


INTRODUCTION
Leptospirosis is a zoonotic bacterial disease affecting most mammalian species. In New Zealand (NZ), up to 81% of adult deer herds, 97% of adult beef cattle herds, and 97% of adult sheep flocks have seropositive animals [Reference Dreyfus1, Reference Ayanegui-Alcerreca2]. The two most frequent serovars in cattle, deer and sheep in NZ are Leptospira borgpetersenii serovar Hardjo (Hardjo) and Leptospira interrogans serovar Pomona (Pomona) [Reference Ayanegui-Alcerreca2–Reference Marshall and Manktelow4]. Animal-level prevalence to either of these serovars was shown to be as high as 50% (sheep), 58% (beef) and 60·8% (deer) in the pastoral dry-stock population [Reference Dreyfus1, Reference Ayanegui-Alcerreca2].
In NZ, livestock appear to be the main source of human leptospirosis, with farmers and meat workers being most at risk [Reference Thornley5]. Whereas almost all dairy farmers vaccinate their stock against leptospirosis and the NZ pig industry has introduced compulsory vaccination of pig herds [6], less than 10% of deer, sheep or beef farmers are currently using vaccination [Reference Wilson7, Reference Keenan8].
NZ is classified as having a moderate incidence of human leptospirosis in the Asia Pacific region (1–10/100 000) [Reference Victoriano9]. From 2006 to 2010, 427 clinical cases of leptospirosis were notified (86·4% laboratory confirmed), an average annual risk of 2 cases/100 000 total population. Of those with occupation recorded (91%), 52% (range 36–71% annually) were farmers or farm workers and 30% (range 18–48% annually) abattoir workers or butchers [10]. Consequently, the risk for meat workers and farmers of contracting leptospirosis was very much higher than in the general population. The reported infection risk may vary geographically. The highest rates in 2010 were reported in West Coast (18·3/100 000 population, six cases), followed by Whanganui (12·7/100 000, eight cases), Mid-Central (7·8/100 000, 13 cases), and Hawke's Bay (7·1/100 000, 11 cases) [11]. However, due to underascertainment these numbers may not represent the true incidence. Leptospira species and serovars were recorded for 67% of cases on average, of which 41% tested positive against Hardjo, 24% against L. borgpetersenii serovar Ballum (Ballum), 19% against Pomona and 16% against other serovars. Leptospirosis can result in severe human illness but is rarely fatal in NZ. In 2005 2·3/100 000 leptospirosis cases were notified [12] and on average 69 persons were hospitalized per year due to leptospirosis between 2003 and 2005 [12–Reference Vickery15]. Numbers reported by passive public health surveillance mainly represent severe clinical cases, and milder forms are believed to remain unreported [Reference Thornley5].
In the last four decades, three cross-sectional studies investigated Leptospira seroprevalence in meat workers slaughtering pigs, sheep, and/or cattle in NZ (n = 242, n = 567 and n = 1248, respectively) [Reference Blackmore, Bell and Schollum16–Reference Dreyfus19] estimating seroprevalences against Pomona, Hardjo, and/or L. borgpetersenii serovar Tarassovi of between 3·2%, 4·7% and 5·4% (Pomona), 1·4%, 4·1% and 9·2% (Hardjo) and 0·4% (Tarassovi). However, no longitudinal study on Leptospira incidence in NZ in general and in abattoirs specifically has been conducted; hence the true rate of new infections and their association with mild or severe clinical leptospirosis in any occupational group and the potential economic impact was unknown.
The aims of this study were therefore to determine the annual risk of infection, the associated incidence of confirmed or suspected clinical leptospirosis and the proportion of influenza-like illness (ILI) attributable to Leptospira.
METHODS
Study design, data collection and management
We conducted a cohort study among meat workers from eight purposively selected abattoirs comprising four sheep [one (‘Sheep 1’) studied twice and three studied once], two beef and two deer abattoirs in NZ. The two deer abattoirs were located in the South Island and the sheep and beef abattoirs were in the North Island. The vaccination status of animals being slaughtered was unknown. Abattoir managers, health and safety personnel, meat union representatives and workers were provided with information about the study aims and sampling procedure. Participation was, of necessity, voluntary rather than based on random sampling. To estimate the rate of new infection with Leptospira, sample and data collection occurred twice, at intervals ranging from 50 to 61 weeks. Participating meat workers were blood sampled by certified phlebotomists and interviewed at each blood sampling by trained researchers using a questionnaire (see online Supplementary material). The first blood sample was used to establish the antibody titre status against Pomona and Hardjo and the second determined whether or not a worker was infected during the study period, as described below. Study participants of ‘sheep abattoir 1’ were sampled the first time between February and April 2008 and the second time in April 2009. All abattoirs were sampled initially in November 2009–March 2010, and again in November 2010–May 2011. A participation ‘rate’ was calculated as the study population divided by the entire workforce of an abattoir.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures were approved by the Massey University Human Ethics Committee in 2008 and 2009 (Southern A, application 05/123 and 09/08).
Sample size estimation
To detect a relative risk (RR) of 2·5 for new infections, and to achieve 80% power with 95% confidence, 280 meat workers had to be sampled twice. The number was doubled to consider a design effect due to sampling at several abattoirs [Reference Dohoo, Wayne and Stryhn20].
Serological testing
Ten millilitres of blood were collected into Becton Dickinson Vacutainer® Plus tubes (BD, USA), coated with silicone and micronized silica particles to accelerate clotting, stored between 4 °C and 10 °C in a mobile refrigerator, and couriered within 24 h in an icepack-cooled Bio-Bottle™ (Bio-Bottle New Zealand Ltd) to the mEpiLab at Massey University in Palmerston North, NZ. After centrifugation at 3000 rpm for 6 min, the serum was aliquoted into duplicate cryovials and microtitre plates and stored at −80 °C.
The microscopic agglutination test (MAT) was used to measure serum antibodies against Pomona and Hardjo at doubling dilutions from 1:24 to 1:1536 as described previously [Reference Faine21]. The MAT was always performed by the same trained laboratory technician. To measure seropositivity, a titre cut-off of ⩾1:48 was used to declare that a worker was previously exposed to leptospires [Reference Faine21, Reference Shivakumar and Krishnakumar22]. Seroconversion occurred where a seronegative worker (<1:48) had a MAT titre increase by at least two dilutions, hence from 0 to ⩾1:48, or from 1:24 to ⩾1:96. If an initially positive MAT titre increased by at least two dilutions between the first and second sampling, the worker had an anamnestic response, for example a titre change from 1:48 to 1:192.
Study population and case definitions
The study population comprised all workers who were sampled at least twice. Some workers (n = 57, 9·6%) in abattoir Sheep 1 were sampled over two study periods, hence their infection rates were measured twice (up to four blood samples per participant). All workers who were seropositive (a MAT cut-off ⩾1:48) at the beginning of the sampling period were retained in the study population, as they remained at risk of becomimg infected with another Leptospira serovar or re-exposed to the same serovar, the latter being called an ‘anamnestic response’.
Cumulative incidence: a worker who either seroconverted or who had an anamnestic response against Pomona and/or Hardjo between the first and second sample was defined as newly infected and contributed to incidence. The incidence of workers reporting ILI between sampling dates was compared between seroconverting and anamnestic response groups to provide evidence for the assumption that both definitions equally indicated a new infection episode. The cumulative incidence was adjusted to 365·25 days for each abattoir assuming that the risk for infection was constant.
Probable clinical leptospirosis was determined as a worker reporting having been diagnosed with leptospirosis of any serovar by a health professional between the two sampling times, on the basis of clinical symptoms with or without confirmation by laboratory test.
Possible clinical leptospirosis was determined as a worker reporting to have had an ILI and having seroconverted or showed an anamnestic response between the two sampling times but without confirmation by a health professional, and not being in the above category.
Influenza-like illness was defined as an event of illness associated with fever, headache, arthralgia, myalgia, lethargy, nausea/vomiting and/or photosensitivity and includes the above two categories. It was explained to workers that the symptoms had to be severe enough that they felt like going home to rest.
Data analysis
Questionnaire information and serological test results were entered into an Access database and analysed using Microsoft Excel (Microsoft Corp., USA), Stata v. 10 (StataCorp, USA) or SAS (SAS Institute Inc., USA). Accuracy of data entry was validated by randomly selecting 5% of the questionnaires from each abattoir and comparing them with manual questionnaire entries.
Exploratory data analysis was conducted using histograms, 2 × 2 tables and summary measures.
Outcomes and exposure
The four outcomes of interest were (i) a ‘new infection’ with Hardjo and/or Pomona (by seroconversion or anamnestic response), (ii) an episode of ‘probable clinical leptospirosis’, or (iii) ‘possible clinical leptospirosis’ between samplings, and (iv) whether a worker experienced an ILI. The latter (iv) included outcomes (ii) and (iii).
Workers were asked about their age, gender and ethnicity. Of further interest was how many days they were absent from work with an ILI (see Supplementary material).
New infection risk and titre duration
The abattoir-specific cumulative annual incidence or risk of infection (%) was calculated as the number of new infections with Hardjo and/or Pomona divided by the sum of days between samplings of all participating workers and multiplied by 365·25. Confidence intervals were calculated by the Fleiss method [Reference Fleiss23]. The difference between the infection risk of meat workers slaughtering different species was analysed by χ 2 test. Since participation was voluntary, it was likely that a sampling bias had been introduced. Therefore, the cumulative annual incidence was corrected by weighting the distribution of workers in different work positions in the sample by the distribution in the entire workforce. This was necessary since a parallel analysis revealed that workers from highly exposed work positions were more likely to participate [Reference Dreyfus24] (Table 1).
Table 1. Percentage of abattoir-specific annual infection risk (or cumulative incidence) with Leptospira interrogans serovar Pomona (Pom) or Leptospira borgpetersenii serovar Hardjo (Har)

CI, Confidence interval.
* Abattoir Sheep 1 took part in the study in two consecutive years; 57/160 (35·6%) persons participated twice.
† To adjust for sampling bias due to voluntary sampling, the incidence was adjusted by weighting the distribution of workers in different work positions in the sample by the distribution in the entire workforce.
Crude associations between the risk of infection with Hardjo and/or Pomona and demographic exposure variables (listed in Table 2) were calculated for sheep abattoir workers by bivariable logistic regression.
Table 2. Frequencies of clinical and demographic risk factors and their unconditional association with new infection with Leptospira interrogans serovar Pomona and/or Leptospira borgpetersenii serovar Hardjo in sheep abattoir workers (n = 384)
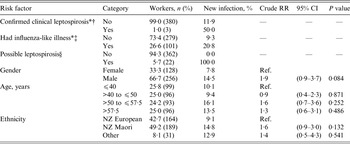
RR, Relative risk; CI, confidence interval.
* Not included in the logistic regression model, as it was an intermediate variable between exposure and antibody level.
† n = 383.
‡ n = 380.
§ Not included in the logistic regression model, as it includes the outcome.
In order to increase sample size and power, 57 persons from abattoir Sheep 1 participated twice in the study (they had been sampled in 2009 in a pilot study). Therefore, over-dispersion was estimated to decide whether adjustment for clustering due to repeated measurements was required in the analysis. Over-dispersion was declared present if the ratio between the residual Pearson χ 2 and residual degrees of freedom was >1·5 [Reference McDermott and Schukken25].
The duration of the antibody titre (D) over the threshold of 1:48 following infection of sheep abattoir workers was derived from the relationship between the mean seroprevalence at first sampling (P) and the mean study period incidence for serovars Pomona or Hardjo ( i ) as described in Dohoo et al. [Reference Dohoo, Wayne and Stryhn26]. Hence, the duration of the antibody titre is the average time a sheep meat worker took between having a MAT titre >1:48 and returning to a titre <1:48 following a typical infection episode. It was calculated as follows:
 $${{D}_i} = \displaystyle{{{{P}_i}} \over {\left( {1 - {{P}_i}} \right) \cdot {{I}_i}}}$$
$${{D}_i} = \displaystyle{{{{P}_i}} \over {\left( {1 - {{P}_i}} \right) \cdot {{I}_i}}}$$
Illness and population impact
The incidences of confirmed and probable clinical leptospirosis cases were calculated. The frequency, serological status and time away from work were described. To evaluate whether Leptospira antibody titres were higher for workers with influenza-like symptoms, compared to those without, we performed the Wilcoxon rank-sum (Mann–Whitney) test.
Population impact estimators were limited to workers from the four sheep abattoirs as they constituted the largest part of the sample providing adequate statistical power. The attributable risk (AR), which is the risk of ILI in persons who seroconverted/had an anamnestic response minus the risk of ILI in those who did not seroconvert/had an anamnestic response, was calculated [Reference Dohoo, Wayne and Stryhn26]. The average annual risk of experiencing influenza-like symptoms due to infection with Leptospira in sheep abattoirs was estimated by subtracting the risk in the unexposed group from the risk in the total population (population attributable risk, PAR). The proportion of illness cases that could be attributed to a Leptospira infection (population attributable fraction, PAF) was calculated by dividing the PAR by the total risk [Reference Brady27]. Confidence intervals for PAF were obtained by using the method described in Brady et al. [Reference Brady27]. Confidence intervals for PAR could not be provided as a variance formula for PAR was not readily available in the literature.
The incidences of probable and possible clinical leptospirosis cases and the PAF were extrapolated to the total sheep abattoir worker population to estimate the impact of leptospirosis on the sheep abattoir workforce. For the estimation of the degree of under-ascertainment of officially notified leptospirosis cases, we compared the proportion of notified leptospirosis cases from the meat industry (n ~ 25 000 workers) between 2005 and 2010 (between 14 and 42 cases per year), with the proportion of possible and probable leptospirosis cases in the sheep abattoir worker population of this study [10].
The economic impact of absenteeism was calculated as the number of days away from work due to probable or possible leptospirosis.
RESULTS
The participation rate in the first sampling was on average 32% of all workers with a range of 11–61% between abattoirs. At the first blood sampling 809 workers participated but 217 (27%) were lost to follow-up, i.e. the second sample, resulting in a final study population of 592 workers. Reasons for loss to follow-up were: 54 withdrew from the study (mainly for fear of pain at sampling), one died, one was on maternity leave, two were not released from their work position during sampling, 67 had already left work for the day and were unavailable, 29 had left employment at the abattoir or were laid off for the season, and 63 were absent for unknown reasons. Fifty-seven workers from abattoir Sheep 1 of a total of 592 workers from all abattoirs (9·6%) participated over both years and were hence sampled four times.
The number of participating workers per abattoir ranged from 21 to 135 (sheep), 58–100 (beef) and 18–32 (deer) with a total of 384 sheep, 50 deer and 158 beef abattoir workers (Table 1). The seroprevalence against Hardjo and/or Pomona measured at the first sampling was on average 13% in sheep, 17% in deer and 5% in beef abattoir workers. The seroprevalence against Hardjo measured at the first sampling was on average 8·6% in sheep, 14% in deer and 4·9% in beef abattoir workers. The seroprevalence against Pomona measured at the first sampling was on average 7·1% (sheep), 5·3% (deer) and 4·9% (beef) [Reference Dreyfus19].
Sixty-one from 1148 randomly chosen questionnaires were evaluated for data-entry errors. Each questionnaire contained at least 70 questions. We found 11 entry errors, hence the error rate was 11/(70 × 61) = 0·002%. Thus, an estimated 99·8% entries were correct, and this was deemed acceptable.
The over-dispersion factor was <1, hence a variance adjustment for repeated sampling of the same worker in two subsequent years was not required.
Antibody titres, new infection and titre duration
Table 3 shows the proportion of workers in each category of antibody titre change from first to second sampling against Hardjo, Pomona or both. The titres against Hardjo and Pomona ranged for both serovars from 1:24 to 1:768, with a median of 1:96 for positive titres (1:48 to 1:768).
Table 3. Number and percentage of workers from each abattoir type who had each category of antibody titre changes against Leptospira interrogans serovar Pomona (Pom) and Leptospira borgpetersenii serovar Hardjo (Har) or against either of these two serovars between first and second sampling
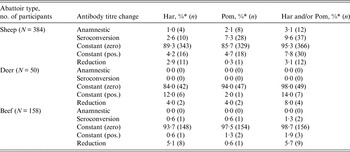
* Calculated as a proportion of N (species specific).
The ‘Har and/or Pom’ column does not have to sum the ‘Har’ and ‘Pom’ columns. It does sum up in the ‘Har and/or Pom’ column if an event occurs in one or the other group; however, if the event occurs in both groups as with constant zero, it will only be counted once in the ‘Har and/or Pom’ column.
Persons with the same antibody status between sampling are in the category ‘constant (pos.)’, those which remain negative in the ‘constant (zero)’ category and those who had a declining antibody titre are summarized under ‘reduction’.
Thirty-nine seroconversions and 12 anamnestic responses against either Pomona and/or Hardjo were observed in 51 workers; i.e. 51 new infections during the study period. Three workers seroconverted or had an anamnestic response against both serovars.
Forty-nine of 51 newly infected workers were from sheep abattoirs and two from beef abattoirs. More seroconversions and anamnestic responses were against Pomona than Hardjo (37 vs. 15). Hence, a higher proportion of workers developed antibodies against Pomona than against Hardjo (9·4 vs. 3·6%, P = 0·02).
The annual abattoir-specific infection risk (cumulative incidence, %) with Pomona and/or Hardjo was on average 7·7% (range 0·0–16·4%). The annual infection risk was higher in sheep abattoir workers [11·9%, 95% confidence interval (CI) 8·5–14·8, range 8·4–16·4%], than in beef (1·2%, 95% CI 0·2–4·6, range 1·0–1·5%, P < 0·001) or deer (0·0%, 95% CI 0·0–10·9, P = 0·01) abattoir workers. The annual abattoir-specific infection risk (cumulative incidence, %) in sheep abattoir workers on average was higher for Pomona (9·5%, 95% CI 6·2–11·9, range 3·9–16·4%) than Hardjo (2·7%, 95% CI 1·9–5·7, range 0·0–6·4%) (Table 1).
The weighting of the sampling fractions revealed that the abattoir-specific cumulative incidence tended to have been overestimated (apart from one abattoir) due to sampling bias. Crude annual incidences compared to adjusted incidences in sheep abattoirs were as follows: 11·5% vs. 6·7%, 16·4% vs. 11·6%, 12·6% vs. 6·3%, 10·7% vs. 12·4% and 8·4% vs. 6·6% (Table 1).
Because of low/no numbers of newly or re-infected workers in the beef and deer abattoirs, associations between demographic exposure variables and new infections were only analysed for workers at sheep abattoirs. Table 2 presents new infection rates of workers at sheep abattoirs by serovar and exposure categories. Unconditional analysis did not render gender, age or ethnicity to be significantly and positively associated with the risk of a new infection (P > 0·05).
The average titre duration of antibodies, given the cut point 1:48, was estimated to be 10 months against Pomona and 29 months against Hardjo. This means, for example, that on average a sheep abattoir worker was expected to be seropositive against Hardjo at a minimum MAT titre of ⩾1:48 for 29 months following a typical infection episode with Hardjo.
Illness and population impact
The annual risk of confirmed clinical leptospirosis was 0·78% (3/384, 95% CI 0·20–2·46) with all cases occurring in sheep slaughtering abattoirs. The three confirmed clinical leptospirosis cases constituted 6·3% (95% CI 1·6–18·6) of all new infections in sheep abattoir workers. Two of those seroconverted from negative and 1:48 to 1:192 against Pomona. The third had a positive titre of 1:192 against Pomona at both sampling times and against Hardjo a titre of 1:96 in the first followed by 1:48 in the second sampling time. All three were males, aged between 43 and 67 years and worked in sheep abattoirs in the area where the pelt is cut open (beginning of the slaughter board) or the gut is removed, or in the offal room. They reported being constantly exposed to organs of the urinary tract or to urine, and found the protective gear to be unpleasant. They reported having been 0, 3 and 84 days, respectively, away from work due to leptospirosis.
Since information on influenza-like symptoms was missing for four persons, only data from 380/384 sheep abattoir workers could be used in the analysis. A total of 104/380 (27·4%, 95% CI 23·0–32·2) sheep abattoir workers including 22/47 (47%, 95% CI 32–62) with new infections and 82/333 (24·6%, 95% CI 20·2–29·7) without evidence of infection, reported having influenza-like symptoms during the 1-year study period. Four workers who did not seroconvert could not make conclusive statements about influenza-like symptoms since the first blood sampling 12 months ago. Workers with influenza-like symptoms had significantly higher titres against Pomona than those without influenza-like symptoms (P = 0·02). Hardjo titres of workers with influenza-like symptoms did not differ from those without influenza-like symptoms.
Table 4 summarizes data of Leptospira infection related to the incidence and proportion of ILI in the total sheep abattoir study population. New infections with Leptospira increased the risk of illness with influenza-like symptoms 1·9-fold (95% CI 1·3–2·7, P = 0·007) and new infection only with Pomona 2·1-fold (95% CI 1·5–3·0). Assuming causality, in those who experienced new infection, 10% (PAF, 95% CI 2–16) of influenza-like cases were attributable to new infection with Pomona and/or Hardjo. The risk of ILI in seroconverting participants that could be attributed to seroconversion against Leptospira was 22·2% (AR, 95% CI 7·2–37·2), and against Pomona alone 28·1% (AR, 95% CI 11·1–45·0). Hence 78% (or 72% if only Pomona was considered) of infections were ‘silent’ and the majority of leptospiral infections did not result in noticeable signs of disease. The average annual risk of a worker, over all workplaces, experiencing influenza-like symptoms due to infection with Leptospira or due to infection with Pomona alone was 2·7% (PAR).
Table 4. The relative risk, attributable risk, population attributable risk and population attributable fraction of sheep abattoir workers (n = 380) having influenza-like illness when newly infected with Leptospira interrogans serovar Pomona and/or Leptospira borgpetersenii serovar Hardjo or when only newly infected with Pomona
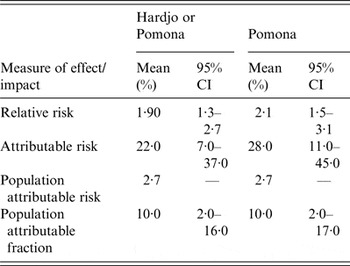
CI, Confidence interval.
The under-ascertainment of officially notified cases of leptospirosis was estimated at between 16 and 56 times based on data reported in the past 5 years [10]. However, this rate includes persons with the mild symptoms of leptospirosis. The average time away from work due to ILI was 4·4 days (95% CI 2·7–6·1), independent of seroconversion.
DISCUSSION
The novel information in this study arises from combining serological data with personal illness episodes to provide an estimate of pathogen-attributable disease incidence. We estimated the extent to which abattoir workers, who were subjected to seemingly high levels of exposure to sheep carcases shedding Leptospira [Reference Dorjee28], acquired infection and developed clinical disease consistent with leptospirosis. The economic impact of this disease was quantified by inquiry as days absent from work in the preceding 12-month period. In sheep abattoirs, 12% of the workforce showed evidence of a new infection with Hardjo or Pomona in one calendar year. About 78% of infections were silent (non-clinical) whereas 22% of infected workers reported signs consistent with leptospirosis, and 2·7–6·1 days absence from work. Extrapolated to the total workforce at New Zealand sheep plants of about 10 000, this means about 276 workers may be getting ill with leptospirosis every year due to working at an abattoir, causing a loss of about 1200 total work-days. However, this information should be interpreted with caution, as the authors used a subjective method of assessing illness by self-reporting and were not able to confirm the correctness of the information by checking a random sample of work records.
Assuming that the association between seroconversion and reported illness was causal, the risk of illness due to leptospirosis for individual workers during the study year in sheep plants was 2·7%, hence 1/37 workers experienced clinical leptospirosis, a rate 16–54 times higher than the rate of notified cases within the meat worker population for that year. This was equivalent to 10% of all ILI that was potentially caused by Pomona or Hardjo. We regard this as a substantial public health risk due to leptospirosis. The risk might even be higher if blood had been tested by MAT for other serovars, e.g. Tarassovi, Ballum or Copenhageni all of which are also known to occur in notified cases [Reference Thornley5].
The sheep slaughtering abattoirs are located in the east and west of the North Island, so they were geographically not entirely representative of the whole country. However, slaughtered animals originated from all over the North Island. Assuming a total of 10 000 sheep abattoir workers in NZ (exact numbers were not available by species) and the target population (total numbers of workers who were asked to participate) consisted of 17·5% (n = 1747), we did recruit our study population from almost 20% of the total sheep abattoir worker population [Reference Dreyfus19].
The data revealed differences in new infection risk between slaughter species and between abattoirs. Workers in abattoirs processing sheep had a substantially higher annual risk of infection (11·9%) than workers processing deer (0·0%) or cattle (1·2%). Possible reasons for the higher incidence in sheep abattoirs, despite similar infection rates in sheep and beef [Reference Dreyfus1], is that sheep abattoirs process more animals per day than cattle abattoirs and have a different slaughter procedure. During interviews, participants reported that sheep urinate spontaneously when stunned, whereas cattle do not. Therefore, sheep abattoir workers may be more exposed to Leptospira than beef abattoir workers, especially when stunned sheep drop onto a platform contaminated with pools of urine from other sheep. Another speculative reason could be the variability in pathogenicity for humans within serovar strains infecting sheep and cattle.
Even though deer abattoir workers had a 17% seroprevalence at the beginning of the study, the annual risk of infection during this study was 0%. These findings are consistent with a range of possible interpretations. Our study may have missed seroconversions due to the small sample size at deer plants (n = 50) where only 16 initially seronegative persons worked in highly exposed positions (slaughter, offal). Alternatively, deer workers may have adapted better preventative measures and were less exposed. Or there may have been a decline in the prevalence of leptospirosis in these deer herds over time. In general, deer abattoirs are small, operating one slaughter line. The workers of the slaughter board perform most activities manually doing multiple tasks. Hence, the risk of getting exposed to deer urine is likely to be high.
This study inferred ‘infection’ from serological evidence as there was no attempt to measure leptospires in blood or urine, or ‘the entry, development or multiplication of the agent’ as infection was defined earlier [Reference Last29]. However, we believe serology to be a reasonable approximation because bacterial challenge is required to produce an immune response in the absence of vaccination, and an immune response was significantly associated with clinical disease.
The relative risk (RR) for a person to have influenza-like symptoms was similar in the anamnestic response and seroconversion groups with a RR of 1·5 (P = 0·26) and 1·8 (P = 0·008), respectively, compared to persons without new infection. Commonly, it is believed that a booster of the humoral immune system, which is measured by an anamnestic response, will extend the period of immunity, during which a person does not develop clinical symptoms. The data, however, suggest that repeated exposure may also lead to a new illness episode, albeit statistically non-significant (small sample).
The average titre duration of antibodies against Pomona was estimated to be 10 months and against Hardjo 29 months, demonstrating that antibodies may persist longer than a year in an infected person. This is useful information for infectious disease modelling and for calculating incidence from more readily available prevalence data. Thai et al. [Reference Thai30] showed that in apparently healthy schoolchildren in an area in Vietnam with endemic leptospirosis, antibody titres can persist for longer than a year, as 61% of study participants had antibodies against any possible L. biflexa serovar 2 years after first sampling. Both study methods were limited as there was no control for re-infection. Antibody titre persistence is highly variable and depends on host and pathogen factors, such as immunity, silent or clinical infection, antibody titre, age of the host, infectious dose, serovar and serovar virulence [Reference Lupidi31, Reference Cumberland32].
The annual leptospirosis infection risk across the study population was 5·8% for Pomona and 2·3% for Hardjo, despite the fact that Hardjo was more seroprevalent in workers at the beginning of the study [Reference Dreyfus19], and also in the source animals (sheep, deer, beef) [Reference Dreyfus1]. By contrast, an earlier analysis of notified leptospirosis data found that the annual number of cases in meat workers due to Pomona decreased from 62 in 1990 to 26 in 1996, while cases due to Hardjo increased from 23 to 30 [Reference Thornley5]. Speculative reasons for the higher incidence of Pomona than Hardjo in the current study may be the difference in duration of antibody persistence, host specific susceptibility, a higher amount of shedding from Pomona-infected sheep carcasses, a difference in exposure between farmers and abattoir workers, or different trends in 1990/1996 to 2008/2009. Moreover, most of the association between seroconversion and ILI in our data was attributable to Pomona whereas it was non-significant for Hardjo, suggesting that Pomona might be relatively more virulent in humans.
Since 2008 serovar Ballum has on average accounted for approximately a quarter of notified human leptospirosis cases. Notwithstanding we did not test all serum samples for this serovar. This decision was based on a pilot study that tested 60 serum samples from this cohort for Ballum and all were negative. Furthermore, although detailed information on infecting serovar by occupation is not currently available nationwide, an analysis of 97 notified cases in the Waikato region of New Zealand from 2004 to 2010 found Ballum only in farmers and not in meat workers [Reference Cowie and Bell33]. Ballum is reported to be transmitted by mice, rats and hedgehogs [Reference Marshall and Manktelow4, Reference Hathaway34] and generally not transmitted by livestock.
In conclusion, this study demonstrated that workers in sheep abattoirs were at substantial risk of new infection with Pomona and/or Hardjo within a single slaughter season. It further showed that newly infected workers from sheep abattoirs had a twofold higher risk of ILI with 2·7% of the workforce being absent from work for 4 days on average within a single slaughter season due to leptospirosis. Infection rates and their association with clinical illness were both attributable to Pomona, and were non-significant for Hardjo. The rate of illness due to leptospirosis in the sheep abattoir study population was about 16–56 times higher than the official rate of notified leptospirosis cases. The risk was higher in sheep abattoir workers than in workers at deer and beef plants. In order to localize the infection risk in sheep abattoirs, it is recommended to investigate the association of work-related risk factors, such as work position with Leptospira infection in meat workers and the effect of protective gear on infection rates. To assess the risk of infection with Leptospira in meat workers independent of work, risk factors, such as hunting, slaughtering at home and farming, should be included in the analysis. Further, it may be useful to analyse the platforms on which stunned sheep drop for Leptospira contamination.
SUPPLEMENTARY MATERIAL
For supplementary material accompanying this paper visit http://dx.doi.org/10.1017/S0950268814002477.
ACKNOWLEDGEMENTS
We are indebted and grateful to study participants, managers and health and safety workers of the participating abattoirs, nurses and phlebotomists, without whom the study would have been impossible (names confidential).
We thank the occupational health physicians John Reekie and John Kerr for advice and support, Heather Duckett for helping to organize sampling, Christine Cunningham and Wendy Maharey for administrative support, Brian O'Leary, Masood Sujau and Simon Verschaffelt for help developing the database, Fang Fang, Prakriti Bhattarai, Rayon Gregory, Claire Cayol and Emilie Vallee for interviewing, Neville Haack and Rae Pearson for MAT testing, Roger Lentle for advice for the Massey University Human Ethics Committee application and Lesley Stringer and Sarah Rosanowski for analytical and software support. Further, we thank the Department of Labour for support.
We gratefully acknowledge funding donated by Rural Woman New Zealand, and commissioned by the Tertiary Education Commission (TEC) via the Institute of Veterinary, Animal and Biomedical Sciences, Massey University [TEC no. RM12703 (2008)], and the Swiss National Science Foundation (SNF) (PBBEBS-124186).
DECLARATION OF INTEREST
None.






