


Introduction
Millions of children in low- and middle-income countries (LMICs) fail to develop to their full cognitive potential.Reference Walker, Wachs and Grantham-McGregor 1 There is robust evidence that investments in early childhood development (ECD) are vital for children to fulfil this potential. Consequently, there has been strong support for strategies aimed at reducing risk factors and promoting protective factors for ECD in LMICs.Reference Engle, Black and JR 2 Important risk factors which need to be addressed are malnutrition, stunting and childhood disease such as HIV, while factors which have been positively associated with child development include sustained exposure to breastfeeding and higher maternal education.Reference Walker, Wachs and Grantham-McGregor 1
While early childhood investments are key, middle childhood and the transition into formal schooling is also a critical developmental time for children and has been shown to impact on their long term educational success.Reference Entwistle, Alexander and Olson 3 For example in both high-income countries (HICs) and LMICs, children who repeat the first grade of school are significantly more likely to experience academic disengagement and dropout in later years,Reference Jimerson, Anderson and Whipple 4 , Reference Gomes-Neto and Hanushek 5 which is, in turn, linked to poorer health and economic outcomes in adulthood.Reference Freudenberg and Ruglis 6 , Reference Oreopoulos 7 Understanding the factors that drive early failures in children’s schooling is critical to the development of targeted interventions to improve children’s educational outcomes,Reference Kamal and Bener 8 , Reference Hamre and Pianta 9 particularly in the context of poverty.
Important early factors were identified in two longitudinal studies from the United States which examined the association between early child and maternal factors and grade repetition. The first included a nationally representative sample of 996 children, aged 7–17 years, and found poverty, male sex, child behaviour problems and low maternal education to be associated with increased grade repetition, while higher maternal education and residing with both parents reduced the risk of grade repetition.Reference Byrd and Weitzman 10 A more recent longitudinal study in the United States with a sample of 220 low-income primary school-aged African-American children,Reference Blair 11 found a lack of stimulation at home before school enrolment and high externalizing behaviour (related to aggressive and criminal behaviour),Reference Liu 12 to be significantly associated with increased likelihood of grade repetition.
These studies did not examine the effect of the broader familial context, such as the effect of having older siblings, which has been suggested to be as important as parental contribution to younger children’s cognitive development and consequent schooling outcomes.Reference Dai and Heckman 13 Furthermore, the effect of having had exposure to crèche and reception year, which have been shown to be important in promoting ECD, were not included. 14 Importantly, the effect of HIV infection or exposure, which is of particular importance in high HIV prevalence settings, was not examined. A critical review of global literature on HIV-exposed children’s educational outcomesReference Guo, Li and Sherr 15 mostly focused on orphaned children and reported poorer educational outcomes among HIV-orphaned than non-orphaned children,Reference Birdthistle, Floyd and Nyagadza 16 , Reference Rescorla, Achenbach and Ivanova 17 with particularly strong effects on girls.Reference Ainsworth, Beegle and Koda 18 – Reference Yamano and Jayne 20 This review elucidated several gaps in the literature including a tendency to focus on already orphaned children without examining effects on schooling before parental death; few data on sex differences; and a lack of longitudinal studies. Most studies have also focused only on school enrolment and attendance,Reference Birdthistle, Floyd and Nyagadza 16 , Reference Ainsworth and Filmer 21 , Reference Evans and Miguel 22 or failure in later stages of schooling among adolescents,Reference Birdthistle, Floyd and Nyagadza 16 , Reference Kobiané, Calvès and Marcoux 23 with little research focusing on grade repetition, or earliest grade failure.
In South Africa, some research has examined early school factors associated with grade repetition across the primary school years.Reference Fleisch and Shindler 24 , Reference Motala, Dieltiens and Sayed 25 However, to our knowledge, no studies have examined whether early life exposure to maternal HIV infection influences grade repetition among children in the early years of schooling, and if exposure to reception year and current familial factors mediate these effects.Reference De Neve, Fink, Subramanian, Moyo and Bor 26
The primary aim of this research was to investigate early life factors associated with earliest repeated grade, and to explore child characteristics and parental report of reasons for failure among early repeaters. We examined this question in a well-established cohort using a longitudinal design including children exposed to HIV in fetal life or childhood, and HIV-unexposed children in rural South Africa.
Methods
Setting
This research took place at the Africa Centre for Health and Population Studies (Africa Centre), in Northern KwaZulu-Natal, South Africa, a predominantly rural area with one of the highest prevalence of HIV worldwide.Reference Zaidi, Grapsa, Tanser, Newell and Bärnighausen 27 A successful large scale Prevention of Mother-to-Child Transmission programme and HIV treatment programme, providing free drugs and clinical care, have been operating in the district since the early 2000s.Reference Houlihan, Bland and Mutevedzi 28 , Reference Mkwanazi, Patel and Newell 29
Participants
The sample consisted of children aged 7–11 years, who were born, and currently reside in, the study area of the Africa Centre. All children were part of an early life intervention to support exclusive breastfeeding (EBF), the Vertical Transmission Study (VTS).Reference Bland, Coovadia, Coutsoudis, Rollins and Newell 30 , Reference Coovadia, Rollins and Bland 31 This was a non-randomised, prospective, intervention cohort study (2001–2006), that supported mothers to exclusively breastfeed and followed children from birth to 2 years of age.
Procedures
Data collected in the VTS included maternal HIV status during pregnancy, maternal education, income source, socioeconomic status at the time of the child’s birth and daily infant feeding practices collected at weekly intervals in the first 6 months postnatally.Reference Bland, Coovadia, Coutsoudis, Rollins and Newell 30 , Reference Coovadia, Rollins and Bland 31 Household ownership of a fridge was used as a proxy for socioeconomic status (SES), as is common in other research in LMICs.Reference Galobardes, Shaw, Lawlor and Lynch 32
In 2013/2014 we re-enrolled HIV-negative children from the VTS to investigate the impact of this early life intervention on their longer term development, in the ‘Saving Brains Cohort’. Inclusion criteria for re-enrolment included that the mother and child were alive, the child was still residing in the research area, the mother’s HIV status in pregnancy was known, and the child was HIV-negative.
While children’s mothers had to be alive to be included in the Saving Brains cohort, they did not have to currently reside with the mother; children were still eligible if they resided with an alternative caregiver. Children and their mothers and/or caregivers were visited three times by field staff, all of whom had at least 4 years’ experience collecting research data. In Visit 1 consent to enrol (also from alternative caregiver if applicable), basic demographics and whether the mother met the inclusion criteria were measured. In Visit 2, data were collected from the primary caregiver (mother or other) about the child’s schooling history and repeated grades, and mothers/caregivers completed both the Competence Scale and the Behaviour Rating Scale of the Child Behaviour Checklist (CBCL), which has been validated in a variety of cultural settings.Reference Rescorla, Achenbach and Ivanova 17 , Reference Achenbach and Edelbrock 33 The Competence Scale includes parent ratings of children’s social and peer relationships, their level of independence and their performance on specific academic subjects. It also collects qualitative descriptive data on parental understandings of reasons for children’s failure in school or other problems the child may be experiencing. In Visit 3, the Kaufman Assessment Battery for Children, second edition (KABC-II) was administered to measure children’s cognition. Using the Luria approach a global score called the Mental Processing Index (MPI), which is reflective of the child’s global intelligence, was determined. The KABC-II has been shown to be a valid measure of cognition in LMICs.Reference Bangirana, Seggane-Musisi and Allebeck 34 , Reference Malda, van de Vijver, Srinivasan, Transler and Sukumar 35
Figure 1 illustrates the data collected and used in this analysis, and how we developed an early life factor model and additional models of predictors of repeat grade.
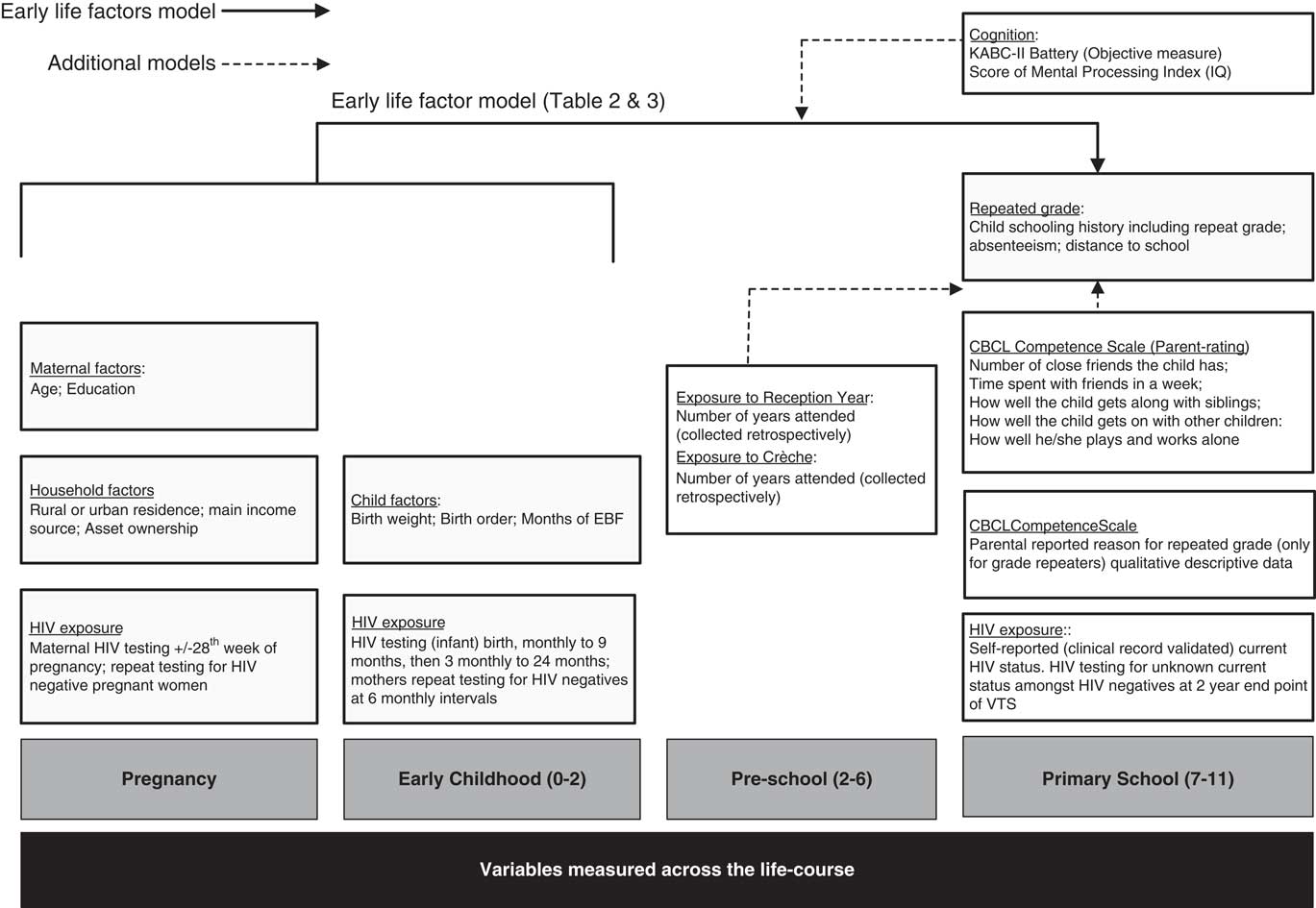
Fig. 1 Variables measured across the life course, and how these were used into models predicting repeated grade.
Definitions
Repeat school grade
In South Africa school starts at age 5 in Grade R (reception class), and finishes with Grade 12 and includes several phases: Grade R to Grade 3 (foundation phase), Grade 4 to 6 (intermediate phase), Grade 7 to 9 (senior phase) and Grade 10 to 12 (further education and training phase). Compulsory schooling extends from Grade one through to the end of the senior phase (expected age of 15 years). Each child in this analysis was classified as having repeated a school grade or not; repeating Grade R was not included as some children spend more than one year in Grade R if they start school very young.
Exclusive Breastfeeding
Standard World Health Organization definitions of exclusive breastfeeding were used, 36 that is the child received breastmilk only and no other fluids or solids. Days of EBF in the first 6 months were counted, and divided into months of EBF.
Statistical analyses
Statistical analyses were conducted using Stata version 13, 37 based on data extracted on 30 October 2014.
Early life factors model
We first estimated a logistic regression of repeated grade (adjusted for children with the same mother, i.e. twins) on early life covariates, including: maternal age, maternal education, type of residence, main income provider, fridge ownership, child’s age, child sex, birth order, birth weight, months of EBF and HIV exposure (mother negative/positive in pregnancy/positive since pregnancy). We were able to include maternal seroconversion since pregnancy as we had data on maternal HIV status during pregnancy from the VTS and her current HIV status in the Saving Brains cohort. Given the significance of child sex in the full model, we repeated the logistic regression stratified by sex.
Additional models
Given the relevance in the literature of current life variables in children’s repeated grade, we also tested the robustness of our findings to mediation by the child’s current cognition (which included quartiles of the sum of scaled scores for the MPI). Since we found a significant difference in children who repeated grades based on current sibling relationships, and given this is supported by the literature,Reference Dai and Heckman 13 we also tested the parent/caregiver reported quality of the sibling relationship (whether the child was reported to get along well with their siblings) in the mediation model.
Since preparation for school through participation in ECD services is known to increase school readiness and subsequent success at school, a separate model examining whether exposure to crèche and/or to reception year were associated with grade repetition was conducted.
Content analysis
For the children who had repeated a grade, content analysis was used to analyze parent responses to the question on the Competence Scale of the CBCL of why the child had repeated a grade. The analysis involved reading through the 894 responses several times to identify commonly reported reasons for repeated grade in the free text of parent answers. These formed a codebook of reasons for repeat grade, which were used to identify common categories. These patterns were clearly distinguished by key words that the parent used for example ‘immature’ ‘not ready’ or ‘absenteeism’ and were mutually exclusive, and grouped into theoretically similar concepts. Once all the data had been coded, categories were reviewed together with the second (a psychologist) and last author (a paediatrician) and consensus was reached whereby all responses were coded and categories were precisely defined.Reference Hsieh and Shannon 38 These categories were then disaggregated by sex and HIV exposure. Given the small cell counts, children who were exposed to HIV in fetal life, and those whose mothers had become HIV infected post pregnancy, were grouped into one HIV exposed group for the purposes of this analysis.
Results
Sample
A total of 906 children from the original VTS completed follow-up in the Saving Brains cohort. For this analysis, we excluded children who had enrolled in grade one for the first time (n=6), as they had not had the opportunity to repeat a grade, and children with missing schooling data (n=6). A final sample of 894 children was included in the analysis.
Rates of repeated grade
Of the 894 children 385 (43.1%) had repeated a grade of whom 242 (62.9%) were boys. Table 1 illustrates sample characteristics by repeated grade.
Table 1 Descriptive statistics of children and mothers by repeated grade (n=894)

Bold values are significant at P<0.05. EBF, exclusively breastfeed.
a Defined as number of days (not cumulative) when child received only breast milk and no other fluids or solids, divided into months.
b In South Africa, grade 12 is the final year of high school.
We found significant group differences between children who had repeated a grade and those who had not (see Table 1). Larger proportions of children who had repeated a grade had a mother with HIV and less education (none or primary school only), compared to those who had not repeated a grade. Group differences on the questions on the Competence Scale revealed only one significant difference; that children who repeated grades were also more frequently reported by caregivers to not get along with their siblings (P=0.022).
Early life factors
The results of the logistic regression model examining early life factors among all children are shown in Table 2. Maternal education at grade 12 relative to no formal education, and birth order of 5+ relative to 1–2, were significantly associated with reduced odds of repeated grade in the adjusted model. In the multivariable analyses allowing for a number of other variables (Table 2), boys were three times more likely than girls to repeat a grade (aOR 2.99; 95% CI 2.22–4.01).
Table 2 Factors associated with grade repetition (n=842)
EBF, exclusively breastfeed.
Bolded results are significant (P<0.05) and italicized results are trends, defined by P>0.05 and P<0.09.
a Defined as number of days (not cumulative) when child received only breast milk and no other fluids or solids, divided into months.
Given the strong associations between child sex and repeated grade, we next tested the model stratified by sex (Table 3). Girls whose mothers had completed grade 12 were less likely to have repeated a grade than those whose mothers had no education (aOR 0.33; 95% CI 0.1–0.9). Girls whose mothers were HIV-positive in pregnancy had double the odds of repeating a grade than those whose mothers were HIV-negative (aOR 2.17; 95% CI 1.3–3.8). However relevant variables were different for boys: ownership of a fridge compared to non-ownership and exposure to breastfeeding for 6-months relative to less than 1 month showed a trend towards reducing the odds of repeating a grade. Maternal HIV status was not associated with grade repetition in boys.
Table 3 Factors associated with grade repetition, by child sex (n=842)

EBF, exclusively breastfeed.
Bolded results are significant (P<0.05) and italicized results are trends, defined by P>0.05 and P<0.09.
a Defined as number of days (not cumulative) when child received only breast milk and no other fluids or solids, divided into months.
Table 3 shows that there was a trend for both boys and girls being higher in birth order (having at least some older siblings) to have reduced odds of repeated grade, but this was only of borderline significance.
Additional models
We next tested the effects of including the child’s MPI score and parent/caregiver report of quality of sibling relationship in the sex-stratified models. For girls, the effect of maternal education (Grade 12) on repeated grade was no longer significant (aOR 0.56; 95% CI 0.2–1.7), most likely due to the well-established strong association between maternal education and child cognition. Most other effects remained consistent: the birth order trend for girls 3rd to 4th or 5th and more and for boys who were 5th or more remained. The effect of HIV exposure in pregnancy for girls remained significant (aOR 2.1; 95% CI 1.7–3.8) and for boys, the effect of fridge ownership became significant (aOR 0.59; 95% CI 0.4–1.0).
Overall, most children started school aged seven or older, just under half of the children attended at least one year of crèche (429/894) and the majority completed at least one reception year (770/894) before entry into first grade. Exposure to crèche (aOR=0.88; 95% CI 0.7–1.2) and reception year (aOR=0.78; 95% CI 0.5–1.1) showed a trend of reducing odds of grade repetition, but were not significant.
Content analysis
Caregiver responses from the question on the Competence Scale regarding the reasons why the parent/caregiver thought the child had repeated grades were grouped into six main categories with several corresponding subcategories.
Overall, a third of children were categorized as having experienced issues with school readiness. This category was defined by caregivers describing their children as being too playful and emotionally immature and unable to self-regulate sufficiently to be successful at school. These descriptions were interpreted as referring to social and emotional development. The next most common reason for failure was children who had experienced difficulty with specific aspects of schooling or subjects, with caregivers reporting that children had difficulty with literacy and with first language isiZulu. Thirdly, a proportion of parent responses alluded to their child experiencing learning difficulties. This category was made up of responses where parents specifically reported problems with not coping, concentration difficulties and being concerned that their child may potentially have a learning difficulty or disability. A smaller, but still substantial group of children were reported to be poorly motivated to attend school, including truancy and other behavioural problems.
These categories and subcategories can be seen in Table 4 where they were further disaggregated by sex and HIV. Z tests for proportions showed that most of these differences were not significant, however for boys there was a significant difference in disrupted schooling by HIV exposure (HIV unexposed 3.8% v. HIV exposed; 12.4% Z=−2.36 P=0.018).
Table 4 Mother/caregiver report on reasons the child repeated a grade, disaggregated by HIV exposure and child sex (n=384)

Bold values are significant at P<0.05.
Discussion
Our study showed a high rate (43%) of grade repetition among children in the early years of school (aged 7–11 years), almost double previous estimates from studies elsewhere in South AfricaReference Anderson, Case and Lam 39 , Reference Hungi 40 and higher than a recent estimate (25.8%) among 15 year olds in the Birth to Twenty Cohort (BT20).Reference Ginsburg, Richter, Fleisch and Norris 41 Similar to literature in South Africa, and internationally,Reference Fleisch and Shindler 24 , Reference Voyer and Voyer 42 boys were three times more likely to repeat a grade than girls, after adjusting for other variables associated with grade repetition.
When examining the characteristics of children who repeated a grade we see that, as has been shown in the United States and rural South Africa,Reference Byrd and Weitzman 10 , Reference Liddell and Rae 43 higher numbers of children whose mothers had a lower education level repeated a grade. Importantly, higher numbers of HIV exposed children had repeated a grade than non-exposed children. Many studies in AfricaReference Ainsworth, Beegle and Koda 18 , Reference Case, Paxson and Ableidinger 44 have suggested that HIV-related orphanhood is associated with poor educational outcomes, including repeated grade.Reference Nyirenda, McGrath and Newell 45 , Reference Bicego, Rutstein and Johnson 46 In this study, we focused on children whose mothers were still alive, with our results suggesting that grade repetition and problems with failures in school begin earlier, and may even precede maternal illness or death.
We also found that good sibling relationships were more common among non-repeaters. While some literature has shown that a larger family size may be detrimental to educational outcomes for children,Reference Downey 47 the potential influence of a good sibling relationship to mediate these effects has been largely unexamined. Some recent literature has suggested that older siblings positively influence the cognitive development of younger siblings.Reference Dai and Heckman 13 It is plausible that children who have good sibling relationships might have better social skills more generally, and as a consequence may have better access to support for schooling, and better relationships with teachers.Reference Rudasill and Rimm-Kaufman 48 However if this was the case, one might have expected to see significant differences with regards to other social relationships, such as those with peers. Meanwhile, in this study, the differences seem to be sibling-specific. The significance of increased birth order reducing the likelihood of grade repetition and the finding that fewer children who got along well with their siblings had repeated a grade, might suggest some potential for older siblings to play a protective role in educational outcomes in this context. In HICs, a higher birth order has been shown to result in poor educational outcomes as parents invest fewer resources in each child as the family grows.Reference Downey 47 , Reference King 49 However, the inverse of this hypothesis has been found in LMICs with children and adolescents.Reference Cockburn and Dostie 50 – Reference Niehaus 52 In South Africa, researchers have argued that older siblings often contribute financially to younger siblings’ education,Reference Niehaus 52 and may be closely involved with younger siblings’ daily lives, in particular since it is culturally normative to take on increased responsibilities towards younger siblings.Reference Cicirelli 53 Older siblings who have a good relationship with younger siblings might be more likely to be involved with supporting and facilitating learning, which may be particularly important in South Africa where, given historical disadvantages, siblings are likely to have received a higher level and quality of education than their mothers.Reference Soudien 54 This might point to opportunities for family interventions to support older siblings in the care of younger siblings in the household. Further research is needed to understand the nature of sibling relationships in large, extended, rural households.
When we examined the early life factors, stratified by sex, we found maternal education to reduce odds of grade repetition for girls, but not boys. The influence of maternal education for girls only was also found in a study from Guinea in Western Africa.Reference Glick and Sahn 55 In Western Africa the authors proposed that this disparity by sex could be attributed to maternal household power, particularly in patriarchal societies where schooling access is low. For instance, if a mother has a higher level of education she may have increased decision-making power in the household and direct resources towards her daughter’s education, even though the culture may favour the boy child.Reference Glick and Sahn 55 A limitation of the current study is that we did not measure father’s education. Previous research from the Africa Centre settingReference Case, Paxson and Ableidinger 44 showed some selective sex effects following orphanhood, whereby maternal outcomes were more strongly associated with girl children’s outcomes and paternal outcomes more associated with boys’ outcomes.
Maternal HIV in fetal life was associated with an increased risk of repeating grade for all children, with the strongest effect for girls. While the existing literature has shown HIV-exposed girls to be more vulnerable to poor educational outcomes,Reference Guo, Li and Sherr 15 this study shows the effect to be stronger when the girl is exposed to HIV from fetal life, as opposed to during childhood. We expect that this may be a result of the effects of the mother’s longer exposure to infection, which may have led to ill health and reduced caregiving capacity over time. This is consistent with literature that supports the hypothesis that maternal HIV impacts on children’s education indirectly through the caregiver.Reference Orkin, Boyes, Cluver and Zhang 57
Regarding impact on girls, previous studies have hypothesized that the girl child’s vulnerability is linked to the mother’s illness which in turn leads to increased domestic responsibilities, chores and care giving activities when their mothers are ill.Reference Foster and Williamson 58 , Reference Robson 59 This in turn is associated with a drop in school attendance.Reference Case, Paxson and Ableidinger 44 However evidence from parent report in our study does not corroborate either maternal illness or disrupted schooling as primary reasons for repeating grades among girls. Instead, a lack of school readiness and developmental immaturity, along with specific learning problems were more commonly cited as reasons for grade repetition among HIV-exposed girls. Interestingly, HIV-exposed girls were as commonly reported to have motivational problems (including a lack of focus and truancy) as HIV-exposed boys. Research is needed to elucidate the pathways of this effect on girls’ education in the early years in order to inform interventions, as it is likely pathways are more complex than the onset of parental illness alone. Understanding these pathways is also made more urgent given that HIV exposure for girls is a predictor of later engagement in HIV-risk behaviourReference Cluver, Orkin, Boyes and Sherr 60 and additional years in school has been shown to mediate this risk.Reference De Neve, Fink, Subramanian, Moyo and Bor 26
When current cognition and the effect of sibling relationships were tested as mediators, socioeconomic status, measured here by fridge ownership, was significantly associated with a reduced likelihood of repeating a grade for boys. While there is evidence that boys living in poverty are more stunted in their physical development than girls in sub-Saharan Africa,Reference Wamani, Åstrøm, Peterson, Tumwine and Tylleskär 61 the mechanisms by which poverty affects schooling outcomes for boys particularly, are less clear. Some literature has suggested that the number of hours in a day that a boy attends school in South Africa is particularly vulnerable to variation in permanent income for the household.Reference Cockburn and Dostie 50 It is hypothesized that in these income insecure settings, boys (more than girls) may be more vulnerable to being drawn into child labour or not being able to afford school fees, which in turn might increase disruptions in attendance.Reference Edmonds 62 For instance, boys’ school attendance in Ethiopia was found to be influenced by partaking in farming activities and generating income for the family.Reference Cockburn and Dostie 50
In the sex stratified model the association between maternal HIV status and repeating a grade did not reach statistical significance for boys. However in the parent reports for boys who did repeat a grade, we see a significantly higher proportion of HIV-exposed boys being reported to have failed as a result of school disruption compared to HIV-unexposed boys. Disrupted schooling included inconsistent attendance, school relocation and missed examinations. This may lend support to the hypothesis that boys’ schooling is disrupted by socio-economic factors, and that this is particularly heightened in the presence of maternal HIV. However, it is equally plausible that a mother’s HIV status has indirect effects for boys. For example, a mother may have relocated to access HIV treatment, which might have been good for her health, but resulted in school mobility which may have had disruptive effects on her child’s education outcomes. In a cross-sectional analysis of the BT20 cohort, school mobility was one of the stronger factors associated with having repeated a grade by age 15,Reference Ginsburg, Richter, Fleisch and Norris 41 adding support to existing evidence from Africa which shows that HIV-exposed children (including boys) are prone to disrupted schooling.
We found that, among subject specific learning problems, the most common was related to children’s first language (IsiZulu). For many South African children, the first two years of schooling may be the first time they learn English (their second language) and it will also be the first time they attempt to read and write in their mother tongue. Challenges with the instruction of young children in isiZulu have been cited in the literature, and while mother-tongue learning is encouraged in KwaZulu-Natal, teachers often opt to focus on English, perceiving it to be the more important language to master for later opportunities.Reference Mashiya 63 This may result in inadequate support for language subjects in the early years, yet the child’s passing a grade is contingent on them passing their first language subject from as early as first grade.
A worrisome number of children (11%) were reported by their parents to have failed due to motivational problems, including truancy. These children may be exhibiting the first signs of becoming disengaged in school which may lead to eventual dropout,Reference Lehr, Sinclair and Christenson 64 which is concerning given their young age. Estimates of truancy are poorly documented, in particular for younger children, but it has been acknowledged as a problem in South Africa.Reference van Breda 65 A study of truancy among adolescents in Swaziland found rates of 21.6% (27% boys; 17% girls). Being a male, having been bullied, lower school grades, and alcohol use were positively associated with truancy. Home environment has been shown to be an important determinant of truancy, with parental supervision and involvement curbing truancy and promoting motivation among children at school.Reference Hill and Tyson 66 – Reference van Breda 68 Motivational problems as a reason for failure were as common among girls as boys in this research.
Lastly, our results also point to the importance of preparation for schooling and subject specific schooling support in the early years of a child’s life. When examining other factors commonly reported as reasons for failing grade by the parent, the most common was a lack of school readiness and what parents described as developmental immaturity, followed by subject-specific learning problems and overall learning problems. Children reported to be developmentally immature may not be ready for school, as is commonly reported among children living in poverty.Reference Welsh, Nix, Blair, Bierman and Nelson 69 Interventions focused on improved screening of school readiness could be promoted, as well as early identification of learning disabilities, so the appropriate referral can be made. While children should not enter school before they are ready, later school entry can also have a negative impact on educational attainment.Reference Ginsburg, Richter, Fleisch and Norris 41 As such, efforts to improve school readiness through increased quality, or more years of, reception year may be beneficial. However, as illustrated in this research access to reception schooling alone may not be sufficient. Future research could examine the effects of sibling and family support on younger children’s schooling, and the advantages this may offer as a potential area of intervention support for particularly vulnerable, including HIV-exposed, children.
The limitations of this study include that we did not collect data on the quality of schooling, and that our data is limited to parental report. Further, we do not include data from children of their understanding of reasons for repeated grade or reports from teachers.
The strengths of this research include its longitudinal design, the inclusion of both HIV-exposed (during pregnancy and post pregnancy) and HIV-unexposed children, the examination of earliest records of failures in school, and an objective measure of children’s cognition. Importantly, while we are limited to parental report, we used well validated measures to capture these. To our knowledge this is the only examination of early life factors associated with repeated grade in early primary school in South Africa. We find that HIV exposure has particularly detrimental effects for girls. Although the mechanism of this requires further research, it is likely to reflect social, rather than biological, effects of exposure. While poverty has unfavourable effects for boys, they are also vulnerable to school disruptions, an area requiring further research. Maternal education and support from older siblings along with early school readiness preparation may provide opportunities for intervention. Educational outcome are directly linked to longer term health and human capital outcomes, and early failures are strong predictors of later educational outcomes. Understanding the mechanisms by which children fail in school can inform intervention investments, and further research is needed, in particular to understand the differential gender effects.
Acknowledgements
The authors are grateful to all women and children enrolled in the study, the field and data management team, in particular Samu Dube. They thank Colin Newell for data management during the study, Kobus Herbst and Dickman Gareta and the research platform management team for support during the analysis. They thank the Community Liaison Office of the Africa Centre and Community Advisory Board for their guidance throughout the study.
Joanie Mitchell contributed to interpretation of data, drafted the manuscript and critically revised the manuscript. Brian Houle contributed to the analysis and interpretation of the data. Tamsen Rochat and Ruth Bland contributed to interpretation of data and critically reviewing the manuscript. Marie-Louise Newell and Alan Stein critically revised the manuscript and contributed to refining the analysis and manuscript. The investigators of the Vertical Transmission Study are acknowledged and include Professor Hoosen Coovadia (PI), Anna Coutsoudis and Nigel Rollins.
Financial Support
The authors are grateful to Grand Challenges, Canada, who funded this re-enrolment study as part of their ‘Saving Brains’ initiative (Grand Challenges 0063-03).
Conflicts of Interest
None.
Ethical Standards
Ethics permission was granted by the Biomedical Research Ethics Committee (BREC), University of KwaZulu-Natal, South Africa (BF184/12).






 Open access
Open access