



Highlights
-
Venovenous collaterals are a common cause of hypoxaemia in Fontan patients, associated with morbidity and mortality. Limited data suggest transcatheter venovenous collateral occlusion improves oxygenation but is associated with reduced survival in a higher-risk Fontan population, particularly with elevated Fontan pressures.
-
In this study of a more contemporary Fontan cohort, transcatheter venovenous collateral occlusion appeared safe and effective, without evidence of significant harm over a median follow-up period of 4 years. The largest benefit was observed in the setting of lower baseline Fontan pressures.
-
Transcatheter venovenous collateral occlusion may be beneficial in the management of chronic hypoxaemia, without adversely effecting longer-term outcomes, in carefully selected Fontan patients.
Introduction
Venovenous collaterals are a common complication of the Fontan circulation, reported in up to 62% of patients. Reference Evans, Acherman and Mayman1 These abnormal connections between the systemic and pulmonary venous systems are thought to act as decompressing vessels in the situation where the systemic venous pressure must always exceed the pulmonary venous pressure for the Fontan circulation to “work”. Reference Magee, McCrindle, Mawson, Benson, Williams and Freedom2 Right-to-left shunting via these collaterals may assist in sustaining cardiac output via the provision of ventricular preload but results in reduced oxygen saturations and an increased risk of paradoxical embolism. As chronic hypoxaemia is associated with increased mortality and morbidity in the Fontan population, Reference Schafstedde, Nordmeyer and Schleiger3– patients may be considered for closure of their venovenous collaterals, typically by transcatheter occlusion. Short-term improvements in oxygenation have been demonstrated; however, concern exists whether these improvements are sustained, and whether any clinical benefits are derived. Reference Lluri, Levi and Aboulhosn8– Indeed, a single retrospective cohort study suggested occlusion was associated with increased mortality without any long-term improvement in oxygen saturations, though this was in a relatively high-risk Fontan cohort. Reference Poterucha, Johnson and Taggart12 We aimed to explore clinical outcomes following venovenous collateral closure in a modern population of total cavopulmonary Fontan patients followed by the Australian and New Zealand Fontan Registry.
Materials and methods
This is a retrospective cohort study of data collected from the Australian and New Zealand Fontan Registry. This includes all patients from both countries with a Fontan circulation, updated annually with correspondence from treating cardiologists and linkage with the National Death Index. The registry protocols and ethics approvals have been previously described. Reference Iyengar, Winlaw and Galati13
Patients who had undergone transcatheter venovenous collateral occlusion within the registry were identified by direct correspondence with the major interventional centres across Australia and New Zealand. Patients were excluded if they had an atriopulmonary or Kawashima-type Fontan circulation, had undergone` surgical venovenous collateral closure, had closure performed for an indication other than cyanosis, or had undergone concurrent Fontan fenestration closure.
Data were extracted from the registry between years 2000 and 2022 inclusive. Oxygen saturations were determined from ambulatory clinic visits. Baseline oxygenation was the most recent saturation prior to initial venovenous collateral occlusion procedure. Subsequent oxygen saturations were included until latest follow-up or until re-intervention (defined as additional venovenous collateral closure or Fontan fenestration closure) occurred. Clinical outcomes were assessed until latest follow-up, including beyond any potential re-intervention. Venovenous collateral size were categorised into large or small based on proceduralist description, and not objectively measured routinely.
All statistical analyses were performed using R Studio (version 4.3.2). Continuous variables are summarised as mean (standard deviation [SD]) or median (interquartile range [IQR]) where appropriate, following normality assessment by Shapiro-Wilk’s method. Categorical variables are summarised with counts and percentages. The number and percentage of missing data for each variable are reported. The pre-specified criteria of achieving a clinically important response (“a responder”) were defined as having an increase in oxygen saturations following initial venovenous collateral occlusion of greater than or equal to 5% to a resting saturation greater than or equal to 90% at latest follow-up. Difference in oxygen saturation before and after venovenous collateral closure was assessed using paired-sample student’s t-test. To compare differences between responders and non-responders, an independent student’s t-test or Wilcoxon rank sum test for continuous variables, and a Fisher’s exact test for categorical variables were performed. Two-tailed P-values less than 0.05 were considered statistically significant, and where possible, estimates were provided with the corresponding 95% confidence interval.
Results
There were 38 patients identified from the registry (n = 1,787), of which 19 were excluded (Figure 1). The remaining 19 patients comprised the cohort, where 53% were female, and the mean age was 19.3 ± 7.8 years (range 6–32). There were no previous instances of heart failure admission, transplant referral, or Fontan failure. Baseline characteristics are presented in Table 1. At the time of Fontan surgery, six patients (32%) had a fenestration created. Prior to VVC occlusion, three had undergone percutaneous closure, and two had spontaneously closed, therefore one patent Fontan fenestration remained.
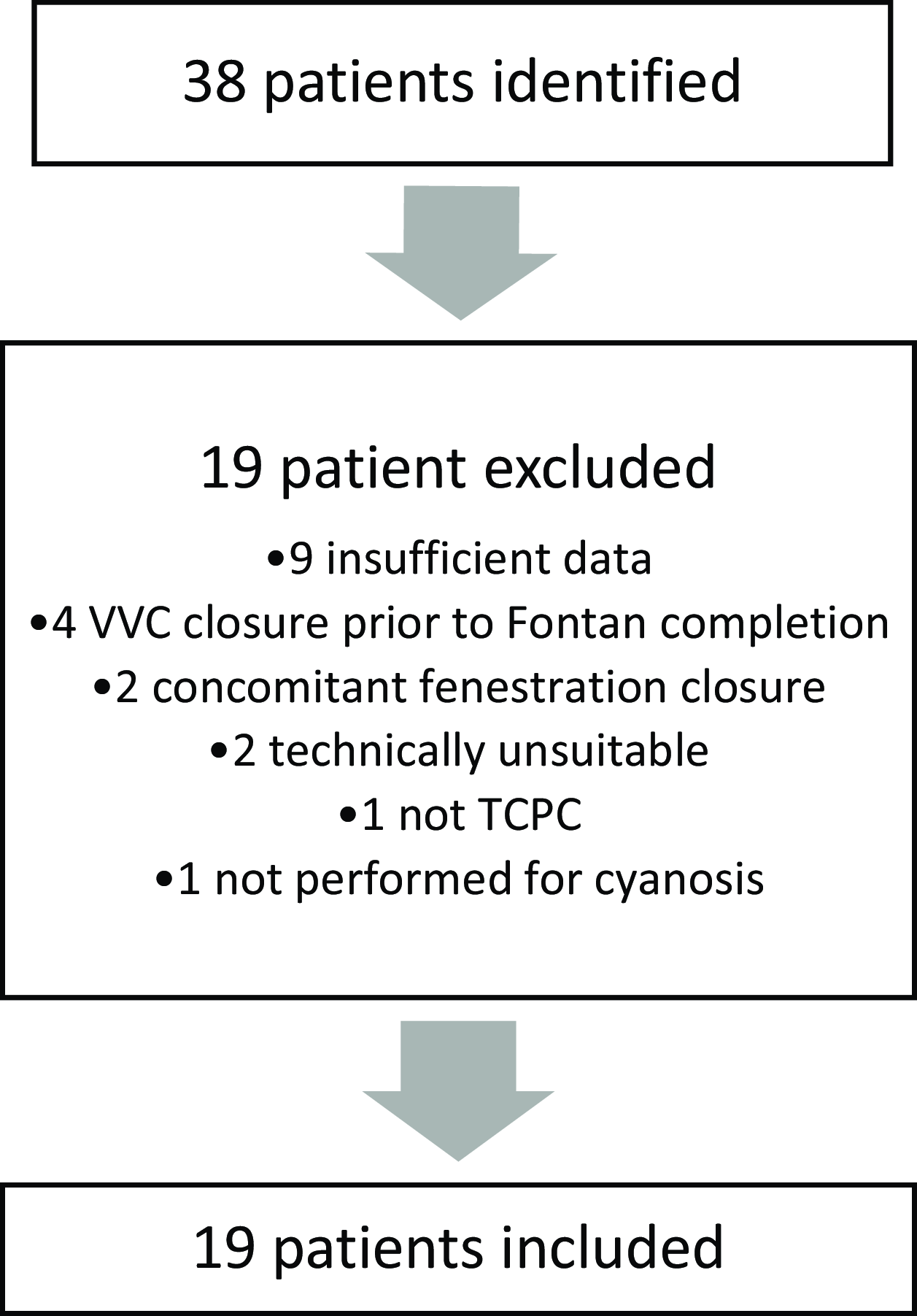
Figure 1. Flow diagram: VVC, venovenous collateral; TCPC, total cavopulmonary connection.
Table 1. Total cohort baseline, procedural, and outcome characteristics

AICD= automatic implantable cardioverter-defibrillator; AVVR= atrioventricular valve regurgitation; PLE= protein-losing enteropathy; VVC= venovenous collateral. There were 2*, 3‡ and 4† missing observations, respectively.
At the time of transcatheter venovenous collateral occlusion, the mean oxygen saturation was 87% (4.3). A total of 26 collaterals were identified, averaging 1.4 per patient. Successful closure of at least one collateral was achieved in all patients. There were two unsuccessful attempts involving additional collaterals that were both described as small by the proceduralist and unable to be engaged. Complications were reported in two patients without significant long-term sequelae. One complication involved coil embolisation, successfully snared without issue. The second complication was an intimal disruption that caused local thrombus formation following device deployment and retrieval.
The median duration of follow-up after transcatheter occlusion was 4.0 years (IQR 2.9–6.6). At latest follow-up assessment, prior to any re-intervention, mean oxygen saturations had increased to 90.5% (4.4), a mean difference of 3.5% (95%CI 1.3–5.6; p = 0.003) from baseline. Oxygen saturations over time are plotted in supplementary Figure 1.
Functional status across the whole cohort, as measured by patient-reported NYHA classification remained unchanged compared to baseline. There were no instances of heart failure hospitalisation, arrhythmia, heart transplant referral, or death observed throughout the follow-up period. One patient, with complex comorbidities including combined variable immune deficiency and chronic granulomatous bronchiectasis, experienced progressive ankle oedema at 6-month follow-up. This condition later progressed to protein-losing enteropathy and Fontan failure at 12 months.
Thromboembolic complications were observed in two patients. One experienced a stroke 22 months after venovenous collateral closure while receiving aspirin therapy, with the aetiology suspected to be embolic. Despite a clinically significant improvement in oxygen saturations (from 77% to 90%), residual flow was identified during a repeat catheterisation, and further occlusion of the same collateral vessel was performed. For the second case, stroke occurred 16 months following venovenous collateral occlusion, but was determined to be unrelated as thrombus was identified within the pulmonary artery stump. Of note however, the patient had been transitioned from warfarin to aspirin following venovenous collateral occlusion.
Among the cohort of 19 patients, 9 (47%) met the pre-specified criteria for achieving a clinically important response (Table 2). Only one patient achieved increased oxygen saturations by 5% to greater than 90%, but did not sustain this, falling below 90% oxygen at latest follow-up. This patient had elevated Fontan pressures (18 mmHg). A comparison between responders and non-responders revealed significant differences in Fontan pressures at baseline. Responders had lower central venous pressure (12.9 mmHg v 15.6 mmHg; p = 0.02) and lower superior vena caval pressure (12.7 mmHg v 15.2 mmHg; p = 0.007) compared to non-responders (Figure 2). Responders also reported improvements in functional status (NYHA classification) compared to non-responders (-0.7 vs. 0.4, p = 0.02). Sensitivity analysis excluding the patient with a patent Fontan fenestration revealed similar results (see supplementary Table 1).
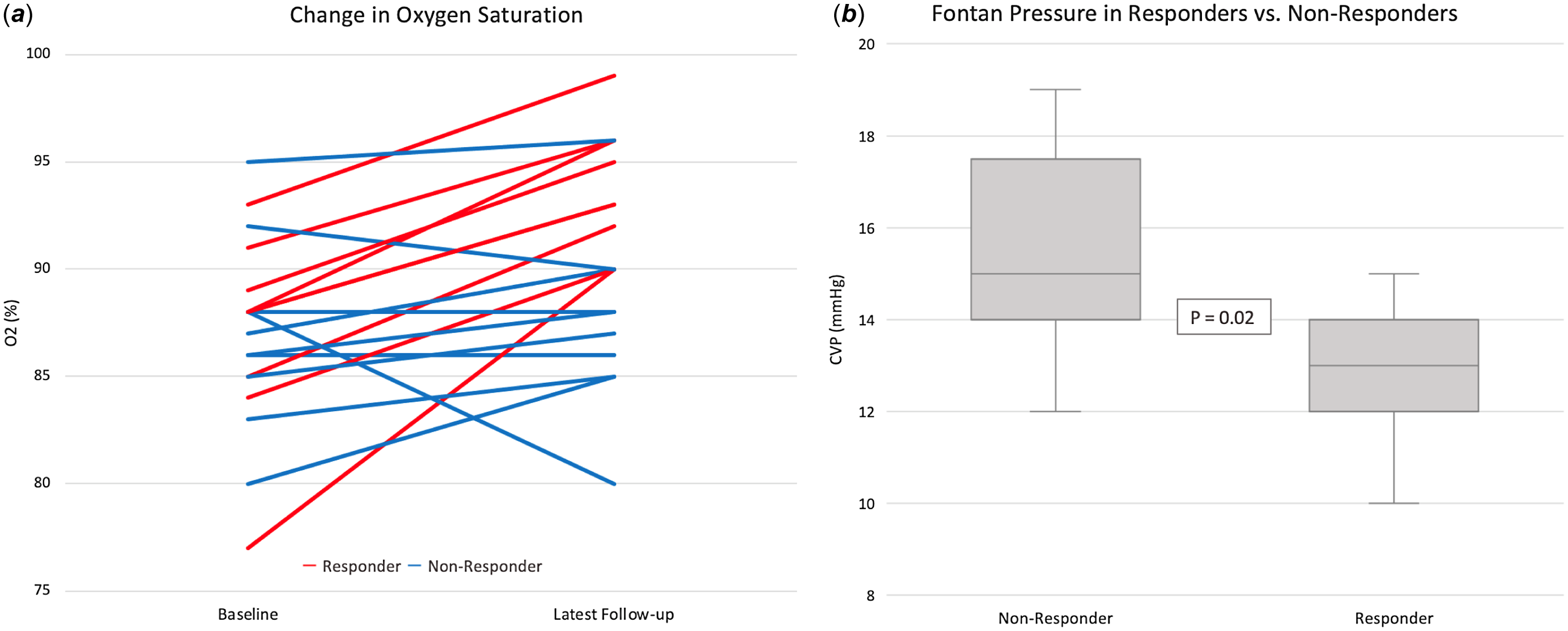
Figure 2. Oxygen saturation at baseline and latest follow-up (A) and the fontan pressure at baseline between responders and non-responders (B).
Table 2. Comparison between responders and non-responders
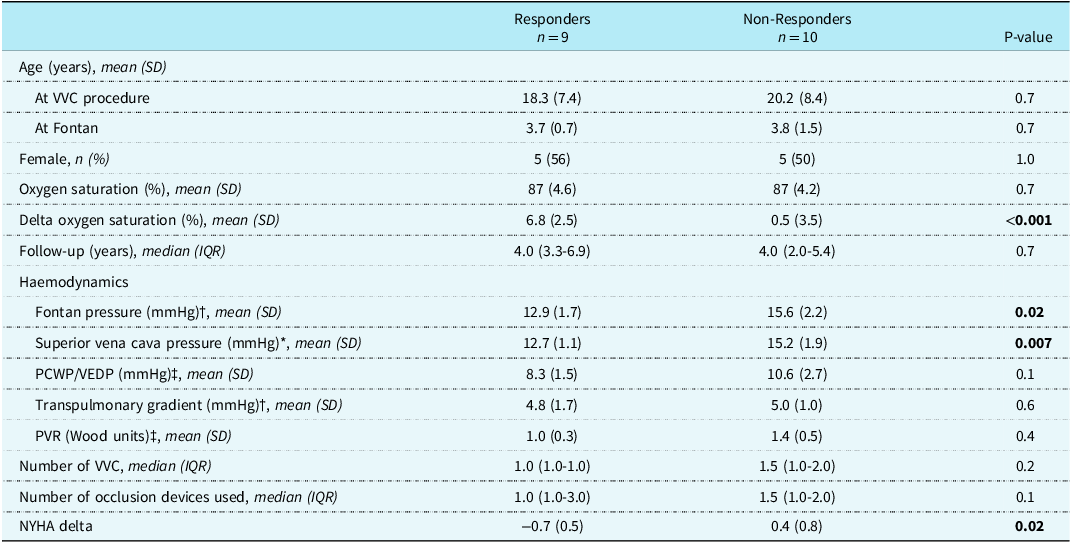
PCWP= pulmonary capillary wedge pressure; PVR= pulmonary vascular resistance; VEDP= ventricular end-diastolic pressure; VVC= venovenous collateral. There were 3*, 6†, and 7‡ missing observations, respectively.
Out of the initial cohort of 19 patients, 5 (26%) underwent re-intervention following initial venovenous collateral closure, with a mean time of 2.3 (1.3) years between procedures. The most common indication for re-intervention was hypoxaemia, in four out of the five cases. The remaining patient underwent re-intervention following a stroke, as described previously. Among the four patients who required re-intervention for cyanosis, one experienced a clinically important improvement in oxygenation but continued to report exertional symptoms and demonstrated desaturation upon exercise. Consequently, this patient underwent additional transcatheter occlusion procedure 2 years after the initial procedure with symptomatic improvement, yet to undergo further exercise testing. The three remaining patients did not experience clinically important improvements following initial closure. One had a patent Fontan fenestration, subsequently closed 6 months later, resulting in a clinically important improvement in oxygenation. The other two patients underwent further transcatheter venovenous collateral occlusion procedures, performed at 3 and 4 years after the initial intervention, respectively, resulting in modest improvements in oxygenation.
Discussion
We observed a modest increase in oxygenation post-transcatheter venovenous collateral occlusion in a small contemporary Fontan cohort. Importantly, this effect was sustained over a median follow-up duration of 4 years, the longest such reported in the literature. These results are consistent with pre-existing data reporting similar improvements in systemic oxygenation but over a shorter 2-year follow-up period. Reference Lluri, Levi and Aboulhosn8,Reference Sugiyama, Yoo and Williams10
Although the effect on oxygen saturations was modest, chronic hypoxaemia is an important predictor of mortality amongst those living with a Fontan circulation Reference Schafstedde, Nordmeyer and Schleiger3 , as well as impaired fertility and pregnancy loss, renal dysfunction, impaired neurocognitive development, and perioperative morbidity. Reference Zentner, Celermajer and Gentles4–Reference Egbe, Khan and Ammash7 The development of hypoxaemia should prompt clinicians to investigate potentially treatable causes, of which venovenous collaterals are amongst the most common. Reference Masura, Bordacova, Tittel, Berden and Podnar14
Despite the aetiology of venovenous collaterals not being completely understood, the predominating theory is they develop due to the recanalisation of embryological venous connections in response to the elevated systemic venous pressure inherent to Fontan physiology. Reference Magee, McCrindle, Mawson, Benson, Williams and Freedom2 This is supported by multiple case reports and small cohort data suggesting a relationship between their presence and higher Fontan pressures. Reference Sugiyama, Yoo and Williams10 Conflicting data from larger series have found no difference in Fontan pressures in those with and without venovenous collaterals, though this may be due to the decompressive nature of the collaterals themselves. Reference Evans, Acherman and Mayman1,Reference Lluri, Levi and Aboulhosn8
Controversy regarding the safety and long-term effectiveness of this procedure exist. In the setting of elevated Fontan pressures, venovenous collateral occlusion may be harmful and has been associated with increased mortality, especially when Fontan pressures exceeded 18 mmHg. Reference Poterucha, Johnson and Taggart12 Importantly, this cohort included relatively high-risk Fontan patients including those with isomerism and atriopulmonary connections, as well as performing venovenous collateral closure in preparation for heart transplant referral or Fontan conversion, and not solely for the indication of cyanosis. In our cohort, we observed few adverse outcomes associated with the intervention. Importantly, no instances of heart failure hospitalisations, transplant referrals, or mortality were reported during the median follow-up period of 4 years, among the longest durations reported in the literature. Although two thromboembolic events were observed, this is a known complication of the Fontan circulation even in the absence of venovenous collateral occlusion, reported in up to 25% of adults. Reference Egbe, Connolly and Niaz15
The other prevailing argument against venovenous collateral closure is that it may be a futile undertaking. Following occlusion of a decompressing collateral, a subsequent increase in central venous pressure may lead to the recanalisation of “new” collateral networks and the return of progressive hypoxaemia. This has been observed anecdotally, and in the setting of elevated Fontan pressures, the formation of new collateral networks appears more likely Reference Ozawa, Hoashi, Ohuchi, Kurosaki and Ichikawa16 , though in a minority of patients (6%). Reference Poterucha, Johnson and Taggart12 The sustained improvement in oxygenation and the low rate of re-intervention for new venovenous collaterals may suggest futility is less of a concern in this relatively low-risk, contemporary Fontan cohort.
Although only 47% of patients achieved the pre-specified clinically important response, this was associated with lower Fontan pressures at baseline, as well as modest improvement in functional capacity. These findings offer hope that following careful patient selection, a potentially favourable outcome may be associated with venovenous collateral closure in patients experiencing symptomatic cyanosis in the absence of elevated Fontan pressures.
Limitations of this study include the small sample size and the presence of missing and non-standardised variables inherent to registry-based data reliant upon treating specialists submitting correspondence. The study would have been enhanced with the inclusion of formal exercise data and objective quantification of collateral size and flow. Advances such as 4D flow at cardiac MRI may improve our ability to explore associations between collateral size, Fontan pressures, and the development of new collaterals post-closure. Reference Raimondi, Martins and Coenen17 Future prospective studies may consider incorporating longitudinal assessment of Fontan pressures, venovenous collateral flow, and cardiopulmonary exercise testing.
Conclusion
In a contemporary group of Fontan patients with chronic hypoxaemia, transcatheter occlusion of venovenous collaterals proved to be a safe procedure and yielded a modest increase in oxygenation over a median follow-up of 4 years. A clinically important improvement in oxygenation was more likely to be observed when Fontan pressures were lower. Importantly, longer-term prognosis did not appear to be adversely affected.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951124025708.
Acknowledgements
None.
Financial support
This research received no specific grant funding from any funding agency, commercial, or not-for-profit sectors.
Competing interests
None.







 Open access
Open access