (33) | 1 (9) |
| Hostel/shelter/prison/RSU | 5 (5) | 0 | 1 (5) | 0 |
| Employment status | ||||
| Full/part-time/homemaker/retired | 11 (11) | 23 (34) | 2 (10) | 5 (45) |
| Unemployed/sickness benefit/other | 87 (89) | 45 (66) | 19 (90) | 6 (55) |
Diagnostic certainty of ATPD
At the time of initial assessment there had been uncertainty about acuteness of onset in a proportion of ATPD cases in which the possibility of previous symptoms, prior to the acute emergence of psychosis, could not be completely ruled out. Onset had been unequivocally acute in 9 of 11 women, with two women having an alternative diagnosis of bipolar affective disorder, current episode mixed (F31.6) and severe depressive episode with psychotic symptoms. In more than half of the men (11 out of 21) there was uncertainty regarding the acuteness of onset, with alternative diagnoses assigned in seven cases as follows: one case each of cannabis-related psychosis (F12.5), stimulant-induced psychosis (F15.53), psychotic mania (F30.2) and psychotic depression (F32.3) and three cases of multiple drug use psychosis (F19.53).
Diagnostic stability
After 3 years the longitudinal diagnosis remained unchanged in 8 out of 11 women (73%) but in only 3 out of 21 men (14%) with an intake diagnosis of ATPD. In 9 men (43%) with an intake diagnosis of ATPD the longitudinal diagnosis was changed to schizophrenia or delusional disorder and in 5 men (24%) it was changed to affective psychosis. The corresponding figures for women were 18% (2/11) and 9% (1/11) respectively. In none of the women, but in 3 men (14%), the intake diagnosis of ATPD was changed to substance-related psychosis.
Reasons for diagnostic change
The most common reason for a change in diagnosis (in half of the 32 cases) was that subsequent episodes met criteria for a non-ATPD diagnosis such as schizophrenia or affective psychosis (Fig. 1). In 5 cases (16%) the diagnosis was changed because when the duration of the initial episode was reassessed at follow-up, it was thought to have been longer than the duration criteria for ATPDs. What appeared to have been a complete remission during the intake diagnostic meeting was, at follow-up assessment, considered to have been only a brief remission of positive psychotic symptoms, with symptoms re-emerging without the patient having achieved a return to premorbid level of functioning. No case given a non-ATPD diagnosis at onset subsequently satisfied ICD–10 criteria for ATPDs at follow-up. This validated our a priori decision-tree assumption that change in ATPD diagnosis would always be from ATPD to a non-ATPD category. Comparing schizophrenia-like and non-schizophrenia subgroups of ATPDs revealed that the diagnosis was stable in 6 of 22 (27.3%) cases in the non-schizophrenia categories (F23.0 and F23.3) and in 5 of 10 (50%) cases of schizophrenia-like categories (F23.1 and F23.2). However, this difference did not reach statistical significance (χ2=1.56, d.f.=1, P=0.25), although the small number of cases has a low power to detect any potential difference.
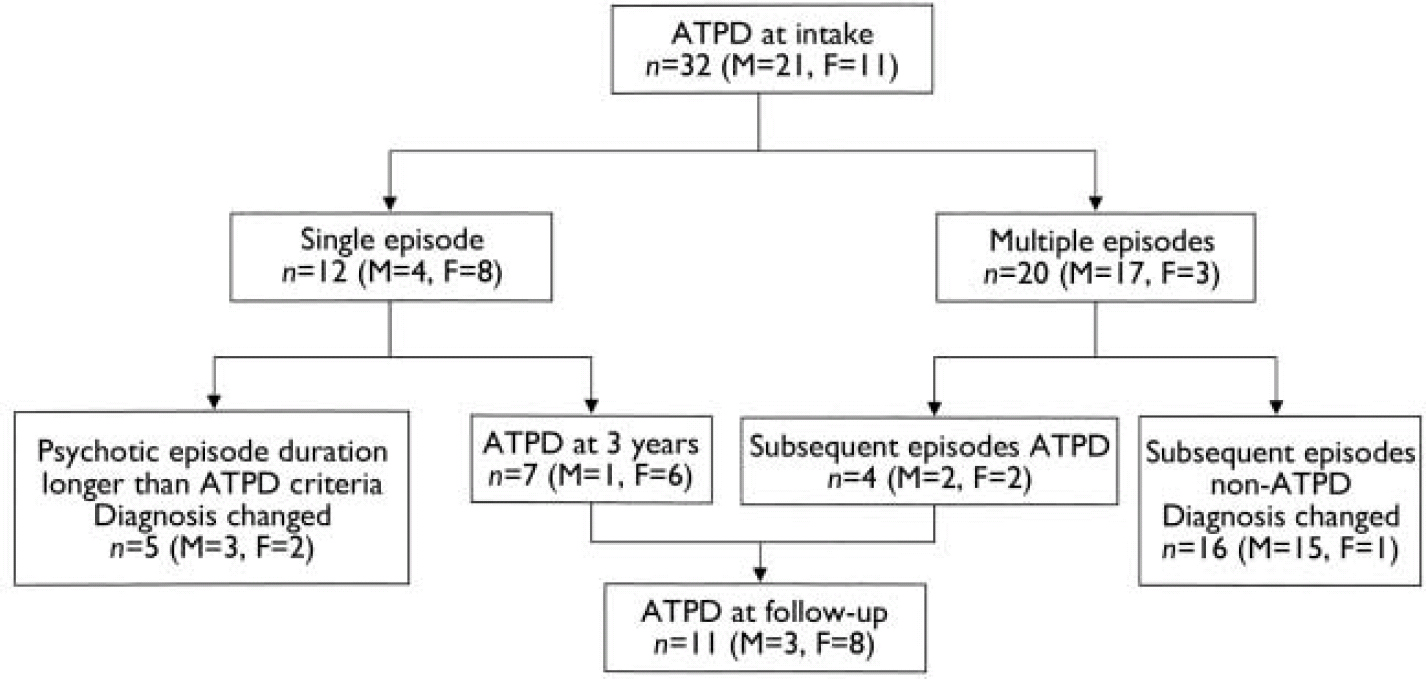
Fig. 1 Change in diagnosis of acute and transient psychotic disorders (ATPDs) over 3 years (M, male; F, female).
Epidemiology of ATPDs
The incidence rates and gender ratios given here are age- and gender-standardised for the population of England and Wales, 1991 census. Based on the intake consensus diagnosis, the annual incidence rate of ATPDs was 3.90 per 100 000 population (95% CI 2.55 to 5.26). The rate in men was almost double that in women (5.08 v. 2.72) with a male/female ratio of 1.87 (95% CI 0.90 to 3.88). The overall annual incidence rate for the ‘true’ 3-year diagnosis of ATPDs was much lower (1.36 per 100 000, 95% CI 0.56 to 2.17) with a female preponderance (men: 0.74 per 100 000, 95% CI 70.09 to 1.58; women: 1.99 per 100 000, 95% CI 0.61 to 3.38; male/female ratio 0.037, 95% CI 0.02 to 0.08).
Family history and premorbid functioning
Table 2 summarises premorbid functioning and family history of patients with ATPDs (diagnosed at both intake and 3-year assessments), schizophrenia and affective psychosis, subdivided by gender. In the ATPD group diagnosed at intake, men were more likely than women to have a positive family history of a psychiatric disorder or of premorbid dysfunction. None of this group had a family history of schizophrenia. In the 3-year ‘true’ ATPD subgroup, no one had a positive family history of any psychiatric disorder, and one man and one woman had a history of premorbid dysfunction. The small numbers did not permit further statistical analysis.
Table 2 Premorbid functioning and family history according to ICD–10 diagnosis and gender
| Variable | n | Intake ATPDs, n (%) | ‘True’ (3-year) ATPDs, n (%) | Schizophrenia, n (%) | Affective psychosis, n (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Men (n=21) | Women (n=11) | Men (n=3) | Women (n=8) | Men (n=38) | Women (n=18) | Men (n=16) | Women (n=25) | ||
| Family history | |||||||||
| Family history of any psychiatric disorder | 41 | 4 (19) | 1 (9) | 0 | 0 | 8 (21) | 3 (17) | 10 (62) | 6 (24) |
| Family history of schizophrenia | 9 | 0 | 0 | 0 | 0 | 4 (10) | 1 (6) | 0 | 0 |
| Family history of affective disorder | 23 | 3 (14) | 0 | 0 | 0 | 1 (3) | 2 (11) | 9 (56) | 4 (16) |
| Premorbid functioning | |||||||||
| Poor premorbid work adjustment | 39 | 7 (33) | 1 (9) | 0 | 1 (12) | 17 (46) | 3 (17) | 0 | 2 (8) |
| Poor premorbid social adjustment | 33 | 5 (24) | 0 | 0 | 0 | 13 (35) | 3 (17) | 0 | 3 (12) |
| Premorbid personality disturbance | 29 | 5 (24) | 0 | 1 (33) | 0 | 8 (22) | 3 (17) | 0 | 2 (8) |
Three-year course and outcome
Table 3 shows a range of outcomes, comparing ATPDs with schizophrenia and affective psychosis. Compared with the schizophrenia group, patients with ATPDs were significantly more likely to have had an episodic course with full remission between episodes, although the two groups did not differ on total number of admissions, days spent in hospital or the proportion detained under the Mental Health Act 1983. The social, occupational and symptomatic outcomes of the ATPD group in the year preceding follow-up assessment were also significantly better than those of the schizophrenia group. Cross-sectionally, patients with ATPDs had a significantly better outcome in terms of disability and symptoms, including negative symptoms, than patients with schizophrenia. Compared with the group with affective psychosis, patients with ATPDs had similar longitudinal and cross-sectional outcomes in every domain.
Table 3 Course and outcomes of acute and transient psychotic disorders compared with schizophrenia and affective psychosis
| ATPDs (n=32) | Schizophrenia (n=56) | Affective psychosis (n=41) | ATPDs v. schizophrenia | ATPDs v. affective psychosis | |||
|---|---|---|---|---|---|---|---|
| Mean difference/OR (95% CI) | P | Mean difference/OR (95% CI) | P | ||||
| Outcome over 3 years | |||||||
| Single episode or multiple episodes with full interepisodic remission, n (%) | 24 (75) | 20 (36) | 32 (78) | 5.4 (2.0 to 14.20) | 0.001 | 0.8 (–6.3 to 4.7) | 0.78 |
| Hospitalisation | |||||||
| In-patient days, mean (s.d.) | 83.3 (124.2) | 92.59 (144.6) | 70.46 (133.4) | 9.2 (–69.8 to 51.4) | 0.76 | 12.9 (–48.0 to 73.7) | 0.67 |
| Admissions, mean (s.d.) | 2.1 (1.8) | 1.61 (1.26) | 1.63 (1.53) | 0.5 (–0.2 to 1.1) | 0.14 | 0.5 (–0.3 to 1.2) | 0.25 |
| Any compulsory admission, n (%) | 18 (56) | 28 (50) | 15 (37) | 1.2 (0.5 to 3.3) | 0.63 | 2.5 (0.8 to 5.0) | 0.1 |
| Outcome in the past year | |||||||
| Strauss–Carpenter categories, n (%) | |||||||
| None/minimal symptoms | 21 (66) | 22 (43) | 29 (71) | 2.5 (1.1 to 10.0) | <0.04 | 0.6 (0.3 to 2.5) | 0.79 |
| Employed | 12 (37) | 8 (16) | 22 (54) | 3.3 (1.2 to 10.0) | 0.01 | 0.6 (0.2 to 1.4) | 0.26 |
| No hospitalisation | 22 (69) | 40 (76) | 30 (73) | 1.2 (0.4 to 3.3) | 0.65 | 1.1 (0.4 to 3.3) | 0.84 |
| Weekly contact with friends/family | 18 (56) | 11 (22) | 26 (63) | 5.0 (2.0 to 10.0) | <0.001 | 0.8 (0.3 to 2.0) | 0.64 |
| None/minimal impairment | 22 (69) | 18 (35) | 30 (73) | 5.0 (1.6 to 10.0) | <0.01 | 0.9 (0.3 to 2.5) | 0.84 |
| Cross-sectional outcome, | |||||||
| GAF score mean (s.d.) | |||||||
| Symptoms | 70 (20.4) | 55.2 (18.9) | 72.2 (15.7) | 13.5 (5.2 to 21.9) | 0.002 | 2.5 (–11.0 to 6.0) | 0.56 |
| Disability | 71.3 (18.3) | 58.7 (15.8) | 74.5 (15.2) | 11.2 (3.9 to 18.4) | 0.003 | 3.1 (–11.0 to 4.7) | 0.43 |
| SANS score, mean (s.d.) | 2.6 (4.3) | 5.2 (3.4) | 1.5 (1.9) | – 2.3 (–3.9 to –0.6) | 0.007 | 1.0 (–0.5 to 2.6) | 0.19 |
Acute onset and early remission in first-episode non-affective psychoses
Of the 112 cases of non-affective psychoses (56 schizophrenia, 32 ATPDs, 13 delusional disorder, 5 schizoaffective psychosis, 1 induced delusional disorder and 5 other or unspecified psychosis), 42 patients (38%) were female, 22 (20%) had an acute onset (reassessed onset at follow-up assessment), 34 (30%) had experienced a stressful life event prior to the emergence of psychosis, 71 (63%) had a duration of psychotic episode of less than 6 months, and 56 (50%) had a favourable, episodic course. Figure 2 shows the distribution of duration of initial psychotic episodes in participants with acute, non-affective psychotic disorder. Eighteen (82%) had an initial episode lasting less than 32 weeks; in the majority (15/22, 73%) its duration was less than 6 months, and three patients (14%) had an episode longer than 1 year (data missing in one case). It appears, therefore, that people with acute-onset non-affective psychosis either tend to recover within about 6 months, or are ill for more than a year.
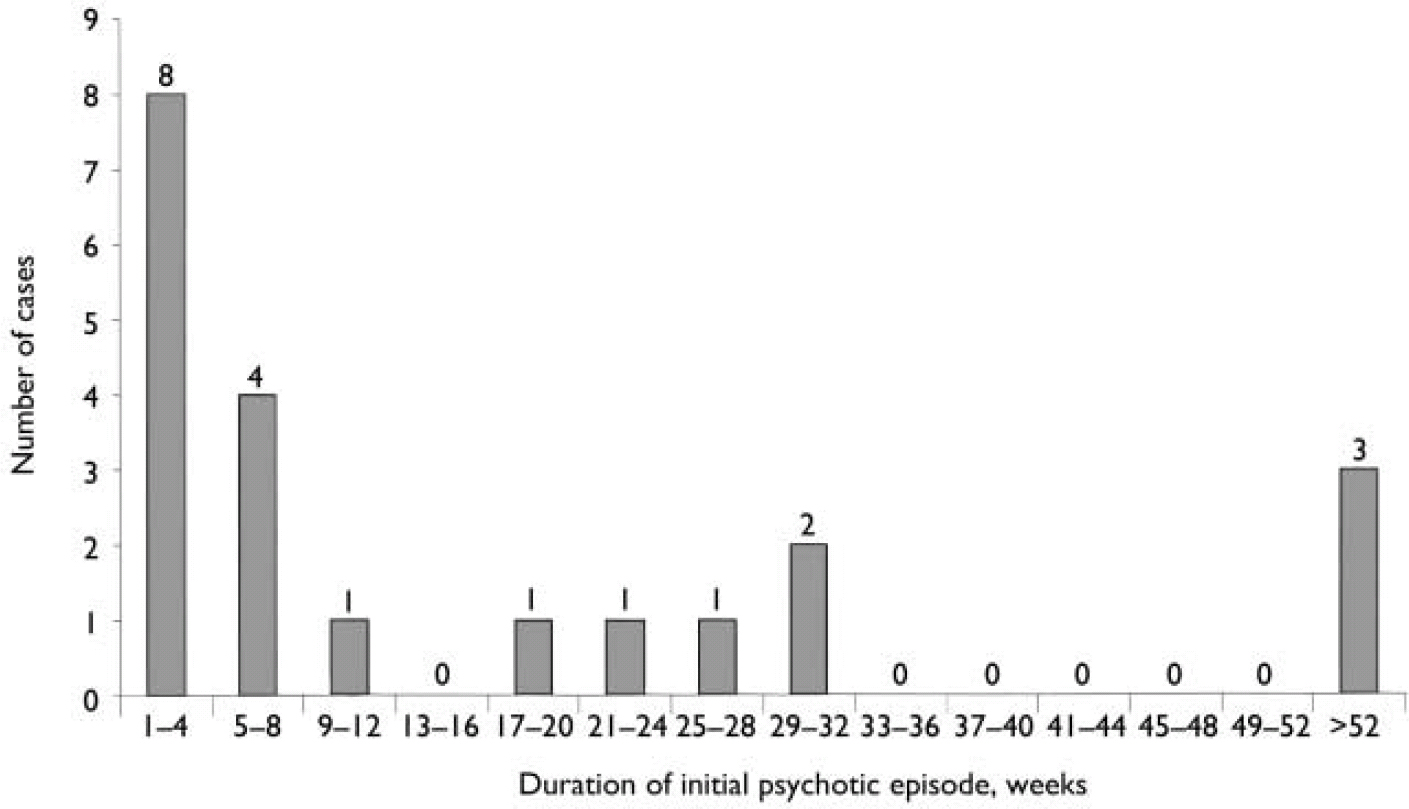
Fig. 2 Duration of initial psychotic episode in all cases of non-affective psychosis (F20–29).
There was no ethnic difference in acute onset (White v. non-White: χ2=0.03, P= 0.53; White v. African–Caribbean: χ2=0.04, P=0.55) or a duration of initial episode <6 months (White v. non-White: χ2=0.384, P=0.65; White v. African–Caribbean χ2=1.28, P=0.33). An earlier study from our data-set had found that course and outcome did not differ between White patients and African–Caribbean patients with first-episode psychosis (Reference Harrison, Amin and SinghHarrison et al, 1999). Ethnicity was therefore not included as an independent variable in subsequent analyses.
Multivariate analysis: predictors of favourable outcome
To test the independent effects of acute onset and brief duration of initial psychotic episode and good outcome, logistic regression was conducted with good cross-sectional and longitudinal outcome as the dependent variable and gender, age at first contact, acute onset, brief initial duration of psychotic episode, life event prior to first episode, premorbid functioning and family history as independent variables.
Table 4 displays the results of the logistic regression showing adjusted odds ratios for variables predicting favourable cross-sectional and longitudinal outcome. Only female gender and favourable premorbid social functioning predicted favourable symptomatic outcome, and female gender and good premorbid occupational functioning predicted good longitudinal outcome. Acute onset, duration of initial psychotic episode, age at first contact, life event, premorbid personality dysfunction or a positive family history did not have an independent effect on either cross-sectional or longitudinal outcome. We repeated the analyses using different definitions of acute onset (less than 1 month) and early remission (episode duration less than 3 months) and on all first-episode psychoses, including affective psychoses. However, in each of these analyses, the only consistent predictors of good outcomes were female gender and good premorbid functioning in social and occupational domains.
Table 4 Adjusted odds ratios for variables predicting favourable outcome in first-episode psychosis (n=112)

| Predictive variable | Good cross-sectional outcome (no/minimal symptoms at follow-up) | Good longitudinal outcome (episodic course over 3 years) | ||
|---|---|---|---|---|
| OR (95% CI) | P | OR (95% CI) | P | |
| Male gender | 0.38 (0.15 to 0.93) | 0.03 | 0.26 (0.11 to 0.60) | 0.002 |
| Age at first contact | 0.99 (0.95 to 1.04) | 0.79 | 0.96 (0.92 to 1.04) | 0.06 |
| Onset period <1 week | 2.87 (0.78 to 9.71) | 0.12 | 1.75 (0.55 to 5.55) | 0.21 |
| Duration of episode <6 months | 2.3 (0.81 to 6.70) | 0.12 | 1.2 (0.46 to 3.26) | 0.68 |
| Life event prior to first episode | 0.99 (0.34 to 2.86) | 0.99 | 0.53 (0.19 to 1.44) | 0.21 |
| Good premorbid social functioning | 7.52 (1.88 to 30.13) | 0.004 | 2.32 (0.67 to 8.44) | 0.20 |
| Good premorbid occupational functioning | 1.52 (0.43 to 5.35) | 0.51 | 4.09 (1.32 to 12.71) | 0.01 |
| Good premorbid personality adjustment | 0.99 (0.26 to 3.72) | 0.99 | 1.05 (0.30 to 3.71) | 0.94 |
| Family history of mental illness | 0.55 (0.17 to 1.78) | 0.31 | 0.70 (0.23 to 2.16) | 0.54 |
DISCUSSION
Our study assessed 3-year cross-sectional and longitudinal outcomes of an intake cohort of all people with first-episode psychoses identified within a geographically defined catchment area. The intake population included patients from both hospital and community-based services. At followup, the sample was homogeneous for time since participant's first contact with mental health services. Multiple sources of information were used and data were collected with well-developed and validated research instruments. Interrater reliability of the research instruments was established prior to data collection (Reference Brewin, Cantwell and DalkinBrewin et al, 1977; Reference Singh, Croudace and AminSingh et al, 2000). Consensus diagnoses were made using ICD–10 criteria. The strengths of the study are the completeness and comprehensive tracing of the intake cohort, a high proportion of face-to-face interviews, use of operational criteria for diagnosis and the use of standardised instruments with high interrater reliability. To the best of our knowledge, within the psychiatric literature, this is the only epidemiological study of first-episode ICD–10 acute and transient psychotic disorders collected within an inception cohort of all first-episode psychoses.
Limitations of the study
The most significant limitations of the study are the small sample size and the limited follow-up period. This partly reflects the rarity of ATPDs, especially in the developed world, and limits the power of the study to detect small but potentially important differences in course and outcome. Second, this is a study of treated outcomes of first-episode psychosis. The ‘true’ natural history of psychotic disorders cannot be determined from studies of treated populations (Reference Waddington, Scully and YoussefWaddington et al, 1997). In a secondary care setting such as the one in which this study was conducted, it is unlikely that patients with psychosis would be antipsychotic-free. Hence, comparisons between historical outcomes with those in current mental health care settings have to be made cautiously. Finally, cultural differences in the incidence and presentation of ATPDs suggest caution in generalising our findings to other cultural settings.
Epidemiology, diagnostic stability and outcome of ATPDs
The ICD–10 recognises that there is little empirical information on ATPDs, and ‘the limited data and clinical traditions that must therefore be used instead do not give rise to concepts that can be clearly defined and separated from each other’ (World Health Organization, 1992a : p. 99). Our data suggest that ICD–10 criteria identify a diagnostically unstable group of disorders comprising good-outcome schizophrenia, affective psychosis and a small group of non-affective, non-schizophrenic psychoses with an acute onset and benign 3-year course. Diagnostic stability is not associated with any particular subgroup of ICD–10 ATPDs. Jørgensen et al (Reference Jorgensen, Bennedsen and Hyllested1997) have also questioned the value of having subgroups of ATPDs because the small numbers virtually preclude empirical validation.
The male preponderance at intake in this study is at striking variance with most previous reports, which report female preponderance in all forms of ATPD (Reference LeonhardLeonhard, 1975; Reference Cutting, Clare and MannCutting et al, 1978; Reference Lindvall, Hognell and OhmanLindvall et al, 1986; Jørgensen et al, Reference Jorgensen, Bennedsen and Christensen1996, Reference Jorgensen, Bennedsen and Hyllested1997; Reference Pillmann, Hairing and BalzuweitPillmann et al, 2002; Reference Marneros, Pillman and HaringMarneros et al, 2003). Our follow-up suggests that men – especially men with schizophrenia – were more likely to have been assigned a false-positive diagnosis of ATPD at intake. This might also partly explain why in a greater proportion of patients the change in diagnosis was to schizophrenia rather than to affective psychosis, contrary to earlier reports (Reference Jorgensen, Bennedsen and HyllestedJørgensen et al, 1997; Reference Sajith, Chandrasekaran and Sadanandan UnniSajith et al, 2002). However, the gender ratio based on the 3-year longitudinal diagnoses is similar to that of the World Health Organization's Determinants of Outcome of Serious Mental Disorders (DOSMED) study, although the total incidence is twice that of the DOSMED rates for developed countries (Reference Susser and WanderlingSusser & Wanderling, 1994). Our 3-year incidence rate and gender ratio for ATPDs are possibly close to the ‘true’ incidence of ATPDs in the developed world.
Even though the diagnosis changes over time, the overall outcome for ATPDs over 3 years is better than that in schizophrenia and similar to affective psychosis, confirming the good outcome of acute psychoses (Reference Stephens, Shaffer and CarpenterStephens et al, 1982; Susser et al, Reference Susser, Varma and Malhotra1995a ,Reference Susser, Fenning and Jandorf b ; Reference Johnstone, Connelly and FrithJohnstone et al, 1996). Our results suggest that ‘true’ ATPDs are not linked genetically to either schizophrenia or affective psychosis. The lack of a positive family history in diagnostically stable ATPDs points to ‘environmental’ aetiological factors which may not have been elucidated by the relatively crude life events measure of this study. An environmental cause of ATPDs is also suggested by the absence of premorbid dysfunction in this and in a previous study (Reference Pillman, Bloink and BalzuweitPillman et al, 2003), since premorbid dysfunction is a measure of developmental ‘deviance’, usually associated with schizophrenia (Reference van Os, Takei and Castlevan Os et al, 1995).
Acute onset and early remission in non-affective psychoses
We confirmed the finding by Susser et al (Reference Susser, Varma and Malhotra1995a ) that acute non-affective psychoses tend either to resolve within 6 months or to have an initial episode longer than 1 year. Susser et al suggested that such a ‘bimodal distribution’ confirms the existence of a group of ATPDs distinct from schizophrenia. We did not feel that a conclusion regarding bimodality was warranted in our data and we did not statistically test for bimodality. Bimodality, in a strictly mathematical or statistical sense, can be tested only when there is an underlying assumption of two normal distributions. The term ‘bimodal’ in this context may thus be misleading, since those who have an initial psychotic episode longer than 52 weeks might not have a single mode at all. However, our findings support the notion that the ICD–10 duration criterion for ATPDs may be too brief and restrictive (Reference Susser, Fenning and JandorfSusser et al, 1995b ).
A third psychosis?
In our study, favourable outcomes in non-affective psychoses were associated with female gender and good premorbid functioning rather than with acute onset and a brief initial psychotic episode. This challenges the notion of a ‘third psychosis’, distinct from schizophrenia and affective psychosis, which can be identified solely on onset and duration criteria. The ICD–10 criteria for ATPDs have attempted to bring together overlapping but discrete clinical constructs – some based on aetiological notions, others on psychodynamic concepts and some based on differences in clinical presentation. In the absence of empirical evidence that might convert such constructs into diagnostic criteria, ICD–10 has selected the two shared aspects that lend themselves to measurement: acute onset and early remission. It is not surprising, therefore, that ICD–10 ATPDs are (diagnostically at least) a heterogeneous group of disorders. Both ICD and DSM systems are based on symptoms and discount the ‘non-empirical’ aspects of diagnosis, which may constitute the ‘phenomenological essence’ of a psychotic disorder (Reference KendlerKendler, 1990). This conflict between logical empiricism and phenomenological understanding of the disorder is reflected in the debates about reliability v. validity of diagnostic categories. ‘Extra-clinical’ aspects of validity, such as positive family history and premorbid dysfunction, could be included in future systems, but developing ‘reliable’ criteria for these is likely to be problematic.
Implications for ICD–11 and DSM–V
Given our findings that neither acute onset nor early remission are independently associated with good outcome, should a separate category of ATPDs, defined by these two criteria, be maintained in diagnostic systems? The answer at this stage of our understanding is ‘probably yes’, for the following reasons. First, the significant cross-cultural differences in the incidence rates and outcome of ATPDs (Reference Sartorius, Jablensky and ShapiroSartorius et al, 1978; Reference Susser and WanderlingSusser & Wanderling, 1994) cannot be discounted on the basis of a small study from a part of the world where ATPDs are rare. Further cross-cultural research may shed light on the reasons behind these cultural differences. Meanwhile, it is important that international classification systems reflect international variations in psychiatric disorders. Second, the ability to identify a distinct group of acute and transient disorders among first-episode psychoses confers important clinical advantages such as predicting course and devising long-term treatment strategies. The criteria for identifying such a group need to be refined rather than the category abandoned. Finally, having a category of ATPDs draws attention to the spurious certainty about the boundaries between schizophrenia and affective psychosis and emphasises the limitations of the Kraepelinian dichotomy. It also highlights the shortcomings of the current emphasis on reliability rather than validity of diagnostic criteria.
We support the recommendation that ICD–11 and DSM–V should include a category of acute non-affective psychoses (Reference Susser, Finnerty and SohlerSusser et al, 1996; Reference Mojtabai, Susser and VarmaMojtabai et al, 2000). However, we propose that a specific criterion-based definition of onset be included. The definition of onset used in this study – the time between the first reported or observed change in mental state or behaviour and the development of psychotic symptoms – is promising. This definition includes both the beginning of onset (i.e. first change, including prodromal symptoms) and its termination (i.e. the point when any psychotic symptoms emerge and reach a diagnostic threshold).
Implications for future research
Our findings highlight the need for further research in two important areas. First, onset in psychosis is not only poorly researched, it is also poorly conceptualised. The ICD–10 defines onset as ‘a change from a state without psychotic features to a clearly abnormal psychotic state’ (World Health Organization, 1992a : p. 99). The Diagnostic Criteria for Research define onset as ‘the time interval between the first appearance of any psychotic symptoms and the presentation of the fully developed disorder’ (World Health Organization, 1994: p. 108). Although the former definition might include prodromal symptoms, the latter excludes them, but fails to explain what the phrase ‘fully developed disorder’ means. There has been practically no research into the chronology and components of the onset of psychosis, and some of the uncertainty probably resides in the nebulous nature of the phenomenon itself. However, if onset is to be a diagnostic criterion, it needs a clearer definition, and some empirical validation of the chronology of onset. Second, the relationship between life events, stress and psychosis is still poorly understood. Identifying a group of psychotic disorders that are precipitated by stress and have a favourable outcome would enhance our understanding of the biological and psychosocial variables influencing the course and outcome of psychosis. Many current debates and controversies, such as the excess of schizophrenia in immigrant groups, the role of psychological v. pharmacological treatments, and early detection and intervention in high-risk groups might be illuminated by a greater understanding of the nature of acute and transient psychotic disorder.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ The ICD–10 criteria for acute and transient psychotic disorders identify a heterogeneous group of disorders, with the diagnosis being stable in women but not in men.
-
▪ The 3-year outcome of these disorders is similar to that of affective psychosis and much better than that of schizophrenia.
-
▪ In non-affective psychotic disorders, female gender and good premorbid functioning, rather than an acute onset and early remission, predict favourable 3-year outcome.
LIMITATIONS
-
▪ Since acute and transient psychotic disorders are rare in the Western world, these findings may not be generalisable to non-developed countries.
-
▪ The sample size is modest and may have limited the power of the study to detect important clinical associations.
-
▪ No structured life events scale was used; hence life event data might have been influenced by recall bias.
Acknowledgements
The study was funded by the National Health Service Trent Research and Development and the Stanley Medical Research Institute.







eLetters
No eLetters have been published for this article.