



UK Biobank is a very large, population-based cohort study established to identify the determinants of common life-threatening and disabling conditions.Reference Sudlow, Gallacher, Allen, Beral, Burton and Danesh1 Most of these conditions, such as heart disease, stroke and mental disorders, are multifactorial, involving multiple genes of small effect and complex relationships with environmental exposures. This means that large samples are required to study associations between these exposures and disease, and to identify targets for treatment and prevention.Reference Weissman, Brown and Talati2 The utility of traditional epidemiological study designs is often limited by their focus on single disorders or exposures and their relatively modest sample sizes.Reference Bell3 UK Biobank is an open-access resource providing detailed characterisation of over half a million people aged 40–69 years at recruitment, with proposed long-term follow-up. Recruitment was completed in 2010, and consent was obtained for future contact and linkage to routinely collected health-related data, such as those produced by the National Health Service (NHS). Baseline measures were extensive, from family history to sensory acuity (a searchable breakdown can be found at www.ukbiobank.ac.uk), and the resource continues to grow. Genotyping of the whole cohort was completed earlier this year, blood biomarkers are due next year, and multimodal imaging is underway for 100 000 participants. Information on local environmental factors, such as air pollution, is also available. The design of UK Biobank offers the opportunity to examine a wide range of risk factors and outcomes in a sample large enough to provide the power to detect small effects, making UK Biobank a highly efficient resource for observational epidemiology.
The effect of mental disorders on disability and quality of life is considerable,Reference Prince, Patel, Saxena, Maj, Maselko and Phillips4 accounting for the equivalent of over 1.2 million person years lost to disability from mental and substance use disorders in England alone in 2013.Reference Newton, Briggs, Murray, Dicker, Foreman and Wang5 Recent work has also highlighted the potential detrimental effect of mental disorders on both onset and outcome of physical disease.Reference Barnett, Mercer, Norbury, Watt, Wyke and Guthrie6–Reference Chang, Hayes, Broadbent, Hotopf, Davies and Møller8 Having mental health phenotypes available, in conjunction with the wealth of other data in the UK Biobank, would offer considerable opportunities to study aetiological and prognostic factors. The UK Biobank baseline data collection involved limited assessment of mental health, consisting of several questions about mood and a neuroticism scale, expanded for the past 172 729 recruited participants with questions to allow provisional categorisation of mood disorder;Reference Smith, Nicholl, Cullen, Martin, Ul-Haq and Evans9 however, there was considerable scope for further characterisation of mental disorders among participants.
Outcome ascertainment
Characterising mental disorders in a cohort such as UK Biobank poses several challenges. First, most mental disorders manifest before 30 years of age and have fluctuating courses,Reference Kessler, Amminger, Aguilar-Gaxiola, Alonso, Lee and Ustun10 so a ‘snapshot’ of disorder status at one point in time, as identified by most screening tools, is likely to be less useful than a lifetime history. Second, traditional diagnostic approaches to mental disorders, relying upon clinician assessment at interview, would be prohibitively expensive in a cohort of this size. Third, using self-report of diagnosis or data from record linkages relies upon recognition of illness and reflects healthcare usage patterns, whereas many people with mental disorders never seek or receive treatment.Reference Kessler, Amminger, Aguilar-Gaxiola, Alonso, Lee and Ustun10, Reference Newson, Karlsson and Tiemeier11 In response to these challenges, we developed a dual approach: secondary care record linkage for identification of more severe illnesses such as schizophrenia,Reference Davis, Sudlow and Hotopf12 and self-report of symptoms of common mental disorders, which might not have come to clinical attention. As part of our mental health phenotyping programme, we therefore developed an online mental health questionnaire (MHQ) for participants to complete regarding lifetime symptoms of mental disorders. The MHQ aimed to exploit the efficiency of ‘e-surveys’Reference Pitman, Osborn and King13 and provide enough detail to identify mental health disorders without the need for a clinical assessment.
The present paper aims to describe the development, implementation and results of this questionnaire. We provide descriptive data on the numbers of UK Biobank participants meeting diagnostic criteria for specific disorders, and on the frequency of exposure to risk factors. We also evaluate the likely representativeness of respondents by comparing respondent sociodemographic characteristics to those of the UK population using census data, and by comparing self-reported mental disorder diagnosis with the Health Survey for England (HSE) data.Reference Bridges14 This will assist researchers considering or undertaking epidemiological research to evaluate the potential and power of using UK Biobank to look at mental health.
Method
Questionnaire development
A mental health research reference group formed of approximately 50 individuals (see Supplementary Appendix 1, available at https://doi.org/10.1192/bjo.2018.12) participated in discussions about a strategy for mental health phenotyping in UK Biobank, including a workshop in January 2015. From this, a smaller steering group was established and led the development of the MHQ. The group recommended that the MHQ should concentrate on depression, as it was likely to represent the greatest burden in the cohort, with some questions about other common disorders, including anxiety, alcohol misuse and addiction, plus risk factors for mental disorder not captured at participants' baseline assessment.
The intention was to create a composite questionnaire from previously existing and validated measures, taking into account participant acceptability (time, ease of use and ensuring questions were unlikely to offend), scope for collaborations with international studies (e.g. the Psychiatric Genomics Consortium) through making results comparable, and the need to balance depth and breadth of phenotyping. The basis of the questionnaire was the measurement of lifetime depressive disorder using the Composite International Diagnostic Interview Short Form (CIDI-SF),Reference Kessler, Andrews, Mroczek, Ustun and Wittchen15 modified to provide lifetime history, as used to identify cases and controls for some existing studies in the Psychiatric Genomics Consortium. The CIDI-SF uses a branching structure with screening questions and skip-rules to limit detailed questions to the relevant areas for each participant. Other measures were then added to this, as summarised in Supplementary Table SM1. Where the group were unable to find existing measures that fulfilled these criteria, questions were written or adapted, as indicated in SM1. These sections have not been externally validated, but the questions can be seen, along with the full questionnaire, on the UK Biobank website (http://biobank.ctsu.ox.ac.uk/crystal/refer.cgi?id=22) for researchers to evaluate how they wish to use them.
Testing and ethical approval
The use of branching questions in the MHQ means that those with established and multiple mental disorders have a longer, more detailed, questionnaire. To improve acceptability in this group, we worked with a patient advisory group at the National Institute of Health Research (NIHR) Biomedical Research Centre at the South London and Maudsley (SLaM) NHS Foundation Trust in designing the questionnaire and invitation.Reference Robotham, Wykes, Rose, Doughty, Strange and Neale16 We then piloted the questionnaire among an online cohort of 14 836 volunteers aged over 50 and living in the UK, who completed the questionnaire as part of signing up to take part in the Platform for Research Online to investigate Genetics and Cognition in Ageing (PROTECT).Reference Wesnes, Brooker, Ballard, McCambridge, Stenton and Corbett17 Of those who started the questionnaire, 98.8% completed it, taking a median time of 15 min. Some PROTECT participants commented that they wanted the opportunity to explain why they felt they had experienced symptoms of depression. In response to this, we added a question to the depression section on loss or bereavement, and a free-text box – neither were designed to change diagnostic algorithms, but may add to future analyses.
The questionnaire was approved as a substantial amendment to UK Biobank by the North West – Haydock Research Ethics Committee, 11/NW/0382.
Administration to UK Biobank participants
We incorporated the final MHQ into the UK Biobank web questionnaire platform and presented it to participants as an online questionnaire entitled ‘thoughts and feelings’. We sent participants who had agreed to email contact a hyperlink to their personalised questionnaire. The invitation explained the importance of collecting further information about mental health and emphasised that UK Biobank was unable to respond to concerns raised by the participant in the questionnaire, instead directing them to several sources of potential support. Participants could skip questions they preferred not to answer, and they could save answers to return to the questionnaire later. We sent reminder emails at 2 weeks and 4 months to those who had not started or had partially completed the questionnaire. The MHQ will continue to be available on the participant area of the UK Biobank website, and the annual postal newsletter contains an invitation to log on to the participant area and complete the MHQ, to reach those for whom no email contact was possible. Data from this questionnaire will therefore continue to accrue. The current numbers and aggregate data can be accessed from the public data showcase (http://biobank.ctsu.ox.ac.uk/crystal/label.cgi?id=136). More detail on the roll out and associated communications can be found on the UK Biobank website (http://biobank.ctsu.ox.ac.uk/crystal/refer.cgi?id=22).
Defining cases from the MHQ
Case definitions for the evaluation of the responses to the MHQ are detailed in Supplementary Appendix 2. They arose either from the instruments used in the MHQ or by consensus criteria agreed by the working committee who wrote the MHQ. Diagnostic criteria were evaluated for depression (major depressive disorder), hypomania or mania, generalised anxiety disorder, alcohol use disorder, and post-traumatic stress disorder (PTSD). Addiction to substances and/or behaviour was defined based on self-report alone. Unusual experiences (describing potential symptoms of psychosis) and self-harm were also defined as phenomena that are important for phenotyping, but not disorder specific. We combined outcomes to divide the cohort into five mood disorder groups, as shown in Supplementary Figure MD1.
Fulfilling the diagnostic criteria based on a self-report questionnaire did not allow us to rule out other psychiatric disorders, or psychological or situational factors that might better explain the symptoms and may have been elicited in a clinical evaluation. Therefore, we regarded any case classification arising from the MHQ as ‘likely’ rather than confirmed psychiatric disorder. The issue becomes particularly problematic for disorders that are less common in the population, such as bipolar affective disorder, where the literature shows that using questionnaires to screen the population may over-estimate prevalence.Reference Cerimele, Chwastiak, Dodson and Katon18 Therefore, although we reported the presence of hypomania/mania symptoms for the whole population, we only made the likely diagnosis of bipolar affective disorder in people with a history of depression, a sub-population where the prevalence of bipolar affective disorder is higher, and therefore screening questionnaires have better positive predictive values.Reference Carvalho, Takwoingi, Sales, Soczynska, Köhler and Freitas19
Analysis and data sharing
Data were supplied by UK Biobank on 8th August 2017 under application number 16577. We used R version 3.4.0 and MS Excel for analyses. We reported numbers and proportions within the sample and did not attempt to give population prevalence estimates. The large sample size meant that all 95% confidence intervals were less than 0.3 away from percentage proportions and are therefore not shown.
The data for tables can be found in online Supplementary materials. The code is available from Mendeley Data (http://dx.doi.org/10.17632/kv677c2th4.1). Raw data are available from UK Biobank subject to the usual access procedures (www.ukbiobank.ac.uk).
Role of the funding source
The questionnaire was developed and administered with UK Biobank funding. Individual authors were funded by their institutions and research grants as detailed below. No funding body influenced the study design or the writing of this article. M.H. had access to all data through a standard data sharing agreement (Material Transfer Agreement) with UK Biobank and had final responsibility for the decision to submit the article for publication.
Results
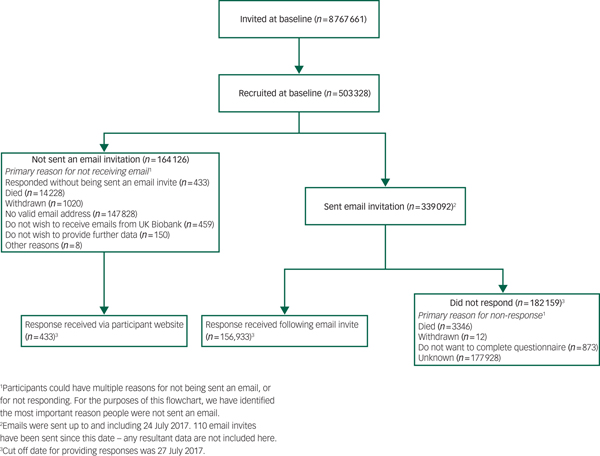
The setting, recruitment and methods of selection of participants in UK Biobank have been published elsewhere.Reference Sudlow, Gallacher, Allen, Beral, Burton and Danesh1, Reference Smith, Nicholl, Cullen, Martin, Ul-Haq and Evans9 For the MHQ study, 339 092 participants were sent an email invitation, and 157 366 (46% of those emailed) fully completed the questionnaire by August 2017 – which means that the MHQ currently has 31% coverage of the UK Biobank cohort. Figure 1 shows a flow chart of the UK Biobank participants who completed the MHQ. The median time for completion was 14 min, and 82% of respondents completed the questionnaire in under 25 min.
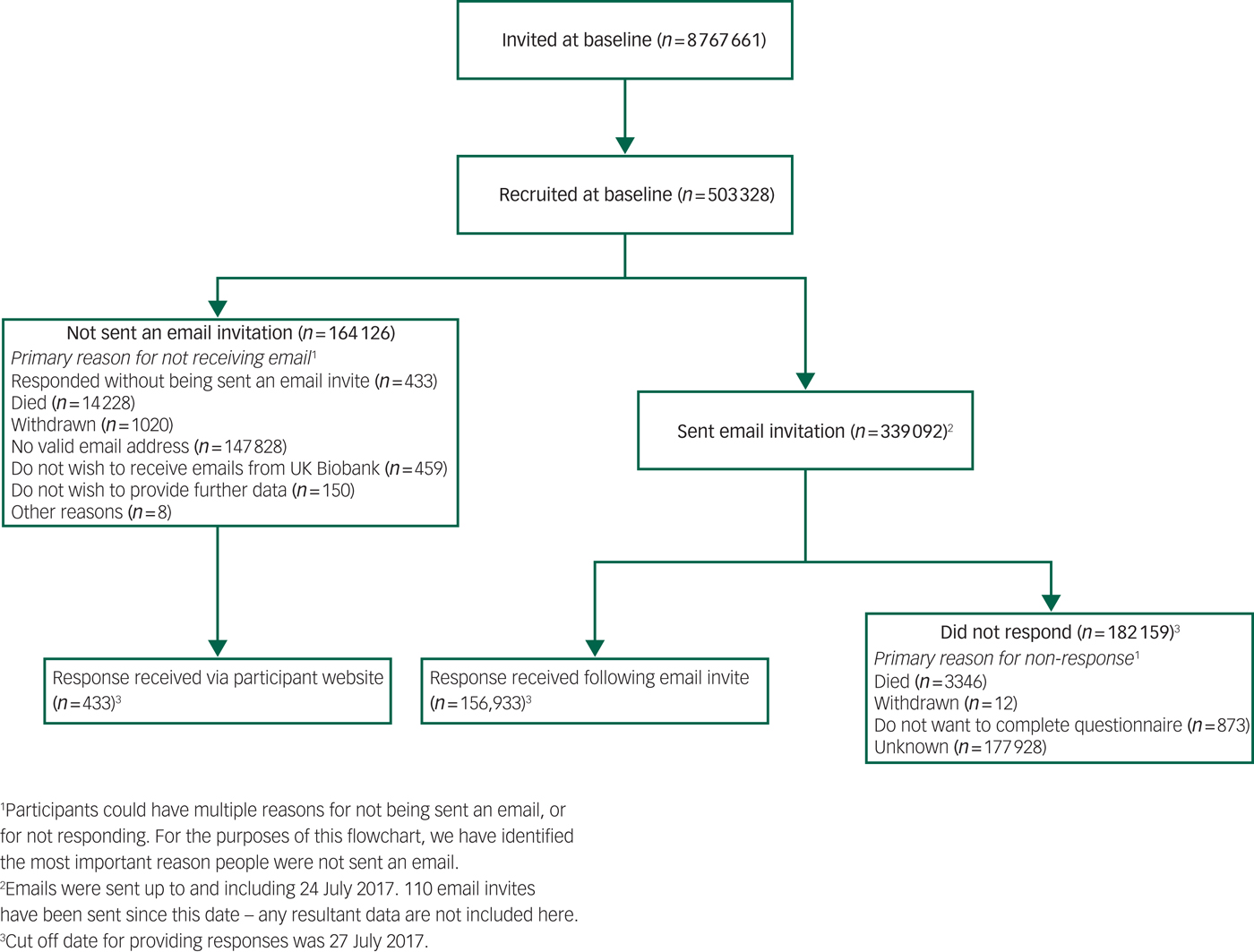
Fig. 1 Flowchart of UK Biobank participants from invitation to completion of mental health questionnaire. Invitations were based on NHS registration, age and location. Numbers correct for July 2017.
Supplementary Table SM2 shows participant characteristics for all UK Biobank participants and those who completed the MHQ, compared with population-level data for UK residents in the same age range. Participants were different from the whole UK Biobank cohort and the general population in that they were better educated (e.g. 45% held a degree v. 32% of UK Biobank participants v. 23% in the census), of higher socioeconomic status according to job type, and healthier (longstanding illness or disability 28% v. 32% v. 37%), with lower rates of current smoking.
As shown in Table 1, 34% of respondents reported they had received at least one psychiatric diagnosis from a professional at some time, and 12% had received two or more. The most commonly reported diagnosis was depression, followed by ‘anxiety or nerves’. Data were compared with the HSE, because this annual survey aims to report data that is a representative estimate for the population in England through its sample and weighting.Reference Craig, Fuller and Mindell20 The comparison shows that the pattern and prevalence of diagnosis is similar; for example, a depression diagnosis was self-reported by 21% of individuals in both samples, eating disorders by around 1%, and bipolar-related disorders by around 0.5%. The definition in the MHQ differed from that in the HSE for anxiety (MHQ definition was broader) and addiction (MHQ did not require professional diagnosis), and the higher overall prevalence in the UK Biobank MHQ compared with the HSE (35% v. 28%) may be due to those wider definitions.
Table 1 Self-reported previous physician diagnosisa (self-reported without physician diagnosis for addictionb)
NA, not reported.
a. UK Biobank participants were asked: ‘Have you been diagnosed with one or more of the following mental health problems by a professional, even if you don't have it currently? (tick all that apply): By professional we mean: any doctor, nurse or person with specialist training (such as a psychologist or therapist). Please include disorders even if you did not need treatment for them or if you did not agree with the diagnosis’. HSE participants were asked to identify all the mental health conditions they had experienced, then asked whether they had been told by a doctor, psychiatrist or professional that they had it.
b. UK Biobank participants were asked: ‘Have you been addicted to or dependent on one or more things, including substances (not cigarettes/coffee) or behaviours (such as gambling)?’ HSE definition of addiction includes physician diagnosis.
c. HSE participants were asked about generalised anxiety disorder, and not about anxiety and nerves more generically.
As shown in Table 2, 35% of participants met criteria for one or more operationally defined syndromes. The most common was lifetime depression at 24%, followed by anxiety disorder and alcohol use disorder (both 7%), PTSD (6%), unusual experiences (5%) and self-harm (4%). Hypomania/mania was the least common, for 2% of respondents. As shown in Supplementary Table SM3, women were more likely than men to have a history of one or more of the defined syndromes (39% v. 30%), particularly depression, anxiety or PTSD. Men were more likely than women to have an alcohol use disorder (10% v. 5%), and there was little difference in the rate of report of unusual experiences (both 5%). Table 2 also shows the substantial comorbidity of defined syndromes. Notably, around three-quarters of participants who met criteria for lifetime anxiety disorder also met criteria for lifetime depression, while individuals with PTSD had at least a two-fold increase in lifetime prevalence of all other syndromes. Alcohol use disorder appeared less related to the others.
Table 2 Comorbidity between operationally defined syndromes

Percentages refer to the proportion of participants with the row syndrome who also have column syndrome. See lettered table notes, and Supplementary Appendix 2 for case definitions. GAD, generalised anxiety disorder; PTSD, post-traumatic stress disorder.
a. Criteria met for major depressive disorder on CIDI-SF lifetime.
b. Criteria met for hypomania/mania lasting for at least one week.
c. Criteria met for generalised anxiety disorder on CIDI-SF lifetime.
d. Reported potential hallucination or delusion at any point in their life.
e. Reported deliberate self-harm at some point in their life, asked to report self-harm ‘whether or not you meant to end your life’.
f. Criteria met for moderate alcohol use disorder on AUDIT during the past year.
g. Criteria met for post-traumatic stress disorder on PCL-6 in the past month.
The proportion of respondents meeting criteria for the lifetime occurrence of at least one of depression, anxiety, unusual experiences and addiction varied according to age and gender (Fig. 2), from 16% in men over 75 years old to 42% in women aged 45–54 years. Respondents with any of these lifetime syndromes were more likely than those without to live in areas of higher deprivation, especially if they had bipolar disorder or reported addiction (Table 3). They were also more likely to have had adverse life events and to have met criteria for loneliness and, to a lesser extent, social isolation. They were more likely to have smoked cigarettes and/or used cannabis, and to have had a ‘longstanding illness’ at baseline (although the presence of a mental disorder may have been the illness to which the participants referred in some cases). Achieving recommended levels of physical activity did not appear to be associated with any of the syndromes.
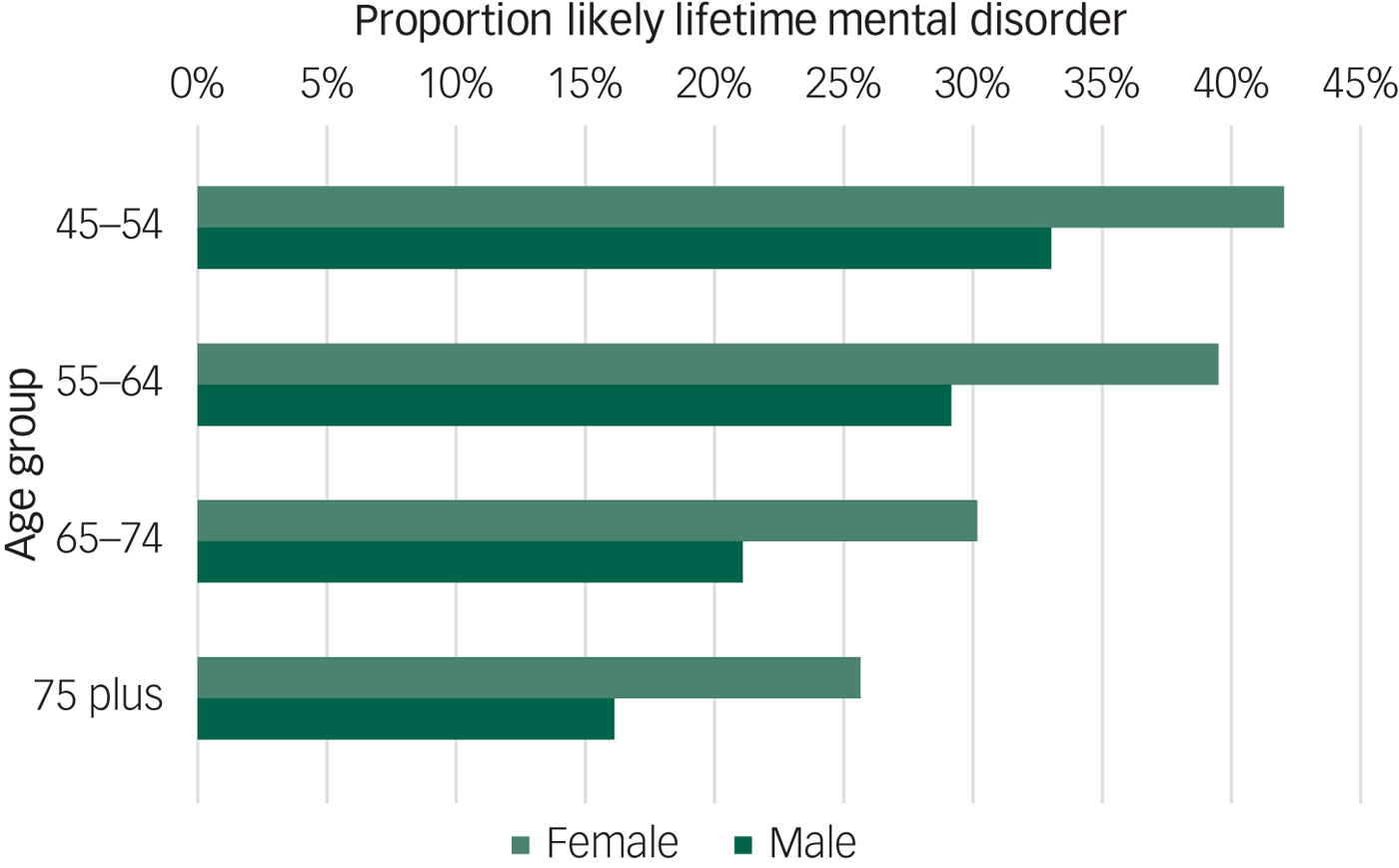
Fig. 2 Proportion of respondents positive for one or more of depression (and bipolar disorder), generalised anxiety disorder, unusual experiences and addiction according to lifetime diagnostic criteria. By age and gender.
Table 3 Socioeconomic factors by status for lifetime occurrence (people may be included in more than one category)
See lettered table notes, and Supplementary Appendix 2 for full case definitions.
a. Criteria not met for depression, GAD, unusual experiences or addiction.
b. Criteria met for disorder on CIDI-SF lifetime.
c. Criteria met for both lifetime depression and lifetime mania.
d. Reported potential hallucination or delusion at any point in their life.
e. Positively endorsed: ‘Have you been addicted to or dependent on one or more things, including substances (not cigarettes/coffee) or behaviours (such as gambling)?’
f. Age when mental health questionnaire released, derived from date of birth.
g. Townsend Material Deprivation Score is based on postcode areas.
h. Renting in the private sector and renting social housing combined.
i. From baseline assessment 2007–10.
j. Criteria met for possible abuse or neglect on Childhood Trauma Screener.
k. Criteria met for adverse situations as an adult: lack of confiding relationship, abusive relationships and money problems.
l. Reports one or more of six situations that are known to be triggers for trauma-related disorders.
m. There is some overlap between the adult screen and loneliness screen, which both ask about confiding relationships: adult screen includes lack of confiding relationship over the adult lifetime; loneliness includes lack of confiding relationship at the time of baseline assessment.
The Supplementary materials have a section on mood disorder, showing the results of analyses of MHQ participants by likely disorder categories (Supplementary Figure MD1). Supplementary Table MD1 shows the features of these groups. The characteristics of people who meet diagnostic criteria for depression appear to be shared by those with subthreshold depressive symptoms. Supplementary Table MD2 shows comorbidity, and demonstrates a gradient effect in the presence of a non-depression syndrome rising from 7% in no depression to 43% in recurrent depression. Supplementary Table MD3 shows an association between the presence of lifetime unipolar depression or bipolar affective disorder and worse scores for current mental health.
Discussion
This paper has described the development, implementation and principal descriptive findings from the UK Biobank MHQ. The implementation of this questionnaire demonstrates that a web-based questionnaire is an acceptable means of collecting mental health information at low cost and large scale. Although the data collection methods might result in more limited data acquisition than conventional interview methods, with associated uncertainties in true diagnostic categorisation, we suggest that the survey achieved an acceptable trade-off between depth of phenotypic information and scale of sample size.
The MHQ achieved a participation rate of 31% of the original UK Biobank participants and 46% of those emailed. This response rate is substantially higher than previous UK Biobank questionnaires, largely owing to the attention paid to ensuring the acceptability of the invitation and questionnaire and the efficient use of reminders. Those who completed the MHQ appeared to be better educated and to have higher socioeconomic employment status than those recruited into UK Biobank overall, and the UK population. Despite this, we found that rates of self-reported diagnoses were similar to population estimates from the HSE. The patterns of association between disorders and demographics were also broadly as predicted by previous research, which adds to the face validity of the questionnaire. For example, depression and anxiety were more common in women, while addiction and alcohol misuse were more common in men, and all disorders were less common in respondents older than 65 years. The decrease in prevalence of lifetime disorder with increasing age has been previously noted in cross-sectional studies, although the causes and implications are not clearly understood.Reference Streiner, Patten, Anthony and Cairney21, Reference Kessler, Birnbaum, Shahly, Bromet, Hwang and McLaughlin22
The ‘healthy volunteer’ selection bias within the UK Biobank has previously been explored.Reference Fry, Littlejohns, Sudlow, Doherty, Adamska and Sprosen23 The influence of selection biases on disease prevalence are likely to be particularly strong for mental disorders, where disorder status or symptoms may influence participation in research,Reference Knudsen, Hotopf, Skogen, Øverland and Mykletun24, Reference Atherton, Fuller, Shepherd, Strachan and Power25 and non-participation has also been associated with many risk factors for these disorders, including polygenic risk.Reference Martin, Tilling, Hubbard, Stergiakouli, Thapar and Davey Smith26 Therefore, the results of the MHQ should not be used to provide prevalence estimates. However, the pattern of the measured risk factors among the participants with mental disorders in the MHQ, including neuroticism, trauma, loneliness and housing tenure, was in accordance with established literature, supporting the use of the data to study the relationships between exposures and outcomes. Previous work on health surveys with selection bias due to non-participation, including UK Biobank, have indicated that although they can be used to give estimates of association,Reference Newson, Karlsson and Tiemeier11, Reference Knudsen, Hotopf, Skogen, Øverland and Mykletun24, Reference Macfarlane, Beasley, Smith, Jones and Macfarlane27 bias may occur in some cases.Reference Hernan, Hernandez-Diaz and Robins28, Reference Sperrin, Candlish, Badrick, Renehan and Buchan29 For example, the relative under-participation of unskilled workers in the MHQ (around 21% of that expected) could mask an association with a variable that was related to unskilled work.
Strengths and limitations
We developed a questionnaire through a consensus approach with clear aims of capturing enough data to characterise participants as having a lifetime history of depression and other phenotypes. Validated instruments were used where possible. The consortium working on the questionnaire included mental health researchers and members of the UK Biobank team working in collaboration to develop the optimum approach. The derived variables of likely categorical diagnoses will be added to the UK Biobank resource, facilitating those less familiar with mental health to use the results efficiently.
The ‘healthy volunteer’ effect may limit applications of the data. Owing to restrictions of time and space, the questionnaire was limited in the topics it could cover. The focus of the questionnaire was on categorical diagnoses rather than dimensional traits, which will tend to confirm conventional ICD/DSM nosology of psychiatric disorder and may not suit some research.Reference Lilienfeld and Treadway30 In particular, tools were chosen that are based on DSM-IV disorders, which reflects current practice (for example, National Institute for Health and Care Excellence guidelines on depression and anxiety use DSM-IV definitions).31, 32 Of the disorders with operational classification, all would generalise to DSM-5, except PTSD,33 and the concepts are valid for ICD-10 disorders, although the threshold of disorder may be different, e.g. depression is diagnosed with fewer symptoms in DSM than in ICD.31 The questionnaire was heavily reliant on participant report, which may be affected by the stigma of reporting psychiatric symptoms, and tends to underestimate lifetime prevalence through forgetting or re-evaluating distant events.Reference Newson, Karlsson and Tiemeier11, Reference Streiner, Patten, Anthony and Cairney21, Reference Nevin34 We hope that some of these shortcomings can be addressed in the future by a more fine-grained analysis of the MHQ data, supplemented with other data from UK Biobank to create a richer picture of mental health in the cohort.
Conclusions
UK Biobank offers a unique opportunity to research common disorders in a well-characterised longitudinal cohort of UK adults. A detailed MHQ has now been completed by 157 366 participants, including self-report, operationally defined lifetime disorder status, and detailed phenotype information on mood disorder. The proportion of cases and the patterns of participants experiencing symptoms and disorders was as expected, despite a ‘healthy volunteer’ selection bias. Future work on mental health phenotyping for UK Biobank will include validation of Hospital Episode Statistics for mental health diagnoses, validation of general practice records, and triangulation of health record and questionnaire data. Examples of existing projects utilising the UK Biobank MHQ can be seen in Supplementary Appendix 3, with a searchable database of approved research (http://www.ukbiobank.ac.uk/approved-research/).
This study also demonstrates the substantial burden of mental disorders. Given the known effects of mental health on physical health, mental health data should interest researchers from every biomedical specialty looking at associations with health and disease. This study suggests that UK Biobank could be a powerful tool for such studies, and, since it is open to all bona fide health researchers for work in the public good, we hope this study will inspire both existing and new users of UK Biobank.
Funding
This paper represents independent research funded by the NIHR Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King's College London. B.C. is funded by the Scottish Executive Chief Scientist Office (DTF/14/03). E.F. is supported by the European Research Council (ERC) under the European Union's Seventh Framework Programme (FP7/2007–2013)/ERC grant agreement no: [324176]. L.M.H. is supported by an NIHR Research Professorship (NIHR-RP-R3-12-011) in Women's Mental Health. W.L. is supported by the NIHR Collaboration for Leadership in Applied Health Research and Care South West Peninsula. D.J.S. is supported by the Lister Institute Prize Fellowship. S.Z. is supported by the NIHR Bristol Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, Department of Health, ERC, Scottish Government, UK Biobank or other funders or institutions.
Acknowledgements
We thank the staff and participants of UK Biobank, the PROTECT study and the SLaM Service Users Group for their participation.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2018.12.







 Open access
Open access
eLetters
No eLetters have been published for this article.