



Maternal depression (including depressive disorder and symptoms) is a major risk factor for children’s maladjustment and psychopathology (Goodman et al., Reference Goodman, Rouse, Connell, Broth, Hall and Heyward2011; Sutherland et al., Reference Sutherland, Nestor, Pine and Garber2021), particularly contributing to children’s internalizing problems (i.e., symptoms of depression and anxiety; Fanti & Henrich, Reference Fanti and Henrich2010). Yet, according to the multifinality principle of developmental psychopathology (Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996), not all children of depressed mothers develop internalizing problems. Previous research has demonstrated that the association between maternal depressive symptoms and children’s internalizing problems may be attenuated by individual-level factors (e.g., child gender, temperament; Goodman, Reference Goodman, Widiger and Cannon2020). Yet, resilience factors in the context of maternal depressive symptoms may also manifest on the dyadic level, since dyadic aspects of the mother–child relationship play a vital role in child development (Brumariu, Reference Brumariu2015; Ranson & Urichuk, Reference Ranson and Urichuk2008). Mother–child relationships (e.g., attachment, interaction quality) may not be uniformly undermined by maternal depressive symptoms (Galbally & Lewis, Reference Galbally and Lewis2017; Lovejoy et al., Reference Lovejoy, Graczyk, O’Hare and Neuman2000), such that mother–child dyads could retain good-quality relationships. Positive mother–child relationship processes, in turn, have been found to buffer the negative impact of maternal depressive symptoms on children’s internalizing problems (e.g., Milan et al., Reference Milan, Snow and Belay2009; Whittenburg et al., Reference Whittenburg, Stern, Brett, Straske and Cassidy2022).
One potential indicator of the mother–child dyadic relationship is physiological synchrony (Davis et al., Reference Davis, West, Bilms, Morelen and Suveg2018; Feldman, Reference Feldman2012), referring to the dynamic coordination of physiology between social partners during interpersonal interactions. Whereas prior research has shown that physiological synchrony may contribute to resilience for children by supporting mother–child bonding (Feldman, Reference Feldman2012) and children’s emotion regulation (Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018), less is known about the role of physiological synchrony on infant and toddler adjustment in the context of maternal depressive symptoms. Physiological synchrony may operate as a moderator of risk transmission since it could potentially facilitate infant emotion regulation, which could attenuate the development of internalizing symptoms and buffer the negative impact of maternal depressive symptoms (Davis et al., Reference Davis, Suveg, Whitehead, Jones and Shaffer2016; Silk et al., Reference Silk, Shaw, Forbes, Lane and Kovacs2006). Thus, the present study sought to build on previous work by illuminating the potential moderating role of mother–infant physiological synchrony in the intergenerational transmission of internalizing symptoms, specifically with respect to the parasympathetic nervous system given its role in supporting interpersonal emotion regulation processes (Porges, Reference Porges2007). We examined whether and how maternal postnatal depressive symptoms and mother–infant RSA synchrony during free play at 6 months interacted to predict children’s internalizing problems at 24 months.
Maternal depressive symptoms and children’s internalizing problems
Maternal depressive symptoms are associated with children’s internalizing problems and have long-lasting effects on children’s well-being (Goodman, Reference Goodman, Widiger and Cannon2020). For instance, meta-analyses indicated that greater maternal depressive symptoms were related to children’s greater internalizing problems (Goodman et al., Reference Goodman, Rouse, Connell, Broth, Hall and Heyward2011), poorer socioemotional development (Rogers et al., Reference Rogers, Obst, Teague, Rossen, Spry, Macdonald, Sunderland, Olsson, Youssef and Hutchinson2020), and lower cognitive and behavioral functioning (Sutherland et al., Reference Sutherland, Nestor, Pine and Garber2021). Nevertheless, the effects of maternal depressive symptoms on child adjustment are not always consistent and prior research has sometimes yielded null findings for such associations (e.g., Davis et al., Reference Davis, Suveg, Whitehead, Jones and Shaffer2016). Potential resilience factors that may mitigate the intergenerational transmission of internalizing symptoms include but are not limited to, child and parent characteristics (Goodman, Reference Goodman, Widiger and Cannon2020). For example, maternal depressive symptoms were not related to children’s internalizing problems when children had higher emotion regulation (Silk et al., Reference Silk, Shaw, Forbes, Lane and Kovacs2006) or physiological regulation levels (Davis et al., Reference Davis, Suveg, Whitehead, Jones and Shaffer2016). In another study, the association between maternal depressive symptoms and infant distress was buffered by father involvement (Lewin et al., Reference Lewin, Mitchell, Waters, Hodgkinson, Southammakosane and Gilmore2015). Despite these contributions, previous studies have mostly focused on individual-level moderators with limited attention to dyadic mother–child processes. Dyadic-level moderators should be considered, as they reflect the unique characteristics of dyads formed through the combination of mother and child input and play a major role in the development of children’s emotion regulation (Brumariu, Reference Brumariu2015) and socioemotional functioning (Ranson & Urichuk, Reference Ranson and Urichuk2008).
Dyadic physiological synchrony as a moderator
Researchers have documented the potential benefits of positive mother–child relationship quality for depressed mothers (Leckman-Westin et al., Reference Leckman-Westin, Cohen and Stueve2009), including the protective role of various dyadic relationship indicators (e.g., attachment security, Milan et al., Reference Milan, Snow and Belay2009; interaction quality, West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020) on the associations between maternal depressive symptoms and children’s internalizing problems. For example, the positive prediction of children’s internalizing problems from maternal depressive symptoms is weakened (Whittenburg et al., Reference Whittenburg, Stern, Brett, Straske and Cassidy2022) or nonsignificant (Milan et al., Reference Milan, Snow and Belay2009) under conditions of higher mother–child attachment security. Additionally, positive mother–child interaction characteristics (e.g., positive affective climate, mutual engagement, and responsivity) buffer the effects of maternal depressive symptoms on children’s internalizing problems (Endendijk et al., Reference Endendijk, De Bruijn, Van Bakel, Wijnen, Pop and Van Baar2017; Goodlett et al., Reference Goodlett, Trentacosta, McLear, Crespo, Wheeler, Williams, Chaudhry and Smith-Darden2017; Leckman-Westin et al., Reference Leckman-Westin, Cohen and Stueve2009; West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020). Taken together, this line of research indicates that positive mother–child relationship characteristics may operate as a resilience factor for children in the context of maternal depressive symptoms.
The mother–child relationship is a multilevel process (Calkins et al., Reference Calkins, Propper and Mills-Koonce2013; Feldman, Reference Feldman2012) that involves mothers’ and children’s continuous responses and modulation of each other’s emotional, behavioral, and physiological signals during face-to-face interaction (Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018). Physiological synchrony refers to the temporal coordination of mothers’ and children’s physiological activity during an interaction. According to biobehavioral synchrony theory (Feldman, Reference Feldman2012), mother–child physiological synchrony is formed through repeated dyadic interactions, in which mother and child coordinate their physiological response with the partner’s physiological state. Physiological synchrony has been found in multiple physiological systems (e.g., heart rate, cortisol, RSA; Birk et al., Reference Birk, Stewart and Olino2022; Davis et al., Reference Davis, West, Bilms, Morelen and Suveg2018; DePasquale, Reference DePasquale2020). Importantly, physiological synchrony is theorized to provide the biological foundation for mother–child attachment and facilitate children’s regulatory development (Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018).
We focused on the mother–child synchrony of RSA within the parasympathetic nervous system given that RSA synchrony has strong burgeoning empirical evidence and that RSA is a noninvasive biomarker of emotion regulation (Beauchaine, Reference Beauchaine2015). Specifically, the growing empirical literature has shown that RSA synchrony is present during early mother–child interaction, it is a potential mechanism for the development of children’s self-regulation, and it is related to child psychopathology (see review, DePasquale, Reference DePasquale2020; Miller et al., Reference Miller, Armstrong-Carter, Balter and Lorah2023). RSA refers to the high-frequency component of heart rate variability, indexing parasympathetic control of the heart through the myelinated vagus nerve (Porges, Reference Porges2007). Vagal control (indicated by RSA), acting as a brake on cardiovascular activity, helps individuals maintain homeostasis at rest, whereas the withdrawal of vagal control (i.e., lower RSA) allows for the mobilization of physiological resources for coping with challenges (Porges, Reference Porges2007). Thus, individual RSA activity reflects how one responds and regulates themselves to emotionally related challenges (Beauchaine, Reference Beauchaine2015).
RSA synchrony is often operationalized as the degree of covariation between mother and child RSA around their own mean levels (Helm et al., Reference Helm, Miller, Kahle, Troxel and Hastings2018), thus reflecting how dyads dynamically co-regulate each other’s emotion-related physiology (Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018). Prior research has documented significant concordant mother–child RSA synchrony during interactions in infancy and early childhood (e.g., Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Buss, Lucas-Thompson, Boker and Timpe2015; Waters et al., Reference Waters, West, Karnilowicz and Mendes2017). Although the interpretation of RSA synchrony has not yet reached a consensus and the adaptiveness of RSA synchrony partly depends on context (e.g., the emotional context of the interaction and specific risk characteristics; Birk et al., Reference Birk, Stewart and Olino2022; Fuchs et al., Reference Fuchs, Lunkenheimer and Lobo2021; Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021), prior work conceptualizes RSA synchrony as a process that generally supports dyadic interaction and facilitates children’s self-regulation (Davis et al., Reference Davis, West, Bilms, Morelen and Suveg2018; DePasquale, Reference DePasquale2020; Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018).
Mother–child RSA synchrony may operate as a moderating factor for the association between maternal depressive symptoms and children’s internalizing problems for two reasons. First, the theory has stipulated that physiological synchrony provides the foundation for higher mother–child relationship quality and attachment (Feldman, Reference Feldman2012). Empirical evidence has linked higher RSA synchrony (in contrast with absent or lower synchrony) with higher interaction quality and lower negative interaction overall (McKillop & Connell, Reference McKillop and Connell2018; Wang et al., Reference Wang, Suveg, West, Han, Zhang, Hu and Yi2021; Waters et al., Reference Waters, West, Karnilowicz and Mendes2017; Woody et al., Reference Woody, Feurer, Sosoo, Hastings and Gibb2016), as well as more sensitive and less negative parenting behaviors (e.g., higher engagement, less maltreatment; Brown et al., Reference Brown, Lunkenheimer, LeBourgeois and Heilman2021; Lunkenheimer et al., Reference Lunkenheimer, Busuito, Brown and Skowron2018; Skoranski et al., Reference Skoranski, Lunkenheimer and Lucas-Thompson2017). Thus, RSA synchrony may provide the biological basis for positive emotions and behaviors in mother–child interactions that could attenuate the transmission of risks (Leckman-Westin et al., Reference Leckman-Westin, Cohen and Stueve2009; Milan et al., Reference Milan, Snow and Belay2009; Whittenburg et al., Reference Whittenburg, Stern, Brett, Straske and Cassidy2022). Second, as highlighted by theory and prior literature, RSA synchrony may promote children’s regulation of physiological arousal that ultimately contributes to socioemotional adjustment (Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018). As such, higher RSA synchrony may mitigate the intergenerational transmission of risks by reducing children’s psychopathology symptoms. For instance, higher mother–child RSA synchrony has shown associations with greater infant distress regulation (Abney et al., Reference Abney, daSilva and Bertenthal2021), fewer child internalizing problems (Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018; Suveg et al., Reference Suveg, West, Davis, Caughy, Smith and Oshri2019; Wang et al., Reference Wang, Suveg, West, Han, Zhang, Hu and Yi2021), and lower risk of developing anxiety disorders for children after trauma (gray et al., Reference Gray, Lipschutz and Scheeringa2018).
To our knowledge, few studies have directly examined the moderating role of mother–child RSA synchrony on the associations between contextual risks and child outcomes. Only two studies from the same project on high-risk families have taken this endeavor (Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021; West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020), and one of them focused on maternal depressive symptoms. In this cross-sectional study, West et al. (Reference West, Oshri, Mitaro, Caughy and Suveg2020) measured mother–youth RSA synchrony (age: 9–12 years) during a dyadic conflict discussion task. They found that higher levels of maternal depressive symptoms were associated with youths’ greater behavioral problems; surprisingly, this link was further exacerbated by higher mother–youth RSA synchrony, although the direct effect of RSA synchrony on behavioral problems was non-significant. One potential explanation for this result is developmental differences such that higher mother–child RSA synchrony operates as a protective factor for young children (e.g., Abney et al., Reference Abney, daSilva and Bertenthal2021) but seems to hinder individual adjustment in later childhood. Another explanation is that higher RSA synchrony within a stressful conflict discussion task may indicate a shared dysregulated stress response (Oshri et al., Reference Oshri, Liu, Huffman and Koss2021) rather than coordinated supportive coregulation during low-stress interaction task (e.g., Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018; Wang et al., Reference Wang, Suveg, West, Han, Zhang, Hu and Yi2021). Given the scarce evidence so far and potential heterogeneity in findings across different developmental stages or task contexts (e.g., high- vs low-stress contexts) (Birk et al., Reference Birk, Stewart and Olino2022; Davis et al., Reference Davis, West, Bilms, Morelen and Suveg2018), more research is warranted in examining this issue.
The present study
This study aimed to examine the moderating effect of mother–infant RSA synchrony on the association between maternal depressive symptoms and children’s internalizing problems. We adopted a two-wave design in a community sample to investigate whether and how maternal postnatal depressive symptoms interacted with mother–infant RSA synchrony during free play at 6 months in predicting children’s internalizing problems at 24 months. Specifically, we tested concurrent synchrony of RSA (the covariation of mother and infant RSA fluctuation around their own mean level at each time point; Helm et al., Reference Helm, Miller, Kahle, Troxel and Hastings2018), since this form of synchrony was commonly captured in parasympathetic system activity compared to the less-examined lagged synchrony (prediction from one time-point to next) (DePasquale, Reference DePasquale2020; Miller et al., Reference Miller, Armstrong-Carter, Balter and Lorah2023). We chose 6 months as the first time point since it is a critical time for infant socio-emotional development, especially within mother–infant interaction processes (Moore et al., Reference Moore, Hill-Soderlund, Propper, Calkins, Mills-Koonce and Cox2009; Thomas et al., Reference Thomas, Letourneau, Campbell, Tomfohr-Madsen and Giesbrecht2017). We measured mother and infant RSA during free play given that the synchronous RSA activity during this low-stress context may reflect coordinated mother–infant interaction, which may promote the formation of attachment and contribute to the development of children’s emotion regulation (Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018). Infant negative affect at 6 months was included as a covariate to account for individual differences in baseline negative affectivity given that it was an earlier proxy for children’s internalizing problems (Eisenberg et al., Reference Eisenberg, Cumberland, Spinrad, Fabes, Shepard, Reiser, Murphy, Losoya and Guthrie2001).
Drawing on the literature of RSA synchrony (DePasquale, Reference DePasquale2020; Miller et al., Reference Miller, Armstrong-Carter, Balter and Lorah2023), we hypothesized that within the current community sample, there would be significant and positive mother–infant concurrent RSA synchrony on average during free play and significant between-dyad variation in levels of RSA synchrony. Specifically, on average, fluctuations in mother RSA would positively predict fluctuations in infant RSA at the same moment and vice versa (i.e., concurrent positive RSA synchrony). In addition, RSA synchrony across dyads might range from low levels (negative or non-significant synchrony) to high levels (positive synchrony), with higher RSA synchrony indicating stronger positive coordination in mother-infant RSA fluctuations.
Regarding our primary research question, we had three hypotheses. First, we hypothesized that greater maternal depressive symptoms at 6 months would be associated with children’s higher internalizing problems at 24 months. Second, we hypothesized that higher mother–infant RSA synchrony during free play might be associated with fewer child internalizing problems at 24 months. Third, we hypothesized that higher mother–infant RSA synchrony would attenuate the association between maternal depressive symptoms and children’s internalizing problems. We considered the main-effect hypothesis of RSA synchrony preliminary for two considerations. First, prior findings on the main effect of synchrony have been limited in infancy and the evidence regarding the direct effect of synchrony has been inconsistent in childhood (e.g., Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018; West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020). Second, early mother–infant coregulation patterns (e.g., synchrony) might not yet be well-ingrained enough (Cohn & Tronick, Reference Cohn and Tronick1987) to directly shape child psychopathology symptoms during infancy.
This study, to our knowledge, is the first to examine the role of dyadic-level physiological synchrony in the intergenerational transmission of depressive and internalizing symptoms by a longitudinal design, which may have critical clinical implications for prevention and intervention.
Method
Participants
Mother–infant dyads (N = 166) participating in our two-wave longitudinal study were recruited from a rural area in China through birth registration in local health centers. This was a convenience sample in local communities and participants with major health disorders such as heart disease were excluded. At Time 1, infants were 6 months old on average (80 girls; M age = 6.61, SD age = 0.86) and mothers were 29 years old on average (M = 28.85, SD = 4.70, Range: 23–43). Roughly half (53%) of mothers did not finish high school, 23% had a high school diploma, and the rest had college or university degrees. Annual household income ranged from ¥10,000 to ¥200,000 (Average = ¥43,480), with 47% below ¥40,000 and 39% ranging from ¥40,000 to ¥70,000. Overall, this sample was a rural, low-to-middle SES class in China. Most mothers were married (90.3%) and most families were of the same ethnic group (99% Ethnic Han). At Time 2, 115 dyads attended the follow-up visit, with 31% of dyads dropping out who indicated that they had no interest or time for a follow-up visit or that they had moved to other places. Children were 24 months old on average (55 girls; M age = 23.62, SD = 0.67) at Time 2. Attrition analysis indicated that there were no significant differences between dyads who dropped out and dyads who completed the second visit on primary study variables (i.e., maternal depressive symptoms, infant negative affect, estimated factor scores of mother–infant RSA synchrony) and demographics (age, gender, maternal education, and household income), ps > .05.
Procedure
This study was approved by the Institutional Review Board of School of Psychological and Cognitive Sciences at Peking University. Informed consent was obtained from mothers on both measurement occasions. At 6 months, mothers brought their infants to the local health centers for assessments including observational tasks and survey measures. Mother–infant dyads completed a 3-minute videotaped free-play task while wearing ambulatory physiological devices to record ECG signals. During this task, mothers and infants were seated facing each other, and mothers were instructed to play with infants as they normally would at home. After the observation task, mothers filled in questionnaires that measured their demographics and depressive symptoms. At 24 months, families were invited back for follow-up visits in the same setting, during which mothers reported the toddler’s internalizing problems.
Measures
Maternal postnatal depressive symptoms (6 months)
Mothers completed the 10-item Edinburgh Postnatal Depression Scale (EPDS; Cox et al., Reference Cox, Holden and Sagovsky1987) during the first visit. EPDS is widely used to capture maternal depressive symptoms within one year postpartum and has been validated in China (Wang et al., Reference Wang, Guo, Lau, Chan, Yin and Chen2009). Mothers rated how they had felt in the past seven days (e.g., “I have felt sad or miserable”) on a 4-point Likert scale from 0 (never) to 3 (most of the time). The sum score of all items, with appropriate reverse scoring, was created to indicate maternal postnatal depressive symptoms (Cronbach α = .76). In our sample, 15% of mothers had symptom scores above 13, indicating a risk for clinical depression. This percentage is comparable to previous community samples (e.g., Netsi et al., Reference Netsi, Pearson, Murray, Cooper, Craske and Stein2018).
Infant negative affect (6 months)
Infant negative affect during free play was observed to measure individual differences in negative affectivity (Haltigan et al., Reference Haltigan, Leerkes, Supple and Calkins2014; Pratt et al., Reference Pratt, Singer, Kanat-Maymon and Feldman2015). Infant affect during free play was observed and coded second by second using the adapted AFFEX system (Izard, Reference Izard1980) in the software Observer XT 12 (Noldus Information Technology) by trained research assistants. AFFEX system is a widely used valid tool to micro-code infant affect (including a variety of positive affect and negative affect, e.g., joy, interest, sadness, and distress) by holistic judgments. Specifically, infant negative affect captures sadness and distress from facial expressions (e.g., crying face) and vocalizations (e.g., fussy vocalizations) in our interaction task. In the Observer software, infant affect was continuously rated on a nominal scale of different affect categories (e.g., joy, neutral, sadness). Within each affect category, coders marked the onset and the endpoint of each affect in real time. By this method, we could derive the total duration for each affect. The negative affect score was operationalized as the percentage of time that sadness or distress was expressed out of the total duration of the free play task, with a higher score indicating greater negative affect. On average, infants displayed low levels of negative affect during the 3-minute free play (Mean proportion of display = 8.97%, duration = 16.15 seconds, Range = 0-98%). We adopted typical measures of reliability for affect micro-coding (e.g., Hallgren, Reference Hallgren2012; Lougheed et al., Reference Lougheed, Brinberg, Ram and Hollenstein2020; Somers et al., Reference Somers, Luecken, McNeish, Lemery-Chalfant and Spinrad2021). Using twenty percent randomly sampled videos for double coding, we reached good reliability between a master graduate coder and an undergraduate research assistant (average duration-sequence-based percent agreement was 82.25%, average Cohen’s kappa = .74).
Maternal and infant RSA (6 months)
Mother and infant ECG signals were continuously collected during the 3-minute free-play task by ambulatory physiology-recording devices connected to the data acquisition software Acknowledge 4.4 (Biopac Systems Inc.) with cardiac electrodes worn on the body. Interbeat intervals (IBI) captured from ECG signals were visually displayed and manually cleaned for artifacts (e.g., misidentification of R peaks) in CardioEdit software (Brain-Body Center, 2007) by trained research assistants. Cleaned IBI data was used to calculate RSA (interbeat interval variability within the spontaneous respiration frequency band) in 15-s epochs in CardiobatchPlus software (Brain-Body Center), using Porges’s method (Porges, Reference Porges1985). The epoch length of 15 seconds was chosen because it has been shown to be valid for estimating RSA (Bar-Haim et al., Reference Bar-Haim, Marshall and Fox2000) and was often used in infant and child studies, especially for short tasks (e.g., Moore et al., Reference Moore, Hill-Soderlund, Propper, Calkins, Mills-Koonce and Cox2009). The spontaneous respiration frequency band for calculating RSA was 0.24–1.04 Hz for infants, and 0.12–0.40 Hz for mothers (Fracasso et al., Reference Fracasso, Porges, Lamb and Rosenberg1994). Thus, in the 3-minute free play task, mothers and infants each had 12 epochs of RSA data. If IBI data was missing or unusable in one epoch, RSA for this epoch was set as missing. Descriptive statistics for the epoch-by-epoch RSA data are available in the supplementary material (Table S1).
Children’s internalizing problems (24 months)
Mothers reported children’s internalizing problems using the age-appropriate Child Behavior Checklist (CBCL; Achenbach & Rescorla, Reference Achenbach and Rescorla2000; “looks unhappy for no reason”). Mothers rated children’s behavior on a 3-point Likert scale from 0 (not true) to 2 (very or often true). To relieve mothers’ burden on reporting, we only assessed items for the internalizing subscales of the CBCL. Internalizing problem scores were calculated as the sum of raw scores of emotionally reactive, anxious/depressed, and withdrawn subscales (Storch et al., Reference Storch, Merlo, Keeley, Grabill, Milsom, Geffken, Ricketts, Murphy and Goodman2008), showing high reliability (25 items, Cronbach α = .91).
Demographic information
At 6 months, mothers reported infant age in months, infant gender, maternal age and educational attainment, and household income. Mothers also reported infant weight and height to calculate body mass index (BMI), which relates to child functioning in RSA change (Hinnant & El-Sheikh, Reference Hinnant and El-Sheikh2009).
Data analysis plan
Missing data and attrition
At 6 months, among 166 dyads, 41 dyads (24.70%) had incomplete RSA data that was partially missing for all epochs due to signal noises caused by movement or technological problems. Missing rates for epoch-by-epoch RSA ranged from 0.6% to 7.2%, see Table S1 in supplementary material. Dyads with complete RSA data and dyads with partially missing RSA data were not significantly different in demographics, maternal depressive symptoms, or infant negative affect, ps > .05. At 24 months, children’s internalizing problem scores were partially missing due to dropout (missing rate = 31%). Little’s MCAR test showed that our data were missing completely at random (χ (73)2 = 75.88, p = .39). In the following analyses, we adopted the full information maximum likelihood (FIML) method in model estimation, which could obtain unbiased parameter estimates while retaining the full sample size (Graham, Reference Graham2009).
Examining the moderating effects of RSA synchrony
To calculate within-dyad concurrent RSA synchrony and further examine the moderating role of RSA synchrony on the association between maternal depressive symptoms and children’s internalizing problems, multilevel structural equation models (Preacher et al., Reference Preacher, Zhang and Zyphur2016) were conducted in Mplus 8.3 (Muthén & Muthén, Reference Muthén and Muthén2017). The multilevel SEM model was an effective tool to account for the nested nature of our data (i.e., repeated assessment of RSA nested within-person/dyad) while allowing us to treat random slopes or intercepts as latent outcomes, predictors, or moderators within one model (Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021; Preacher et al., Reference Preacher, Zhang and Zyphur2016). Baseline models with random intercepts of RSA were conducted to examine the within-person dependency in RSA and the necessity for multilevel models. Results showed that intraclass correlation (ICC, proportion of between-person variance out of the total between- and within-person variances) was 0.58 for infant RSA and 0.57 for mother RSA. These ICC values indicated that 58% (42%) and 57% (43%) variance of infant RSA and mother RSA, respectively, were explained by between-person variation (within-person variation). This result supported the utilization of multilevel models to explore the significant proportion of between-person differences while accounting for the within-person dependency in the data (Musca et al., Reference Musca, Kamiejski, Nugier, Méot, Er-rafiy and Brauer2011).
Thus, a multilevel latent moderation analysis (Preacher et al., Reference Preacher, Zhang and Zyphur2016) was adopted to test whether within-dyad concurrent RSA synchrony, a random slope across different dyads, acted as a latent predictor and moderated the relation between observed variables at the between-dyad level. We adopted a similar approach to the prior literature (e.g., Li et al., Reference Li, Sturge-Apple, Liu and Davies2020; Suveg et al., Reference Suveg, West, Davis, Caughy, Smith and Oshri2019) and operationalized concurrent RSA synchrony as within-dyad predictive associations in concurrent mother and child fluctuations around their own mean RSA at each time point. To appropriately differentiate within-dyad vs. between-dyad effects, we performed person-mean centering for mother and child concurrent RSA. Furthermore, two sets of models were conducted with mother and child RSA as the dependent variable, respectively, and only the details of the child model building (i.e., mother RSA predicting → infant RSA) are reported here given the similarity in the model construction.
As the following equation shows, on the first level (within-dyads level) of the model, infant RSA at time t in dyad j was the function of (a) the infant RSA intercept, (b) the concurrent association with their mothers’ person-mean-centered RSA at time t (i.e., RSA synchrony of the jth dyad), (c) the effect of epoch time, and (d) the within-dyad residual error term. Note that we included the time effect here (first epoch denoted as zero, time unit: 15 seconds/epoch) to control for the systematic trend of RSA and estimate concurrent RSA synchrony more rigorously (i.e., capturing dyadic covariation of RSA fluctuations moment by moment after accounting for the overall time trend, Helm et al., Reference Helm, Miller, Kahle, Troxel and Hastings2018). Given that time was set as zero at the first epoch, infant RSA intercepts thus represented the model-estimated mean RSA at the beginning (i.e., first epoch) of the interaction task when other predictors in the model were at zero (e.g., Mother_RSA jt ). On level two, we allowed for random intercepts (i.e., individual mean RSA) and random slopes (i.e., synchrony and time effect) across dyads, such that families could differ in these effects within the sample. Given the specification of this model already allowed for the differentiation of within-person effect (i.e., within-dyad RSA synchrony) vs. context effect (i.e., similarity in mother–infant mean RSA) (Bell et al., Reference Bell, Jones and Fairbrother2018; Bell and Jone, Reference Bell and Jones2015), the former of which was what we were interested in, we did not include the person-mean term of Mother_RSA in the model to estimate the context effect (i.e., how mothers’ mean RSA level over the whole task was associated with infants’ mean RSA level over the whole task).
The equation for RSA synchrony estimation and multilevel interaction analysis
Level 1:
Infant_RSA jt = β0j + β1j (Mother_RSA jt ) (person-mean-centered) + β2j Time t + r jt
Level 2:
β0j = γ00 + μ0j
β1j = γ10 + μ1j
β2j = γ20 + μ2j
Child internalizing problems j = γ30 + γ31 μ1j + γ32 MDS j + γ33 μ1j *MDS j + γ34 Age j + γ35 Gender j + γ36 BMI j + γ37 Negative_Affect j + μ3j . (MDS, maternal depressive symptoms).
Furthermore, on the second level (between-dyad level), structural equation models with (a) main effects only and (b) with interaction effect included were separately constructed to test both the unadjusted main effects of maternal depressive symptoms and mother–infant RSA synchrony and their latent interaction effect on children’s internalizing problems (see Fig. 1 and the Equation for multilevel interaction analysis), in line with prior multilevel SEM applications (e.g., Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021; Preacher et al., Reference Preacher, Zhang and Zyphur2016). RSA synchrony was a latent variable derived from level one, measuring each dyad’s deviation from the grand-mean level of synchrony. Covariates were controlled in the models, including infant age, gender, BMI, and negative affect. All continuous predictors on level two (e.g., infant age and maternal depressive symptoms) were grand-mean centered to minimize multicollinearity between variables (Aiken and West, Reference Aiken and West1991). When a significant interaction emerged, we probed the pattern of the interaction via simple slope tests at high (+1SD), mean, and low (−1SD) levels of RSA synchrony. In addition, we performed region of significance (RoS) on Z analysis using Preacher’s online tools (Preacher et al., Reference Preacher, Curran and Bauer2006), which reveals the range of RSA synchrony for which the association between maternal depressive symptoms and children’s internalizing problems is significant.
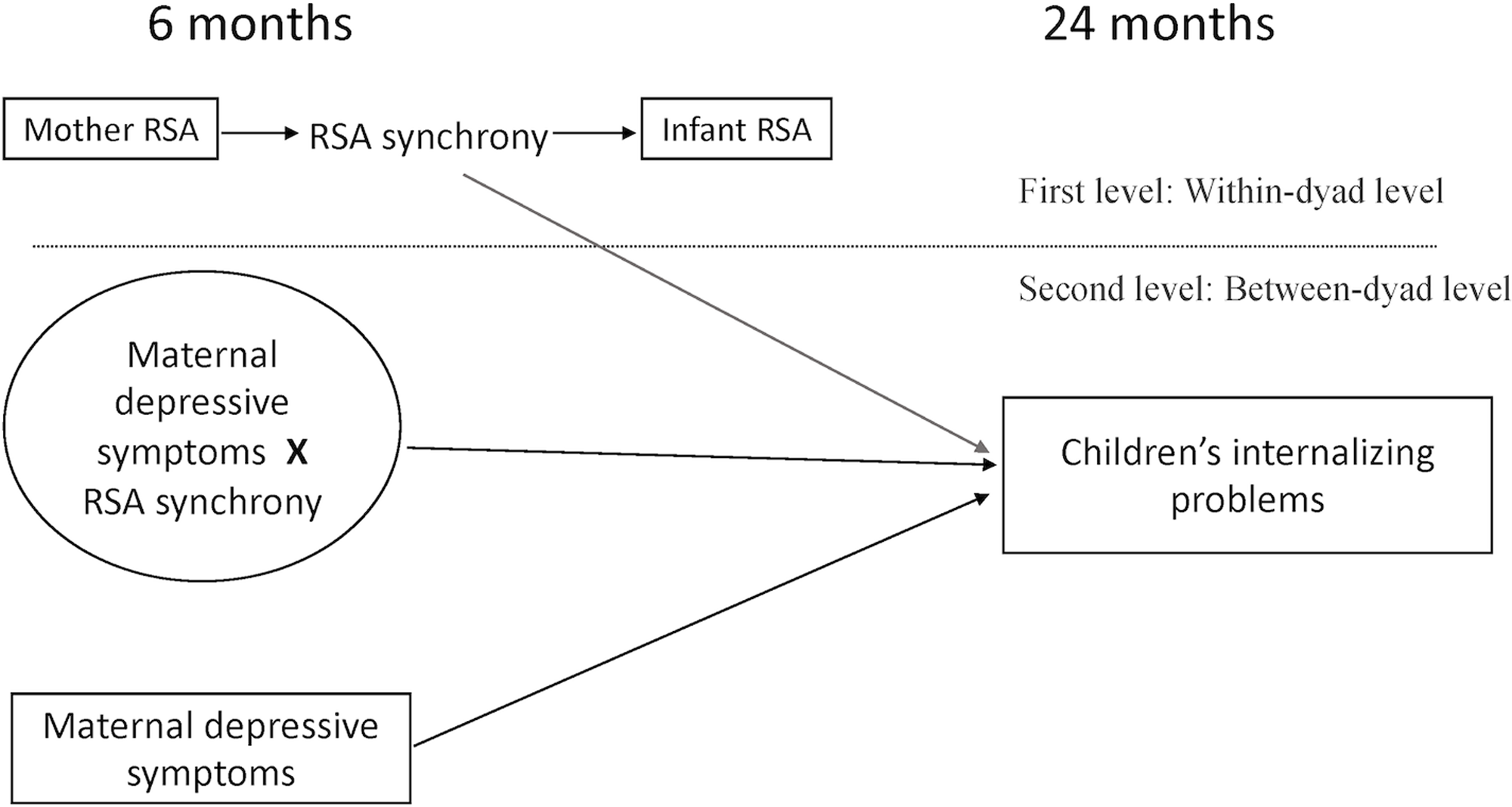
Figure 1. Multilevel SEM model illustration (Infant model: Mother RSA → Infant RSA). This model tested whether within-dyad mother–infant RSA synchrony interacted with maternal depressive symptoms to predict children’s internalizing problems.
Finally, we also conducted supplementary multilevel analyses to explore the concurrent relations between our predictors (maternal depressive symptoms, infant negative affect, and mother–infant RSA synchrony), since dyadic synchrony was a latent variable and its relations with other predictor variables can only be estimated within the multilevel models.
Results
Descriptive statistics and correlations
Descriptive statistics and bivariate correlations between study variables are presented in Table 1. Age and gender were not correlated with other study variables. Maternal depressive symptoms at 6 months were associated with children’s greater internalizing problems at 24 months (r = .18, p = .07, marginally significant). Infant negative affect at 6 months was not related to maternal depressive symptoms or children’s internalizing problems at 24 months.
Table 1. Descriptive statistics and correlations of study variables

Gender was coded -1 for boys, and 1 for girls.
† p < .1
Primary analyses
Moderating role of RSA synchrony
We modeled RSA synchrony in both directions (mother RSA → infant RSA, infant RSA → mother RSA), and the two directions had similar findings (See Table 2). Thus, we only present the infant model (i.e., mother RSA → infant RSA) in detail. As shown in Table 2, the main effects without interaction terms, and the interaction effects are presented separately. First, in both the main-effect model and the interaction-effect model, RSA synchrony model estimation shows similar results. Infant RSA demonstrated a significant intercept, indicating that the infant mean RSA level over the whole task was greater than zero on average. The fixed time effect was nonsignificant, indicating no systematic change of infant RSA with elapsed time on average. The random effect of time was significant, indicating significant variability between dyads in time trends of RSA. Notably, the fixed effect of RSA synchrony was significant, B = 0.04, SE = 0.02, p = .02, which reflected an averaged positive RSA synchrony between mothers and infants. That is, when the mother’s RSA fluctuated above her mean in a certain epoch, the infant also demonstrated higher RSA in the same epoch compared to their own mean level. In addition, the random effect of RSA synchrony was marginally significant or significant (in the main effects model: B = 0.01, SE = 0.01, p = .09; in the interaction effect model: B = 0.01, SE = 0.004, p = .03), indicating significant differences between dyads in the level of RSA synchrony within our sample. For the mother model, there were also significantly positive within-dyad RSA synchrony on average and significant differences in RSA synchrony levels between dyads.
Table 2. Multilevel SEM analyses of the effects of mother–infant RSA synchrony during free play and maternal depressive symptoms at 6 months on children’s internalizing problems at 24 months (N = 166 dyads)
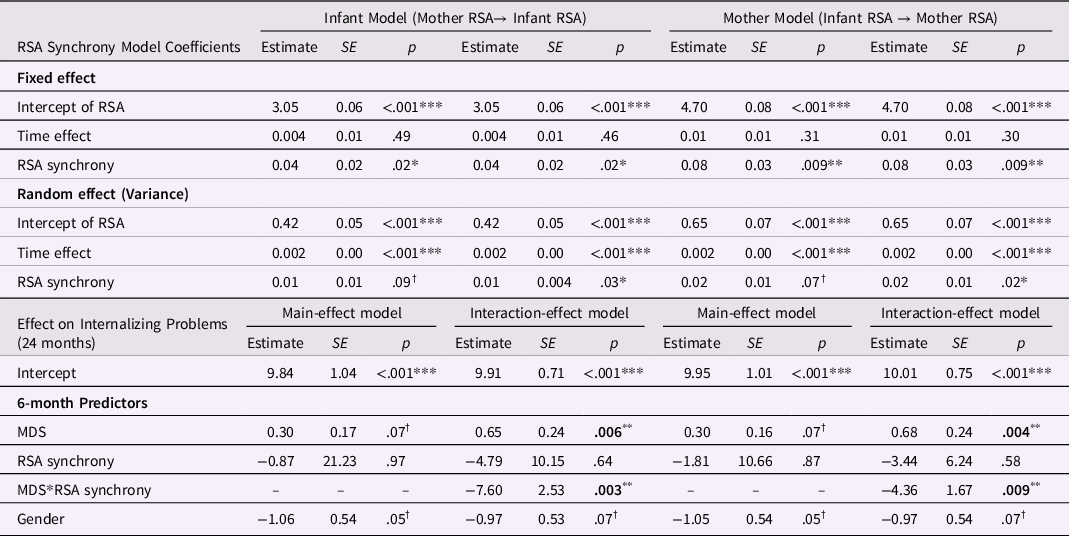
Estimate = unstandardized path coefficients; RSA = respiratory sinus arrhythmia; MDS = maternal depressive symptoms.
RSA synchrony was the slope of an individual’s RSA predicted by the partner’s person-mean-centered state RSA over time. Results for both the main-effect model and interaction-effect model were presented in this table. Significant predicting effects on child internalizing problems were bolded.
† p < .1
* p < .05
** p < .01
*** p < .001
Second, the between-dyad level analyses tested whether mother–infant RSA synchrony moderated the association between maternal postnatal depressive symptoms and children’s internalizing problems controlling for covariates. In the initial analyses, the effects of all covariates except for infant gender (infant age, BMI, and infant negative affect) were nonsignificant, thus we report the results within the parsimonious models (i.e., only gender was controlled for) in the main text. Our primary findings held in models including all covariates (see Table S2). As shown in Table 2, in the infant model, we found a marginally significant main effect of maternal depressive symptoms on children’s internalizing problems (B = 0.30, SE = 0.17, p = .07), but not the main effect of RSA synchrony (B = −0.87, SE = 21.23, p = .97). Importantly, this association between maternal depressive symptoms and children’s internalizing problems was significantly moderated by mother–infant RSA synchrony (B = −7.60, SE = 2.53, p = .003). For the mother model, the same finding emerged such that the main effect of maternal depressive symptoms on children’s internalizing problems was marginally significant, and this effect was significantly moderated by infant–mother RSA synchrony.
Simple slope analysis based on the infant interaction effect model (see Fig. 2) indicated that at low and mean levels of mother–infant RSA synchrony (–1 SD synchrony [−0.05]; mean synchrony [0.04]), greater maternal depressive symptoms were associated with higher child internalizing problems (low RSA synchrony: B = 1.07, SE = 0.34, p = .002; mean RSA synchrony: B = 0.35, SE = 0.20, p = .08, marginally significant). In contrast, at high levels of RSA synchrony (+1 SD synchrony [0.13]), the association between maternal depressive symptoms and children’s internalizing problems was nonsignificant (B = −0.37, SE = 0.28, p = .19). According to the test of the proportion affected (Roisman et al., Reference Roisman, Newman, Fraley, Haltigan, Groh and Haydon2012), under high levels of maternal depressive symptoms (57.05% dyads), infants with higher mother–infant RSA synchrony developed fewer internalizing problems compared to those with lower RSA synchrony.
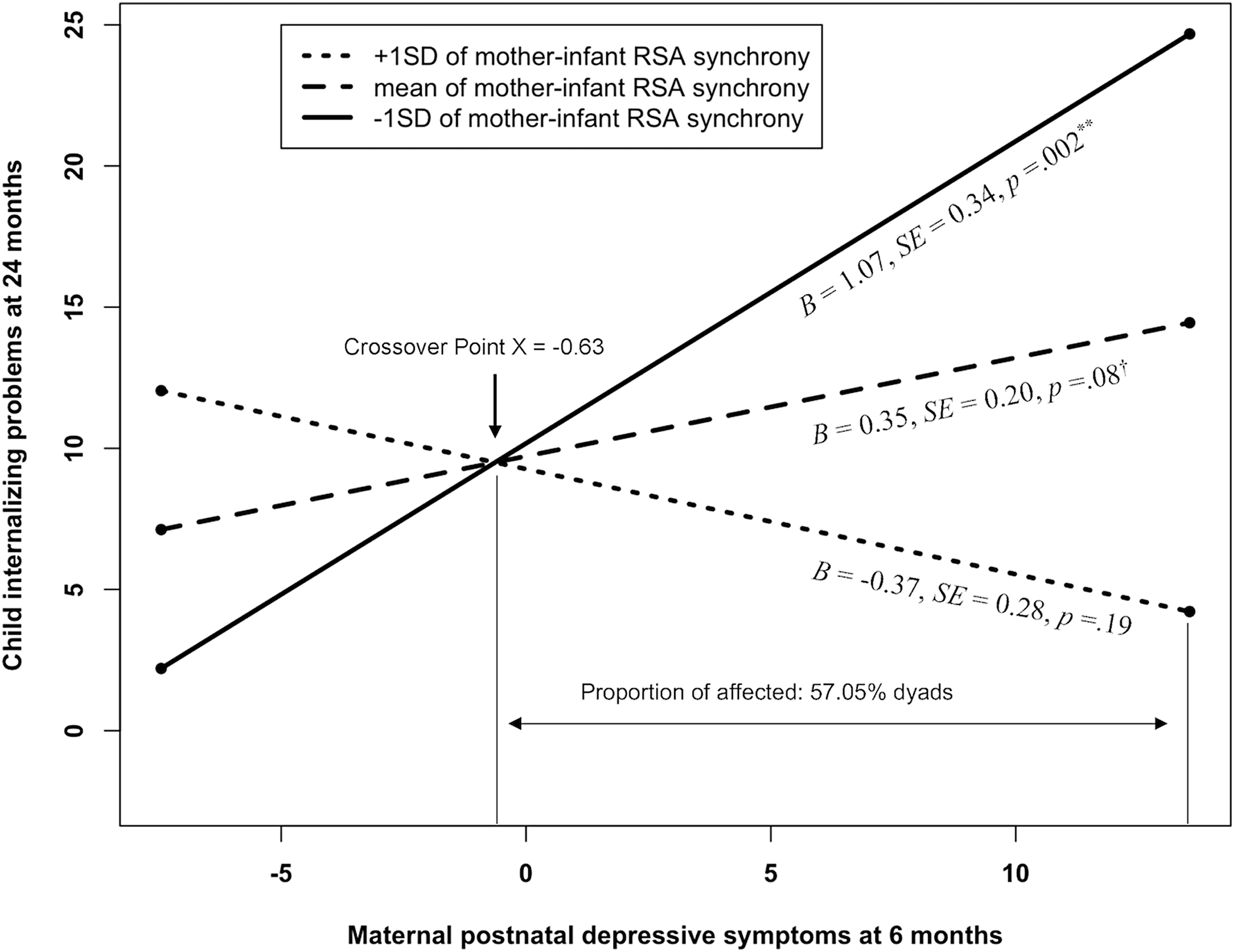
Figure 2. Simple slopes of the predicting effect of maternal depressive symptoms on child internalizing problems at high (+1 SD), mean, and low (−1 SD) levels of mother–infant RSA synchrony (Infant model: Mothe RSA → Infant RSA). Greater maternal depressive symptoms were associated with greater child internalizing problems at low and mean levels of RSA synchrony but not when RSA synchrony was high. Under high levels of maternal depressive symptoms (above the crossover point; 57.05% dyads), infants with higher mother–infant RSA synchrony developed fewer internalizing problems compared to those with lower synchrony. Centered maternal depressive symptoms ranged from −7.45 to 13.55. †p < .1 **p < .01
RoS on Z analysis based on the infant model (Fig. 3) indicated that greater maternal depressive symptoms were significantly linked to higher child internalizing problems only when mother–infant RSA synchrony was below the lower bound (i.e., RSA synchrony < 0.03 [−0.06 SD]; 37.95% of dyads fell within this region). When RSA synchrony fell into the region (from lower bound 0.03 [−0.06 SD] to upper bound 0.19 [1.54 SD]; 62.05 % of dyads fell within this region), there was no significant association between maternal depressive symptoms and child internalizing problems. When RSA synchrony was above the upper bound (i.e., RSA synchrony > 0.19 [1.54 SD]; no dyads fell within this region), the association between maternal depressive symptoms and child internalizing problems became significant and negative. Importantly, based on estimated factor scores for the latent RSA synchrony derived in Mplus, RSA synchrony in our sample ranged from −0.07 to 0.16 (See also Figure S1 for a descriptive illustration of RSA synchrony for each dyad). Hence, based on the estimated factor scores, no mother–infant dyads fell outside the upper bound (i.e., RSA synchrony > 0.19) and thus we did not find any dyads showing the pattern that greater maternal depressive symptoms were linked to lower internalizing problems. Rather, all the dyads in the present sample were showing a positive or a nonsignificant association between maternal depressive symptoms and child internalizing problems.
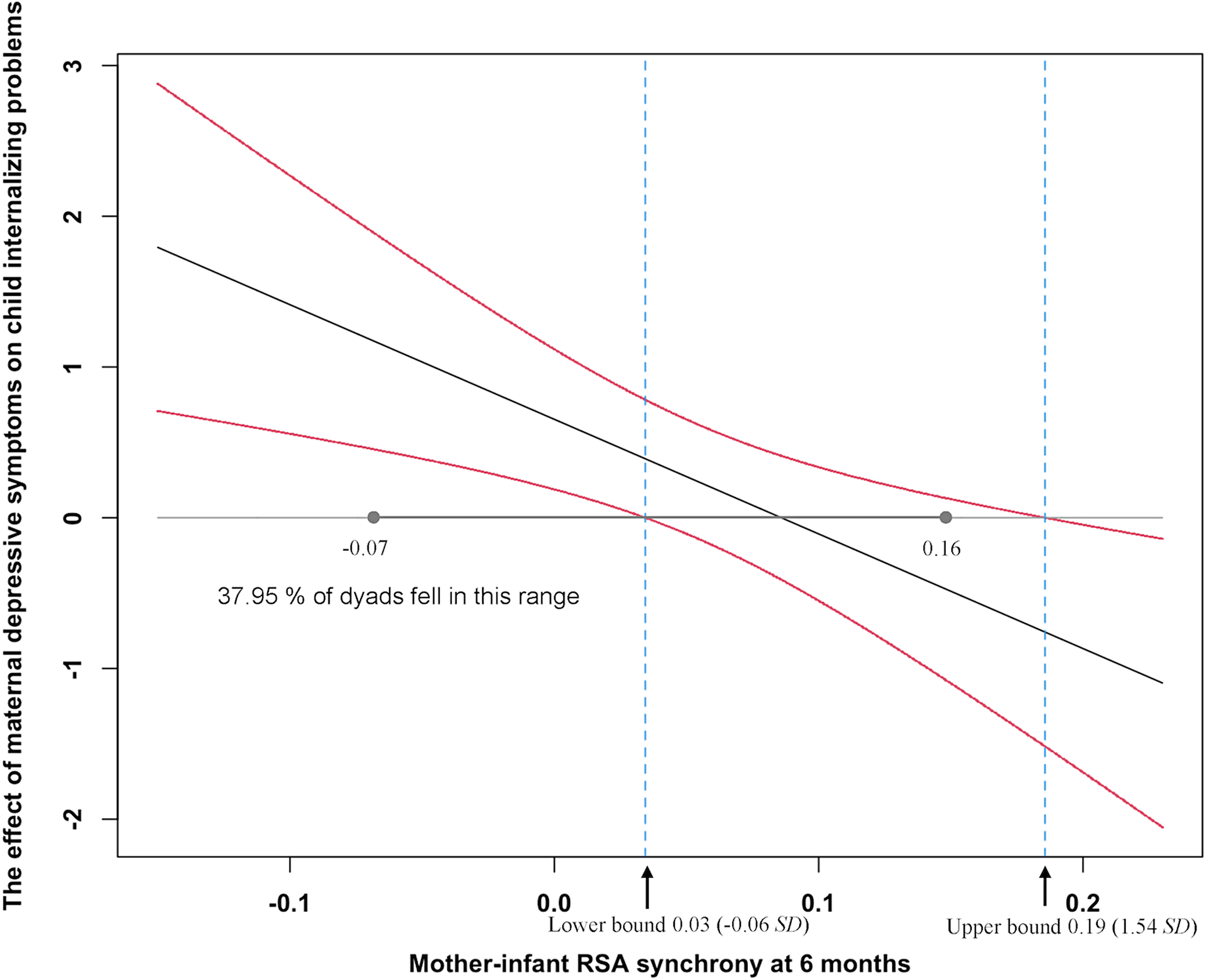
Figure 3. Johnson–Neyman plot of the region of significance (RoS) on Z (moderator: RSA synchrony; range −2 SD to 2 SD) for the effect of maternal depressive symptoms on child internalizing problems (Infant model: Mother RSA → Infant RSA). When RSA synchrony was below the lower bound of RoS (0.03; 37.95% of dyads fell within this region), greater maternal depressive symptoms were associated with higher child internalizing problems (95% confidence interval [CI] of the effect not including zero). When RSA synchrony fell into the region from the lower bound (0.03) to the upper bound (0.19; 62.05% of dyads fell within this region), the association between maternal depressive symptoms and child internalizing problems was nonsignificant (95% CI including zero). When RSA synchrony fell above the upper bound (0.19; no dyads fell within this region), greater maternal depressive symptoms were associated with lower child internalizing problems (95% CI not including zero). As the horizontal line shows, estimated factor scores for the latent RSA synchrony ranged from -0.07 to 0.16, falling below the RoS upper bound.
Finally, the supplementary analyses of concurrent relations between predictors indicated nonsignificant concurrent effects of maternal depressive symptoms and infant negative affect on mother–infant RSA synchrony (see Table S3). Effects of covariates (infant age, gender, and BMI) on RSA synchrony were also nonsignificant except for infant age. Older infants exhibited higher RSA synchrony with their mothers.
Sensitivity analyses
To further examine the robustness of our findings, we conducted additional sensitivity analyses. First, we tested whether our findings were robust to the different types of systematic time effects. In addition to our linear-time-effect model, we tested the quadratic effect of time on RSA and found that both fixed and random quadratic time effects were nonsignificant (Table S4). Furthermore, reanalyses of the primary models indicated that whether to include the quadratic time effect or linear time effect did not influence our findings in terms of the main effects and the maternal depressive symptoms-x-RSA synchrony interaction effect (Table S5). Second, to further examine the potential influence of data attrition, we repeated our primary analyses only among mother–infant dyads who completed the follow-up visit and all the findings remained the same (Table S6).
Discussion
In this two-wave study, we examined the moderating role of mother–infant RSA synchrony during free play at 6 months on the association between maternal postnatal depressive symptoms at 6 months and children’s internalizing problems at 24 months in a rural, low-SES community sample. We found that mother–infant dyads exhibited significant and positive concurrent RSA synchrony on average and significant between-dyad variation in levels of RSA synchrony. Higher levels of maternal postnatal depressive symptoms were associated with children’s (marginally significant) greater internalizing problems. A significant moderation effect of RSA synchrony also emerged, such that the association between maternal depressive symptoms and children’s internalizing problems was significant at lower levels of mother–infant RSA synchrony, but not among higher levels of RSA synchrony. Our finding highlights the protective role of mother–infant coordinated physiological coregulation during an interaction for young children at higher risk of developing internalizing symptoms in community samples.
Mother–infant RSA synchrony during free play
First, we found that mother–infant dyads demonstrated significant and positive concurrent synchrony on average, indicating concordant within-dyad RSA fluctuation around their own mean levels during free play. This finding was in line with the broad literature on RSA synchrony (meta-analysis, Miller et al., Reference Miller, Armstrong-Carter, Balter and Lorah2023). Mother–child positive RSA synchrony during an interaction partly supported Feldman’s biobehavioral synchrony theory (Feldman, Reference Feldman2012), which states that mother–infant dyads develop within-dyad coordination of behavioral and physiological responses through repeated interaction and the coordination process could be captured by biobehavioral synchrony (e.g., RSA synchrony). Such biobehavioral synchrony may have its evolutionary roots (Atzil et al., Reference Atzil, Gao, Fradkin and Barrett2018). That is, being in synchrony serves as a social dependency strategy for survival formed through human evolution. Specifically, the synchronization with caregivers’ state may help human infants develop more efficient self-regulation of allostasis (e.g., temperature, arousal, and ongoing physiology), which benefits infant survival, regulation, and social development.
Second, we found a small proportion of dyads that exhibited negative synchrony or nonsignificant synchrony during free play, although a typical pattern of positive within-dyad synchrony during free play was expected based on prior findings (e.g., Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018). Yet, during free play, negative synchrony or nonsignificant synchrony may occur when infants felt stressed in an unfamiliar experimental setting (vagal withdrawal that leads to RSA decrease), but mothers were not responding (no RSA change), or if mothers were trying to disengage from the infants (vagal augmentation that leads to RSA increase). Both of these scenarios indicate limited maternal support and disrupted coregulation processes (Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Buss, Lucas-Thompson, Boker and Timpe2015). In these cases, stressed infants did not receive the necessary external regulation from their mothers to assist in their stress regulation. Thus, infants from dyads demonstrating negative synchrony or nonsignificant synchrony may not develop self-regulation capacities to the same extent as infants experiencing positive synchrony.
The intergenerational transmission of internalizing symptoms
Our study indicated a marginally significant main effect of maternal postnatal depressive symptoms on children’s internalizing problems after controlling for infant negative affect. Children of mothers with greater depressive symptoms tended to develop more internalizing problems, although this risk transmission appeared to be fairly weak within our community sample. This finding was consistent with the large body of literature on the presence of intergenerational transmission of internalizing symptoms (for a review, Goodman, Reference Goodman, Widiger and Cannon2020). According to Goodman (Reference Goodman, Widiger and Cannon2020), the transmission of maternal depressive symptoms to children’s internalizing problems may be accounted for by several potential mechanisms, including heredity for the vulnerability of psychopathology between mothers and children and passive gene–environment correlation (rGE) such that mothers who passed on their vulnerability genes to children may also create a family environment that may exacerbate the risks. Finally, mothers with greater depressive symptoms are more likely to show greater withdrawal or higher intrusiveness during mother–child interactions (Field et al., Reference Field, Hernandez-Reif and Diego2006), both of which may promote the development of children’s internalizing problems (Gruhn et al., Reference Gruhn, Dunbar, Watson, Reising, McKee, Forehand, Cole and Compas2016). Both genetic and environmental factors may play a role in the risk of transmission in community samples.
The protective role of mother–infant RSA synchrony
Despite a nonsignificant direct association between RSA synchrony and child internalizing problems, we found that mother–infant RSA synchrony significantly attenuated the intergenerational transmission of internalizing symptoms. Whereas greater maternal depressive symptoms were linked to higher internalizing problems for children, this association was no longer significant under higher levels of RSA synchrony. This finding indicates a protective role of mother–child dyadic physiological coregulation in the intergenerational transmission of internalizing symptoms, similar to the protective effects of high-quality mother–child relationships (e.g., secure attachment, Milan et al., Reference Milan, Snow and Belay2009; Whittenburg et al., Reference Whittenburg, Stern, Brett, Straske and Cassidy2022; high interaction quality, Endendijk et al., Reference Endendijk, De Bruijn, Van Bakel, Wijnen, Pop and Van Baar2017; Leckman-Westin et al., Reference Leckman-Westin, Cohen and Stueve2009; West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020). Our finding moves the literature forward by revealing the role of physiology in mother–child coregulation in mitigating the intergenerational transmission of internalizing symptoms and thus underscores the necessity to focus on how mother–child physiology unfolds in real-time in face-to-face interactions. Furthermore, the focus of RSA synchrony advances the prior work by considering dyadic-relationship characteristics rather than focusing solely on the individual.
In documenting the moderating role of mother–infant RSA synchrony, our findings align with prior literature that RSA synchrony levels may shape how families respond to contextual risks (e.g., Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021; West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020). The role of RSA synchrony in buffering the transmission of internalizing symptoms may be accounted for by two reasons. First, RSA synchrony has been regarded as a physiological indicator of the mother–child relationship (e.g., mother–child coregulation, Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Buss, Lucas-Thompson, Boker and Timpe2015; Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018). This is because RSA synchrony, as the dyadic coordination of emotion-related physiological activity throughout an interaction, may provide a physiological basis for coordinated and reciprocal mother–child interactions (Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018; Wang et al., Reference Wang, Suveg, West, Han, Zhang, Hu and Yi2021). More specifically, during a harmonious interaction (e.g., free play), mother and child may mutually engage, modulate, and respond to each other’s emotion and emotion-related physiology, thus forming a coordinated physiological coregulation process indexed by higher RSA synchrony that could promote the formation of secure attachment (Feldman, Reference Feldman2012) and potentially buffer the adverse impact of maternal depressive symptoms on children (Milan et al., Reference Milan, Snow and Belay2009; Whittenburg et al., Reference Whittenburg, Stern, Brett, Straske and Cassidy2022). Second, the dyadic physiological coregulation process indexed by RSA synchrony may directly modulate children’s physiological arousal and facilitate children’s self-regulation (Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018), which might protect children from developing internalizing problems in the context of maternal depressive symptoms (Davis et al., Reference Davis, Suveg, Whitehead, Jones and Shaffer2016; Silk et al., Reference Silk, Shaw, Forbes, Lane and Kovacs2006). Despite these potential explanations, we did not measure mother–child attachment or child self-regulation and thus could not directly evaluate these potential mechanisms. We encourage future research to investigate this lead.
Although we documented that high mother–infant RSA synchrony during free play attenuated the intergenerational transmission of internalizing symptoms, this protective effect is inconsistent with some literature that high RSA synchrony may exaggerate the impact of risk exposure. For example, prior studies found stronger associations between contextual risks (i.e., negative parenting behaviors; Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021; maternal depressive symptoms; West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020) and youths’ behavioral problems under higher levels of mother–youth RSA synchrony (from the same sample). This inconsistency may be explained by several reasons, including sample characteristics and task contexts.
First, sample developmental stages and risk levels differed across studies. Whereas our sample was a rural, low SES, ethnically homogenous community sample of mother–infant dyads in China, Oshri et al. (Reference Oshri, Liu, Huffman and Koss2021) studied a higher risk, racially diverse sample of mother–youth dyads (age: 9-12 years) in the United States. Dyadic interaction and relationship patterns as well as children’s self-regulation ability and needs for external regulation are different in infancy versus older childhood (Feldman, Reference Feldman2010; Zeman et al., Reference Zeman, Cassano, Perry-Parrish and Stegall2006), all of which may influence mother–child physiological coregulation patterns and their implications. Additionally, a higher risk sample may have more variation in environmental factors (e.g., negative parenting) and interaction patterns (e.g., emotional arousal).
Second, the differences in findings might be attributed to differences in task contexts. Although RSA synchrony has been conceptualized as an indicator of mother–child coregulation (e.g., Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Buss, Lucas-Thompson, Boker and Timpe2015; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018), its implications may be defined by the specific task context (e.g., high vs. low stress; Birk et al., Reference Birk, Stewart and Olino2022; Davis et al., Reference Davis, West, Bilms, Morelen and Suveg2018; Fuchs et al., Reference Fuchs, Lunkenheimer and Lobo2021). Specifically, during low-stress tasks (e.g., free play), mother and child could mutually engage and respond in a positive climate, thus forming a coordinated physiological coregulation indexed by higher RSA synchrony that may facilitate children’s self-regulation and further promote children’s adjustment (Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018). Thus, higher RSA synchrony may be a protective factor that could weaken the transmission of mother and child risks as revealed in our study, or could reduce children’s behavioral problems in the context of positive parenting as documented by previous studies (e.g., Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021). In contrast, in stressful and emotionally charged interaction contexts (e.g., mother–youth conflict discussion accompanied by negative parenting behaviors), physiological synchrony may actually reflect dyads displaying mutual negative arousal (joint dysregulation instead of coordinated positive coregulation; McKone et al., Reference McKone, Woody, Ladouceur and Silk2021; Oshri et al., Reference Oshri, Liu, Huffman and Koss2021). This mutual dysregulated emotional response (which could also be indexed by higher RSA synchrony) may model negative coping and engender children to feel overwhelmed instead of being scaffolded in their self-regulation. In this context, higher RSA synchrony could potentially strengthen the adverse effects of contextual risks as documented by prior research (Oshri et al., Reference Oshri, Liu, Suveg, Caughy and Huffman2021; West et al., Reference West, Oshri, Mitaro, Caughy and Suveg2020).
Additionally, even though we treated RSA synchrony as a predictor of child outcomes as theory suggests (i.e., RSA synchrony → child psychopathology; Feldman, Reference Feldman2012; Morris et al., Reference Morris, Cui, Criss, Simmons, Cole and Hollenstein2018), RSA synchrony might also be an outcome of mother and child psychopathology symptoms (e.g., child psychopathology → RSA synchrony). That is, the moderating effect of RSA synchrony revealed in our study may indicate that weaker RSA synchrony is an outcome of higher levels of mother and child internalizing symptoms, compared to higher RSA synchrony acting as a protective factor as we conceptualized. This alternative explanation (i.e., weaker RSA synchrony being an outcome of greater child psychopathology) could not be ruled out, although (a) we measured maternal internalizing symptoms and dyadic RSA synchrony at an earlier occasion (i.e., 6 months) that proceeded the measurement of children’s internalizing problems (i.e., 24 months) and (b) we controlled for the earlier risk indicator for child internalizing problems (infant negative affect at 6 months). Thus, we encourage future studies to assess both RSA synchrony and dyadic internalizing symptoms at multiple time points to better illuminate the directionality of the findings.
Finally, we utilized estimated factor scores as an approximation for the levels of latent RSA synchrony, and we found that RSA synchrony within our sample did not fall into the region outside of the upper bound (Figure 3). Thus, in our sample, we only found evidence that greater maternal depressive symptoms were associated with higher child internalizing problems. Yet, we also note that the estimated factor scores of RSA synchrony may sometimes not equal the true scores of latent synchrony due to biases in estimation (e.g., shrinkage effect, Liu & Rhemtulla, Reference Liu and Rhemtulla2021). Thus, it is possible that in some extremely rare cases, families had true synchrony scores that fell outside the upper bound. Within this region (i.e., true synchrony score is above the upper bound), greater maternal depressive symptoms were associated with fewer child internalizing problems. Our tentative explanation for this effect is that even though mothers experience high levels of depressive symptoms, those who are still capable to engage in coordinated coregulation and maintain high levels of synchrony with their infants might be effective in providing sensitive and responsive parenting due to the presence of other protective factors. For these mothers, their children may develop fewer internalizing problems as a result of receiving positive parenting. Future work is necessary to validate such a hypothesis.
Null association of RSA synchrony with internalizing problems and maternal depressive symptoms
As a final point for our findings, we did not find a significant main effect of mother–infant RSA synchrony on toddlers’ internalizing problems. This finding is inconsistent with prior findings that documented a significant concurrent association between mother–child RSA synchrony and children’s internalizing problems in childhood (Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018; Suveg et al., Reference Suveg, West, Davis, Caughy, Smith and Oshri2019). We note, however, that the timing of our measurement for mother–infant synchrony is much earlier than the other studies. As such, it might be that the pattern of mother–child coregulation has not been well ingrained at this time to directly shape child functioning. Rather, the meaning of mother–child RSA synchrony at this period (i.e., infancy) may be more nuanced and will need to be interpreted depending on the specific developmental contexts (e.g., maternal depressive symptoms and parenting behaviors). That is, RSA synchrony might function in a context-specific manner (i.e., moderation effect) instead of demonstrating a direct effect on infant developmental outcomes.
Furthermore, we found a nonsignificant concurrent association between maternal postnatal depressive symptoms and mother–infant RSA synchrony, in contrast to prior findings for depressive symptoms dampening RSA synchrony (Suveg et al., Reference Suveg, West, Davis, Caughy, Smith and Oshri2019; Woody et al., Reference Woody, Feurer, Sosoo, Hastings and Gibb2016). Such differences may be attributed to several reasons. First, whereas prior research relied on high-risk samples (e.g., Suveg et al., Reference Suveg, West, Davis, Caughy, Smith and Oshri2019), our study focused on a lower risk community sample. Thus, mothers in our study might not be as depressed to be unable to form coordinated physiological synchrony with their infants. Second, in contrast to more stressful tasks (e.g., conflict discussion) that may be particularly challenging for mothers with greater depressive symptoms, our free-play task might not be as stressful for mothers to manifest differences. Third, although we did not find a concurrent association between maternal depressive symptoms and RSA synchrony, the former may shape the development of the latter over time. Thus, we urge future work to adopt repeated measurements of RSA synchrony to examine whether maternal depressive symptoms may shape the development of RSA synchrony over time.
Limitations and future directions
Several limitations warrant discussion. First, the present study involved a community sample, thus our findings may not generalize to a clinical sample. Second, although we controlled for infant negative affect during free play at 6 months, which may act as a proxy for antecedents of internalizing problems (Eisenberg et al., Reference Eisenberg, Cumberland, Spinrad, Fabes, Shepard, Reiser, Murphy, Losoya and Guthrie2001), we could not control for earlier levels of internalizing problems, which would have been preferable. In addition, we tested infant affect as a time-invariant covariate (i.e., one sum percentage score) and future work could further examine infant affect as a time-varying covariate (i.e., moment-by-moment affect scores) to estimate how infant affect may influence RSA and RSA synchrony. Third, we only examined RSA synchrony in a low-stress free-play task, and future research is encouraged to examine the issue in multiple contexts given task contexts in which RSA synchrony is assessed may affect its meaning and interpretation (Birk et al., Reference Birk, Stewart and Olino2022; DePasquale, Reference DePasquale2020). Fourth, although coordinated parent–child interaction may be manifested on multiple levels, here we only assessed synchrony on the physiological level within the PNS. Further studies should evaluate how synchrony within various physiological systems (e.g., ANS, HPA axis, neural systems) and on multiple levels (e.g., behavioral, physiological) may collectively shape children’s adjustment, especially in the context of maternal depressive symptoms. Finally, our study focused on mother–child RSA synchrony, but future studies could explore the role of father-child RSA synchrony, given the differences demonstrated between father–child and mother–child synchrony (Li et al., Reference Li, Sturge-Apple, Liu and Davies2020; Lunkenheimer et al., Reference Lunkenheimer, Brown and Fuchs2021).
Conclusions
Building on previous findings of the direct effect of mother–child RSA synchrony (e.g., Lunkenheimer et al., Reference Lunkenheimer, Tiberio, Skoranski, Buss and Cole2018; Suveg et al., Reference Suveg, West, Davis, Caughy, Smith and Oshri2019), our study indicated that mother–infant RSA synchrony could buffer the effects of intergenerational transmission of maternal postnatal depressive symptoms to toddlers’ internalizing problems in a rural, low-SES community sample. Findings have potential clinical implications in highlighting a protective dyadic-level physiological factor that may mitigate the intergenerational transmission of internalizing spectrum disorders. Thus, future prevention and intervention may focus on promoting a coordinated physiological coregulation between mothers and children.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579423001153.
Acknowledgments
This study was supported by grants from UNICEF, the National Natural Science Foundation of China (grant number 31771230, awarded to Li Wang, and grant number 32200877 awarded to Zhi Li), and the National Institute for Child Health and Human Development (R01HD097189, awarded to Erika Lunkenheimer). We are grateful to all families who participated in the study. We also thank all research assistants for their help in data collection and observational coding.
Competing interests
None.







