



LEARNING OBJECTIVES
After reading this article you will be able to:
• reflect on the ubiquity of email in the healthcare workplace
• understand email's advantages and disadvantages
• describe personal and organisational approaches to enable efficient use of email
Email is a tool for communication that facilitates delivery of messages and information between individuals and organisations (Box 1). Email's origins can be traced back to the 1960s. Since then, sequential technological advances, such as the advent of webmail and smartphones, have facilitated its increasing use. Over the past 20 years it has become a major means of communication between healthcare professionals.
BOX 1 What is email?
‘Email’ is short for ‘electronic mail’ and is a method of exchanging messages between people using electronic devices.
‘Email’ is the medium of message exchange, whereas an individual message is referred to as ‘an email’.
An email can be sent to a single recipient or to multiple recipients and it can include file attachments, such as documents or pictures.
Emails are typically sent or received via applications (apps) installed on desktop computers or smartphones (e.g. Microsoft Outlook) or via apps accessible via a web browser (e.g. Gmail).
Alongside email's ubiquity and ease of use have emerged a variety of challenges. Email has not just changed the way we communicate but also the way we get things done (Newport Reference Newport2022), and email's environmental cost is hidden. Many working days can be dictated by the receipt of and reply to multiple email messages, which can drown out other priorities and compromise both productive output and equanimity.
Email's ubiquity and use in the NHS
In 2021 the total number of business and consumer emails sent and received each day worldwide was forecast as more than 319 billion and predicted to grow to over 376 billion by the end of 2025 (Radicati Group 2020).
The healthcare sector was initially more cautious about the adoption of email than other sectors (Goyder Reference Goyder, Atherton and Car2015), but email is now a primary method of correspondence between healthcare professionals (Malka Reference Malka, Kessler and Abraham2015). It is the assumption of many healthcare organisations that staff will regularly check and act on their email messages (Dennis Reference Dennis and Waterworth2021).
In the UK, National Health Service (NHS) staff can access professional email accounts either via services commissioned and administered nationally, such as NHSmail, or those provided locally. NHSmail is an email, diary and directory system administered by NHS England which has been in operation for more than 20 years (Heather Reference Heather2016).
Healthcare professionals use email for a multitude of purposes: for both formal and informal communications with colleagues and patients; to perform administrative duties; to conduct routine communication; and to undertake research and improvement projects. It is also used by management at all levels to convey information to large or small groups of staff. Some key advantages of email are set out in Box 2.
BOX 2 Advantages of email
• Emails are delivered almost instantaneously, at minimal or no cost to sender or recipient.
• Email can avoid the need for more time-consuming interactions such as telephone calls or face-to-face meetings.
• Digital images and documents can be transferred easily.
• Unlike a telephone conversation, email is an asynchronous method of communication as no coordination is required between participants.
• Messages can be sent and subsequently read at an opportune time, including outside of traditional office hours.
• Emails can be used as reference information for the recipient, aiding recall and providing evidence of the exchange.
• Email allows communication to large groups.
• Correspondents can be geographically distant.
Email is also an integral part of an individual's overall online experience (Radicati Group 2020) and it is likely that in parallel with processing work-related emails, any individual will be managing a busy personal email account.
Challenges: the trouble with email
Workflow
The workflows of today's healthcare professionals are not like those of an era pre-email but now with faster communications (Newport Reference Newport2022). Instead, email has reshaped workflow and workplace interpersonal relations. Healthcare delivery often now unfolds via a continuous unstructured flow of emails, of which an individual is a passive recipient (Ayoub Reference Ayoub2021). The experience can be one of an employee attempting to execute work tasks while also simultaneously managing ongoing email conversations about the same tasks (Newport Reference Newport2022).
People can feel compelled to reply to emails (Dennis Reference Dennis and Waterworth2021). These interruptions come at a cost. After responding to an email, re-engaging in a primary task can take up to 15 min (Jackson Reference Jackson, Dawson and Wilson2001) and answering emails during face-to-face meetings is common (Dennis Reference Dennis and Waterworth2021). Undue focus on email may orientate an employee's efforts towards work that is urgent rather than work that is important (Cooke Reference Cooke, Williams and Esain2010).
Unstructured, inferior to direct communication and unprofessional
With email, messages concerning heterogeneous topics – some relevant, some not – all arrive in the same electronic location (the ‘inbox’). Arranging a patient's care can mean navigating a jumble of back-and-forth messages with numerous emails, copied to multiple recipients, required to reach a single decision (Jones Reference Jones2012).
As text-only communication, emails can lack the nuance of face-to-face interactions (Car Reference Car and Sheikh2004) as the emotive cues from vocal intonation or body language are lost. Email communication is generally less formal than other professional interactions, risking unprofessional conduct and ambiguously formulated messages that do not provide recipients with the information they require to act.
Time burden
Outside healthcare, email processing is identified as time-consuming and a source of workload stress for employees. There is evidence that it is similarly onerous in a healthcare context (Barley Reference Barley, Meyerson and Grodal2011; Akbar Reference Akbar, Mark and Warton2021), although it seems likely that the individual experience of email will be variable and influenced by medical specialty, as well as personal and organisational factors (Grawitch Reference Grawitch, Werth and Palmer2018).
Emails are workload generating, as responding to emails can lead to further emails in reply. Emails can proliferate owing to indiscriminate use of ‘carbon copy’ (cc) and ‘reply all’ functions (McGee Reference McGee, Clemons and Joy2019).
Email's ease of use encourages thoughtless demands on the attention and time of others as it offers little barrier to asking questions or delegating tasks (Newport Reference Newport2022). In an NHS trust of 10 000 people, a single email sent to all staff which takes each recipient 1 min to process will generate 4.5 weeks of organisational time lost, even if no further action is required (Cooke Reference Cooke, Williams and Esain2010).
Technology-related stress
Emails, along with other computer-based technologies, contribute to ‘technostress’ (Golz Reference Golz2021). This has been defined as ‘a modern disease of adaptation caused by an inability to cope with the new computer technologies in a healthy manner’ (Brod, 1984, cited in Golz Reference Golz2021). Components of technostress are listed in Box 3.
BOX 3 Components of technostress
• Techno-invasion (employees can be reached anytime).
• Techno-overload (technology forces users to work faster and longer).
• Techno-complexity (users feel inadequate regarding their competences).
• Techno-uncertainty (ongoing changes lead to uncertainty and constant learning).
• Techno-insecurity (feeling threatened about losing one's job because of automation).
• Techno-unreliability (unreliability of technology used).
(Golz Reference Golz2021)
Documentation, safety and information security
Many clinical conversations presently take place via email, but these do not automatically form part of the clinical record. In the context of a lack of a standard model across the NHS for documenting and communicating information in general (Abdelrahman Reference Abdelrahman and Abdelmageed2014) there is also no standard for how emails are documented.
Email's use in urgent situations may compromise patient safety (Stiles Reference Stiles, Deppen and Figaro2007). If email is relied on for communication, then important issues and deadlines are easily overlooked as email messages may not be read immediately on receipt, or at all, and are easily deleted. A sender and recipient may not have a shared understanding regarding the urgency of a particular issue communicated via email.
The information security of patient records may not be adequately attended to by email users and organisations (Malka Reference Malka, Kessler and Abraham2015). For example, users may mistakenly forward an email containing protected patient data to an unintended recipient, or may access their emails in a public location (Malka Reference Malka, Kessler and Abraham2015). Breaches of cybersecurity are commonplace, in both the private (Department for Digital, Culture, Media and Sport 2022) and healthcare sectors (e.g. BBC News 2022).
Environmental cost
Email is supported by a vast but largely invisible technological infrastructure. Any environmental assessment of email must consider the emissions required to compose, transmit and subsequently store email information (Tsukayama Reference Tsukayama2017; Berners-Lee Reference Berners-Lee2020).
An email is estimated to generate 0.2–26 g of CO2, compared with a letter, which generates 280–350 g (Berners-Lee Reference Berners-Lee2020). However, as so many more emails are sent than letters were once, it seems likely that email is an example of a low-carbon technology that ultimately results in higher carbon emissions because we use it more (Berners-Lee Reference Berners-Lee2020).
Using email effectively and efficiently
Individuals differ in their working styles, and communication tolerances and preferences, so a universal solution to the frustrations of email is likely to be elusive. What one person views as an advantage of email may be experienced by a colleague as a disadvantage. This notwithstanding, advice is available regarding email management (Mann Reference Mann2007; Cooke Reference Cooke, Williams and Esain2010; Forte Reference Forte2022). Most of this is aimed at general, rather than specifically healthcare, audiences and systematic evidence of the most effective approach is lacking.
Individuals and organisations that wish to improve their email experience are likely to benefit first from one-off preparation tasks and second from attention to creating and maintaining a systematised email workflow process that allow emails to be acted on in a timely fashion and not to overwhelm other priorities.
More radically, email can be decoupled from workflow.
Individual preparation: addressing email backlog and other one-off tasks
Manage email apps
If, by default, a user's desktop or laptop email app loads automatically on boot up, this setting can be changed. The user can then undertake other tasks before, at a time of their choosing, addressing their emails.
Clear email backlog
If an individual's email inbox contains more unread emails than can be realistically processed in a timely fashion, it may be necessary for these to be archived. Time can then be subsequently scheduled for their review. This may not be necessary, however, as it is likely that correspondents who are keen for a response will send further messages.
Unsubscribe
Unsubscribing from newsletters, notifications and any other emails that are non-essential will reduce subsequent personal email traffic.
Keep email addresses private
Publicly available email addresses will receive unsolicited mail.
Use of rules
An individual may have a colleague or colleagues who are prolific emailers of unimportant messages. Setting up an email management rule will allow these emails to automatically be channelled into a bespoke folder and addressed periodically.
Organisational preparation
Email is simply a medium for communication; how it is used is down to an organisation's custom and practice. Collective effort to address an organisation's email culture has the potential to promote efficient email communication that takes place in a mutually supportive fashion.
Empowering staff
Organisational culture can empower staff to manage the demands that email can generate during work and when away from work. This might include an organisational understanding that it is acceptable for reasons of staff well-being to periodically disengage from email (Dennis Reference Dennis and Waterworth2021). In 2012 Volkswagen stopped routing emails to some employees when they are out of the office (BBC News 2012).
Staff can be encouraged to think of email as a workflow task like any other, which requires scheduling, but does not inevitably dictate a day's activities.
Technological tweaks
Despite the growth of email traffic and email's ever more prominent role in daily lives, the design of email management apps has changed little over the past 30 years.
A reimagined email experience might look very different from that currently available and would allow an individual to customise their email access to support their pace of work and communication preferences. In the meantime, some tweaks as simple as reducing interruptions by decreasing the frequency with which inboxes refresh or disabling ‘reply all’ as a default option might dramatically improve the working experience of some users.
NHS considerations
The use of email by NHS staff is not explicitly addressed in the NHS's long-term technology strategy, which was set out in the NHS Long Term Plan (NHS England 2019). The plan does observe, however, that at present ‘too much of the technology in the NHS is a burden on our staff’ (p. 94) and that technology has a role in making the NHS a more satisfying employer. It seems likely therefore that, in due course, NHS technology planning will need to consider how the use of email by NHS staff sits within these aspirations.
Systematising personal email workflow: efficiency and speed
Processing email efficiently: ‘inbox zero’
Just like any other work process, email engagement can be managed by the user (Dennis Reference Dennis and Waterworth2021). Employees reporting problems with emails are not necessarily those who receive or send the most emails but rather those who have not developed an effective structure for filing incoming emails (Lantz Reference Lantz1998).
‘Inbox zero’ is one approach (Mann Reference Mann2007; Forte Reference Forte2022), and it draws heavily on the ‘Getting Things Done’ personal productivity system (Allen Reference Allen2019).
The essence of this approach is that following an email's arrival, it is read once only and then immediately processed such that one of the following actions results:
(a) The email is deleted.
(b) The email is archived as reference material. Depending on the nature of the information this can be either to an email folder or to a note-taking app such as Notion or Evernote.
(c) The email generates a task and this is undertaken immediately. The email is then archived or deleted.
(d) The email generates a task and this is scheduled for subsequent attention via, for instance, a calendar entry, a task manager or a read-later app (e.g. Pocket). The email is then archived or deleted.
(e) The email generates a task and this is delegated. The email is moved to an ‘awaiting response’ folder and is then archived or deleted in due course.
This approach is further set out in Fig. 1.
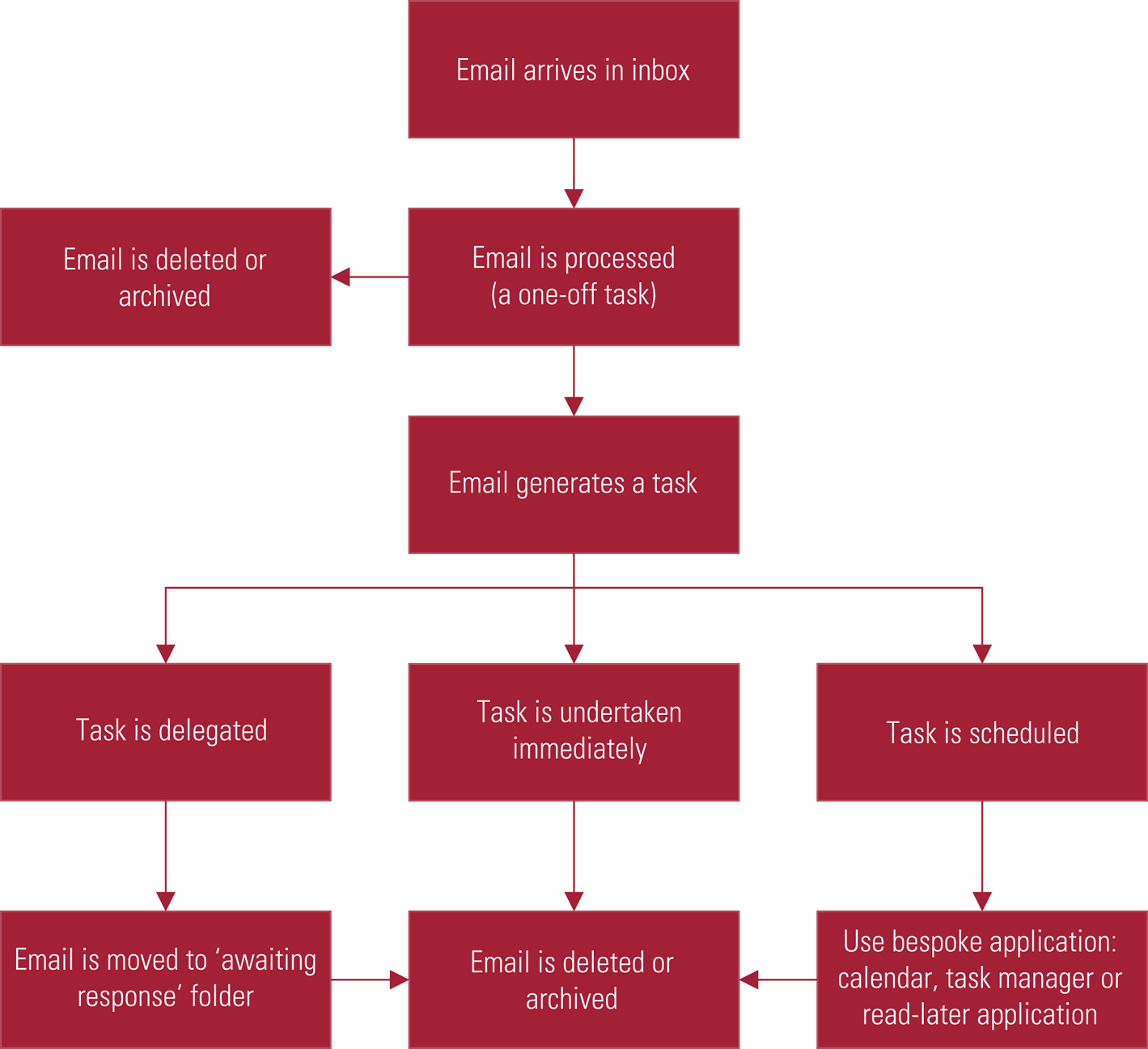
FIG 1 Systematised email workflow.
By the above method an individual's email inbox is used solely for message management and not as a to-do list, calendar or reference library, tasks for which it has no specific functionality and which other apps can perform more successfully. The only emails that remain in the inbox are ones that have yet to be processed.
There is no universally successful way to arrange email archive folders, and again personal preference is important. It would seem sensible for an individual to aim for the simplest system that will allow them to retrieve an email at a later date (Mann Reference Mann2007). A minimum set of folders is likely to include an archive folder and an awaiting-response folder. Users may also wish to have folders for particular projects or particular patients.
Processing email quickly
Common approaches to processing email more quickly include the following.
Batching
Processing emails once or twice a day only, rather than constantly, reduces interruptions. Less frequent inbox checking has been found to be associated with reduced stress and to predict greater well-being (Kushlev Reference Kushlev and Dunn2015). In practice most email requests are not urgent and colleagues can make contact in other ways if a rapid response is required.
Cut composition time – type faster and write less
Learning to touch-type cuts time spent composing emails, as does writing shorter emails. One approach is to make all emails no longer than an SMS message (Davidson Reference Davidson2007) or use bullet points in composition rather than prose.
Using rules and other sorting processes
Email apps can reduce email processing time by allowing for the automatic filtering and sorting of incoming messages. Email rules allow a user to process an email with a certain characteristic. For instance, messages sent as carbon copy (cc) can be automatically highlighted to distinguish them from those that are directly addressed to the recipient and therefore may be more relevant. Importance markers such as flags can also assist email processing and actioning (Dennis Reference Dennis and Waterworth2021).
Use of artificial intelligence (AI)
AI chatbot apps such as ChatGPT have recently become widely available and can be used to compose replies to email messages. AI-generated emails should be carefully checked before they are sent.
Careful composition of emails and use of email with patients
Email composition has been found, among clinicians, to affect the receiver's perception of the sender and the likelihood of a timely response (Malka Reference Malka, Kessler and Abraham2015). Emails that are clear and concise reduce the need for subsequent back and forth exchanges to establish clarity. However, there are no formal guidelines for email use among clinicians (Malka Reference Malka, Kessler and Abraham2015) and evidence is lacking on the impacts of healthcare professionals using email to communicate with each other (Goyder Reference Goyder, Atherton and Car2015).
Advice regarding email composition which is tailored to clinicians tends to mirror advice available to other professions and mixes anecdote and intuition (Malka Reference Malka, Kessler and Abraham2015). One approach to the careful composition of email is the SURE model (Railey Reference Railey, Tuttle and Weiss2017). This is detailed in Box 4. There are also 18 point (Biggin Reference Biggin2018) and 50 point (Hills Reference Hills2011) guides for medical email etiquette.
BOX 4 The SURE model for composing an email
-
S: Have you checked the Spelling and Syntax? Have you included a Subject and Signature?
-
U: How Urgent is your message? Does your reply communicate an Unprofessional tone?
-
R: Have you confirmed the Recipients? Have you Reviewed/Reread the message?
-
E: What Emotion might your email express or evoke? Are there any Ethical considerations?
Email's relative lack of nuance and emotive cues can be addressed to a degree with use of emojis, which are graphic symbols that can be embedded in text. Of these, the ‘grinning face’ or  , is perhaps deployed most frequently.
, is perhaps deployed most frequently.
It is beyond the scope this article to discuss in detail the advantages and disadvantages of clinicians using email to communicate with patients. Many clinicians may be emailing their patients without referring to guidance (Sowerbutts Reference Sowerbutts and Fertleman2016), with possible patient safety and medicolegal consequences. Email may best be viewed as a complementary method of communication with patients and suitable for use in some circumstances, but its use should be avoided for urgent, complex or sensitive messages (Sowerbutts Reference Sowerbutts and Fertleman2016).
Organisational email workflow systematisation
Decoupling email from workflow
Outside healthcare, ‘zero email’ initiatives have sought to decouple work processes from the exchange of email messages and create workflows that avoid unstructured back and forth email chatter. One of the most ambitious drives to eliminate email was started in 2011 by Atos, a global information services company that reduced its internal email traffic by 60% (Oettl Reference Oettl, Beck and Raufer2018).
Instead of accessing a generic email inbox and sending emails to co-workers, Atos's employees’ projects and communications take place within an online working environment. An individual has the discretion whether to work on a particular project or not and is not interrupted by messages about projects with which they are not presently engaged (Stoltzfus Reference Stoltzfus2015).
At present many electronic healthcare records systems used in the NHS have limited functionality in supporting productivity and email is used as a suboptimal work-around solution. Future record systems could include features such as task management and some benefits have already been found when using an electronic health records-based secure messaging system, replacing paging or phone calls (Luu Reference Luu, Spiegelman and Nykin2022).
Training
Email's ubiquity in healthcare does not necessarily translate into skilled use (De Gagne Reference De Gagne, Yang and Rushton2020). Email training that included instruction on the functions of email apps that are useful for filtering and sorting a high volume of email, together with demonstration of the principles of effective personal workflow, was found to increase knowledge and competency (Soucek Reference Soucek and Moser2010).
Conclusions
In the 1970s, in his bestselling book Future Shock, futurologist Alvin Toffler popularised the idea of ‘information overload’, the difficulty in grasping issues and effectively making decisions because of excess daily information (Toffler Reference Toffler1970). Email embodies some of his predictions: its use has now reached saturation point for many people working in healthcare, with their actual productive output squeezed and their days characterised by relentless exchange of email messages.
Email has self-evident advantages and seems likely to be here to stay. However, a reassessment of its use is required if, as is commonly the case for healthcare professionals, answering email messages is overwhelming other priorities and having an impact on work satisfaction.
It seems that, to date in the healthcare context, insufficient attention has been paid to team and individual workflows and unstructured email traffic has filled the void. Achieving success and equanimity in hospitals and clinics may mean that, for the foreseeable future, individuals and teams will need to manage their communications proactively so as to avoid high volumes of emails and to ensure that email works for us, rather than – seemingly – the other way around.
Funding
This work received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
S.G. owns shares in Apple, Google and Microsoft, each of which provides email services.
MCQs
Select the single best option for each question stem
1 By the end of 2025 it is predicted that how many emails will be sent daily?
a 376 billion
b 459 billion
c 126 billion
d 587 billion
e 28 billion.
2 Why is it likely that email generates higher carbon emissions than letters?
a Composing, sending and storing an individual email generates more carbon than a single letter
b During its lifecycle a single email generates less carbon emission than a single letter, but we send many more emails than we once did letters
c A lot of emails are printed out
d Emails are stored on the cloud in data centres: cooling these data centres is energy intensive and is often powered by burning coal
e Most personal computers are left on all the time.
3 After an email interrupts an individual's workflow, evidence suggests it may take how long to return to the primary task?
a 6 min
b 9 min
c 12 min
d 15 min
e 18 min.
4 In the ‘inbox zero’ email management approach an email, once received, results in an action. Which of the following is not an inbox zero action?
a The email is deleted
b The email archived as reference material
c The email generates a task and this is delegated
d The email generates a task and this is undertaken immediately by the recipient
e The email is read and remains in the inbox for future consideration.
5 Which of the following is not a component of technostress?
a Techno-invasion
b Techno-complexity
c Techno-uncertainty
d Techno-unreliability
e Techno-trauma.
MCQ answers
1 a 2 b 3 d 4 e 5 e


eLetters
No eLetters have been published for this article.