



Introduction
Psychosis is a major social burden due to the tendency to chronicity, the impact on physical health, and the reduction of life expectancy by a mean of 14.5 years [Reference Hjorthøj, Stürup, McGrath and Nordentoft1–Reference Wright, Rabe-Hesketh, Woodruff, David, Murray and Bullmore3]. A crucial issue is to understand the mechanisms involved over the course of the illness [Reference Shenton, Dickey, Frumin and McCarley4]. One of the main instruments used in research for first-episode psychosis (FEP) is magnetic resonance imaging (MRI) [Reference Northoff and Qin2]. Many studies have used MRI scans to obtain information about the main volumetric changes in the brain [Reference Wright, Rabe-Hesketh, Woodruff, David, Murray and Bullmore3]. However, the structural changes are not specific and cannot be used as predictors in individual cases, so more sensitive instruments are needed [Reference Shenton, Dickey, Frumin and McCarley4, Reference Brugger and Howes5].
Another way to study the brain is with functional MRI (fMRI), which could provide an important means of understanding what happens in the brain during the processing of different stimuli. In a previous systematic review about this issue, we showed great heterogeneity among different studies [Reference González-Vivas, Soldevila-Matías, Sparano, García-Martí, Martí-Bonmatí and Crespo-Facorro6]. Most studies used resting states or different paradigms with different sensory modalities [Reference Achim, Bertrand, Sutton, Montoya, Czechowska and Malla7, Reference Tan, Choo, Fones and Chee8], in particular, visual sensory modalities [Reference Schmidt, Palaniyappan, Smieskova, Simon, Riecher-Rössler and Lang9, Reference Hawco, Buchy, Bodnar, Izadi, Dell’Elce and Messina10], through the recognition of facial emotions [Reference Tseng, Roiser, Modinos, Falkenberg, Samson and McGuire11, Reference Esslinger, Englisch, Inta, Rausch, Schirmbeck and Mier12] and cognitive paradigms [Reference Vogel, Smieskova, Schmidt, Walter, Harrisberger and Eckert13, Reference Soldevila-Matías, Albajes-Eizagirre, Radua, García-Martí, Rubio, Tordesillas-Gutierrez, Fuentes-Durá, Solanes, Fortea, Oliver and Sanjuan14]. However, relatively few of them have used emotional processing with the auditory modality, despite the importance of language in human emotions.
Our group developed an emotional auditory paradigm based on some of the most common symptoms reported by FEP patients [Reference Sanjuán, Lull, Martí-Bonmatí, Aguilar, Gadea and Moratal-Pérez15, Reference Sanjuan, Lull, Aguilar, Martí-Bonmatí, Moratal and Gonzalez16]. Under our emotional auditory paradigm, an important role of the amygdala in emotional processing in chronic patients with hallucinations can be observed [Reference Sanjuán, Lull, Martí-Bonmatí, Aguilar, Gadea and Moratal-Pérez15], and some remarkable results have been found using this method in chronic samples [Reference Aguilar, Corripio, García-Martí, Grasa, Martí-Bonmatí and Gómez-Ansón17–Reference Escartí, de la Iglesia-Vayá, Martí-Bonmatí, Robles, Carbonell and Lull19], but the issue of brain activation changes in FEP remains unclear. Thus, we hypothesize that psychotic patients will probably show abnormal fMRI-measured activation during our emotional auditory paradigm and that these patterns may be different between patients with FEP and chronic schizophrenia. The purpose of this study is to assess for the first time the fMRI-measured brain activation in response to an emotional auditory paradigm in FEP and chronic patients (compared to a healthy control [HC] group).
Materials and Methods
Subject recruitment and assessment
Patients were recruited from the outpatient psychiatry clinics. People who experienced psychotic symptoms for the first time in life were submitted to the Valencia Clinic Hospital First-Episode Unit for evaluation and treatment. Patients diagnosed with schizophrenia and persistent hallucinations (according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision [ICD-10]) were recruited from the Valencia Clinic Hospital and considered chronic patients. All patients and control participants gave written informed consent to participate in this research, which was approved by the local ethics committee. All subjects, patients, and controls were older than 18 years old.
The inclusion criteria for the patients were as follows: (a) first-episode samples, individuals who had been diagnosed with a psychotic disorder for the first time in their lives within the first 18 months after symptom onset; (b) chronic patient samples, a diagnosis of chronic auditory hallucinations that met the selection criteria for persistent hallucinations [Reference Kay and Opler22]; (c) the ability to speak Spanish fluently; and (d) informed consent for the study signed by the patient.
The exclusion criteria for the patients were as follows: (a) individuals who had previous contact with mental health services for psychosis, (b) evidence of psychotic symptoms precipitated by an organic cause, (c) transient psychotic symptoms resulting from acute intoxication, (d) substance abuse (except tobacco), (e) a metal prosthesis, or (f) claustrophobia. Two weeks after their diagnosis, all of the patients underwent a semistructured interview including sociological information and clinical scales. After the clinical evaluation, they were subjected to an fMRI scan, with a minimum interval of 6 months after their diagnosis.
A sample of HCs matched for age, sex, education level, and work status was recruited from the same geographic areas as the patients. The inclusion criteria for the HCs were the same as those for the patients, except for past or present psychotic symptoms. The exclusion criteria were the same as those for the patients but also included (a) past or present psychotic symptoms or past criteria for psychoactive drug abuse or dependence (except for tobacco) and (b) having a first-degree relative with a history of a diagnosed psychotic disorder. No individual in either group suffered from hearing loss.
The patients’ sociodemographic data are shown in Table 1. There were significant differences in age (0.04), work status (0.032), and coexistence (0.001) between the FEP and chronic groups (0.04).
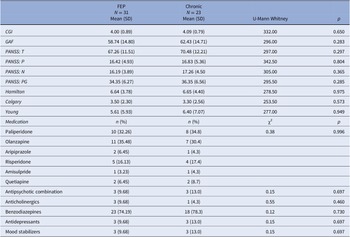
Table 1. Sociodemographic characteristics of subjects.

Abbreviation: FEP, first-episode psychosis.
* Tukey HSD (p < 0.05): Control ≠ Chronic patients; FEP ≠ Chronic patients.
The final sample consisted of 85 subjects, which included 31 FEP patients with nonaffective psychotic disorders (a manic episode with psychotic features, schizoaffective disorder, transient psychotic disorders, persistent delusional disorder, bipolar affective disorder with psychotic features, and schizophreniform disorder), 23 chronic patients with schizophrenia and persistent auditory hallucinations, and 31 HCs.
Psychopathological measurements
Patients were assessed by personnel trained in FEP evaluation. Interviews were conducted during the first episode and a few days after the start of treatment (JS). All FEP patients underwent several psychopathological measurements, including the Clinical Global Impression [Reference Haro, Kamath, Ochoa, Novick, Rele, Fargas, Rodríguez, Rele, Orta, Kharbeng, Araya, Gervin, Alonso, Mavreas, Lavrentzou, Liontos, Gregor and Jones20], to provide a global rating of illness severity, improvement, and response to treatment; the Global Assessment of Function [Reference Jones, Thornicroft, Coffey and Dunn21], to provide understanding about how well FEP patients could perform everyday activities; and the PANSS [Reference Kay and Opler22], which is a well-established scale that has been used to assess schizophrenia symptoms objectively. The results of the clinical measurements are summarized in Table 2. No significant clinical differences were found in any of these scales between the FEP and chronic groups.
Table 2. Clinical characteristics of subjects.

Abbreviations: CGI, Clinical Global Impression; GAF, Global Assessment of Function.
fMRI experimental paradigm
An emotional auditory fMRI stimulation paradigm designed by our group [Reference Sanjuán, Lull, Martí-Bonmatí, Aguilar, Gadea and Moratal-Pérez15, Reference Sanjuan, Lull, Aguilar, Martí-Bonmatí, Moratal and Gonzalez16] was employed. The emotional response paradigm was designed to replicate the emotions related to hallucinatory experiences. Eighty-two patients with schizophrenia meeting DSM-IV criteria with AH were selected to choose words of emotional content specific to their psychoses. All patients were administered the PSYRATS, and their discourses about the content of their AH were recorded on tape. The recordings underwent transcription. Hallucinations based on complex phrases or with neutral content were ruled out. A qualitative analysis of their content in five categories was conducted: negative content and imperative tone, insults, imperative tone, and exclamations related to emotional states and positive content. The final paradigm included 13 emotional Spanish words considering their frequency of presentation in the patient’s hallucinations and 13 neutral words with a similar grammar complexity and frequency of use. For the recording procedure, a professional actor from a specialized center was hired to pronounce the words. He pronounced neutral words using a neutral tone and emotional words using an emotional tone but maintained a constant voice intensity (65 dB) [Reference Algarabel González23]. A set of earphones connected by a pair of air tubes to an external audio player was used. Two different fMRI acquisitions, neutral and emotional, were conducted for each subject. The neutral words were presented first using a block design approach. Four blocks of rest and four blocks of stimulation were interleaved and presented to each participant. Each block lasted 20 s. Subjects were informed before the MR acquisition about the experiment and were asked to focus their attention on the words.
Neuroimaging acquisition and data processing
The mean time between clinical treatment and fMRI acquisition was 4 weeks (sd +/− 6). A 3-T magnet (Achieva, Philips Medical Systems, Best, The Netherlands) was used to acquire the fMRI images. A 32-channel head coil and a dynamic echo-planar imaging T2*-weighted sequence were used (repetition time = 2.000 ms; echo time = 30 ms; flip angle 90; slice thickness = 3.50 mm with no interslice gap; acquisition matrix = 128 × 128; voxel size = 1.80 × 1.80 × 3.50 mm), covering the whole brain with 40 contiguous slices. Additionally, a 3-dimensional spoiled gradient-echo pulse T1 image was also acquired for anatomic assessment (repetition time = 13.18 ms; echo time = 7.38 ms; flip angle = 8°; NEX = 1; slice thickness = 1 with no interslice gap; acquisition matrix = 256 × 256; voxel size = 0.90 × 0.90 × 1 mm; 160 slices, thickness = 1 mm). Each fMRI session (emotional and nonemotional) had a total duration of 160 s. After the acquisition, a radiologist and a computer engineer checked the images to ensure data quality. During the acquisition, the patients were under direct observation and they asked about their experiences immediately after the fMRI procedure. Data were then anonymized and transferred to a workstation for postprocessing analysis.
Functional images were realigned to correct for involuntary movement of the patient’s head during the test. Those subjects with translation movements (x, y, z) >1.80 mm (voxel size) were discarded, resulting in a final sample of 31 HCs, 31 FEPs, and 23 chronic patients. Afterwards, a slice timing correction to adjust for temporal delays between the first and the last slices in each fMRI dynamic was applied. Then, a normalization algorithm to standardize the brains to a referenced template (MNI350, Montreal Neurological Institute) was used. Finally, the normalized images were smoothed with a 6-mm FWHM Gaussian smoothing kernel. These analyses were conducted using the Statistical Parametric Mapping SPM software (SPM8, Wellcome Institute, London, United Kingdom) on MATLAB R2017a (The MathWorks, Natick, MA).
Statistics
To describe the fMRI response in each group of patients (or in HCs), we used one-sample t-tests. To assess whether patients with FEP (or with chronic schizophrenia) showed abnormal fMRI responses, we used two-sample t-tests (i.e., comparing their response to the HCs). Finally, to compare the fMRI responses between FEP and chronic schizophrenia, we also used two-sample t-tests. We did not use ANOVAs because we were not interested in knowing if there were differences between the three groups per se; we only used the HC data to provide a reference of normality. To correct for multiple testing, the familywise error (FWE) was applied. Only uncorrected tests for exploratory purposes were applied when no clusters survived the FWE rate correction. Additionally, an extent threshold was applied to consider only those clusters with the minimum number (k) of contiguous voxels as the expected number of voxels per cluster provided by SPM. Finally, the Automatic Area Labeling [Reference Tzourio-Mazoyer, Landeau, Papathanassiou, Crivello, Etard and Delcroix24] atlas was used to report the areas of activation.
Results
fMRI response to emotional stimulation
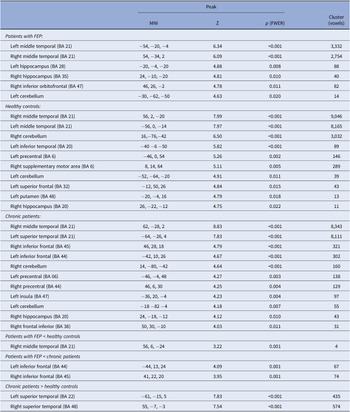
Patients with FEP showed activation during the emotional word task in the bilateral middle temporal (BA 21), bilateral hippocampus (left, BA 28; right, BA 35), right inferior orbitofrontal (BA 47), and left cerebellum (Table 3 and Figure 1).
Table 3. Regions showing activation when hearing of emotional versus neutral words in patients with FEP, healthy controls, and chronic patients.

Note: Additionally differences in functional activation between FEP versus healthy controls and FEP versus chronic patients were showed. Statistical threshold: familywise error rate (FWER) < 0.05 with 10-voxel cluster extent, except for the between-group comparisons (uncorrected p < 0.001).
Abbreviations: BA, Brodmann area; FEP: first-episode psychosis; FWER, familywise error rate; MNI, Montreal neurological institute.

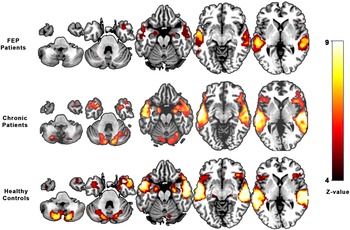
Figure 1. Brain activation during emotional auditory paradigm in first-episode psychosis patients, chronic psychosis patients, and healthy controls.
HCs showed a similar pattern of activation, including the bilateral middle temporal (BA 21), left inferior temporal (BA 20), bilateral cerebellum, left precentral (BA 6), right supplementary motor area (BA 6), left superior frontal (BA 32), left putamen (BA 48), and right hippocampus (BA 20) (see Table 3 and Figure 1).
Chronic patients mainly activated the right middle temporal (BA 21), left superior temporal (BA 21), bilateral inferior frontal (left, BA 44; right, BA 45), bilateral cerebellum, bilateral precentral (left, BA 06; right, BA 44), left insula (BA 47), right hippocampus (BA 20), and right frontal inferior gyrus (BA 38) (see Table 3 and Figure 1).
Compared with control subjects, FEP patients did not show any differences in activation, with FWER <0.05. However, using a liberal threshold (uncorrected p < 0.001), they showed hypoactivation in the right temporal lobe (BA 21). Similarly, the inferior frontal gyrus (bilateral) showed a significant reduction in activation in FEP patients when compared with chronic patients (uncorrected p < 0.001) (BA 44, BA 45) (Table 3).
Discussion
Three main findings resulted from the present study. First, this study provides an image comparison of FEP patients to HCs and found reduced activity in the bilateral temporal cortex (mainly on the right side). Functional studies about emotional processing in HCs have differentiated successive steps (auditory analysis and evaluative judgments) of cerebral processing involving auditory analysis within the temporal lobe [Reference Schirmer and Kotz25, Reference Wildgruber, Ackermann, Kreifelts and Ethofer26].
Second, interestingly, the CHrP group showed the opposite, greater activation in the bilateral superior temporal lobe than HCs and FEP patients during the processing of emotional words. These results suggested that the temporal lobe plays a critical but complex role in the pathogenesis of psychosis. The auditory cortex has been reported to play a pivotal role in the processing of affective prosody [Reference Wildgruber, Ackermann, Kreifelts and Ethofer26, Reference Sander, Grandjean, Pourtois, Schwartz, Seghier and Scherer27].
We observed a decrease in activation in the right middle temporal lobe in the FEP group. This finding is in accordance with the assumption that this area subserves the representation of meaningful prosodic sequences in the processing of emotional words and suggests that abnormal processing of emotional words in FEP patients was conducted in the limbic system rather than in the auditory cortex [Reference González-Vivas, Soldevila-Matías, Sparano, García-Martí, Martí-Bonmatí and Crespo-Facorro6].
Interestingly, our previous systematic review of longitudinal fMRI studies in FEP [Reference González-Vivas, Soldevila-Matías, Sparano, García-Martí, Martí-Bonmatí and Crespo-Facorro6] showed a tendency toward normalization of brain activity after several months of antipsychotic treatment. However, in a recent study, we found different results using an emotional auditory paradigm, likely due to clinical heterogeneity and methodological issues [Reference González-Vivas, García-Martí, Soldevila-Matías, Sanz-Requena, Aguilar and Castro-Bleda28].
In this sense, our results confirm that middle temporal functional alterations in FEP patients represent one key neural factor in the pathophysiology of psychosis. Considering that when HCs’ enhanced brain activity is involved, it is predominantly the temporal cortex, and passive listening to speech with prosody-caused activation relies on the right temporal cortex [Reference Woodruff29, Reference Mwansisya, Hu, Li, Chen, Wu and Huang30].
Activation in the temporal lobes is shown (Figure 1), corresponding to the expected stimulation of auditory brain areas by the auditory paradigm used during the scan. These findings matched the images obtained from HCs. Hyperactivity in the temporal areas was observed, matching the images obtained from chronic psychotic patients in previous studies [Reference Sanjuan, Lull, Aguilar, Martí-Bonmatí, Moratal and Gonzalez16, Reference Martí-Bonmatí, Lull, Garcia-Martí, Aguilar, Moratal-Pérez and Poyatos18, Reference Escartí, de la Iglesia-Vayá, Martí-Bonmatí, Robles, Carbonell and Lull19]. This established a link between enhanced activity in emotional and temporal processing regions [Reference Martí-Bonmatí, Lull, Garcia-Martí, Aguilar, Moratal-Pérez and Poyatos18, Reference Escartí, de la Iglesia-Vayá, Martí-Bonmatí, Robles, Carbonell and Lull19, Reference Modinos, Tseng, Falkenberg, Samson, Mcguire and Allen31] and their centrality in the pathophysiology of psychosis symptoms as a continuum of brain changes.
The fact that the temporal lobe and limbic regions were the most clearly affected areas in our previous studies using the same paradigm in chronic patients [Reference Escartí, de la Iglesia-Vayá, Martí-Bonmatí, Robles, Carbonell and Lull19] shows how limbic system areas are implicated in the emotional response, fitting Kapur’s model in which the core of psychosis could be an abnormal “salience” to external stimuli [Reference Kapur32] or, as more recently suggested, an abnormal connectivity between perceptual and emotional brain areas [Reference Dong, Wang, Chang, Luo and Yao33].
The most likely explanation for understanding the differences between our results and previous studies is that the alterations in the emotion fMRI auditory paradigm in psychotic patients are different in specific stages of the disorder and might be more noticeable during certain stages [Reference González-Vivas, García-Martí, Soldevila-Matías, Sanz-Requena, Aguilar and Castro-Bleda28]. Thus, increased activation during the emotional paradigm may suggest hemodynamic dysfunctions associated with different functional changes in temporal and limbic regions [Reference Sanjuan, Lull, Aguilar, Martí-Bonmatí, Moratal and Gonzalez16, Reference Martí-Bonmatí, Lull, Garcia-Martí, Aguilar, Moratal-Pérez and Poyatos18, Reference Escartí, de la Iglesia-Vayá, Martí-Bonmatí, Robles, Carbonell and Lull19] while considering psychosis as a continuum of changes depending on the illness stage and starting from mild emotional impairments to serious psychotic symptoms.
Although neuroimaging studies have revealed alterations in emotional processing [Reference Green, Bearden, Cannon, Fiske, Hellemann and Horan34] and social functioning [Reference Valmaggia, Stahl, Yung, Nelson, Fusar-Poli and McGorry35] in FEP patients, as well as enhanced brain activity in chronic patients [Reference Sanjuan, Lull, Aguilar, Martí-Bonmatí, Moratal and Gonzalez16], our results provide the first evidence that activation under an emotional auditory paradigm during fMRI in FEP patients was decreased in the bilateral temporal lobes compared with HCs. This attenuation of the response to emotional auditory stimuli may be a key neurobiological mechanism associated with clinical manifestations in the early stages of psychosis. The greater activation of the temporal lobe in CHrPs might be the result of emotional memory with a key role of the amygdala and hippocampus [Reference Escartí, de la Iglesia-Vayá, Martí-Bonmatí, Robles, Carbonell and Lull19].
Third, FEP patients showed lower activation in the bilateral inferior frontal area than chronic patients during the processing of emotional words. Although differences in brain activation patterns between FEP and chronic psychotic stages have been widely assessed, the results have been controversial. In a systematic review, Mwansisya et al. [Reference Mwansisya, Hu, Li, Chen, Wu and Huang30] found a pattern of frontotemporal dysfunction on fMRI in first-episode schizophrenia similar to that classically observed in chronic schizophrenia. In contrast, Li et al. [Reference Li, Wang, Zhang, Rolls, Yang and Palaniyappan36] provided evidence for a different connectivity between FEP and chronic stages. Moreover, our group, in a recent meta-analysis, showed that the left precuneus and insula appear to be the main affected areas in FEP but not the frontal areas [Reference Soldevila-Matías, Albajes-Eizagirre, Radua, García-Martí, Rubio, Tordesillas-Gutierrez, Fuentes-Durá, Solanes, Fortea, Oliver and Sanjuan14]. Nevertheless, this review included only cognitive task studies, and the differences in the results highlight the relevance of the type of paradigm used in relation to the brain activation areas.
This study has some limitations. Although most fMRI studies involve <30 patients, it is a limitation of the field, and this study must be interpreted wisely due to the relatively small sample size recruited. Differences between sample sizes in the HC and FEP groups and gender distribution should also be considered. Although the results in each clinical group were reported using the more restrictive statistical correction for multiple comparisons (FWE), the between-group test did not show any surviving cluster, and the results were presented in an exploratory way, uncorrected. Most likely, the relative number of samples in each group may cause that situation. Additional studies with more samples are needed to confirm these findings. The second limitation was that all FEP patients were on medication, mostly first-generation antipsychotics, at the time of the study, and there was no standardization of medications or doses, which could clearly affect the results. Thus, it cannot be omitted that medication dose had an impact on brain activity; however, dysfunctions in emotional processing can be unaffected by antipsychotics in FEP patients [Reference Modinos, Tseng, Falkenberg, Samson, Mcguire and Allen31, Reference Habel, Reske, Kellermann, Stöcker and Shah37], and their antipsychotic effects have been reported on fMRI as primarily affecting executive and memory function [Reference Fusar-Poli, Broome, Matthiasson, Williams, Brammer and McGuire38]. Moreover, dysfunction in emotional processing has been obtained previously in FEP antipsychotic-naïve patients [Reference Bergé, Carmona, Salgado, Rovira, Bulbena and Vilarroya39]. Finally, another limitation is the difference in the mean age between the FEP and chronic groups (p = 0.04), which could also affect the fMRI results.
Conversely, this study has some strengths that should be noted. The main strength is that this is the first cross-sectional study investigating fMRI changes in FEP and CHrP samples with an emotional auditory paradigm. Paradigm selection is a key question in neuroimaging, and there is a lack of studies using noncognitive tasks during scans. This study provides relevant information to understand the dysfunction of the emotional response in FEP patients compared with CHrP. The study used a rigorous approach to analyze brain activity during the emotional fMRI auditory paradigm.
Conclusions
To the best of our knowledge, this is the first study to identify fMRI activity involved in emotional auditory processing in FEP and CHrP patients. Our results suggested that the temporal lobe might be a key issue in the physiopathology of psychosis, although abnormal activation could also be derived from a connectivity problem. This role of the temporal lobe changes depending on the stage of the illness. Lower activation in the early stage might progress to greater activation when patients become chronic. This study highlights the relevance of using not only cognitive tasks but also emotional paradigms to better understand brain activation at different stages of psychosis and the potential of this method as a biomarker for the prediction of FEP outcomes.
Data Availability Statement
The data that support the findings of this study are not publicly available due to the privacy of research participants. Requests may be sent to the Clinical Research Ethics Committee of INCLIVA.
Author Contributions
Conceptualization: P.S.-M., G.G.-M., I.F-D., and J.S.; Data curation: I.F.-D., J.C.R., C.G.-V., and J.R.; Formal analysis: P.S.-M., G.G.-M., J.C.R., L.G.-N., C.G.-V., and J.R.; Investigation: P.S.-M.; Methodology: P.S.-M.; Supervision: J.S.; Visualization: P.S.-M., G.G-M.; Writing—original draft: P.S.-M., I.F-D.; Writing—reviewing and editing: G.G.-M., J.C.R., L.G.-N., and J.R.
Funding Statement
This study was supported by grants from the Generalitat Valenciana (PROMETEO/2020/024) and Carlos III Health Institute (ISCiii PI20/00473) and was co-funded by the European Union through FEDER funds.
Conflict of interest
The authors declare none.


 Open access
Open access
Comments
No Comments have been published for this article.