


Evidence for changing food environments in Africa
Africa is currently experiencing rapid demographic change, partly driven by increasing migration of individuals to cities. As a consequence, people's food environments and dietary habits are also changing, leading to nutrition transition, which results in a modification in food patterns from famine to affluent diets that are associated with increasing levels of obesity and nutrition-related non-communicable diseases coexisting with undernutrition(1, Reference Steyn and McHiza2). This double burden of malnutrition represents a pressing public health concern and healthy food environments have the potential to prevent multiple forms of malnutrition by targeting shared drivers(Reference Pradeilles, Baye and Holdsworth3). The dietary changes arising from this transition are likely to be both qualitative and quantitative, encompassing shifts in the structure of the diet towards a higher intake of energy-dense foods (especially from fat and added sugars), a higher consumption of processed foods(Reference Holmes, Dalal and Sewram4), animal source foods, sugar and saturated fats, and a lower intake of complex carbohydrates, dietary fibres, fruit and vegetables(Reference Popkin, Adair and Ng5). These changes are also expected to include shifts in meal patterns towards a higher number of meals eaten out-of-home. Besides urbanisation, these dietary changes are driven by economic development, increased access to food markets selling energy-dense processed foods at low prices and a decreased price of certain foods such as vegetable oils(Reference Popkin6, Reference Mattei, Malik and Wedick7).
In Africa, there is a lack of published longitudinal food consumption data to illustrate the dietary changes reported in other contexts. Repeated dietary consumption data are available for South Africa, from the Transition and Health during Urbanization in South Africa study(Reference Vorster, Venter and Wissing8) and from the Adult Prospective Urban and Rural Epidemiology cohort study(Reference Wentzel-Viljoen, Laubscher and Vorster9). In urban areas, during 1996–2005, energy from carbohydrates decreased whilst energy from fats increased(Reference Vorster, Kruger and Margetts10). Subsequently over the period 2005–2010 there was an overall increase in energy intake, as well as an increase in the percentage of energy from animal fats and added sugars(Reference Wentzel-Viljoen, Laubscher and Vorster9, Reference Vorster, Kruger and Wentzel-Viljoen11). In the Northern African region, Egypt conducted two National Food Consumption Surveys (1981 and 1998) reporting a substantial increase in meals eaten out-of-home (from 20·4 to 45·8 %)(Reference Galal12).
The present paper explores how changing diets and nutrition transition are impacting on people's lived food environments in urban Africa. We discuss the different ways that food environments can be characterised from different disciplinary perspectives and summarise the methods that can be used to investigate different levels of the food environment. We summarise evidence for the healthiness of urban food environments in Africa, in which we include the social, physical and macro-environments. Finally, we discuss the implications of unhealthy food environments for interventions, policies and research in Africa.
Characterising food environments
There are overlapping ways of framing the food environment, with some disciplines taking a socio-ecological approach, such as Swinburn et al. (Reference Swinburn, Vandevijvere and Kraak13), defining food environments as: Collective physical, economic, policy and sociocultural surroundings, opportunities and conditions that influence people's food and beverage choices. Agri-food disciplinary perspectives tend to focus more on the individual's relation with the physical food environment and broader food system, defining food environments as: The interface that mediates one's food acquisition and consumption with the wider food system. It encompasses multiple dimensions such as the availability, accessibility, affordability, desirability, convenience, marketing, and properties of food sources and products(Reference Turner, Kadiyala and Aggarwal14). The models associated with a food system approach include most of the same factors that are found in the individual, physical and macro-levels of socio-ecological models, but they tend to minimise or exclude the role of the social food environment on people's dietary behaviours(Reference Turner, Kadiyala and Aggarwal14, 15).
A range of models and frameworks have been developed in order to understand why people eat what they do and the role of food environments in these varies. Understanding what factors drive food consumption is important because they influence the nutritional quality of the diets people purchase, cook and consume. Hence a range of disciplinary perspectives are required, including agriculture, anthropology, behavioural science, economics, geography, nutrition, psychology, public health and sociology(Reference Stok, Hoffmann and Volkert16).
Dietary behaviour frameworks that come from a public health perspective tend to use a socio-ecological approach, which has a long history in health promotion(Reference Stok, Hoffmann and Volkert16, Reference Story, Kaphingst and Robinson-O'Brien17). They encompass the importance of social inequalities in health and the need to acknowledge the crucial role of wider contextual socio-economic factors and sex(Reference Richard, Gauvin and Raine18, Reference Dahlgren and Whitehead19). They acknowledge the complexity of health behaviours and aim to disentangle the way people's lives are connected with their environments at multiple levels(Reference Story, Kaphingst and Robinson-O'Brien17, Reference Richard, Gauvin and Raine18). These frameworks draw on Dahlgren–Whitehead's ‘rainbow model’(Reference Dahlgren and Whitehead19), which mapped the relationship between the individual, their environment and health, placing individuals at the centre, surrounded by levels of influence: lifestyle, social and community networks, living and working conditions, and general socio-economic, cultural and environmental conditions.
All socio-ecological dietary behaviour frameworks are based on a similar structure, usually including four levels. The example we detail here (Fig. 1) summarises the evidence of factors influencing dietary behaviours from the African context(Reference Gissing, Pradeilles and Osei-Kwasi20). At the individual level, personal factors are included that can impact on food consumption through cognitive factors (motivation, self-efficacy and skills/competencies)(Reference Story, Kaphingst and Robinson-O'Brien17). Three environmental levels are then proposed to influence dietary behaviours at the social, physical and macro-level. The social environment encompasses social interactions with friends, families, neighbours and others. Story postulates that this influences dietary behaviours through role modelling, social norms and social support. The physical food environment captures the settings where people may produce/purchase/acquire food, cook and eat/drink, such as the local neighbourhood or home, or where people work. These physical settings influence the accessibility and availability of healthy and unhealthy foods. Macro-level environmental factors (such as marketing and advertising policy, food prices, trade) have an important influence on dietary behaviours, but there is less published evidence for them in Africa than the other levels(Reference Gissing, Pradeilles and Osei-Kwasi20), probably because they are more distal, making them harder to investigate.
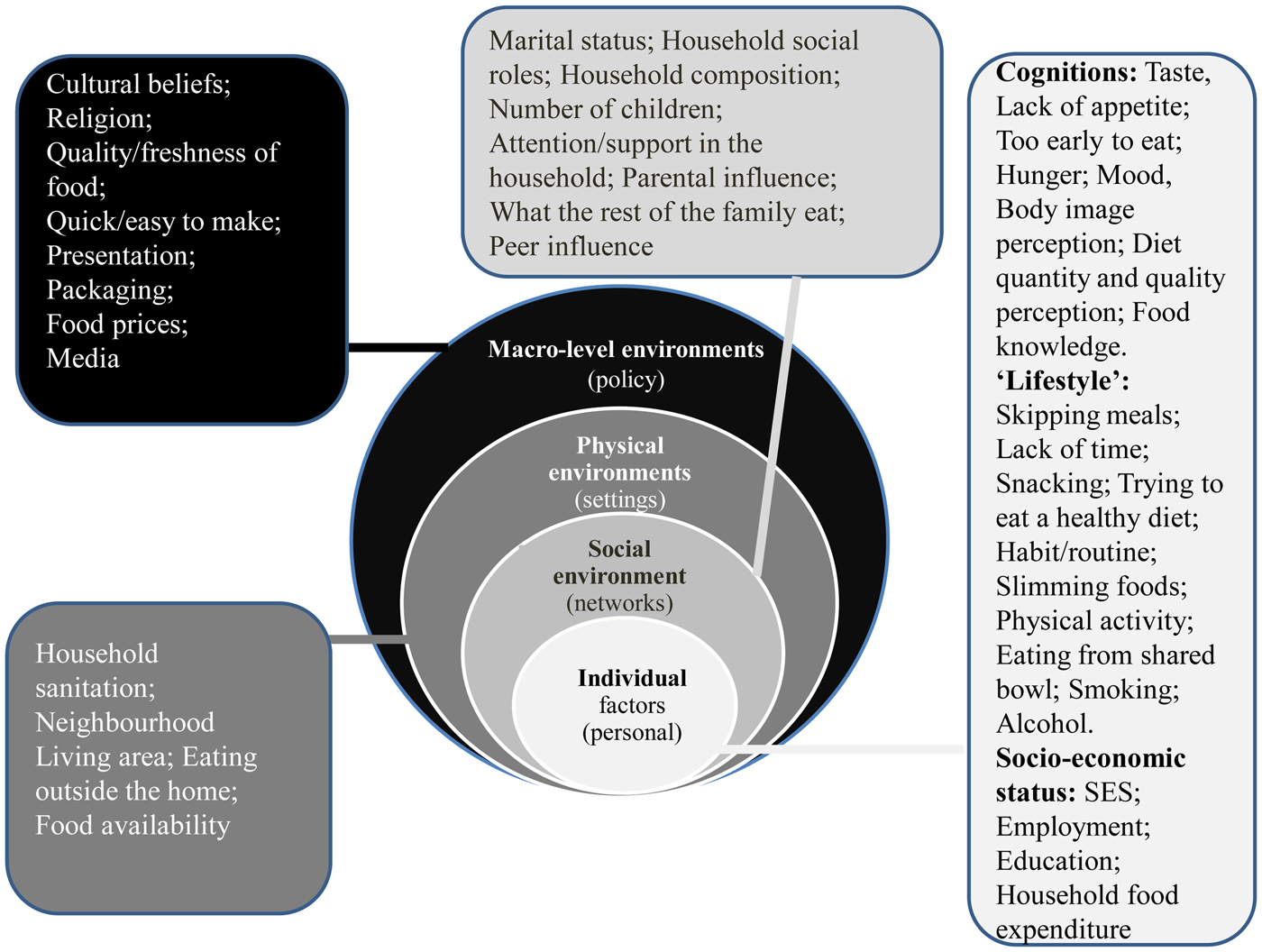
Fig. 1. (Colour online) Factors influencing dietary behaviours in Africa (evidence from urban studies of women; adapted from Gissing et al.)(Reference Gissing, Pradeilles and Osei-Kwasi20).
Socio-ecological approaches postulate that factors in these four levels all interact in different ways to then influence dietary behaviours. This is similar in many ways to a systems approach(Reference Carey, Malbon and Carey21), which has also been proposed in public health to summarise the inter-relation of different factors influencing dietary behaviours(Reference Holdsworth, Nicolaou and Langoien22, Reference Butland, Jebb and Kopelman23) and physical activity behaviours(Reference Chastin, De Craemer and Lien24, Reference Condello, Ling and Bianco25) because it acknowledges that factors within the levels are not static, but that there are connections between clusters within a dynamic system(Reference Homer and Hirsch26). Systems approaches can be useful for improving public health because even though some shifts in behaviours only have a small impact on individuals, when combined they have the potential to stimulate population changes(Reference Rutter, Savona and Glonti27). There is a lack of evidence about the causal pathways through which different factors influence dietary behaviours in Africa(Reference Gissing, Pradeilles and Osei-Kwasi20) and globally(Reference Story, Kaphingst and Robinson-O'Brien17), which makes the production of a systems map challenging(Reference Holdsworth, Nicolaou and Langoien22, Reference Chastin, De Craemer and Lien24). Data science may offer the opportunity to provide the much needed evidence for a systems approach by leveraging big data, which if combined with traditional data could shed light on the wider determinants of dietary behaviours across multiple levels(Reference Morris, Wilkins and Timmins28).
Social food environments
Examining how food consumption is embedded in everyday life in Africa, by investigating what factors drive consumption in social environments is crucial to developing effective interventions that account for these. Dietary habits are structured and organised in social practices(Reference Shove, Pantzar and Watson29), such as when/where food and beverages are eaten, how quickly and with whom, so they have an important influence on food decisions. Within the social food environment, we can include the role of family, friends, peers and role models on dietary behaviours, as well as the social support that individuals receive for their dietary choices and the social norms in their social networks that inform expectations.
There is a lack of evidence about how social environments drive dietary habits in African cities, as most research has focused on individual-level drivers(Reference Gissing, Pradeilles and Osei-Kwasi20). Studies from outside Africa(Reference Robinson, Blissett and Higgs30, Reference Powell, Wilcox and Clonan31) suggest that mirroring dietary practices as a way of pleasing others or signalling identity and norms are important drivers of food choice. One study in South Africa found that ‘what the rest of my family will eat’ was an important influence on food choice(Reference Charlton, Brewitt and Bourne32). Other evidence from Africa found that marital status and women's household social status influenced the nutritional quality of diets, fattening practices or snacking habits during food preparation(Reference Gissing, Pradeilles and Osei-Kwasi20). Indeed, sex has been linked to food choice in many societies. The social environment seems to be particularly important for adolescents, including sharing food with family and mirroring of friends’ dietary behaviour.
Body size norms in Africa are a potentially important factor driving eating habits, particularly for women, with a preference for overweight observed in some African countries, associated with social status and economic success. One mixed methods study that encompassed urban Senegal (Dakar) conducted qualitative interviews and a quantitative survey of adults, and reported that overweight was socially valued and seen as a symbol of wealth and integration into the city for those that had migrated from rural Senegal(Reference Cohen, Gradidg and Ndao33).
Physical food environment
The physical environments that may influence dietary intake includes different settings where people eat or buy foods(Reference Story, Kaphingst and Robinson-O'Brien17). These settings include home, work, schools, retail food stores and eating out food outlets. In most studies, the physical environment is characterised using geographic measures (e.g. proximity, density, variety) using geospatial data (e.g. Geographical Information System, distance measurements).(Reference Herforth and Ahmed34–Reference Townshend and Lake39) Most such studies have been conducted in high-income countries(Reference Caspi, Sorensen and Subramanian36, Reference Pitt, Gallegos and Comans38, Reference Townshend and Lake39), with a few in African cities (mainly in South Africa), where they have focused on the school, retail and eating out-of-home environments.
School environment
School environments have the potential to influence children's diets in a number of ways, from foods served in/near schools, food sold in tuckshops and the hidden curriculum of how foods and advertising can pervade classroom teaching. A study conducted in ninety South African primary schools located in poor settings reported that fruit was on the menu of only 28 % of schools and was served in only 4 % on the day of the survey(Reference Faber, Laurie and Maduna40). The same study reported that most food vendors based within/outside schools sold unhealthy foods, such as chips, sweets or biscuits and that only 19 % of schools had a policy about foods sold in schools(Reference Faber, Laurie and Maduna40). Other studies in urban South African primary schools(Reference Wiles, Green and Veldman41, Reference Abrahams, de Villiers and Steyn42) concluded that poor food purchasing practices may contribute to childhood overweight/obesity, as pupils who purchased food items from school tuckshops had a higher BMI compared with those who did not. Amongst adolescent South Africans living in Soweto, the majority (85 %) purchased food from school vendors and about two-thirds of these were unhealthy (sweets, sweetened beverages, crisps, fried chips and white bread)(Reference Feeley, Musenge and Pettifor43).
Retail food environment
In Africa, the informal food sector plays an important role in the retail food environment. However, most studies have focused on the impact of supermarkets on dietary behaviours. In sub-Saharan Africa, the first supermarkets were established in Southern and Eastern Africa in the early 1990s(Reference Reardon and Gulati44), particularly in South Africa and Kenya(Reference Reardon, Timmer and Barrett45). In the Southern African region, the growth in supermarket share of retail sales has increased rapidly from 10 to 50–60 % between the 1990s to mid-2000s(Reference Reardon and Gulati44). In Western Africa, the development of supermarkets only began in the 2000s. In most sub-Saharan African countries, the supermarket share of retail is still relatively low, but it is increasing. When supermarkets are first established, the main foods sold tend to be dry, processed and packaged foods; but with time fresh products are sold (e.g. meat, fruit or vegetables)(Reference Reardon, Timmer and Barrett45).
In African cities, supermarkets establish first in high-income neighbourhoods followed by lower income areas, enabling access to supermarkets to poor urban households(Reference Battersby and Crush46). However, a survey conducted in Cape Town, South Africa, reported that supermarkets in low-income neighbourhoods sold less healthy foods, potentially impacting negatively on diets of the urban poor(Reference Battersby and Peyton47). A study conducted in three Kenyan towns amongst adults reported that individuals purchasing foods in supermarkets had significantly higher BMI compared with those who did not(Reference Demmler, Klasen and Nzuma48). The same study also reported that individuals who purchased foods in supermarkets consumed more energy, and had higher intakes of energy from processed meat, highly processed foods, dairy and vegetable oils(Reference Demmler, Ecker and Qaim49–Reference Kimenju, Rischke and Klasen51). Contrary to this, a study in North Africa (Tunis) reported that individuals doing most of their food shopping at supermarkets had a significantly (albeit small) higher overall diet quality(Reference Tessier, Traissac and Maire52, Reference Kim, Haines and Siega-Riz53). In West Africa, a study conducted in three poor neighbourhoods of Accra, Ghana inventoried three different sales points of foods using global positioning system(Reference Dake, Thompson and Ng54). The study reported that out-of-home cooked foods sales points (that mainly sell rice-based dishes and local staple foods) outnumbered other kind of sales points, i.e. convenience stores (that mainly sell processed and pre-packaged foods) or fruit and/or vegetables sales points, which were the least common.
Eating out-of-home environment
A study conducted in 2009–2010 amongst Moroccan women of childbearing age living in the urban area of Rabat-Salé reported that women who ate out-of-home more frequently ate significantly less vegetables(Reference Landais, Bour and Gartner55). However, no distinction was made for the venue or type of food outlet. In Benin, street food was an important source of energy, providing 39 % of total daily energy intake of adolescents in the capital city, where it was also associated with lower fruit and vegetable intake(Reference Nago, Lachat and Huybregts56). A study in three poor areas of Accra reported that each additional out-of-home cooked foods sales points was associated with a significant decrease in individuals’ BMI(Reference Dake, Thompson and Ng54).
Macro-food environment
Macro-level environmental factors have an important influence on dietary behaviours. They include a wide range of factors (Fig. 1), some of which make up the ‘food system’ (food supply/production, food storage, transportation, food prices, food trade, food processing/transformation and food retailing) and the policies that shape them, including food and agriculture policies, economic and trade policy, political structures, food assistance, health and social support policy and marketing/advertising policy. Here we focus on evidence for some of these.
Food supply
Food supply data reflect the food available on a macro-environmental level. Food balance sheets from the FAO are a useful means to describe trends in food availability for human consumption as a gross proxy of food consumption. We divided Africa into the five FAO regions (Fig. 2). Food supply trends were analysed using food balance sheet data from 1961 to 2013 for energy supply and for foods that would be expected to shift over time, given evidence in other continents experiencing nutrition transition(57). For the African region, data suggest an increasing availability of energy, animal products (but the picture is complex), fruit and vegetables, vegetable oils, sugar and sweeteners but a decrease in availability of animal fats. There were inconsistent changes in cereal/pulses and alcohol availability across Africa.
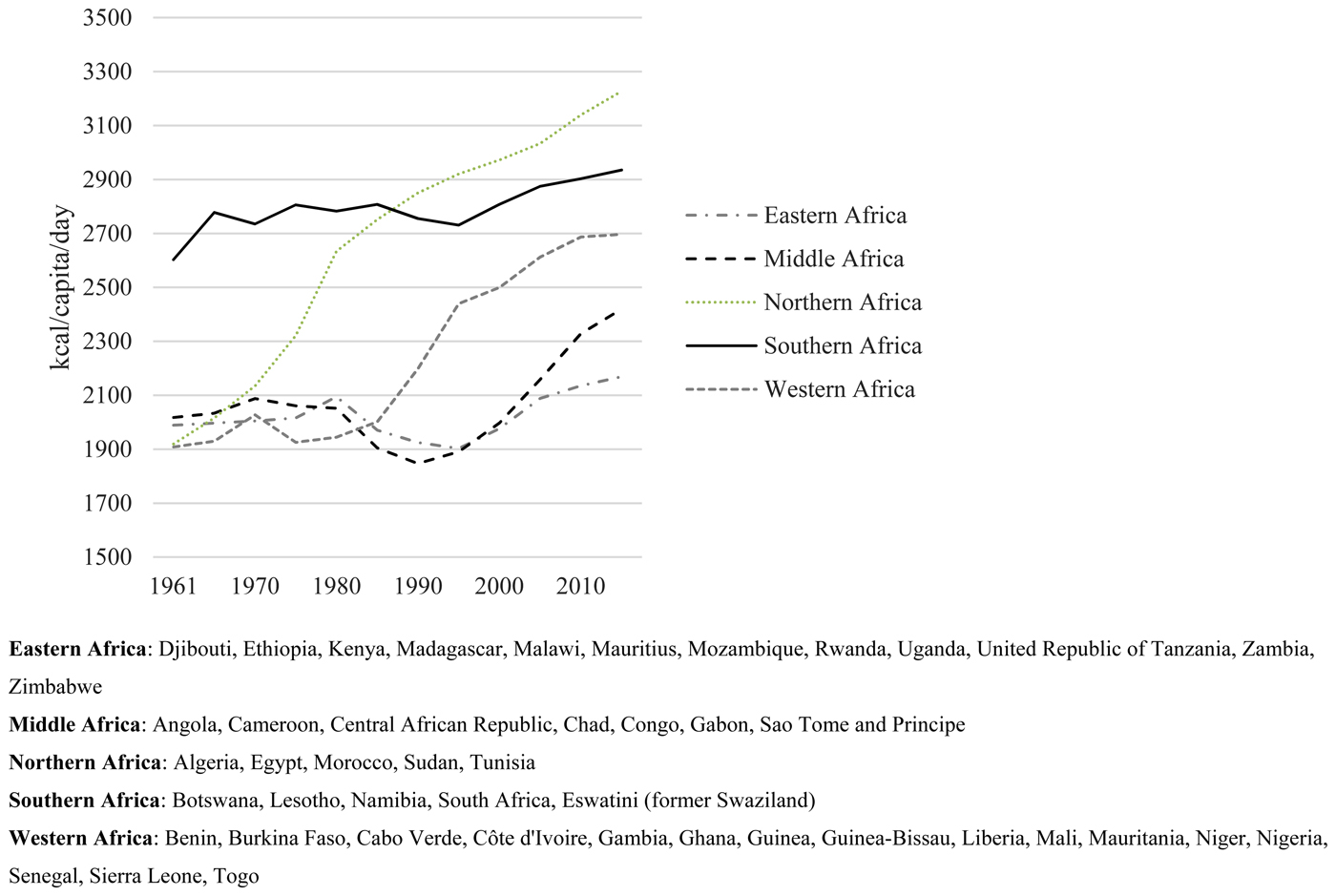
Fig. 2. Energy supply trends in African regions, 1961–2013, from FAO, 2017.
Energy (kJ (kcal)) availability increased in all five African regions (Fig. 2). The biggest increase was observed in Northern Africa, where it increased by almost 40 %, from 8033.3 (1920) to 13506 kJ (3228 kcal)/capita per d. For Western Africa, energy supply was quite stable until the mid-eighties but has since increased rapidly to 11284.2 kJ (2697 kcal)/capita per d. The same pattern was observed in Middle and Eastern Africa, but beginning later. Energy supply trends in Southern Africa were different as even though energy supply increased over time in this region, it was already high in 1961 (10891 kJ (2603 kcal)/capita per d)) and has not increased subsequently as much as the other African regions.
As has been described in high-income countries, supply of animal products has increased across Africa (meat, eggs, milk and dairy products, fish and seafood) (Fig. 3). Meat supply increased in Southern, Northern and Middle Africa, whilst it remained stable in Western and Eastern Africa (Fig. 3a). In Southern Africa, the increase and level of supply was highest, i.e. in 2013, it was more than twice the level for Northern and Middle Africa and almost three times that of Eastern and Western Africa. Eggs availability increased over the same period in Southern, Northern and Western Africa, with the fastest increase observed in Southern and Northern Africa (Fig. 3b). Contrary to what is usually described with the nutrition transition, the availability of milk and dairy products decreased in Southern Africa (from 64 to 57 kg/capita per year). The opposite was reported for Northern Africa, where the increase was the fastest and greatest. In Western and Middle Africa, milk and dairy products availability remained stable (Fig. 3c). Fish and seafood availability remained stable in Southern Africa, whilst it increased in other regions, particularly in Northern Africa (Fig. 3d).
Fig. 3. Animal products supply trends in African regions, 1961–2013, from FAO, 2017.
Cereals availability rose in all African regions except Southern and Eastern Africa (where they remained stable) (Fig. 4a). Pulses availability was highest in Eastern Africa compared with the other regions and remained stable (Fig. 4b). In Southern Africa, pulses availability, which was the lowest compared with the other regions in 1961 continued to gradually decrease until 2013 (from 5 to 3 kg/capita per d). In Middle, Northern and Western Africa, pulses availability increased, particularly in Middle and Western Africa.
Fig. 4. Plant-based products supply trends in African regions, 1961–2013, from FAO, 2017.
Vegetables availability was highest in Northern Africa and lowest in Eastern Africa. Contrary to what is usually described with the nutrition transition, vegetables availability did not decrease. Indeed, whilst it remained stable in Southern and Eastern Africa, it increased in the other regions. Once again, the greatest increase was in Northern Africa, where vegetables availability increased from 68 kg/capita per d in 1961 to 161 kg/capita per d in 2013 (Fig. 4c). Similarly, the expected trend for fruit consumption with the nutrition transition was not found for Africa, as fruit availability increased in all African regions at different rates and magnitude, with the greatest increase in Northern Africa (Fig. 4d).
Vegetable oils increased in every African region between 1961 and 2013, which is consistent with the trend that has been reported in other parts of the world with the nutrition transition (Fig. 5a). Animal fats remained overall stable and low (<1 kg/capita per d) in Eastern, Middle and Western Africa, whilst they sharply decreased in Northern and Southern Africa (Fig. 5b), which is inconsistent with what we would expect with nutrition transition. At first glance, these changes in oils/fats seem to be encouraging as they could lead to an improved profile of available fatty acids. However, food processing industries use a lot of hydrogenated vegetable oils in highly processed foods, which are often associated with salt and added sugar.
Fig. 5. Vegetable oil and animal fats supply trends in African regions, 1961–2013, from FAO, 2017.
Between 1961 and 2013, sugar and sweeteners’ availability increased across Africa except the Southern region, where it was already highest (Fig. 6a). In Eastern, Middle and Western Africa, availability was lowest but increased steadily. In Northern Africa, sugar and sweeteners availability was more than twice as high compared with Eastern, Middle and Western Africa in 2013. In Southern Africa, availability decreased until 2005 but then began to increase again. Whilst alcoholic beverages availability remained stable in Northern Africa, it increased in Middle, Southern and Western Africa, but decreased in Eastern Africa (Fig. 6b).

Fig. 6. Sugar and sweeteners, alcoholic beverages supply trends in African regions, 1961–2013, from FAO, 2017.
Food prices
Evidence of the impact of macro-level food prices on dietary behaviours in urban Africa comes from the 2008 food price crisis. One study(Reference Martin-Prevel, Becquey and Tapsoba58) assessed food price rises in urban Burkina Faso (Ouagadougou) of over 3000 households, finding that both food security and dietary diversity deteriorated when food prices increased. Even though households increased their food expenditure, this was not enough to mitigate the impact of food price rises. A second study of over 2000 households in Ethiopia(Reference Hadley, Linzerb and Belachewc59) also reported that the dramatic increase in food prices between 2005 and 2008 was accompanied by a decline of household food insecurity across urban (and rural) areas, concluding that wealth was the most important factor for whether households could weather external shocks, especially in urban areas but less so in peri-urban or rural areas. This seems to confirm to some extent, that poor urban dwellers are especially vulnerable to price shocks because they spend a large proportion of their budget on food. Moving beyond the impact of food price rises on diet to health outcomes, longitudinal analysis of thirty-one low- and middle-income countries, including some African countries, suggested that rising food prices have an impact on obesity prevalence in adult women from high socio-economic status groups, but there was no evidence that they impact on low-income groups(Reference Conklin, Daoud and Shimkhada60).
Food advertising and marketing
Systematic reviews of the role of food/beverage advertising on dietary behaviours targeting children globally have provided convincing evidence that advertising promotes energy-dense nutrient-poor foods and has a negative nutritional impact(Reference Cairns, Angus and Hastings61, Reference Sadeghirad, Duhaney and Motaghipisheh62). A meta-analysis of seventeen studies indicated that exposing children to unhealthy food and beverage marketing increases dietary intake and preference (to a lesser extent) for energy-dense, nutrient-poor food and beverages(Reference Sadeghirad, Duhaney and Motaghipisheh62). The rapid expansion of foods and beverages advertising in low- and middle-income countries is based on similar approaches to that of high-income countries, which threatens traditional food habits by introducing new food products(Reference Cairns, Angus and Hastings61). The use of celebrities and sports personalities is common, e.g. in South Africa(Reference Mchiza, Temple and Steyn63). Some studies in Africa have investigated the food advertising environment on television. For example, one study from South Africa(Reference Mchiza, Temple and Steyn63) found that 44 % of television adverts (15.00–21.00 hours) were related to food, of which 63 % were for food products, with unhealthy foods and sweetened drinks (and other hot drinks) most likely to be advertised. Particularly alarming was the finding that 21 % of adverts were for alcohol and two-thirds of these were within children/family viewing periods.
From a regulatory perspective, calls have been made for controls on marketing to children in Africa, as well as globally. However, food marketing continues to ‘target children as consumers in their own right, and as intermediaries who can influence other consumers especially their parents and peers’(Reference Cairns, Angus and Hastings61). The WHO, endorsed by the World Health Assembly, has developed recommendations to facilitate the reduction in marketing to children of unhealthy foods/beverages (defined as high in free sugars, salt, saturated fats or trans-fatty acids)(64). Introducing such controls on marketing policy will be a challenge in the African context, as they are globally.
Food trade
Liberalisation of food trade is a crucial element of food systems at different geographical scales, which has impacted on the nutritional quality and range of food available in people's food environments, by opening up domestic markets towards international trade and investment, including provision and advertising from transnational food corporations(Reference Friel, Hattersley and Snowdon65). Urban residents in Africa are most likely to be exposed to these food imports, although the urban poor can usually only access food and beverage products of a lower nutritional quality(Reference Schram, Labonté and Sanders66), which may be energy dense and nutrient poor. Schram et al.(Reference Schram, Labonté and Sanders66) conducted an empirical modelling study in sub-Saharan Africa investigating the relationship between globalisation, economic growth and CVD outcomes (metabolic risk factors and deaths attributable to CVD), finding that trade and investment liberalisation impacted on CVD outcomes. A systematic review(Reference Barlow, McKee and Basu67) yielding seventeen quantitative studies (including evidence from Africa) found consistent evidence that trade agreements were associated with increased consumption of sugar-sweetened beverages and processed foods.
What are the implications for policy and interventions in Africa?
Interventions that tackle the individual-level have limited success when they do not account for the wider contextual factors that drive food consumption in an individual's social, physical and macro-environments(Reference Story, Kaphingst and Robinson-O'Brien17, Reference Mackenbach, Rutter and Compernolle68). Many decisions about food consumption are habitual and understanding the social, physical and macro-environments that drive these routines is crucial to identifying effective interventions to promote healthier diets. Therefore, interventions to support healthier food environments need to be developed across all levels, which would enhance their reach because dietary behaviours will vary between individuals. Developing effective interventions will require engagement from a wide range of stakeholders (Table 1), emphasising the need for cross-sectoral interventions across different food environment levels.
Table 1. Interventions and stakeholders at different environmental levels and stakeholders needed
Acknowledging the socially embedded nature of dietary behaviours is crucial. Interventions in the social environment appear to be particularly effective in shifting social norms in culturally homogenous contexts(Reference Powell, Wilcox and Clonan31). Interventions that involve existing social networks, such as community peer support groups (e.g. women's groups) and community groups (e.g. churches or mosques) offer ideal opportunities to promote healthy eating and its nutritional advantages in the African context.
Interventions in the physical environment are likely to require policy and regulations. Evidence globally suggests that policy levers at the macro-level are likely to be most effective(69). Interventions to address macro-level environments target policies by guiding choice through changing default policy, incentives and disincentives and by eliminating choice. Because personal freedom is potentially reduced if interventions involve removing choice (due to potential increasing conflict and intrusion), greater evidence may be needed to justify interventions and policies at the macro-level to convince policy makers to implement them(69). Macro-level policies are notoriously difficult to implement, and they will require committed leadership in government and effective governance and infrastructure from African governments.
What are the implications for research in Africa?
Research methods for investigating food environments
Research across the different food environment levels will require a range of interdisciplinary studies using mixed or multiple methods involving qualitative and quantitative research (Fig. 7). Qualitative methods will be especially useful for shedding light on the social processes that drive behaviours in the social environment. Quantitative research methods will be especially useful for mapping the physical food environment. Research on the macro-environment is likely to use both quantitative and qualitative methods. Lytle and Sokol(Reference Lytle and Sokol37) conducted a systematic review of the methods used in food environment research, reporting that geographic analysis was most commonly used and all studies were quantitative. The review included studies on physical and macro-level food environments only, but the authors acknowledge the importance of social factors in mediating the choices individuals make when faced with physical and macro-food environments. Public health nutritionists will need to work with experts from a range of disciplines to undertake food environment research, including sociologists and anthropologists (social environment); health geographers, demographers and economists (physical environments); and political scientists and economists (macro-environment), amongst others.
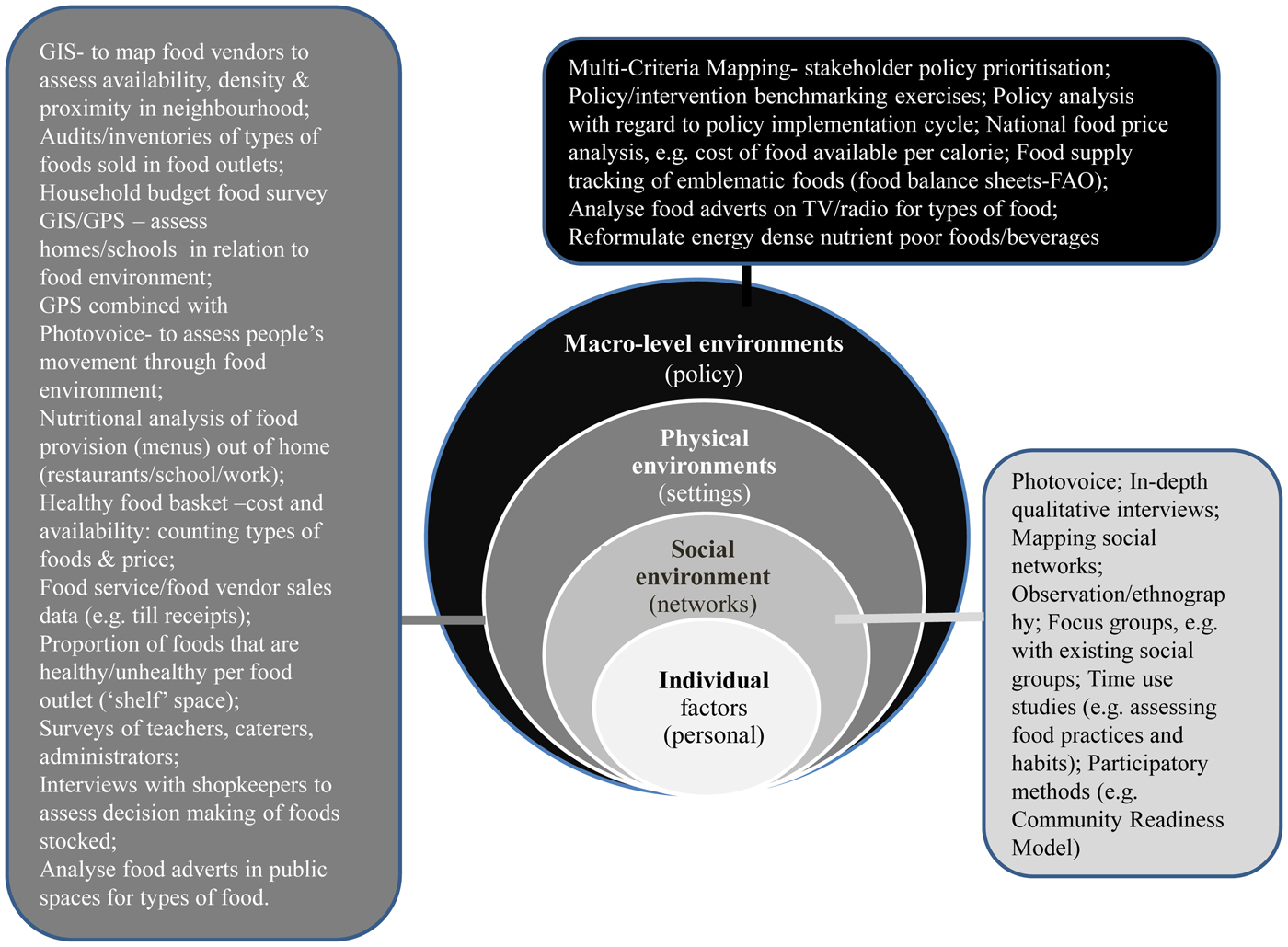
Fig. 7. (Colour online) Research methods for investigating the food environment at different levels. GIS, Geographical Information System; GPS, Global Positioning System.
Research priorities for healthy urban food environments
An Africa-wide stakeholder consultation reported that African researchers prioritise the need for more research on community-level neighbourhoods that create an environment that prevents malnutrition (acknowledging the physical food environment, especially environmental sanitation) and the cultural and macro-environment suggesting the need for social protection programmes and safety nets, which would counter concern about food prices(Reference Holdsworth, Kruger and Nago70, Reference Lachat, Nago and Roberfroid71). Shifting research away from individual-level drivers of food choice to food environments will need increased capacity development for competency in the range of research methods that can be used to explore food environments (Fig. 7).
Research on food environments needs to be sensitive to all forms of malnutrition, as a nutritionally adequate diet in terms of macro- and micro-nutrients is the common goal to prevent all forms of malnutrition. Hence, research needs to focus on all forms of malnutrition, including the inter-relationships between them, acknowledging the social and physical environments that drive people's dietary habits.
This review has highlighted a number of important research gaps that need addressing to shed light on the role of urban food environments in Africa, which will require a range of in-depth qualitative and longitudinal quantitative studies to answer the following: (1) How have diets changed over time and how does this differ across population groups, e.g. socio-economic groups, age and sex and different geographies (cities, towns and peri-urban contexts, countries and regions in Africa)? Africa is vast and diverse and there are a range of urban contexts within and between countries. (2) How do factors in the different environmental levels interact to shape dietary behaviours? Particularly how does the social environment and habitual social practices mediate dietary behaviours in urban Africa? (3) What are the common drivers of malnutrition (in all its forms) in urban African environments and which policies/interventions can be developed, supported and implemented by a range of stakeholders to best address these most cost-effectively without widening social inequalities?
Conclusions
Improving African food environments represents a pressing public health concern and has the potential to prevent all forms of malnutrition. For the African region, data over a 50-year period suggest an increasing availability of energy, animal products (but is heterogeneous), fruit and vegetables, vegetable oils, sugar and sweeteners but a decrease in availability of animal fats. There have been inconsistent changes in cereal/pulses and alcohol availability across Africa in the same period. Contrary to what is usually described with the nutrition transition, vegetable and fruit availability has not decreased.
A range of models and frameworks have been developed in order to understand why people eat what they do and the role of food environments in these varies. Understanding what factors drive food consumption is important because they influence the nutritional quality of the diets people purchase, cook and consume. Dietary behaviour frameworks that come from a public health perspective tend to use a socio-ecological approach but systems approaches offer future potential.
Interventions that tackle the individual-level have limited success when they do not account for the wider contextual factors that drive food consumption in an individual's social, physical and macro-environments. Many decisions about food consumption are habitual and understanding the social, physical and macro-environments that drive these routines is crucial to identifying effective interventions to promote healthier diets. Interventions in the physical environment are likely to require policy and regulations. Evidence globally suggests that policy levers at the macro-level are likely to be most effective. Interventions to address macro-level environments target policies by guiding choice through changing default policy, incentives and disincentives and by eliminating choice. However, introducing controls on marketing policy will be a challenge in the African context, as they are global. Research across the different food environment levels will require a range of interdisciplinary studies using mixed or multiple methods involving qualitative and quantitative research. Qualitative methods will be especially useful for shedding light on the social processes that drive behaviours in the social environment. Quantitative research methods will be especially useful for mapping the physical food environment. Research on the macro-environment is likely to use both quantitative and qualitative methods.
Hence, by conducting research into the role of urban social, physical and macro-environments, emerging interventions/policies and research are likely to positively impact on nutritional status, thereby enhancing social and economic development.
Financial Support
None.
Conflict of Interest
None.
Authorship
The authors had joint responsibility for all aspects of preparation of this paper.








