



Coronavirus disease 2019 (COVID-19) has created a mortality shock around the world, it may create a second wave of psychosocial problems tied to bereavement. Reference Morris, Moment and Thomas1 First reported in Wuhan, the capital city of Hubei, China, in December 2019, COVID-19 then spread across China. Reference Liu, Tan and Li2,Reference Shi, Wang and Cai3 Particularly, the death toll of the COVID-19 in Wuhan increased sharply from January to April in 2020. Reference Mizumoto and Chowell4,Reference Palacios Cruz, Santos and Velázquez Cervantes5 As of January 9, 2021, the death toll from COVID-19 in Chinese mainland was 4798, and in Wuhan, it was 3869. 6 Owing to the sudden infection and rapid deterioration of patients affected by the illness, many Chinese families were unprepared to accept the death of a family member. Reference Mayland, Harding and Preston7 When the COVID-19 patients passed away, many bereaved families encountered various mental and psychological problem, for instance depression, anxiety, and complicated grief. Reference Sun, Bao and Lu8 More seriously, some of those grieving the loss of family members due to COVID-19 engaged in self-harm or violence against other people. Reference Hao and Huang9 There were also reports of a series of conflicts between bereaved families and health-care workers in Wuhan. Reference Hao and Huang9
Grief counseling plays an important role in postdisaster psychological service. Reference Borins10,Reference Navidian, Saravani and Shakiba11 It is a service for those who have suffered a significant loss. Reference Breen, Croucamp and Rees12,Reference Gamino, Sewell and Hogan13 The target groups of grief counseling mainly included adults who have lost their husband or wife, pregnant women who have lost their fetuses, parents who have lost their children, and children who have lost their parents. Reference Aoun, Breen and Howting14 In general, health-care workers are the first to contact bereaved families, and the grief counseling they provide can relieve the mental and psychological problems of bereavement to a considerable degree. Reference Hsiao15 Grief counseling was first introduced in mainland China as a result of a great earthquake that occurred in Sichuan Province, China, in 2008. Reference Cui, Sim and Xu16 However, to date, grief counseling is still not included in the medical curriculum system in China. Reference Luo and Fu17 Therefore, many Chinese health-care workers have not received relevant systematic courses. Reference Yuan, Zhou and Tang18 When Chinese health care workers encounter the death of patients, they also feel sympathy, but they often are unaware of what measures can be taken to support bereaved families. Reference Dai, Xia and Ma19
To date, research on healthcare workers combating COVID-19 have mainly focused on mental health, manpower management, and infection prevention. Reference Chen, Zhang and Jahanshahi20–Reference Chidiebere, Tibaldi and Torre22 As far as we know, there is no research investigating health-care workers’ grief counseling service for bereaved families of COVID-19 victims in China. Thus, this research was conducted to fill this gap. It is hoped that our research will provide an opportunity to stimulate all-round development of grief counseling in China.
Methods
Study Design and Participants
We launched a cross-sectional survey using an electronic questionnaire. Taking into consideration data collection availability and quality, health-care workers from 7 hospitals in Wuhan were investigated by convenience sampling. The electronic questionnaires were distributed to the health-care workers’ cell phones through their medical service departments and nursing departments. Participants were informed that they needed to meet the inclusion criteria for research enrollment, which included: (1) nurses or doctors who had worked on the frontline against COVID-19 in Wuhan, (2) those who had received bereaved families of COVID-19 victims, and (3) those who voluntarily joined this research. All participants received information about the research aim and were informed that participation was voluntary, and results would be kept confidential. Informed consent was obtained before conducting each on-line survey. This study anonymously investigated the status of grief counseling among health-care workers, and did not involve human biomedical research. Therefore, this research was ruled exempt by the Institutional Review Board of Wuhan Polytechnic University. In total, 785 health-care workers completed our questionnaire from February 2020 to May 2020. In total, 61 questionnaires lacking indispensable information were excluded, and finally 724 questionnaires were collected.
Survey Questionnaire
The questionnaire contained 3 parts, and it took the health-care workers approximately 7 min to complete.
Sociodemographic Characteristics
Sociodemographic characteristics were gathered on gender (male, female), occupation (nurse, doctor), work experience (1-5 y; 6-10 y; 11-45 y), education background (bachelor, master, doctorate), marital status (unmarried, married), religion (religious, nonreligious), professional title (junior title, intermediate title, senior title/deputy senior title), frequency of contact with bereaved families (low, middle, high), training related to grief counseling (untrained, trained), and bereavement experience (without, with).
Skills of Grief Counseling Scale
Zhang established the skills of grief counseling scale (SGCS) in 2017. Reference Zhang23 The Cronbach’s α coefficient is 0.851, the content validity index is 0.871, and the reliability index is 0.834. Reference Dai, Xia and Ma19,Reference Zhang23 SGCS includes 2 parts: communication skills (3 items) and other grief counseling skills (5 items). All items were answered on a 4-point Likert scale ranging from 1 (totally disagree) to 4 (totally agree). Higher scores reveal increased competency in grief counseling for bereaved families.
Attitudes of Grief Counseling Scale
Zhang established the attitudes of grief counseling scale (AGCS) in 2017. Reference Zhang23 The Cronbach’s α coefficient is 0.935, the content validity index is 0.892, and the reliability index is 0.915. Reference Dai, Xia and Ma19,Reference Zhang23 AGCS includes 3 parts: sense of responsibility (3 items), willingness to receive relevant training (3 items), and enthusiasm for grief counseling (4 items). All items were answered on a 5-point Likert scale ranging from 1 (totally disagree) to 5 (totally agree). The higher the score, the more positive the health-care workers’ attitude toward bereaved families.
Statistical Methods
We used IBM SPSS Statistics 25.0 for statistical analysis. The data normal distribution was tested by Kolmogorov Smirnov analysis. After testing, SGCS and AGCS were both normally distributed. Multicollinearity was measured by the variance inflation factor (VIF). After testing, values of VIF were all lower than 10, so there is no multicollinearity. The comparison of different sociodemographic characteristics of health-care workers’ skills and attitudes toward grief counseling were analyzed by univariate analysis. The correlations between grief counseling skills and attitudes toward grief counseling were analyzed using Pearson correlation analysis. Multiple-factor analysis of skills of grief counseling and attitudes of grief counseling were, respectively, analyzed using multiple regression analysis. For all tests, values of P < 0.05 were considered statistically significant.
Results
Skills and Attitudes of Grief Counseling Among Health-Care Workers
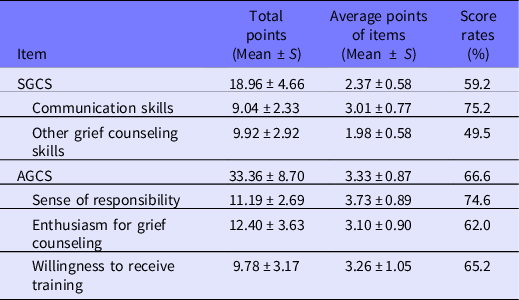
Table 1 showed health-care workers’ skills and attitudes of grief counseling toward bereaved families of COVID-19 victims in Wuhan. The average SGCS score was 18.96 ± 4.66, with a mean score rate of 59.2%. The maximum score of SGCS was 30, and the minimum was 9. The total point of AGCS was 33.36 ± 8.70, with a mean score rate of 66.6%. The maximum score of AGCS was 46, and the minimum was 15.
Table 1. Scores of skills and attitudes of grief counseling among health-care workers during the COVID-19 pandemic (n = 724)
Comparison of Different Sociodemographic Health-Care Workers’ Skills and Attitudes of Grief Counseling
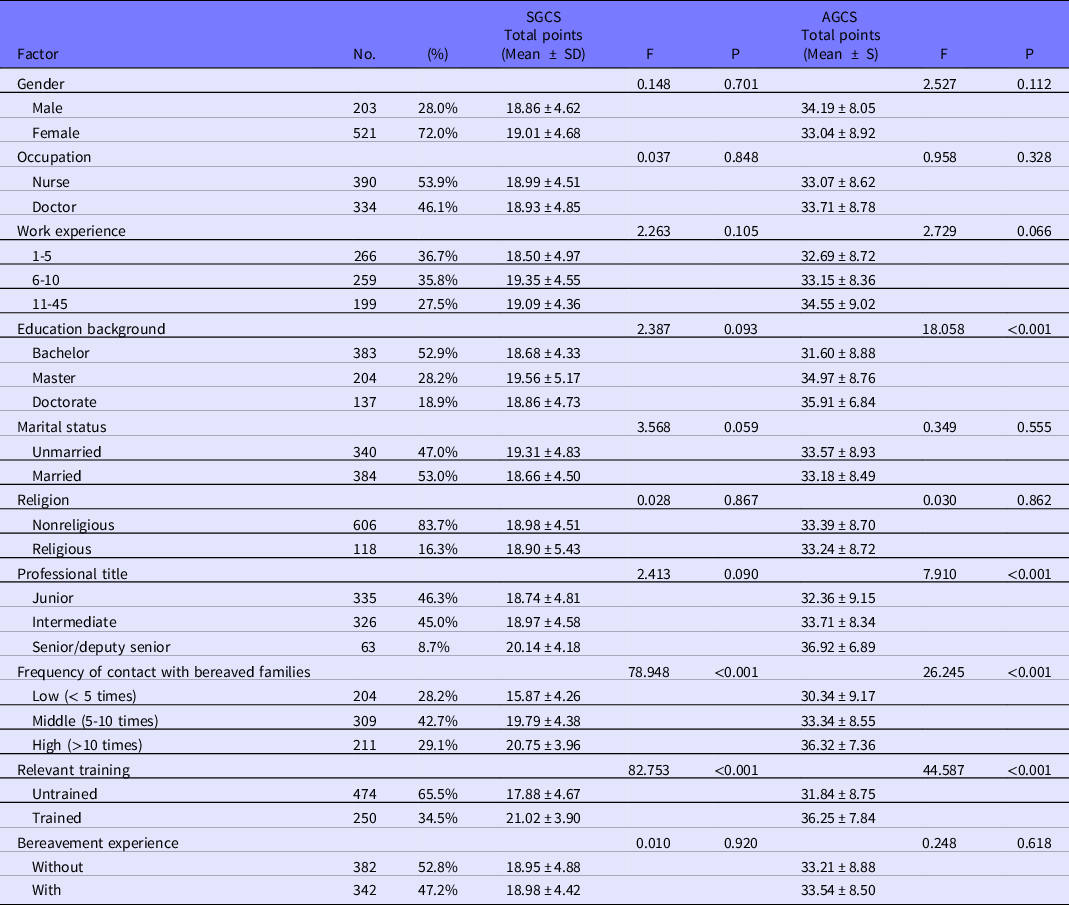
As indicated in Table 2, health care workers’ SGCS scores were significantly associated with frequency of contact with bereaved families and relevant training (P < 0.05). Health-care workers’ AGCS scores were significantly associated with education background, professional title, frequency of contact with bereaved families, and relevant training (P < 0.05).
Table 2. Comparison of different sociodemographic health-care workers’ skills and attitudes of grief counseling during the COVID-19 pandemic (n = 724)
Correlation Between Skills of Grief Counseling and Attitudes of Grief Counseling Among Health-Care Workers
The total SGCS score and its dimensions were positively correlated with AGCS and its dimensions as shown in Table 3 (P < 0.01). Better grief counseling skills of health-care workers corresponded with better attitudes.
Table 3. Relevance between skills of grief counseling and attitudes of grief counseling among health-care workers during the COVID-19 pandemic (n = 724)

Multiple-Factor Analysis of Skills of Grief Counseling Among Health-Care Workers
The main influence factors of skills of grief counseling consisted of sense of responsibility, frequency of contact with bereaved families, and training, as shown in Table 4. Therefore, the negative factors were lack of responsibility, low frequency of contact with bereaved families, and no relevant training.
Table 4. Multiple-factor analysis of skills of grief counseling among health-care workers during the COVID-19 pandemic (n = 724)

Annotation: R2 = 0.316, adjusted R2 = 0.313, F = 110.701, P < 0.05.
Multiple-Factor Analysis of Attitudes of Grief Counseling Among Health-Care Workers
The main influence factors of attitudes toward grief counseling consisted of other grief counseling skills, communication skills, education background, and training, as shown in Table 5. Therefore, the negative factors were lack of other grief counseling skills, lack of communication skills, low education levels, and no relevant training.
Table 5. Multiple-factor analysis of attitudes of grief counseling among health-care workers during the COVID-19 pandemic (n = 724)

Annotation: R2 = 0.259, adjusted R2 = 0.254, F = 62.677, P < 0.05.
Discussion
In any epidemic or pandemic, bereaved families are often ignored. At present, the COVID-19 pandemic in China has been basically controled, but the psychological trauma of bereaved families may linger for an extensive period of time. This is the first research to analyze health-care workers’ grief counseling toward bereaved families of COVID-19 victims in China.
Skills of Grief Counseling Among Health-Care Workers
The results of our survey showed that the average SGCS score among health-care workers was 18.96 ± 4.66, with a mean score rate of 59.2%. This indicated that health-care workers’ grief counseling skills need to be improved urgently. The following 2 reasons may explain this phenomenon. First, it is likely that a large number of Chinese health-care workers have not received systematic grief counseling training. Reference Gao, Kong and Fan24 Unlike some developed countries that have established a complete grief counseling system, grief counseling is still in its preliminary stage in China. Reference Zhou25 As mentioned before, grief counseling has not been included in the medical curriculum in China. Reference Luo and Fu17 Nevertheless, it is gratifying that more and more Chinese hospitals have realized the importance of grief counseling and have started providing relevant training for their health-care workers in recent years. Reference Cui, Li and Zhao26 Second, some of the health-care workers on the frontline of pandemic fight had limited experience of receiving bereaved families in their previous work, which also resulted in their poor grief counseling skills. During the COVID-19 outbreak period, health-care workers from almost all departments were mobilized to deal with issues of insufficient human resources in Wuhan. Reference An, Ye and Chen27,Reference Liu, Wang and Chen28 Generally speaking, health-care workers from the emergency department, intensive care unit, and oncology department are more likely to contact bereaved families. Hence, a large proportion of health-care workers lack sufficient experience in receiving bereaved families.
Attitudes of Grief Counseling Among Health-Care Workers
The average AGCS score among health-care workers was 33.36 ± 8.70, with a score rate of 66.6%, indicating that the attitude of grief counseling among health-care workers toward bereaved families of COVID-19 victims was not very positive. The following 3 reasons may account for this result. First, job burnout among health-care workers may have an impact on their attitudes toward grief counseling. An emergency hierarchical medical system was established in Wuhan during the first quarter of 2020. Reference Peng, Tu and Yang29 A total of 51 hospitals were transformed into COVID-19–designated hospitals by the Wuhan municipal government; these hospitals were responsible for treating patients with severe clinical symptoms. Reference Fang, Pan and Li30,Reference Li, Lu and Zhang31 As the pandemic progressed, tens of thousands of patients flooded into these COVID-19–designated hospitals, leading to severe shortages in hospital personnel. Reference Liu, Wang and Chen28 Many health-care workers in Wuhan had to continuously work overtime, resulting in different degrees of job burnout. Reference Mo, Deng and Zhang32,Reference Wu, Wang and Luo33 Previous research demonstrated that job burnout of health-care workers may cause compassion fatigue. Reference Zhang, Zhang and Han34 Thus, it is reasonable to infer that a huge workload may have weakened the compassion of health-care workers toward bereaved families to some degree. Second, it is possible that psychological issues among health-care workers affected their service attitudes. A vast number of health-care workers suffered from psychological issues, such as depression, fear, and anxiety in combating the COVID-19 pandemic. Reference Lai, Ma and Wang35,Reference Van Mol, Kompanje and Benoit36 While health-care workers struggled with severe acute respiratory syndrome, their psychological issues had a negative impact on their work attitude. Reference Maunder, Lancee and Balderson37 These health-care workers afflicted by various psychological problems engaged in a series of unprofessional behaviors and poor work performance, such as decreased punctuality, less contact with patients, and reduced working time. Reference Maunder, Lancee and Balderson37 Last, bereaved families’ behaviors will also affect the of health-care workers’ attitudes toward grief counseling. Among Chinese, death is regarded as a taboo topic whose mention is usually avoided in social interactions. When relatives pass away, Chinese either bear the grief alone or seek comfort from family members. Reference Zhang, Zou and Zhang38 Because bereaved families in China rarely seek help from health-care workers, health-care workers take for granted that they are not responsible for offering grief counseling service to the bereaved.
Factors Affecting Skills of Grief Counseling Among Health-Care Workers
Our research demonstrated that the potential influencing factors of grief counseling skills comprised of sense of responsibility, frequency of contact with bereaved families, and relevant training. To begin with, we found that possessing a strong sense of responsibility was closely related to health-care workers’ good grief counseling skills. It is likely that a responsible health-care worker will not only devote much attention to a patient’s condition but also show concern for bereaved families. Responsible health-care workers have accumulated abundant experience in the process of receiving bereaved families, which has continuously improved their skills. Next, we found that health-care workers with more experience receiving bereaved families in general are better equipped to offer grief counseling. This result was generally consistent with that of previous research. Reference Dai, Xia and Ma19,Reference Gao, Kong and Fan24 It is likely that, during frequent contacts with bereaved families, health-care workers not only realized the need for grief counseling but also grasped stronger communication skills. If grief counseling training is carried out in the future, it is recommended that trainers should specifically focus on health-care workers with less experience of receiving bereaved families. Last, health-care workers who have received relevant training have significantly better grief counseling skills. Relevant training included grief counseling, grief therapy, death education, and hospice care. Reference Zhang23 Luo and Fu’s research also proved that relevant training can help Chinese health-care workers quickly master the theory and practical skills of grief counseling. Reference Luo and Fu17
Factors Affecting Attitudes of Grief Counseling Among Health-Care Workers
Our research demonstrated that the potential influencing factors of attitudes of grief counseling are other grief counseling skills, communication skills, education background, and relevant training. First, we found that the stronger their skills of grief counseling health-care workers were, the more positive their attitudes would be. Other grief counseling skills included health education skills, grief risk assessment, psychological interventions, and self-emotional regulation. Reference Zhang23 This result was aligned with a previous research. Reference Dai, Xia and Ma19 It is likely due to the fact that health-care workers with excellent abilities in grief counseling often have rich practical experience in grief counseling emphasizing strong humanistic care. Therefore, they are more enthusiastic about getting involved in efforts related to bereaved families. Second, we found that health-care workers’ communication skills were closely related to their attitudes of grief counseling. Communication skills included counseling skills, empathy ability, listening ability, and expressive ability. Reference Zhang23 This is probably because health-care workers with good communication skills can often accurately and rapidly grasp the personality characteristics and psychological condition of bereaved families, and choose the corresponding communication strategy. Third, the higher the education level of health-care workers, the more positive their attitude toward the bereaved. In addition to receiving abundant training as part an advanced medical curriculum, highly educated health-care workers have a better comprehensive quality, which enables them to implement the concept of humanistic medicine in clinical work. Finally, this research showed that after receiving relevant training, health-care workers can clearly improve their attitude toward grief counseling. The relevant training included death education, life education, hospice care, grief counseling, and grief treatment. It is strongly recommended that relevant training or education should be offered to health-care workers as soon as possible.
To this end, the following suggestions are put forth. First, grief counseling is a complex systematic task involving multiple professionals, including health care workers, grief therapists, psychological counselors, psychiatrists, social workers, and family therapists. A hospital-community information system should be established so that health care workers can share the therapeutic process of the deceased with family therapists and social workers. In this way, social workers and family therapists can provide more targeted grief counseling to bereaved families. Second, a standardized training course should be established immediately in China. Because the threat posed by the pandemic remains, online public classes, webcast, and short videos are recommended for training. Health care workers with lower education levels and health care workers with less experience of receiving bereaved families should be paid more attention to in the training. Third, it is necessary to strengthen the promulgation of grief counseling in China. Workers in communities, schools, and hospitals can all be mobilized to publicize and popularize the concept of grief counseling to the public.
Limitations
Several limitations of this research should be considered. First, as a cross-sectional survey, this research could only assess the status of grief counseling at a specified time without follow-up observations of the health care workers. Second, due the limited number of hospitals that participated in this survey, our sample size might be too small to generalize the results. Thus, it is necessary to carry out a larger scale research in the future. Finally, as AGCS and SGCS are relatively new scales, so they may not have a history of much use. Considering the urgency of the COVID-19, time stresses did not allow us to test these scales fully ahead of use.
Conclusions
During the COVID-19 pandemic, over 2 million people have lost their lives worldwide. 6 While the primary focus of the public has been on COVID-19 patients, less attention has been paid to struggles of bereaved families. This study is the first research to focus on Chinese health care workers’ grief counseling for bereaved families of COVID-19 victims. The skills and attitudes toward grief counseling among health care workers combating COVID-19 were at a lower level in Wuhan, indicating the need to urgently improve grief counseling. The main influence factors of grief counseling skills consisted of sense of responsibility, frequency of contact with bereaved families, and relevant training, while the main influence factors of attitudes toward grief counseling consisted of other grief counseling skills, communication skills, education background, and relevant training. China should build a comprehensive grief counseling system, establish a standardized training course, and strengthen the popularization of grief counseling to the public.
Author contributions
Xudong Gao, Jing Wang, and Zhimin Wang conceived and designed the subject. Chan Kong, Hongru Fan, Jinyao Wang, and Jing Wang collected and analyzed data. All authors were involved in writing the study and had final approval of the submitted and published versions.
Funding statement
This work was supported by the COVID-19 prevention and control Project of University of South China (nk20200334); Special Project of COVID-19 Prevention and Control of Datong (No.4); Science and Technology Foundation of Hengyang (202010071555); Scientific Project of Wuhan Polytechnic University (2020Y25); Teaching Research Project of Wuhan Polytechnic University (XQ2019005); Talents Introduction Project of Wuhan Polytechnic University; Scientific and Technological Innovation Programs of Higher Education Institutions in Shanxi (2019L0762); Teaching Reform Research Project of Hubei province in 2020 (2020509); Science and Technology Project of Hubei Education Department (Q20201606).
Conflict of interest
The authors declare no conflict of interest.






 Open access
Open access