Many epidemiological studies have identified positive associations between whole-grain consumption and reduced risk of mortality and chronic disease such as type 2 diabetes, CVD, cancer and obesity(Reference Chen, Tong and Xu1–Reference Newby, Maras and Bakun7). As a result, whole-grain consumption is recommended internationally and incorporated into dietary guidelines across the globe(Reference Ferruzzi, Jonnalagadda and Liu8). In Australia, the Grains and Legumes Nutrition Council (a not-for-profit organisation) recommends a 48 g/d whole-grain daily target intake(Reference Griffiths and Nestel9), while in Nordic countries, these recommendations are higher and embedded within dietary guidelines. In Sweden, individuals are encouraged to aim for a whole-grain intake of 75 g/10 MJ per d, while in Denmark and Norway, 75 g/d and 70–90 g/d, respectively, are recommended(Reference Brugård Konde, Bjerselius and Haglund10–13).
Despite an abundance of recommendations, dietary intake studies among many countries report low consumption of whole grains(Reference Galea, Beck and Probst14–Reference Sette, D’Addezio and Piccinelli19). However, the intake values gleaned from the literature may be difficult to compare due to inconsistencies in the calculation of whole-grain intake, particularly where only contributions from ‘whole-grain foods’ are included(Reference Ferruzzi, Jonnalagadda and Liu8,Reference Wu, Flint and Qi20) . Discrepancies in studies regarding associations between whole-grain intake and health outcomes, in particular mortality, are also noted. For example, some studies(Reference Jacobs21–Reference Jacobs24) indicate significant associations with reduced mortality risk, while no associations are found among others(Reference Sahyoun, Jacques and Zhang25,Reference He, van Dam and Rimm26) . Again, varied methods of estimating whole-grain intake may partly explain these anomalies. This is problematic as dietary guideline recommendations for whole-grain intake depend on the associations drawn from such studies, which may not be directly comparable. It is recognised that agreement on a unified whole-grain food definition is needed(Reference Ferruzzi, Jonnalagadda and Liu8), although the relevance of such definitions may be better reflected in public health efforts to promote whole-grain intake. In contrast, the best practice for reporting of whole grains in research is suggested as a gram value gained from all foods(Reference Ross, Kristensen and Seal27).
Recently, the Whole Grain Initiative has worked on defining whole-grain foods, with an aim of encouraging whole-grain intake(28). Previously, the Healthgrain forum, an international body aimed at promoting production and consumption of healthy cereal foods, made recommendations for a whole-grain food definition that can be applied globally(Reference Ross, van der Kamp and King29). As outlined in Ross et al. (Reference Ross, van der Kamp and King29), it is recommended that a whole-grain food contains ≥30 % whole grain on a dry weight basis, more whole than refined grain ingredients and meet accepted standards for ‘healthy foods’ based on local regulations. Based on the final criterion, foods in Australia that are classified as ‘discretionary’ are not considered a whole-grain food. These discretionary foods tend to be higher in saturated fat, added sugars, added salt and energy(30), and limited consumption is recommended. Classification of these foods is based on specification and/or inference in the 2013 Australian Dietary Guidelines and supporting documents. For grain-based products, discretionary classification was given to breakfast cereals where sugar content was >30 g/100 g, or >35 g/100 g for breakfast cereals with added fruit. Mixed grain-based dishes such as muesli bars were given discretionary classification if saturated fat was >5 g/100 g. Whole-grain content is not considered to determine discretionary classification. This differs to countries like Sweden, where ‘healthy’ rather than ‘unhealthy’ classification is applied to foods. Here, foods that display the Keyhole symbol are identified as ‘healthy’ and therefore meet the last criterion of the Healthgrain definition. Foods displaying the Keyhole must fulfil certain conditions around fat, sugar, salt, dietary fibre, whole grain, fruit and vegetable content(31). These conditions are based on the Nordic Nutrition Recommendations(32) and vary between food groups. For example, breakfast cereals are Keyhole eligible if they contain at least 55 % whole grain, at least 6 g/100 g dietary fibre and do not exceed 13 g/100 g sugar, 9 g/100 g added sugar, 1 g/100 g salt or 8 g/100 g fat.
We have previously shown that the application of a whole-grain food definition has significant impacts when estimating whole-grain intakes based on an Australian food supply(Reference Kissock33). Application of the Healthgrain whole-grain food definition significantly lowered estimations of whole-grain intake by up to 8 g/10 MJ per d in comparison with absolute grams of whole grain. The current study aimed to firstly determine the varied impacts of a whole-grain food definition when estimating whole-grain intakes in a Swedish cohort compared with the Australian context. It secondly aimed to investigate whether utilisation of whole-grain food definitions affects the observed associations between whole-grain intake and CVD risk factors, including anthropometric, blood pressure and biochemical measures. Data from two national surveys conducted in Australia and Sweden were utilised. Swedish data are a useful comparison as firstly whole-grain intake in Nordic countries is higher than Australia (and countries such as the USA and UK). Second, grain products in particular differ in their origin between countries, for example, higher rye use in Sweden. Comparing these varied contexts will provide insights into the impact of different whole-grain definitions across food supplies.
Methods
The current study explored the application of the Healthgrain whole-grain food definition to dietary intake data within the Australian National Nutrition and Physical Activity Survey (NNPAS) 2011–2012 (published previously(Reference Kissock33)) and the Swedish Riksmaten Adults 2010–2011. Whole-grain intakes were estimated based on foods complying with the Healthgrain definition and compared with intake where all grams of whole grain from any food source were included. Following this, the impact of utilising the Healthgrain definition on the association between whole-grain intake and CVD risk factors, namely anthropometric, blood pressure and biochemical measures, was investigated.
Data and survey population
The Australian NNPAS 2011–2012 collected data specifically related to nutrition and dietary intake on 12 153 participants aged 2 years and over from 9519 households across Australia. Selection of participants used a stratified multistage area sample of private dwellings. The Swedish national dietary survey, Riksmaten Adults 2010–2011, collected dietary intake for 1797 participants aged 18–80 years. The nation-wide survey recruited and selected participants from the population registry representative of sex, age group and region in the adult population. Further details related to participant recruitment and selection of each survey are described elsewhere(34–Reference Amcoff, Edberg and Barbieri36).
Dietary intake data
NNPAS 2011–2012 dietary intake data were collected through two separate 24-h recalls. The first 24-h recall was conducted through face-to-face interviews with computer assistance (n 12 153), while a second 24-h recall was conducted via telephone (n 7735 with a 63·6 % response rate)(37). Specific details are described elsewhere(34). To note, this study specifically analysed data from the Australian Health Survey: Nutrition and Physical Activity, 2011–12 expanded confidentialised unit record files data set.
Dietary data in the Riksmaten Adults 2010–2011 were obtained through a 4-d dietary registration using a web-based tool developed by the Swedish Food Agency. This tool has been previously validated among middle-aged adults for energy and macronutrient intake using the doubly labelled water technique(Reference Nybacka, Bertéus Forslund and Wirfält38), in addition to intake of fruit, vegetables and whole grains using objective biomarkers(Reference Nybacka, Lindroos and Wirfält39). The ability to capture whole-grain intake was weak; however, correlations between the alkylresorcinol biomarker and consumption were similar to previous studies. All data were collected by Statistics Sweden, on behalf of the Swedish Food Agency. Further detail of the Riksmaten adults 2010–2011 methods is available elsewhere(Reference Amcoff, Edberg and Barbieri35,Reference Amcoff, Edberg and Barbieri36) .
Estimation of whole-grain intakes
Methods to estimate whole-grain intakes were adapted from work previously published by the authors(Reference Kissock33). Briefly, whole-grain intakes were calculated based on four separate approaches surrounding application of the Healthgrain whole-grain food definition. Collectively, these whole-grain food definition approaches include approach 1: total whole-grain intake in grams (no whole-grain food definition), including ‘unhealthy foods’ (1a), and excluding ‘unhealthy foods’ (1b); and approach 2: applying the Healthgrain whole-grain food definition, including ‘unhealthy foods’ (2a) and excluding ‘unhealthy foods’ (2b).
The Australian whole-grain database(Reference Galea, Dalton and Beck40), based on the Australian Food, Supplement and Nutrient Database 2011–2013(41), was previously expanded to identify compliance of foods with the Healthgrain whole-grain food definition(Reference Kissock33). Here, ‘unhealthy foods’ were identified based on ‘discretionary’ classification within the Australian Health Survey: Users’ Guide, 2011–2013 – Discretionary Food List(42). In the Swedish context, the Swedish Food Agency’s national food composition database (Livsmedelsdatabasen, version Riksmaten adults 2010–11) was utilised. This database version was developed as a food list to be used specifically with the Riksmaten adults 2010–2011 for the purpose of dietary intake analysis and hereafter referred to as the Riksmaten adults food list or survey food list. Methods similar to Australian analysis were used to determine compliance of the Riksmaten adults food list to the Healthgrain whole-grain food definition (online Supplementary Material 1). However, Swedish foods do not receive ‘unhealthy’ or ‘discretionary’ classification. Instead, the Keyhole – a food label to help identify healthier products within food groups – is used, and ‘unhealthy foods’ are identified as those not meeting Keyhole criteria, that is, ‘non-Keyhole’ foods. In Swedish intake calculations, all 4 d of dietary intake data (where available) were used to estimate whole-grain intakes. As some participants completed <4 d of dietary registrations, the multiple source method (MSM) was utilised to calculate usual whole-grain intakes for each participant, for each of the four approaches. The MSM is an online-based statistical method utilising a three-step procedure involving regression models to account for usual intake from multiple dietary data collection(43). Methods related to the MSM programme are provided elsewhere(Reference Kissock33). Australian whole-grain intakes were estimated using ‘day 1’ dietary intake data only (n 12 153) as the MSM programme could not be used due to privacy requirements associated with utilisation of Australian Bureau of Statistics expanded confidentialised unit record files data.
Initially, whole-grain intakes were calculated for each of the four approaches on a gram weight per d basis for the total participants and further by various sex and age categories. Age categories in Australia were based on age ranges outlined in the Australian nutrient reference values for children, adolescents and adults(44). Age categories in Sweden were based on age ranges outlined in the Nordic Nutrition Recommendations 2012(32). Whole-grain intakes were further adjusted for daily energy intakes as g/10 MJ per d, to account for differences in total dietary intakes between age and sex(Reference Mann, Pearce and McKevith15).
Health outcome measures
Anthropometric, blood pressure and biochemical measures were available in the Australian data, while anthropometric and a single biochemical measure of C-reactive protein (CRP) were available in the Swedish data. In the Australian context, height (cm), weight (kg) and waist circumference (WC, cm) were obtained by trained interviewers using a stadiometer, digital scales and metal tape measure, respectively. Systolic and diastolic blood pressure were measured using an automated blood pressure monitor by trained interviewers. Further details on the methodology behind anthropometric and blood pressure measurements within the NNPAS 2011–2012 are described elsewhere(34).
Data related to Australian biochemical measures were obtained from the National Health Measures Survey 2011–2012. The National Health Measures Survey measured specific biomarkers for chronic disease and nutrition status using blood and spot urine samples from a subsample of participants from the NNPAS 2011–2012 and National Health Survey 2011–2012. Biochemical measures included total cholesterol, HDL-cholesterol and LDL-cholesterol (mmol/l), fasting TAG (mmol/l), fasting blood glucose (mmol/l), apoB (g/l), HbA1c (%) and CRP (mg/l). Results for LDL-cholesterol, TAG and plasma glucose were only obtained if the participant fasted for 8 h or more prior to providing the blood sample. Further details about each measure are provided elsewhere(45).
Swedish anthropometric measurements including height, weight, WC and hip circumference were obtained through completion of a web-based, self-reported questionnaire. Participants who did not have access to a computer were provided with a paper version of the questionnaire. Instructions were provided to participants on how to measure waist and hip circumferences. Weight was reported in kg, while height, WC and hip circumference were reported in cm. For biochemical measures, 300 participants of a 1008 subsample agreed to provide blood and urine samples. All blood and urine samples were collected by seven Occupational and Environmental Medicine clinics across the country, as previously reported(Reference Öhrvik, Lemming and Nälsén46). For the purpose of this study, only values relating to CRP were included.
Statistical analyses
Analyses were conducted using Stata (StataCorp Stata Statistical Software: Release 15, 2017). Australian analyses utilised the complex survey design method, incorporating sampling and replicate weights to generalise the results to the Australian population at the time of the survey(Reference Birrell, Steel and Batterham47). Two separate sets of weighting were used in order to maximise the population size and increase precision of results for each health outcome measure. Analyses surrounding whole-grain intakes, anthropometric and blood pressure measures used person-level weights, while analyses surrounding population characteristics and biochemical measures utilised biochemical weights. Weighting was available for Swedish data, although it was not appropriate for use when calculating whole-grain intakes or investigating associations with anthropometric measures. Participants from the Riksmaten adults 2010–2011 were derived from two sample populations: (1) the main sample (n 1436) and (2) the biochemical sample (n 361), where weighting was calculated differently for each sample. Since data on dietary intake and anthropometric measures were taken from both survey samples, corresponding weightings for each participant were derived from different methods and therefore could not be used in conjunction with one another. Previous analyses comparing weighted and unweighted intakes (macronutrients and certain food groups) for each sample showed minimal differences in the means, particularly for carbohydrates (Livsmedelsverket – unpublished results). Furthermore, participant sex proportions did not differ greatly from the representatively drawn sample(Reference Amcoff, Edberg and Barbieri35), indicating that the combined population is generally representative. As CRP analysis was conducted on a small sample size (n 280) and was measured only for participants within the biochemical sample, weighting was applied to regression analyses.
Whole-grain intakes were calculated as g/d and energy-adjusted g/10 MJ per d for all participants and age/sex subgroups for each whole-grain food definition approach. Swedish whole-grain intakes were based on MSM-adjusted intake values. Change in energy-adjusted whole-grain intakes across approaches, in comparison with absolute intake (approach 1a), was calculated. The proportion of participants with any decrease in whole-grain intake and within specified ranges of decrease was determined (unweighted analyses). Three separate comparisons for significant mean differences between whole-grain food definition approaches were conducted through paired t tests on Swedish data only. A statistically significant difference was determined at P < 0·05. Similar comparisons were conducted previously on Australian data(Reference Kissock33) and therefore are not reported here; however, methodology for estimation of whole-grain intake differed slightly. Participants were separated into ‘non consumers’ and quartiles of consumers, hereafter referred to as categories of whole-grain intake, for each whole-grain food definition approach and demographic characteristics analysed. Continuous variables were analysed through linear regression with a combination of age, sex and/or energy intake as confounding variables. A P-value for linear trend across groups was determined. Categorical variables were analysed through Pearson’s χ 2. An overall significant difference was observed at P < 0·05. A significant difference between two groups was observed at P < 0·005 through individual Pearson’s χ 2 analysis with a Bonferroni correction for multiple comparisons.
Linear regression analyses were conducted to determine the associations between whole-grain intake as categories and grams with anthropometric, blood pressure and biochemical measures for each whole-grain food definition approach. Analyses for categories of intake used ‘non-consumers’ as the reference category (i.e. 0 g of whole-grain intake). Normality and descriptive statistics of each outcome variable were analysed prior to conducting regression analyses. Due to non-normal distributions, linear regressions were conducted based on the natural log values for total cholesterol, LDL-cholesterol, HDL-cholesterol, fasting TAG, fasting blood glucose levels and HbA1c in the Australian data, and CRP in the Swedish data. All log-transformed output data were back-transformed to the normal scale post-regression analysis. In the Australian data, a Tobit model for linear regression was applied to CRP in order to account for left censoring of data. Normality of residuals, homoscedasticity and linearity were checked for each regression analysis.
Regression models and confounding variables differed depending on the outcome variable of interest (online Supplementary Table S3). Adjusted means of outcome variables were calculated for categories of whole-grain intake for each whole-grain food definition approach. A P-value for linear trend and P-value for significant difference were reported. For grams, regression analyses, beta-coefficient, standard error, P-value for linear trend and 95 % CI were reported. Statistical significance was determined at P < 0·05. In Australian characteristic and regression analyses, participants were excluded if they were ≤18 years of age (n 2812) or their energy intake:BMR ratio was <0·90 based on Goldberg cut-offs(Reference Goldberg, Black and Jebb48) (18·7 % of adult participants, 15·2 % missing data). In the Swedish analyses, participants were excluded if they had an energy intake:BMR ratio <0·93 or >3·01(Reference Amcoff, Edberg and Barbieri36), based on cut-off values previously determined specifically for the survey (18·5 % of participants, 0·9 % missing data). In both contexts, participants were excluded if at least one confounding variable or the outcome of interest was missing.
Ethics
Ethics was not required due to the secondary analysis nature of this study. Accessibility and dissemination of the Australian data are governed by section 15 of the Census and Statistics (Information Release and Access) Determination 2018 under the Census and Statistics Act 1905. Approval for access and utilisation of the Swedish data was sought and granted by the Swedish Food Agency. The collection of blood samples in the Riksmaten adults survey was approved by the Uppsala University ethics committee, and all participants provided verbal consent to participate.
Results
Compliance of foods with the Healthgrain definition
Compliance of food items within the Riksmaten adults food list with the entire Healthgrain definition was low, such that only twenty-nine out of 155 food items containing whole grain (after exclusion of corn) were compliant (see online Supplementary Material 1). Our previous work on Australian foods showed 214 out of 609 food items were compliant with the entire Healthgrain definition(Reference Kissock33).
Characteristics of the population
Demographic characteristics of Australian and Swedish adult survey populations were similar (see online supplementary material, Supplemental Tables S4 and S5).
Whole-grain intakes
Here, utilising a single day of Australian dietary intake data produced similar results to previously published work utilising 2-d data(Reference Kissock33). Median and mean intakes of the adult population decreased incrementally from approach 1a through to approach 2b, including energy-adjusted values (Table 1, see online supplementary material, Supplemental Table S6). Male adults had higher median whole-grain intakes than females across approaches; however, females showed higher relative intakes when adjusting for energy, with the exception of approach 2b where both male and female median intakes were equal to 0. Within age category-specific analyses, those > 70 years old were the highest whole-grain consumers across all approaches, while the 19–30 age group consumed the lowest (Table 2, see online supplementary material, Supplemental Table S7). Interestingly, the 31–50-year-old age group equally consumed the least in approaches where a whole-grain food definition was applied (i.e. approach 2). This indicates that the 19–30 age group generally consumes less whole grain, and together with the 31–50-year-old group consume foods low in whole grain and/or high proportions of refined grain. The proportion of Australian participants with any decrease in whole-grain intake, compared with absolute intake (approach 1a), increased across approaches (see online supplementary material, Supplemental Table 8). We found the highest proportion when comparing to approach 2b (42·8 %) where the majority of participants (22·6 %) had a 75–100 % decrease of whole-grain intake. There were similar findings between males and females.
Table 1. Energy-adjusted whole-grain intakes of Australian and Swedish adults across whole-grain food definition approaches*,†
(Median values and interquartile range)
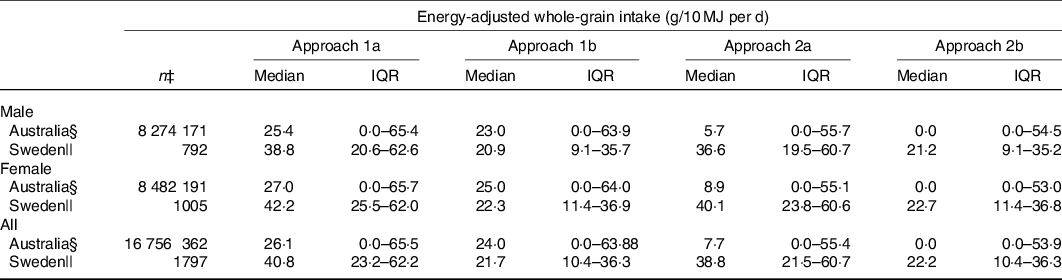
* Australian adults = 19 years and over; Swedish adults = 18–80 years.
† Approach 1a, no whole-grain food definition (including discretionary); Approach 1b, no whole-grain food definition (excluding discretionary); Approach 2a, whole-grain food definition (including discretionary); Approach 2b, whole-grain food definition (excluding discretionary).
‡ n in Australian data derived using sampling and replicate weights within a complex survey design method.
§ Data based on 1 d of dietary intake from National Nutrition and Physical Activity Survey (NNPAS) 2011–12.
|| Data based on MSM-adjusted values from up to 4 d of dietary intake from Riksmaten Adults.
Table 2. Energy-Adjusted whole-grain intakes of Australian and Swedish adults across age subcategories and whole-grain food definition approaches*
(Median values and interquartile range)
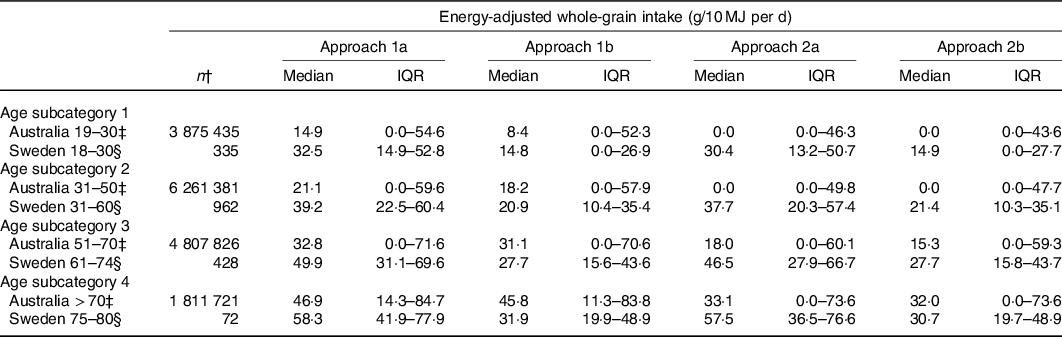
* Approach 1a, no whole-grain food definition (including discretionary); Approach 1b, no whole-grain food definition (excluding discretionary); Approach 2a, whole-grain food definition (including discretionary); Approach 2b, whole-grain food definition (excluding discretionary).
† n in Australian data derived using sampling and replicate weights within a complex survey design method.
‡ Data based on 1 d of dietary intake from National Nutrition and Physical Activity Survey (NNPAS) 2011–12.
§ Data based on MSM-adjusted values from up to 4 d of dietary intake from Riksmaten Adults.
In Swedish analysis, whole-grain intakes did not decrease with each subsequent whole-grain food definition approach. While the median and mean intakes of whole grain greatly decreased when applying the entire Healthgrain definition (approach 2b) in comparison with including all grams of whole grain from any food source (approach 1a) (Table 1, see online supplementary material, Supplemental Table S6), large decreases were also prevalent when excluding non-keyhole foods (i.e. approach 1b/2b). Interestingly, median intakes were higher in approach 2b when compared against approach 1b. Similar to Australian data, whole-grain intakes were highest among the eldest age group (≥75 years), while lowest intakes were among the younger age group of 18–30 years, across all approaches (Table 2, see online supplementary material, Supplemental Table S7). This is indicative that consumption of non-Keyhole foods and to some degree the consumption of foods containing small amounts of whole grain are consumed in similar amounts across age groups. Like Australian analyses, males had higher median and mean whole-grain intakes; however, females had higher relative intakes after adjusting for energy. However, Swedish analyses showed larger proportions of participants with any decrease in whole-grain intake (see online supplementary material, Supplemental Table S8). As might be expected, the proportion of any decrease was highest among comparisons between absolute intake (approach 1a) and approach 2b (90 %), although a larger number of participants had a <50 % decrease in whole-grain intake (< 25 % decrease = 25·3 %; 25–50 % decrease = 24·9 %). Again, findings were similar between males and females.
Comparison of approaches (Swedish data only)
Significant mean differences (P < 0·05) of whole-grain intake were found for the total adults when comparing approach 1a with 2b (comparison 1) and further between approach 1a and 2a (comparison 2) (Table 3). These significant differences remained when comparing by age categories. Difference in mean intake was up to 20·5 g/d (24·6 g/10 MJ per d) in comparison 1, while difference in intake was up to 2·2 g/d (2·7 g/10 MJ/d) in comparison 2. Interestingly, when comparing approach 1b with 2b (comparison 3), no significant mean differences were found for the total adult population (P > 0·05). However, a significant difference was evident when comparing by age categories for the 31–60, 61–74 and ≥ 75-year-old groups. This was similar for energy-adjusted values, although a significant difference was not present for the 31–60 years age group.
Table 3. Difference in mean whole-grain consumption between whole-grain food definition approaches for Swedish adults*,†
(Mean values with their standard errors)
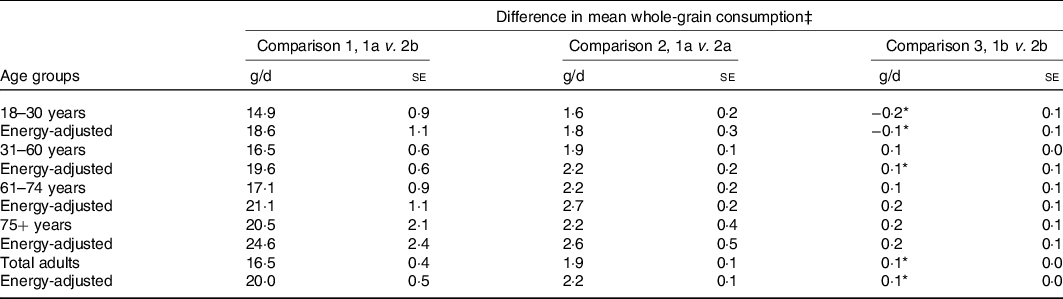
* Not statistically significant (P ≥ 0·05).
† Approach 1a, no whole-grain food definition (including non-keyhole); Approach 1b, no whole-grain food definition (excluding non-keyhole); Approach 2a, whole-grain food definition (including non-keyhole); Approach 2b, whole-grain food definition (excluding non-keyhole).
‡ Difference in means obtained through paired t test (test for equality of means).
Associations with health measures
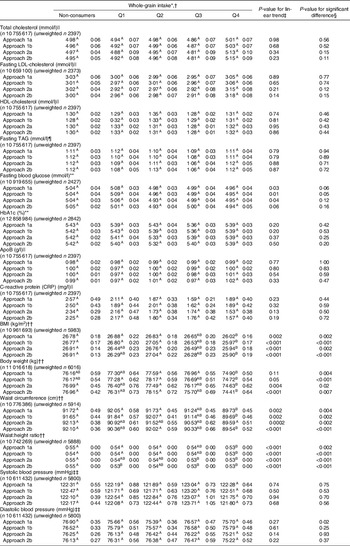
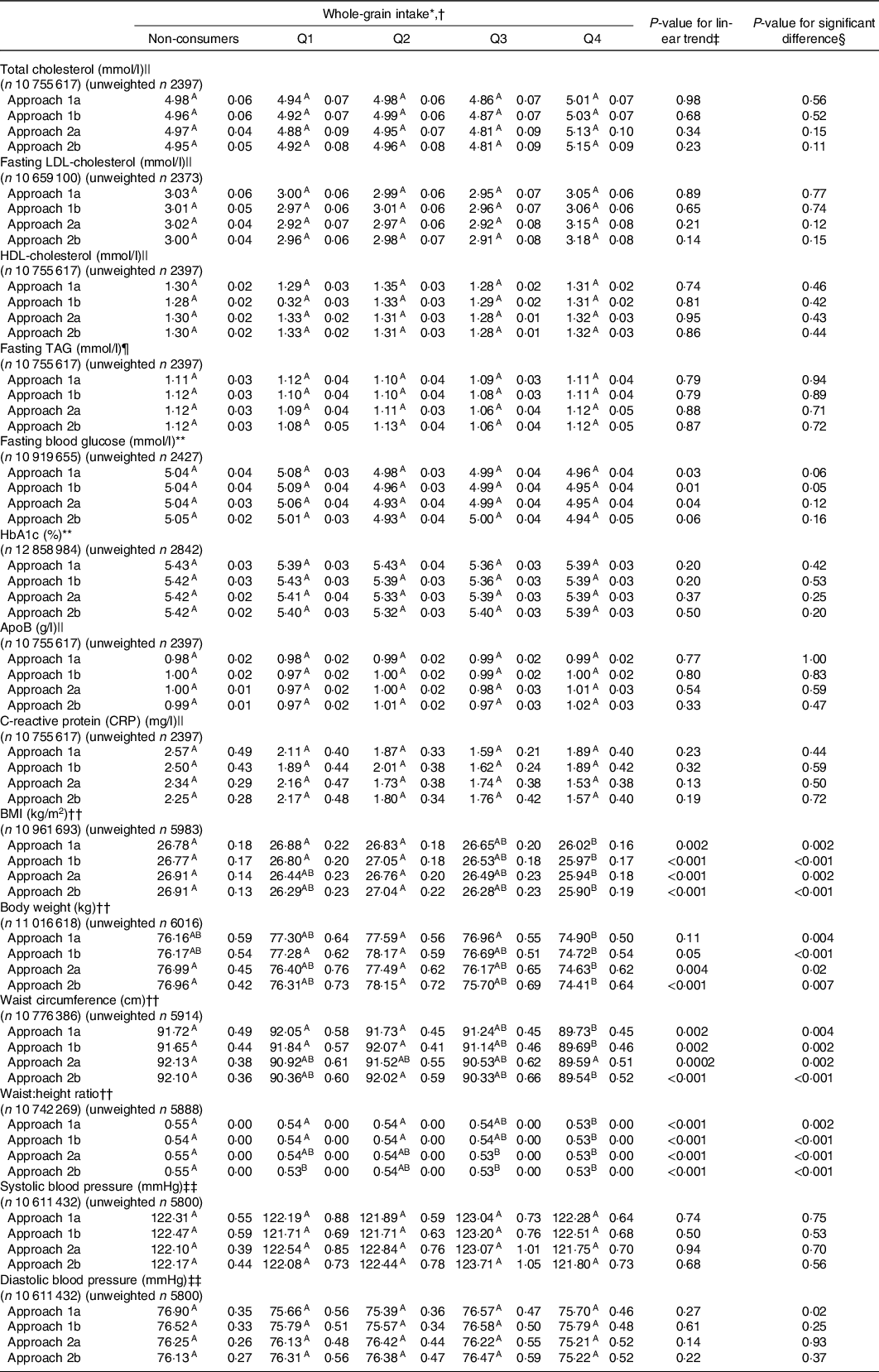
In general, application of a whole-grain food definition did not substantially change the apparent associations between whole-grain intake and CVD risk factor measures, although some differences were noted. In the Australian context, differences in associations between categories of whole-grain intake with body weight and fasting blood glucose were shown. Here, categories of whole-grain intake were significantly associated with a decrease in body weight in approaches where a whole-grain food definition was applied (approach 2a/2b) (Table 4). There was also a significant decrease in fasting blood glucose for approach 1a, 1b and 2a; however, significance was lost when applying the entire Healthgrain definition (approach 2b, P = 0·06). There were no significant changes in associations between categories of whole-grain intake and total cholesterol, fasting LDL-cholesterol, HDL-cholesterol, fasting TAG, HbA1c, apoB, CRP, BMI, WC, waist:height ratio, systolic or diastolic blood pressure across approaches. Similarly, there were little differences in associations when applying a whole-grain food definition for analyses using grams of whole-grain intake (online Supplementary Table S9). A significant association with a decrease in fasting blood glucose was present when including absolute grams of whole grain but excluding discretionary intake (β = −0·015, P = 0·04) (approach 1b), while there were no statistically significant associations among the other approaches.
Table 4. Association between categories of energy-adjusted whole-grain intake and CVD risk factor measures for different whole-grain food definition approaches in Australian adults
* Values are reported as
 $\mathop x\limits^ - $
| sem.
$\mathop x\limits^ - $
| sem.
† Means sharing capital letters within rows are not statistically significant from each other. Significance is determined at P < 0·005 (Pairwise comparison with Bonferroni correction for multiple comparisons).
‡ P-value for linear trend. Significance is determined at P < 0·05.
§ P-value for significant difference determined through test for equality of means. Significance is determined at P < 0·05.
|| Survey linear regression adjusted for age, sex, energy intake, education level, physical activity, current smoking status, intake of saturated fat, trans-fat, monounsaturated fat, polyunsaturated fat, alcohol, lipid lowering medications and BMI.
¶ Survey linear regression adjusted for age, sex, energy intake, education level, physical activity, current smoking status, intake of saturated fat, trans-fat, monounsaturated fat, polyunsaturated fat, alcohol, free sugars, lipid lowering medications and BMI.
** Survey linear regression adjusted for age, sex, energy intake, education level, physical activity, current smoking status, intake of free sugars and BMI.
†† Survey linear regression adjusted for age, sex, energy intake, education level, physical activity and current smoking status.
‡‡ Survey linear regression adjusted for age, sex, energy intake, education level, physical activity, current smoking status, intake of Na, K and BMI.
In the Swedish context, there were no significant differences across whole-grain food definition approaches in associations between categories of whole-grain intake and any health outcome measure of interest (all P ≥ 0·05, see online supplementary material, Supplemental Table S10). Interestingly, differences in associations were present when investigating whole-grain intake as grams (Table 5). A significant association was found with decreased BMI, WC and waist:height ratio in approaches where non-Keyhole foods were included, regardless of applying a whole-grain food definition (approach 1a/2a). Associations were lost in approaches where non-Keyhole foods were excluded, likely due to the low number of foods included. There were no significant changes in associations between whole-grain intake and body weight, waist:hip ratio or CRP in gram analyses when a whole-grain food definition was applied.
Table 5. Association between grams of energy-adjusted whole-grain intake and CVD risk factor measures for different whole-grain food definition approaches in Swedish adults
(Coefficient and standard errors)

* Significance is determined at P < 0·05.
† Survey linear regression adjusted for age, sex, energy intake, education level, physical activity at work, physical activity for leisure and current smoking status.
‡ Survey linear regression adjusted for age, sex, energy intake, education level, physical activity at work, physical activity for leisure, current smoking status, intake of saturated fat, monounsaturated fat, polyunsaturated fat, alcohol and BMI.
§ Coefficient, se and 95 % CI expressed as percentage increase/decrease (back-transformed from natural log).
Discussion
The use of a whole-grain food definition, namely the Healthgrain definition, has varying impacts within a research context. Specifically, it significantly impacted whole-grain intake estimations among two separate cohorts, where the degree of impact is related to both the food supply and local regulations on what constitutes a ‘healthy’ food. However, impacts on the associations between whole-grain intake and CVD risk factors were minimal. These impacts are important to consider as they may affect conclusions, recommendations and ultimately public health messages drawn from these studies. While estimations of intake show significant variation, it was difficult to show any consistent and relevant changes with the use of whole-grain food definitions. These definitions may be of greater relevance in public health promotion as, combined with regulated labelling, consumers would be encouraged to make choices which are higher in whole grain and healthier in general.
Whole-grain intakes of Swedish adults were much higher than Australian adults within the present study. However, utilising a whole-grain food definition significantly decreased whole-grain intake estimations in both the Australian, and even more so the Swedish cohort. Greater mean decreases of 20·0 g/10 MJ per d were observed in Swedish data compared with adults in Australian data with 7·8 g/10 MJ per d(Reference Kissock33). Interestingly, applying criteria only related to the percentage of whole grain in foods had little impact in the Swedish context with mean differences up to 2·7 g/10 MJ per d (comparison 2), while this difference was greater among Australian adults (up to 8·0 g/10 MJ per d, comparison 2)(Reference Kissock33). This indicates that typical Swedish foods contain ≥30 % whole grain and lower refined grain, while Australian whole-grain foods consumed in the survey contain smaller amounts of whole grain and/or larger amounts of refined grain. This highlights a difference in the food supply between the two countries and identifies a possibility for improvement in Australian whole-grain foods.
The whole-grain density of primary whole-grain intake products in Sweden (such as breakfast cereals, whole-grain bread and whole-grain crisp bread) is high(Reference Kyro, Skeie and Dragsted18). Eighty percentage of crisp bread products contains a high (≥75 %) whole-grain content, while 80 % of cereals consisted of muesli, porridge, oatmeal or other whole-grain breakfast cereals(Reference Johnsen, Frederiksen and Christensen49). For a food to be characterised and labelled as ‘whole grain’ in Sweden, at least 50 % of the DM must be whole-grain ingredients(Reference Asp and Bryngelsson50). On the other hand, breads and breakfast cereals are the major sources of whole grain among Australians(Reference Kissock33), where 70 % of breakfast cereals have at least 8 g whole grain per serve(Reference Curtain, Locke and Grafenauer51), while only 29 % of breads have at least 8 g whole grain per serve, with 27 % of high whole-grain density (≥24 g/serve)(Reference Grafenauer and Curtain52). These patterns may be partly explained by the lack of regulation regarding whole-grain content in Australia. While a definition of whole grain is regulated by Food Standards Australia New Zealand(53), there is no such regulation for whole-grain foods. Guidance exists as a voluntary code promoted by the Grains and Legumes Nutrition Council where standards for whole-grain content are much lower – only a minimum of 8 g whole grain per serve. With higher quantified recommendations and traditional diets that include whole grain, in conjunction with well-designed and successful promotion strategies like the Danish Whole Grain Partnership(Reference Mann54), it is no surprise that Nordic countries have higher whole-grain intakes(Reference Kyro, Skeie and Dragsted18). Swedish food manufacturers are incentivised to include >50 % whole grain to label the food as whole grain or meet a minimum whole-grain percentage between 30 and 100 % if they also wish to display the Keyhole symbol.
Patterns of whole-grain intake across approaches also differed between the two cohorts. Whole-grain intakes decreased across each subsequent whole-grain food definition approach for Australian data, whereas for Swedish data, a decreased intake was prominent in approaches where non-keyhole foods were excluded. There are two potential reasons for this: 1) Swedish whole-grain foods tend to contain larger whole-grain proportions in comparison with Australian whole-grain foods (limiting the relevance of excluding foods with <30 % whole grain) and 2) Swedish regulations to identify healthy foods through the Keyhole contain more restrictive criteria than discretionary classification in Australia. This is important as discretionary foods in Australia are differentiated from ‘core foods’ but the latter includes food items such as breads and cereals, even if they are primarily made of refined grain.
Other studies using restrictive whole-grain food definitions also observed lower whole-grain intakes. A UK study found that only considering foods containing ≥51 % whole grain compared with ≥10 % underestimated whole-grain intake by up to 27 %.(Reference Thane, Jones and Stephan55). Even a lower cut-off point of 25 % whole grain underestimated whole-grain intake by up to 10 %. Another UK study found that whole-grain intakes decreased when only considering foods with ≥51 % whole grain in comparison with absolute intakes, although intake when considering foods containing ≥10 % whole grain and absolute intake were similar(Reference Mann, Pearce and McKevith15). Likewise, utilising a ≥25 % and more so a ≥51 % whole-grain cut-off lowered whole-grain intake in comparison with absolute intake in a cohort of male health professionals(Reference Koh-Banerjee, Franz and Sampson56). This exemplifies that it is possible to consume substantial amounts of foods containing small whole-grain proportions, which contribute substantially to total whole-grain intake.
Unexpectedly, Swedish analyses showed higher whole-grain intakes in approach 2b than approach 1b. This is likely due to independently conducting MSM analysis for each approach and minimal exclusion of foods based on the first two criteria points of the Healthgrain definition. The MSM programme calculates usual whole-grain intakes based on regression analyses, such that it is possible that a minor increase in non-consumers could increase the whole-grain intakes of consumers.
The definitions used to estimate whole-grain intake will vary in affect between countries, due to varied food supplies and regulations to categorise ‘healthy foods’. Like Sweden, other Nordic countries such as Denmark are likely to have a large proportion of foods with higher whole grain in their food supply. This is typically a result of whole-grain labelling regulations and strong whole-grain promotion, in addition to variation in traditional food patterns(Reference Mejborn, Biltoft-Jensen and Trolle11,Reference Lourenço, Hansen and Frank57) . As such, definitions in these countries are unlikely to affect estimated intakes from a whole-grain proportion basis, but rather may be affected by the ability to meet ‘healthy food’ standards. However, in countries such as Australia, the USA and UK, there is greater consumption of refined grain foods, with whole-grain intake typically coming from foods with a low percentage whole-grain content. Here, estimated intakes are typically more affected by definitions specifying a high whole-grain percentage.
Although utilisation of a whole-grain food definition significantly underestimated whole-grain intakes, the impact when investigating associations with CVD risk markers was minimal. There were no substantial impacts on associations with anthropometric, blood pressure or biochemical measures in the Australian context, bar a few exceptions for fasting blood glucose and body weight. In Swedish analyses, there were no substantial impacts on associations with categories of whole-grain intake; however, some outcomes, namely BMI, WC and waist:height ratio, were significant for specific approaches in grams analyses. Here, significant associations were only found when whole grain was calculated from all foods (not just Keyhole compliant foods), rather than calculations where ‘whole-grain’ foods were included. This exemplifies the potential influence of whole-grain food definitions on health associations; however, the relevance of components other than the whole grain within excluded foods must also be considered. The interaction of components such as saturated fat, sugar, salt and refined grain on health measures with the presence of whole grain is unknown. Association analyses in the current study accounted for some of these components as confounding factors, and therefore, differences between approaches were potentially minimised. Additionally, accounting for various dietary and lifestyle factors reduced the possibility of residual confounding. It is important to note that impacts of whole-grain food definitions on health outcomes are not consistent across the two countries, such that one cannot infer that utilisation of these definitions affects specific outcomes, rather impacts must be considered within individual contexts.
Similar to the current study, Koh-Banerjee et al. (Reference Koh-Banerjee, Franz and Sampson56) found significant associations with 8-year weight gain among men regardless of the method or whole-grain food definition used to quantify whole-grain intakes. However, a stronger association was present when applying a ≥25 % whole-grain or bran content cut-off compared against a ≥51 % whole-grain cut-off or absolute whole-grain intakes. In analyses, some dietary and lifestyle factors were accounted for to reduce residual confounding. To note, this study is one of few published that compares different whole-grain food definitions on associations between whole-grain intake and outcomes.
Studies exploring associations between whole-grain intake and risk factors for CVD or the metabolic syndrome typically identify whole-grain foods using Jacobs et al. (Reference Jacobs, Meyer and Kushi58) definition whereby foods must contain ≥25 % whole-grain or bran content by weight, with inclusion or exclusion of listing specific foods. Similar to the current study, these studies were favourably associated with anthropometric measures(Reference McKeown, Meigs and Liu59–Reference Esmaillzadeh, Mirmiran and Azizi63,Reference Esmaillzadeh, Mirmiran and Azizi63) . Some studies showed no significant associations with total cholesterol, LDL-cholesterol, HDL-cholesterol, HbA1c or CRP(Reference Lutsey, Jacobs and Kori62–Reference Jensen, Koh-Banerjee and Franz64). In comparison, significant and favourable associations with whole-grain intake were found among other studies for total and LDL-cholesterol(Reference McKeown, Meigs and Liu59); total and HDL-cholesterol(Reference Jensen, Koh-Banerjee and Franz64); elevated blood pressure, high TAG and abnormal glucose homoeostasis(Reference Esmaillzadeh, Mirmiran and Azizi63); blood glucose(Reference Lutsey, Jacobs and Kori62) and CRP(Reference Qi, Van Dam and Liu65). Of note, both of these studies and those showing no associations adjusted for BMI within analyses and therefore reduced the risk of confounding. On the other hand, a recent systematic review investigated the impact of differing whole-grain food definitions on the associations with body weight measures in adults(Reference Kissock, Neale and Beck66). It was identified that great variation across studies existed namely in defining whole-grain foods and methods to estimate intake and that precise associations were therefore difficult to determine.
Use of the Keyhole to indicate nutritionally better or ‘healthy’ foods has great potential in public health promotion. Studies show that replacing non-keyhole foods with keyhole equivalents decreases total energy and fat intake, while intakes of fibre and whole grains increase(Reference Amcoff, Brugård Konde and Jansson67,Reference Biltoft-Jensen, Ygil and Kørup68) . The utilisation of whole-grain food definitions, with inclusion of a ‘healthy food’ criterion, in conjunction with strong regulation around identification and labelling of whole-grain foods, will help strengthen messaging around whole-grain intake and health and encourage consumers in making healthier and higher whole-grain food choices.
Within research, it is recommended that whole-grain intake be reported as absolute grams. Applying a definition is suggested to potentially weaken the association between whole grain and health as less whole grain is captured(Reference Ross, Kristensen and Seal27). Based on this study, application of a whole-grain food definition had large effects on intake estimates but did not significantly affect associations. However, only selected associations based on a snapshot of time were investigated. Associations of cross-sectional nature are less consistent, while greater information is captured in longitudinal studies. Furthermore, the inclusion or exclusion of deleterious components within ‘unhealthy’ whole-grain foods is unlikely to substantially affect associations, and therefore we suggest, should be included when estimating whole-grain intakes.
Similar limitations are present in analyses from both countries. First, analyses were based on cross-sectional data where only short term, intermediate disease outcomes are measured, rather than disease progression. Second, corresponding survey food databases may not reflect current food supplies. Shifts to increase whole-grain product availability to consumers in both contexts are recognised. Third, various assumptions were made to determine compliance of foods with the Healthgrain definition, specifically determining grain composition and compliance with the Keyhole. Assumptions regarding Keyhole compliance in the Swedish context were well informed by Swedish collaborators. Additionally, dietary intake collection methods in both surveys estimate intakes, which may not reflect true intake. Completion of four to eight repeat 24-h recalls is recommended to capture usual intake(Reference Holmes69,Reference Jackson, Byrne and Magarey70) , where Australian analyses used only one day of data. Swedish analyses were based on self-reported anthropometric measures and dietary intake, where participant reporting bias may be present, although intake was previously validated against doubly labelled water(Reference Nybacka, Bertéus Forslund and Wirfält38). Finally, the impact of the Healthgrain definition on associations was determined predominantly based on P-value changes. This is arguably a limitation as P-values are often misinterpreted. Using P-values alongside a cut-off rule (e.g. P < 0·05) for justifying scientific claims or conclusions and without considering contextual factors can lead to inaccurate beliefs and poor decision-making(Reference Wasserstein and Lazar71).
It is evident that utilisation of whole-grain food definitions, namely the Healthgrain definition, has varying impacts within research and across differing food supplies. Specifically, it has substantial impact when estimating whole-grain intakes, but less when exploring associations with CVD health outcomes. Variation among populations is related to a multitude of factors including the food supply, current promotion and local regulations to define ‘healthy’ foods. Overall, it is potentially relevant to consider whole-grain food definitions in research to gather a clear understanding of all intake. However, the identified differences in Australian and Swedish food supplies together with higher whole-grain intake and greater promotion of only high whole-grain foods (>50 %) in Sweden suggest that application of a whole-grain food definition will affect promotion and intake. Utilisation of these definitions may be more relevant to public health promotion and messaging to guide and encourage consumers in achieving higher whole-grain intakes.
Acknowledgements
The authors thank Marijka Batterham for her assistance with statistical analyses.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
The author’s contributions were as follows: K. R. K., E. W. L., E. P. N. and E. J. B. contributed to the study design; K. R. K., E. W. L., C. A., E. P. N. analysed the data; K. R. K., E. W. L., E. P. N. and E. J. B. interpreted the data; K. R. K. wrote the manuscript; E. W. L., C. A., E. P. N. and E. J. B. contributed to the manuscript preparation. K. R. K. had primary responsibility for final content. All authors have read and approved the final version of the manuscript.
The authors have no financial or personal conflicts of interest to declare.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114521000453