


Parents serve important functions in regulating children's responses to stress and challenge (Hostinar, Sullivan, & Gunnar, Reference Hostinar, Sullivan and Gunnar2014). For instance, children look to their parents for signals that the environment or a stimulus they are interacting with is safe to explore or potentially dangerous (Feinman & Lewis, Reference Feinman and Lewis1983; Gunnar & Stone, Reference Gunnar and Stone1984; Walle, Reschke, & Knothe, Reference Walle, Reschke and Knothe2017). Parents also socialize children's coping strategies, encouraging some more than others (Shipman & Zeman, Reference Shipman and Zeman2001). The sheer presence of a caregiver increases children's sense of control over their environment and over their emotional state (Stansbury & Gunnar, Reference Stansbury and Gunnar1994). In addition, social support received from a parent either in person or by telephone can significantly reduce children's endocrine responses to acute stress, a phenomenon that has been termed social buffering (Hostinar, Johnson, & Gunnar, Reference Hostinar, Johnson and Gunnar2015a; Seltzer, Ziegler, & Pollak, Reference Seltzer, Ziegler and Pollak2010).
Social Buffering of Children's Acute Stress Responses
The hypothalamic–pituitary–adrenal (HPA) axis has been implicated in social buffering effects in humans and in various mammalian species (Gunnar & Hostinar, Reference Gunnar and Hostinar2015; Hennessy, Kaiser, & Sachser, Reference Hennessy, Kaiser and Sachser2009). This evidence has shown that social partners can dampen the production of cortisol, a hormone secreted by the hypothalamic–pituitary–adrenal axis and a gene transcription factor impacting multiple aspects of neurobehavioral development (Gunnar, Doom, & Esposito, Reference Gunnar, Doom, Esposito and Lamb2015). Over time, parental buffering of children's physiological responses to acute events may accumulate to have chronic, lasting effects on children's diurnal cortisol output and neurobehavioral development (Flannery, Beauchamp, & Fisher, Reference Flannery, Beauchamp and Fisher2017). However, more research is needed to understand factors that may explain variation in the effectiveness of social buffering.
Some research has identified child characteristics that moderate the effectiveness of social buffering by parents. For example, children with prior experiences of early social deprivation (i.e., orphanage care) did not exhibit the same buffering effects by parent support as children born and raised in their birth families (Hostinar, Johnson, & Gunnar, Reference Hostinar, Johnson and Gunnar2015b). This was true even though observational ratings of the quality of parent support provided in the laboratory did not differ between the two groups, and neither did children's reports of perceived closeness with their parents and parental supportiveness (Gunnar, Reference Gunnar2017). In addition, pubertal stage has emerged as an important moderator, with the effectiveness of social buffering by parents being lower for youth in more advanced stages of puberty compared to pre-pubertal children (Doom, Hostinar, VanZomeren-Dohm, & Gunnar, Reference Doom, Hostinar, VanZomeren-Dohm and Gunnar2015; Hostinar et al., Reference Hostinar, Johnson and Gunnar2015a).
Parent Characteristics and the Effectiveness of Social Buffering
Fewer studies have examined characteristics of the parent–child relationship that promote effective social buffering. In studies with toddlers, attachment security was associated with stronger buffering of cortisol reactivity among temperamentally inhibited children (Nachmias, Gunnar, Mangelsdorf, Parritz, & Buss, Reference Nachmias, Gunnar, Mangelsdorf, Parritz and Buss1996). This study also revealed that parents can sometimes induce inhibition or anxiety-like behaviors. Nachmias and colleagues examined maternal involvement in a paradigm where mothers were instructed to be “noninvolved” or “involved” during presentation of a novel stimulus that might be potentially fear-inducing to the infant. Infants whose mothers were more highly involved and encouraged them to approach the novel stimulus showed more inhibition and greater cortisol reactivity. Mothers’ pressures to approach the novel stimulus were also associated with less positive coping of the infant. Similarly, in a sample of older children diagnosed with clinical anxiety, mothers interacting with anxious children showed more involvement and more negativity compared to mothers interacting with nonanxious children during a speech preparation task (Hudson, Doyle, & Gar, Reference Hudson, Doyle and Gar2009).
Another possibility is that the effectiveness of social buffering might be shaped by broad parental characteristics such as parental education and socioeconomic status (SES). There is limited evidence on the role of SES as a potential moderator of social buffering, and prior theories orient us towards competing predictions. On the one hand, the family stress model (Conger et al., Reference Conger, Conger, Elder, Lorenz, Simons and Whitbeck1992) integrates evidence that economic stress and financial pressures have negative consequences on family functioning and the parent-child relationship, increasing risk of child maladjustment and poor mental health (Conger et al., Reference Conger, Conger, Elder, Lorenz, Simons and Whitbeck1992; Mistry, Lowe, Benner, & Chien, Reference Mistry, Lowe, Benner and Chien2008). Children from low-SES families experience more harsh parenting, and their parents confront more stressors and have higher rates of psychopathology (Masarik & Conger, Reference Masarik and Conger2017; McLoyd, Reference McLoyd1998). On the other hand, a growing body of work indicates that equating low SES with poor parenting and high SES with good parenting is an inaccurate stereotype (Luthar & Latendresse, Reference Luthar and Latendresse2005b). Some studies report evidence that youth from affluent backgrounds can exhibit more internalizing problems, such as anxiety, compared to their lower-income counterparts (Luthar & Latendresse, Reference Luthar and Latendresse2005a; Luthar & D'Avanzo, Reference Luthar and D'Avanzo1999). It has been proposed that heightened anxiety may be due to lack of quality family time as a result of increased career and extra-curricular commitments (Becker & Luthar, Reference Becker and Luthar2002; Luthar, Reference Luthar2003; Luthar & D'Avanzo, Reference Luthar and D'Avanzo1999), and due to high-SES parents exerting high pressure towards academic achievement (Luthar & Becker, Reference Luthar and Becker2002).
To our knowledge, only one study has examined SES in relation to parental buffering of children's responses to acute stress (Johnson, Mliner, DePasquale, Troy, & Gunnar, Reference Johnson, Mliner, DePasquale, Troy and Gunnar2018). In this study, there was no overall main effect of SES on cortisol reactivity to inoculations among toddlers (Johnson et al., Reference Johnson, Mliner, DePasquale, Troy and Gunnar2018), suggesting comparable cortisol reactivity for low-SES and high-SES children. However, attachment security was more strongly associated with the effectiveness of social buffering among toddlers from high-poverty families compared to those from families that were well above the federal poverty limit (Johnson et al., Reference Johnson, Mliner, DePasquale, Troy and Gunnar2018). This suggests that a strong bond is particularly important for children in poverty. However, more research is needed on this question and in older children. The present study sought to shed light on this question by examining parental education as a moderator of social buffering effects.
Social Buffering and Children's Mental Health
To date, there is not a comprehensive understanding of how social buffering of stress may relate to children's mental health symptomatology, such as anxiety. In adults, there is evidence supporting the benefits of social support for concurrent and future mental health (Thoits, Reference Thoits2011; Wang, Mann, Lloyd-Evans, Ma, & Johnson, Reference Wang, Mann, Lloyd-Evans, Ma and Johnson2018). Less is known about this association in childhood.
One clue comes from a neuroimaging study conducted by Gee et al. (Reference Gee, Gabard-Durnam, Telzer, Humphreys, Goff, Shapiro and Tottenham2014), which found that mothers’ images suppressed children's amygdala reactivity and induced a more mature pattern of amygdala–prefrontal connectivity compared to images of strangers. There were links with mental health, as children who displayed negative coupling of the amygdala with the prefrontal cortex when presented with the maternal stimulus reported lower levels of separation anxiety than children who displayed a positive connection between the amygdala and prefrontal cortex. In addition, the presence of their mother led to increased regulation during an affect-related regulation task, such that the mother being present during the regulation task led to better performance. Specifically, the children made fewer mistakes related to the emotional stimulus (rather than performance overall). This suggests that maternal presence had an effect on affect-related regulation.
Given the limited evidence base, the current study aimed to further examine this important relation between parental social buffering and child mental health. Specifically, we aimed to examine the extent to which the effectiveness of parental buffering of cortisol reactivity was linked to child state and trait anxiety.
The Present Study
The present study had three aims: (a) first, we aimed to test the hypothesis that parents buffer children's cortisol stress responses between the ages of 9 and 11 years old, in line with prior work that this is an age range when we can expect effective parental buffering (Hostinar et al., Reference Hostinar, Johnson and Gunnar2015a). (b) Secondly, we aimed to examine parental characteristics that may explain variation in the effectiveness of parental buffering. We focused on parental education and specific parental behaviors in the laboratory. For parental education, a facet of SES, we did not have a directional hypothesis, given the competing theoretical models reviewed above. For specific parental behaviors towards the child coded from observed interactions (positive affect, negative affect, involvement, dominance, and validation), we hypothesized that more positive and responsive behaviors towards the child would predict lower cortisol reactivity in the parent condition – that is, more effective buffering. (c) Thirdly, we aimed to examine whether the effectiveness of parental buffering would be associated with children's symptoms of state and trait anxiety. Specifically, we hypothesized that weaker parental buffering (i.e., greater cortisol reactivity within the parent condition) would be associated with greater state and trait anxiety among children.
Method
Participants
We recruited 181 participants, with 180 providing at least one measure included in the present analyses. Detailed demographics are presented in Table 1. Children were 9 to 11 years old at their laboratory visit (M = 9.9 years, SD = .58 years; 50.6% male and 49.4% female at birth; current gender identification: 48.3% male, 50% female, and 1.7% other). Participants were screened to participate via a phone interview with a parent. Exclusion criteria included having a developmental disability, chronic health condition, not being able to speak or read English, having a speech or language disorder that would prohibit study activities, and currently taking psychotropic or steroid medication. In addition, parents were asked if their child had been ill in the past two weeks, and if so, study visits were scheduled two weeks after their child's symptoms subsided.
Table 1. Descriptive statistics for full sample.
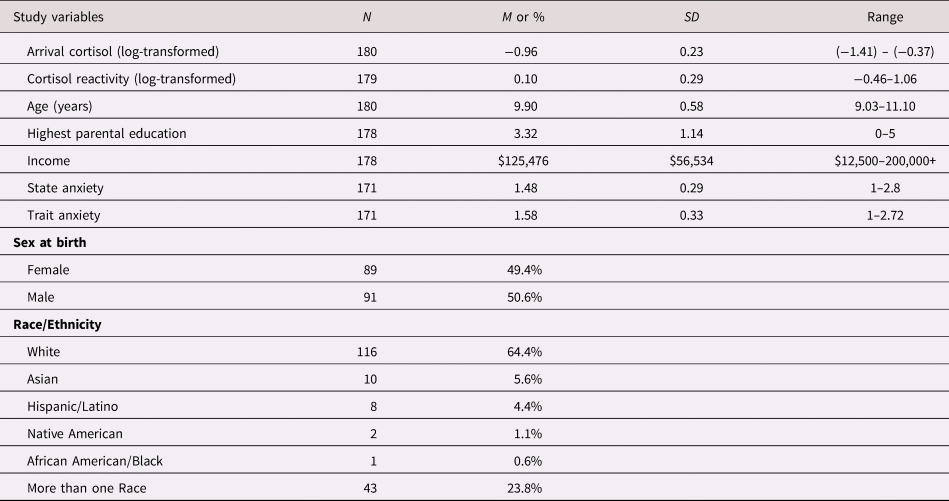
Demographic information was obtained via parent report. For race/ethnicity, 64.6% of children were White, 5.5% were Asian, 4.4% were Hispanic/Latino, 1.1% were Native American, 0.6% were Black/African American, and 23.8% were more than one race/ethnicity. Mean total annual household income was $125,476 (SD = $56,534), ranging from $12,500 to more than $200,000. Highest parental education level was the highest education level among the participant's parents that culminated in the obtainment of a degree, and was coded as a 6-level ordinal variable such that: 0 = less than high school (0.6% of sample), 1 = high school diploma or GED (7.8%), 2 = two-year or vocational degree (11.1%), 3 = four-year degree (34.4%), 4 = master's degree = 4 (30%), and 5 = doctoral/professional level degree (15%), with two unreported (1.1%).
Procedure
Participants attended one laboratory visit accompanied by a parent or legal guardian. All visits occurred in the afternoon, with a start time between the hours of 1:30 pm and 2:30 pm. After informed consent and informed assent were obtained from the parent and child respectively, the first saliva sample was collected (10 minutes after arrival). Saliva samples were collected at eight time points, every 20 minutes, throughout the session. This study was part of a larger investigation into social and emotional development that included additional biological measures (autonomic recordings, blood samples, one 30 minutes from arrival and one after the last saliva sample), and additional social and cognitive measures that were conducted after the acute stressor in an identical manner for all children across the three experimental conditions, thus they cannot explain condition effects and are beyond the scope of this analysis. Participants were randomly assigned to one of three experimental conditions (see description below). Following recruitment of 130 participants, careful monitoring of age bins and sex frequencies was implemented to ensure that the three conditions were balanced by sex and had nearly identical age distributions. This study was approved by the Institutional Review Board of the University of California-Davis and the State of California Committee for the Protection of Human Subjects.
Trier Social Stress Test – modified (TSST-M)
The TSST-M is a modified version of the Trier Social Stress Test (TSST) acute social stressor for adults (Kirschbaum, Pirke, & Hellhammer, Reference Kirschbaum, Pirke and Hellhammer1993). The TSST-M was specifically designed to elicit a mild stress response in children in this age range (Yim, Quas, Cahill, & Hayakawa, Reference Yim, Quas, Cahill and Hayakawa2010). The TSST-M procedure consisted of the following steps: participants were told that they had ten minutes to prepare a speech that would be evaluated by judges and recorded on camera to be later analyzed. For the topic of the speech, participants were asked to imagine that they were in a new classroom and a teacher has asked them to introduce themselves to the class (for details on this protocol, please see Yim et al., Reference Yim, Quas, Cahill and Hayakawa2010). After the 10-minute preparation period, participants were escorted to a novel room where there were two judges in white lab coats and a video camera (the judges were research assistants that remained hidden to participants prior to this point); the video camera was turned on in front of the participant; once the experimenter left the room, a judge asked the participant to begin the speech. The participant then engaged in a 5-minute speech followed by a 5-minute arithmetic subtraction task. Judges refrained from showing facial affect or providing feedback during the process, aside from informing children that they had more time if they paused during the speech and informing them when they gave an incorrect answer during the arithmetic task. Following the TSST-M, the participants completed additional questionnaires and provided four subsequent saliva samples every 20 minutes. At the very end of the laboratory visit, participants and their parents were debriefed regarding the nature of the TSST-M, by explaining why the judges had to remain neutral. The experimenter assured the child that they did a commendable job on the study tasks.
Experimental Conditions
Based on random assignment, half of the participants who were assigned to the TSST-M condition were assigned to prepare the speech with their parent (N = 59), whereas the other half were assigned to prepare for their speech alone (N = 60), with some participants (N = 61) being assigned to the control condition. The three conditions were balanced to be half male/half female, and they did not differ in mean age, F (1, 177) = .01, p = .99. Random assignment was implemented via a random number generator after each recruitment phone call, such that testing alternated randomly between conditions from one day to the next. Children and parents were not informed about their experimental condition until the beginning of the speech preparation period.
In the parent condition, parents were instructed to provide support to their children in a manner that they consider most natural using the following prompt: “Mom/dad, please feel free to provide support to your child in any way you find useful. Anything from helping with ideas for the speech to hugs is alright, so long as it is what feels natural for you.” The preparation period with the parent was video-recorded to be later analyzed. After providing the instructions for the preparation of the task, the experimenter left the room to allow the child and parent to prepare for the speech.
In the alone condition, the experimenter escorted the parent out of the room to allow the child to prepare alone for 10 minutes. After 10 minutes of preparation, participants in both the alone and parent conditions were escorted to a new room unaccompanied by the parent to complete the TSST-M.
Children randomly assigned to the control condition engaged in a placebo TSST-M that consisted of the following steps: participants were informed that they were part of a calm comparison group, and were asked to spend 10 minutes with their parent, thinking about their favorite book or movie, and writing down some ideas about the plot of the book or movie. Following this 10-minute period, participants were taken to a novel room where they engaged in five minutes of friendly conversation about the chosen book or movie with the experimenter, which would match the speaking demands of the TSST-M but exclude the elements of social evaluation since there were no judges present and the conversation was not video-recorded. To match the mental arithmetic component of the TSST-M, the participants were then asked to play a Sudoku game (level: easy) for five minutes; if a participant was unfamiliar with the game, it was explained to them. Participants were told that their performance on the Sudoku was not important and were given access to a sheet with hints and answers on it. The experimenter spent time tidying up the room during this part of the task, to prevent the participant from feeling watched and evaluated on their performance.
Measures
Salivary cortisol
Saliva samples were collected via the passive drool method every 20 minutes beginning 10 minutes after arrival at the laboratory until 60 minutes after the end of the TSST-M, for a total of eight samples (10, 30, 50, 70, 90, 110, 130, and 150 minutes from arrival). Saliva was stored in micro centrifuge tubes in a secure −80°C freezer until being shipped for assay. Samples were assayed at the Salimetrics’ SalivaLab (Carlsbad, CA) using the Salimetrics Salivary Cortisol Assay Kit (Cat. No. 1-3002), without modifications to the manufacturer's protocol. Samples were assayed in duplicate and averaged. Intra-assay coefficient of variation (CV) was excellent (4.6%), as was the inter-assay CV (6%). Complete salivary cortisol data were available for 179 participants, as one participant ended the study visit after completing the second saliva sample.
The current analysis focused on cortisol reactivity, which was indexed through change in cortisol from Sample 4 (taken directly before administration of the TSST-M or control condition) to Sample 6 (taken 20 minutes following the TSST-M or control condition). Sample 4 included three outliers (above 4 SD from the mean); Sample 6 included two outliers. Outliers were winsorized to the highest value within 4 SD from the mean. After winsorizing, all cortisol values were log-transformed to correct for positive skew. Cortisol reactivity was then calculated by subtracting Sample 4 from Sample 6, such that higher values represent greater increases in salivary cortisol from Sample 4 to Sample 6.
Parent support video coding
The preparation period before the TSST-M was video-recorded for later coding of social support behavior in the parent condition. Parental behavior towards the child focused on five dimensions, each receiving a score from 1 to 5: positive affect, negative affect, involvement, dominance, and validation (see Appendix 1 for coding instructions and examples of each behavior). Positive affect included facial expression, tone of voice, and body positioning that suggested a cheerful, supportive, or warm quality to the parent's interaction with the child. Negative affect included facial expression, tone of voice, and body positioning that suggested an unhappy or cold quality. Involvement refers to the level of engagement a parent showed toward the participant's task and was indexed through behaviors such as making suggestions, or asking questions. Dominance reflects the amount of control the parent takes over the task during the preparation period, and was indexed through behaviors such as interrupting the child, or commanding the child. Validation refers to a combination of affect and content cues that a parent utilizes to encourage, support, or comfort the participant and was indexed through behaviors such as acknowledging the participant's worry or stress, or showing support for the participant's ideas. Two trained research assistants who had not interacted with the parent during the research session and did not have access to cortisol data coded the videos. Parent support video data were missing for N = 5 participants due to technical error, resulting in available data for N = 54 participants. Of the 54 participants, 36 videos were double-coded and exhibited high inter-rater reliability. Intra-class correlation coefficients (ICC) were high: positive affect = .92; negative affect = .88; involvement = .96; dominance = .94; and validation = .81. Given these high inter-rater reliabilities, we averaged scores for participant videos that were double-coded. Factor analysis and scale reliability (Cronbach's α = .65) suggested these did not measure a single construct, thus we analyzed the five dimensions separately and corrected for multiple comparisons. In addition, we were interested in isolating specific dimensions of parental behavior that are linked to buffering cortisol reactivity.
State and trait anxiety
Participant's state and trait anxiety were measured using the State-Trait Anxiety Inventory for Children (STAIC; Spielberger, Reference Spielberger1973). The STAIC-trait is a 20-item scale with 3-point Likert-type items that assesses general levels of anxiety that the participant usually feels (reliability in this study was excellent: Cronbach's α = .84). The STAIC-state is a 20-item scale with 3-point Likert-type items asking how the participant currently feels (e.g., “How do you feel at this moment”) and was administered 30 minutes following the TSST-M or control condition (in this study, Cronbach's α = .89).
Data analysis plan
Statistical analyses were conducted using SPSS version 25. Due to the small amount of missingness (less than 5% on primary variables), analyses were conducted with all available data and missing value imputation was not necessary.
For the first aim of testing differences in cortisol reactivity by condition, we conducted a one-way analysis of covariance (ANCOVA) with condition as a fixed effect, controlling for participant age and sex (analyses of variance without covariates are also presented). Bonferroni corrections were employed for post hoc comparisons. For the second aim of examining parental characteristics that may moderate the effectiveness of buffering, we first examined the moderating effect of parent education by conducting another ANCOVA with two fixed factors and their interaction, condition and parent education (a two-level variable coded as 0 = less than college and 1 = college or more). These analyses also controlled for age and sex, but unadjusted analyses are also presented. In addition, we computed bivariate correlations of cortisol reactivity within the parent condition with the five dimensions of parental behavior in the laboratory as coded from video by observers. These measures were extracted based on the speech preparation period with the parent, thus they could only be examined within the parent condition. Finally, for our third aim focusing on possible ramifications of parental buffering for children's mental health symptoms, we examined if cortisol reactivity in the parent condition was associated with children's reports of state and trait anxiety.
Results
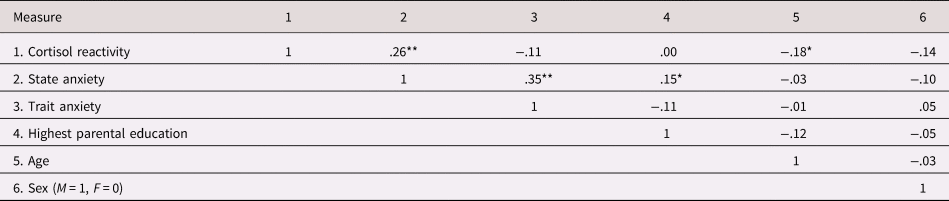
Descriptive statistics for main study variables appear in Table 1, and bivariate correlations in the full sample appear in Table 2. Across all participants, cortisol reactivity was positively associated with state anxiety, r(169) = .26, p = .001, and state anxiety was positively correlated with trait anxiety, r(169) = .35, p < .001. Higher parental education was significantly associated with greater state anxiety, r(169) = .15, p = .048, but not significantly associated with trait anxiety, r(169) = −.11, p = .16.
Table 2. Bivariate correlations among primary measures in the full sample. *p < .05. **p < .01.
Did parents buffer cortisol reactivity to acute stress?
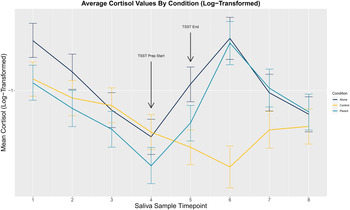
For our first aim, analysis of variance revealed a significant main effect of condition on cortisol reactivity, F(1, 176) = 19.14, p < .001. This main effect remained significant when adjusting for age and sex, F(2, 174) = 19.85, p < .001. Post hoc comparisons using Bonferroni correction indicated a significantly higher cortisol reactivity in the alone condition (M = 0.17, SE = .03) compared to the control condition (M = −0.06, SE = .03; p < .001), and higher reactivity in the parent condition (M = 0.21, SE = .03) compared to the control condition (p < .001). The means for the parent and alone conditions did not differ from each other, p = .99. Figure 1 illustrates these findings that cortisol reactivity (increase from Sample 4 to Sample 6) was similar for the parent and alone conditions, and they were both higher than the control condition. Results also revealed greater cortisol reactivity in females compared to males, F(1, 174) = 4.46, p = .036, and a significant negative relation between participant age and cortisol reactivity, F(1, 174) = 7.4, p = .007.
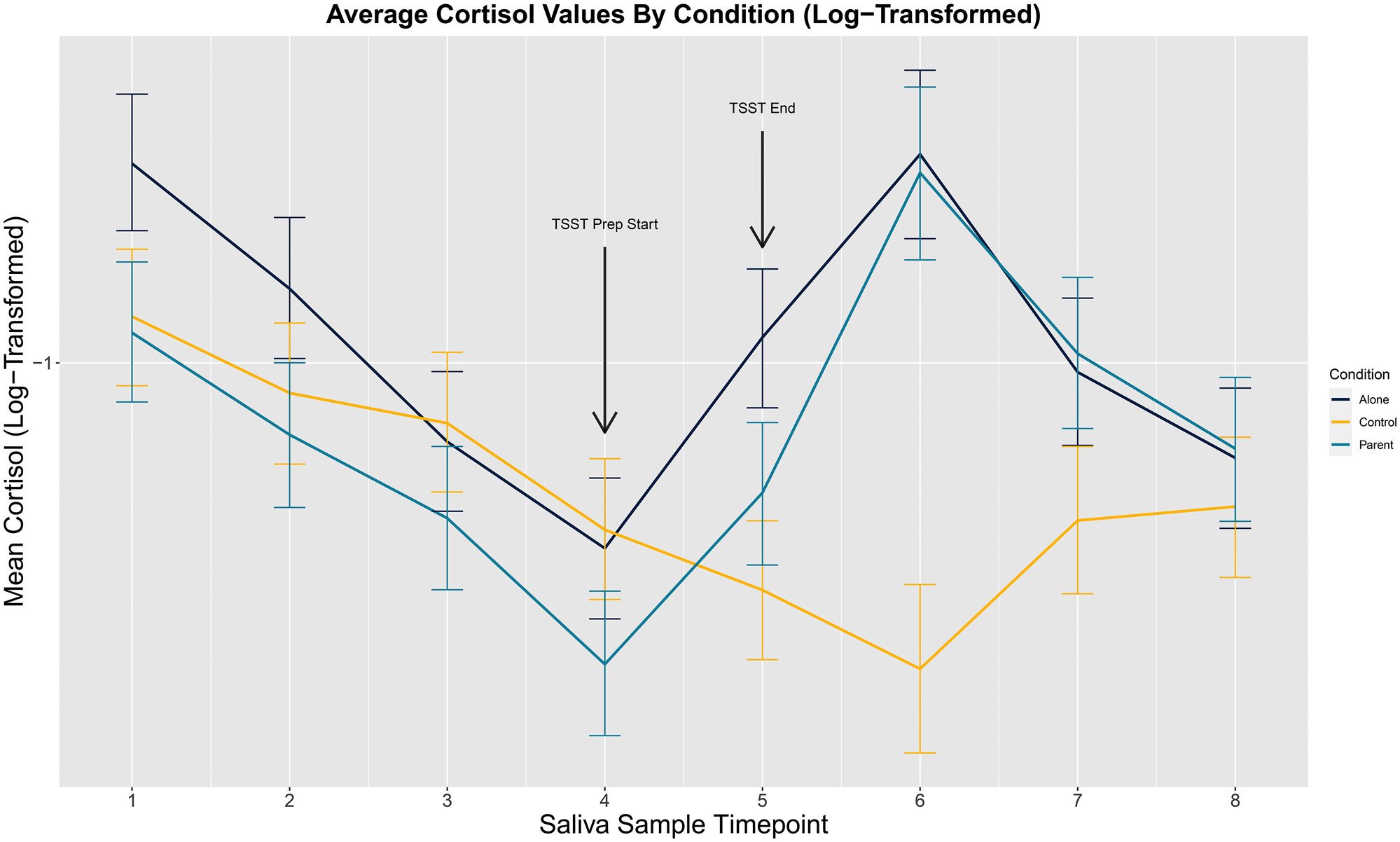
Figure 1. Average cortisol trajectories by condition. The first salivary cortisol sample was collected 10 minutes from arrival, after the consent process. Saliva samples were spaced 20 minutes apart. In total, 179 children provided saliva samples for cortisol assay.
Parental characteristics and buffering of stress responses
To examine the parental characteristics that may explain variation in the effectiveness of parental buffering, we tested whether the effect of condition was moderated by highest parental education level (two levels, less than a 4-year degree vs a 4-year degree or more). Analyses of variance revealed a significant interaction between parental education level and condition in predicting cortisol reactivity, F(2, 171) = 4.69, p = .01, which remained significant when adjusting for age and sex, F(2, 169) = 3.93, p = .02. In this adjusted analysis, the main effect of condition was significant, F(2, 169) = 9.45, p < .001, whereas the main effect of parent education was not significant on its own, F(1, 169) = .03, p = .86. Post hoc comparisons (illustrated in Figure 2) revealed that for children of parents with less than a 4-year degree, cortisol reactivity was significantly lower in the parent condition (M = .08, SE = .07) relative to the alone condition (M = .26, SE = .08), as indicated by the fact that the mean for the parent condition was lower and outside the 95% confidence interval (CI) for the alone condition (CI = .10, .42). The parent condition was not significantly different from the control condition (M = .01, SE = .08, CI = [−.14, .16]) for children whose highest parental education was less than a 4-year degree. Among children whose parents had a 4-year degree or more, children had significantly higher cortisol reactivity in the parent condition (M = .25, SE = .04, CI = [.18, .33]) compared to the alone condition (M = .15, SE = .04, CI = [.08, .22] and the control condition (M = −.08, SE = .04, CI = [−.16, −.01]), as indicated by the higher mean in the parent condition which was outside the 95% CI for both the alone and the control conditions (see Figure 2).
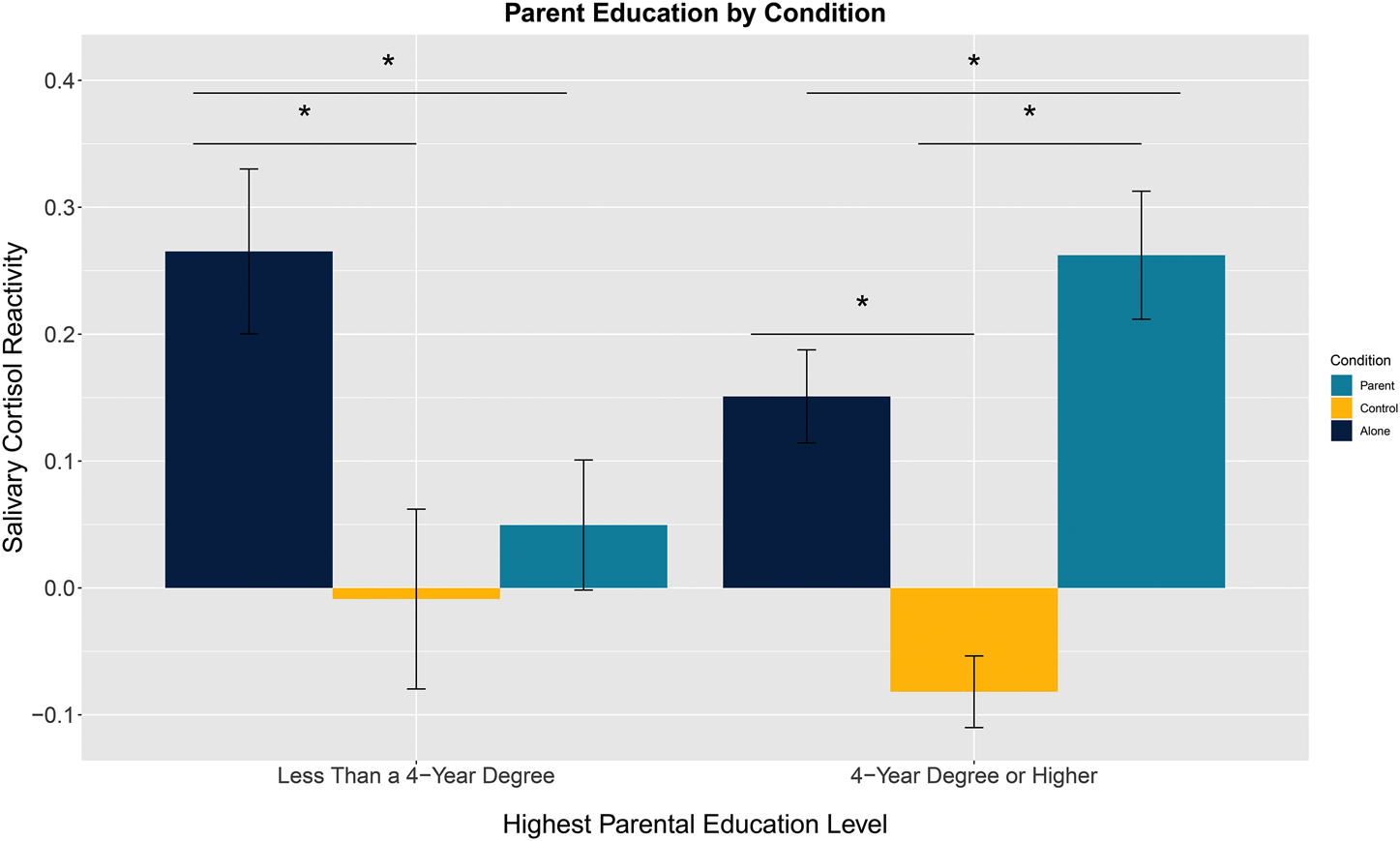
Figure 2. Interaction effect of parental education level by condition. Error bars are standard errors (SE). Means are marginal means from the analysis of covariance (ANCOVA) results, adjusting for age and sex.
To further investigate the role of parental behaviors in shaping cortisol reactivity within the parent condition, we computed bivariate correlations within the parent condition. Results revealed no significant association between the five dimensions of parent behavior coded by observers from videotapes and cortisol reactivity (p's > .09).
Given the significant interaction between parental education and condition, we conducted post hoc exploratory analyses to test whether parental education was associated with differences in parental behaviors during speech preparation as coded by observers. Parent education was not significantly correlated with any of the video-coded dimensions (p's > .08).
Parental buffering and children's anxiety
Correlates of state anxiety
Within the parent condition, state anxiety was positively associated with higher cortisol reactivity, r(51) = .30, p = .03, and with higher parental education, r(51) = .29, p = .04. These associations are illustrated in the two scatterplots in Figure 3. State anxiety was not significantly associated with any of the five video-coded parenting dimensions (p's > .35).
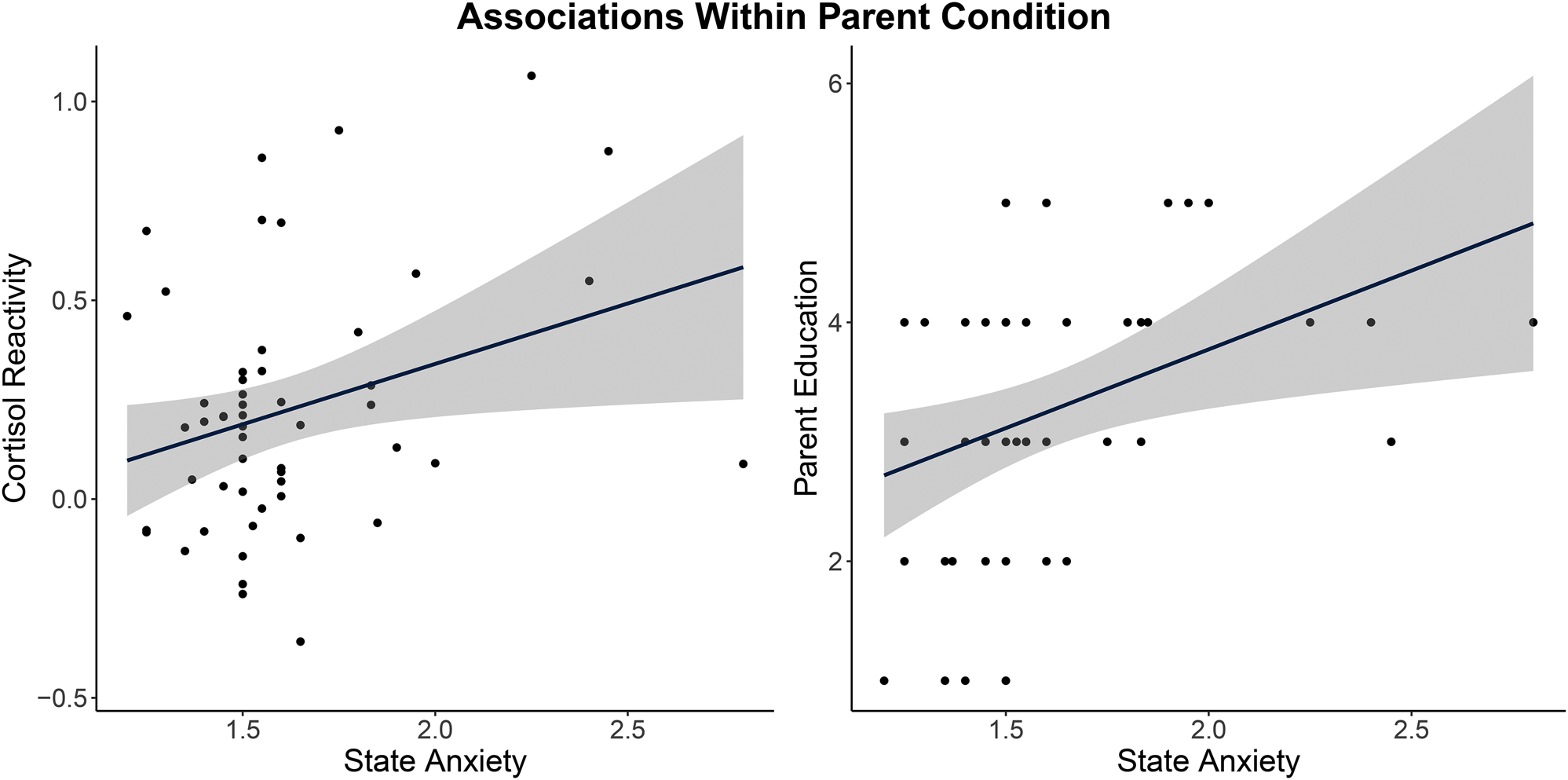
Figure 3. Associations of state anxiety with cortisol reactivity and parent education within the parent condition. Solid lines represent linear regression fit lines, with gray shading illustrating the 95% confidence interval.
Correlates of trait anxiety
Within the parent condition, trait anxiety was associated with cortisol reactivity, r(52) = −.32, p = .02, but was not associated with parental education, r(52) = −.11, p = .44. Trait anxiety was significantly correlated with the video-coded measures of parental behavior, such that children reported higher levels of trait anxiety if observers rated their parents to display more negative affect towards the child, r(48) = .33 p = .02, and less validation of children's ideas during the videotaped speech preparation, r(48) = −.32, p = .03. However, these associations did not survive correction for multiple comparisons (corrected threshold for significance p = .01). The remaining three dimensions of video-coded behaviors were not associated with trait anxiety (p's > .17).
Discussion
The three aims of this experimental study were to test the effect of parental buffering on children's stress reactivity, examine parental characteristics associated with effective buffering, and probe links with child state and trait anxiety. Understanding these processes is a critical foundation for exploring long-term implications of social buffering for children's neurobehavioral development (Gunnar, Frenn, Wewerka, & Van Ryzin, Reference Gunnar, Frenn, Wewerka and Van Ryzin2009; Gunnar & Vazquez, Reference Gunnar and Vazquez2006; Gunnar, Wewerka, Frenn, Long, & Griggs, Reference Gunnar, Wewerka, Frenn, Long and Griggs2009; Hostinar, Reference Hostinar2015).
For our first aim, results revealed that children exposed to the TSST-M exhibited greater cortisol reactivity compared to controls, as expected. Preparing with the parent did not buffer/reduce cortisol reactivity on average relative to preparing alone, which was surprising in light of buffering effects previously demonstrated in this age group (Hostinar et al., Reference Hostinar, Johnson and Gunnar2015a; Reference Hostinar, Johnson and Gunnar2015b). Methodological differences relative to prior studies and moderators of buffering effects may explain this finding. Methodologically, the use of live adult judges in the current protocol may have produced a more potent stressor than audio recordings of “judges” that children believed to be listening behind a one-way mirror in previous studies (Hostinar et al., Reference Hostinar, Johnson and Gunnar2015a, Reference Hostinar, Johnson and Gunnar2015b). In addition, parent support provided before a stressor in the current protocol may be less potent in buffering against subsequent stressors compared to parent support provided immediately after the TSST during recovery, as implemented in a study with 7–12-year-old girls (Seltzer et al., Reference Seltzer, Ziegler and Pollak2010). Further, it has been proposed (Gunnar, Reference Gunnar2017) that social-evaluative stressors (such as the TSST-M) may be more difficult to buffer relative to other types of stressors, due to the potential for social partners to inadvertently increase social-evaluative threat, even when they are instructed to provide support. Future research should explore other types of stressors to test these ideas.
The main effect of condition needs to be interpreted in light of a significant interaction with highest parental educational level. Specifically, we observed that children whose parents had less than a 4-year college degree exhibited a buffered profile, with cortisol reactivity in the parent condition that was comparable to the control condition and lower than the alone condition. In contrast, children whose parents had a 4-year college degree or graduate degree exhibited higher cortisol reactivity compared to children in the alone and control conditions. Cortisol reactivity within the parent condition was correlated with higher levels of state anxiety, suggesting that parents may have amplified children's emotional and cortisol responses to the public speaking task. These intriguing findings may be explained by differences in the type of parental support provided by highly educated parents, who may emphasize performance over comfort. Although some studies have reported more parental warmth in high-SES parents (Hoff, Laursen & Tardif, Reference Hoff, Laursen, Tardif and Bornstein2002), a large study of pre-adolescent children found comparable levels of parent physical and emotional unavailability among the lowest and highest SES families (Luthar & Latendresse, Reference Luthar and Latendresse2005b).
Because our video-coded parenting dimensions were not significantly associated with either cortisol reactivity or parental educational level, we can only speculate about the mechanisms by which highly educated parents might amplify children's state anxiety and cortisol reactivity. Explanations may involve processes of social referencing, stress contagion, and/or performance pressure. Social referencing has been demonstrated in many studies, and refers to a phenomenon during ambiguous or novel situations when infants and children look to parents for cues that signal whether the environment is safe or threatening (Aktar, Majdandžić, de Vente, & Bögels, Reference Aktar, Majdandžić, de Vente and Bögels2013; Boccia & Campos, Reference Boccia and Campos1989; Feinman & Lewis, Reference Feinman and Lewis1983; Gunnar & Stone, Reference Gunnar and Stone1984; Parritz, Mangelsdorf, & Gunnar, Reference Parritz, Mangelsdorf and Gunnar1992; Sorce, Emde, Campos, & Klinnert, Reference Sorce, Emde, Campos and Klinnert1985; van Rooij et al., Reference van Rooij, Cross, Stevens, Vance, Kim, Bradley and Jovanovic2017; Walden & Ogan, Reference Walden and Ogan1988; Walle et al., Reference Walle, Reschke and Knothe2017). If parents with a college degree, visiting a University laboratory, appraised the upcoming public speaking task as a potential threat, this may have informed children's behavioral and physiological response to the environment. It is unclear if this was explicitly conveyed to children verbally, or through the more implicit process of stress contagion. As an example of stress contagion, one study with infants (Waters, West, & Mendes, Reference Waters, West and Mendes2014) showed that infants exhibited higher heart rate reactivity when interacting with their mother if their mother had previously completed a negative social-evaluative stressor in a different room, separate from the infant (Waters et al., Reference Waters, West and Mendes2014). This demonstrates that dyadic interactions can establish physiological covariation or synchrony among social partners even in the absence of explicit verbal transmission. We did not have measures of parent state or trait anxiety, thus we could not test whether anxious parents increase their children's anxiety, though this would be consistent with prior evidence (Barrett, Rapee, Dadds, & Ryan, Reference Barrett, Rapee, Dadds and Ryan1996). In addition, an important future direction regarding social buffering of stress is to consider a two-generation perspective (Gunnar, Reference Gunnar2017). For example, we must consider the life histories and early experiences of parents that may relate to the way in which they form relationships and bond with their own children. Although we do not have these data in the present study, we aim to examine parents’ own mental health and early experiences in future studies. Finally, another possible explanation is that highly educated parents may have engaged in more performance-oriented coaching during the preparation period, focusing on strategies to help the child perform well. Previous research has documented increased performance pressure from parents among higher SES children (Luthar & D'Avanzo, Reference Luthar and D'Avanzo1999). Parents who themselves are highly successful in the educational domain can have high expectations for their children's success (Koplewicz, Gurian, & Williams, Reference Koplewicz, Gurian and Williams2009), which can lead to greater distress in the face of real or imagined failure among affluent youths (Luthar & Becker, Reference Luthar and Becker2002). Highly educated parents in the current study may have conveyed, either explicitly or implicitly, that this task was important and therefore that the child's performance on the task was important. When these children were subsequently faced with the neutral facial expressions and unexpected lack of positive feedback from the TSST-M judges, they may have found this perceived failure to be more stressful. Our coding of videotaped parental behavior focused on capturing parental sensitivity, and the measures were not designed to focus on parental attitudes towards performance or how important they consider it to be to perform well on this task. However, our future research directions include designing an observational coding scheme that can better detect these more subtle differences in involvement styles and track verbal comments about the importance of performing well during the subsequent public speaking task. It is also possible that highly educated parents are more intrusive during the speech preparation period, increasing their child's physiological arousal. As foundational work by Gunnar and colleagues has revealed, toddlers exhibited greater cortisol reactivity if their mothers encouraged them to approach an arousing stimulus more often. This overemphasis on approaching a novel event or stimulus may be “intrusive” and disrupt children's own efforts to regulate (Nachmias et al., Reference Nachmias, Gunnar, Mangelsdorf, Parritz and Buss1996).
Interestingly, parental education was not associated with trait anxiety, which could suggest that the amplification of child anxiety and cortisol responses may be restricted to public performance situations and may not have harmful long-term consequences for child mental health. Alternatively, the effects of repeated instances of high pressure to perform well may take longer to become crystallized into traits. Consistent with this possibility, some studies have reported higher rates of internalizing symptoms and substance use among adolescents from high-SES homes compared to low-SES homes, and this was linked to achievement pressure from their parents (Luthar & Becker, Reference Luthar and Becker2002). More longitudinal studies will be needed to test these long-term scenarios. Nevertheless, we found some interesting trends that video-coded parental behavior was associated with child trait anxiety. Parents who displayed more negative affect towards their child and lower levels of validation according to observers had children who reported higher levels of trait anxiety. Although these associations did not survive correction for multiple comparisons, the trends are consistent with prior research reporting higher parental negativity during interactions with anxious children (Hudson et al., Reference Hudson, Doyle and Gar2009).
In sum, this study documents important moderating effects of parent characteristics on parental buffering of children's cortisol reactivity. As such, the current study provides important novel contributions to a more nuanced understanding of when children most benefit from parental support. However, some limitations warrant attention in order to guide future research directions. First, this study is limited by the relatively high-SES sample. Although our sample is representative of the local community population, it is possible that our findings may not generalize to other geographical regions. Future research could benefit from replicating these findings with a nationally representative sample. Lastly, the effects of higher parental education on cortisol reactivity are correlational. We can therefore only speculate about the causal mechanisms underlying the heightened anxiety and cortisol responses for children of highly educated parents. The parental support instructions for the current study were naturalistic, allowing the parent to provide the type of support that felt natural to them, which increases the ecological validity of our results. Future studies should experimentally manipulate the style of parental support provided, for example, by randomly assigning some parents to a performance-oriented condition and some to an emotional-support condition, in order to provide causal evidence.
Despite these limitations, the current study has several strengths. We used an experimental design, with a relatively large sample that was balanced by age and sex. Importantly, this relatively large sample allowed us to test potential moderators of the parental buffering effect, yielding novel insights. Finally, despite the difficulties associated with psychobiological research in pediatric samples, rigorous data collection methods resulted in minimal missing data.
Conclusions
We found that parents with higher education amplified and parents with lower education reduced children's cortisol responses to an acute laboratory stressor. We found that buffering was effective for some, but not all, children in our sample. This pattern has been found in some prior studies, as attachment, temperament, puberty as well as other characteristics have been found to impact the stress response and effectiveness of social buffering in children (Gunnar, Brodersen, Nachmias, Buss, & Rigatuso, Reference Gunnar, Brodersen, Nachmias, Buss and Rigatuso1996; Gunnar, DePasquale, Reid, & Donzella, Reference Gunnar, DePasquale, Reid and Donzella2019; Hostinar et al., Reference Hostinar, Johnson and Gunnar2015a; Nachmias et al., Reference Nachmias, Gunnar, Mangelsdorf, Parritz and Buss1996). High-education parents may emphasize performance over comfort, with potential long-term ramifications for child mental health. Although parental education was only associated with higher state anxiety and not linked with trait anxiety in this study, evidence from some studies with older adolescents revealed higher levels of internalizing and substance use among high-SES youth, which was linked to achievement pressure (Luthar & Becker, Reference Luthar and Becker2002).
As illustrated in this special section and throughout Megan Gunnar's exemplary research program and public advocacy efforts (Gunnar, Reference Gunnar2017), a comprehensive understanding of when and how parents can reduce or amplify children's state and trait anxiety and physiological reactions to threat has the potential to inform public health policy, with practical implications for both normative contexts (e.g., academic examinations) and more extreme circumstances (e.g., refugee populations, natural disasters). In addition, understanding which parental behaviors lead to the best outcomes under duress provides important potential avenues for intervention.
Financial Statement
Dr. Hostinar's effort on this manuscript was supported by NIH award R01HD093898.
Conflicts of Interest
None
Appendix
Appendix 1. Coding scheme for parental behavior during speech preparation period.
Videos should be coded for 1-minute clips by stopping the video after each minute to assign ratings for each behavior. After watching each clip, the coder should assign a score under each behavior. It will be necessary to watch each clip multiple times in order to code for all five behaviors. After the entire video has been coded in segments, the segment scores will be averaged to assign one score for the entire video for each element. Codes from 1 to 5 will be assigned as follows (do not give half-points such as 2.5):
1: the parent did not display any of the cues described for that behavior, or the parent displayed the cues described specifically under the “low” qualification for that element.
2: the parent may have displayed two or three of the cues described for the element, but the cues were not present for the majority of the clip, or only one cue was displayed for the entirety of the clip.
3: about half of the cues described were displayed at some point during the clip and for the majority of the clip at least one cue was displayed, or three or more of the cues were displayed for the entirety of the clip.
4: a majority of the cues were displayed for extended amounts of time throughout the clip, but some may not have been displayed or may have faltered throughout the clip.
5: all of the cues in the description of the behavior were displayed for the majority of the clip, and no opposing cues were displayed during the clip.
Positive affect
Positive affect displayed by the parent includes physical cues including facial expression, tone of voice, and body positioning that suggest a cheerful, supportive, or warm quality. Positive affect may include facial expressions such as smiling, strong eye contact, and empathetic expressions that reflect what the participant is feeling. Body positioning may include sitting in an open manner, with the body oriented toward the participant, nodding, and a generally relaxed position. Tone of voice should be affectionate, warm, or satisfied. Other vocal cues may include joking and laughter (excluding nervous laughter or laughter at the participant's expense). Positive affect should be measured as a combination of all three cues, so that a parent who scores high in positive affect displays positive facial expressions, tone of voice, and body positioning. A low score on positive affect can mean either neutral or negative affect.
Low Positive Affect High Positive Affect
Parent is not smiling, Parent smiles, makes
maintains neutral or jokes, laughs with
negative face, body participant, tone is
body is not oriented warm, body posture is
toward participant. open.
1 2 3 4 5
Negative affect
Negative affect in the parent includes physical cues including facial expression, tone of voice, and body positioning that suggest an unhappy or cold quality. Negative affect may include facial expressions such as frowning, scowling, or furrowed brows. Avoiding eye contact may suggest a negative affect. Negative affect body language includes body orientation pointing away from the participant, or closed off positions, particularly with body directed away from participant. Crossed arms or legs should be considered as negative affect if the body is crossed away from the participant. Tone of voice may be irritated, frustrated, or cold. Negative affect should be measured as a combination of all three cues, so that a parent who scores high in negative affect displays negative facial expressions, tone of voice, and body positioning. A low negative affect score could be due to the presence of either neutral or positive affect.
Two is rare, three is infrequent, four is frequent, five is persistent
Low Negative Affect Two or three cues High Negative Affect
Parent is not scowling Parent is scowling,
or frowning, does not frowning, body is
express frustration or oriented explicitly
irritation toward participant. away from participant.
1 2 3 4 5
Involvement
Involvement refers to the level of engagement a parent shows toward the participant's task. A high-involvement parent is engaged, helpful, makes suggestions, asks questions, or helps the participant practice their speech while staying focused on the task at hand. Interrupting may be considered a form of involvement if it occurs in a way that appears to engage in the task rather than distract from it. A low-involvement parent may allow the participant to work on their own while completing paperwork, or may actively distract the participant through engaging in task avoidance, such as talking about things other than the task. If a significant amount of time (more than 30 seconds) is spent discussing something other than the task, the parent should receive a one-point reduction to their score, regardless of their level of involvement for the remainder of the clip. Involvement can be helpful or unhelpful from the child's perspective. What counts for this code is not perceived helpfulness but rather the amount of parental participation in helping the child with this task.
Low Involvement High Involvement
Parent is not engaged Parent is engaged in
in task, may initiate or task, encourages
participate in off-topic productivity, makes
discussion, does not provide help. suggestions.
1 2 3 4 5
Dominance
Dominance refers to the control taken by the parent during the preparation period. A high-dominance parent gives strict directions or instructions, uses a forceful tone of voice, interrupts the participant (note that not all interruption is dominating by nature, interruptions should be considered for their content and intent), commands the participant, takes notes or writes speech for the participant rather than allowing them to take notes on their own, or talks significantly more than the participant. When a parent is dominating, communication will appear one-sided or forced. Dominance can be scored high even if the child does not appear upset by it. A low-dominance parent is collaborative, asks open ended questions, attempts to work alongside the participant, and the preparation is mostly led by the participant, with a focus on what the participant would like to discuss.
Low Dominance High Dominance
Parent allows participant Parent takes control
to lead discussion, work of discussion, gives
is collaborative and strict instructions or
cooperative, promotes commands, talks
participant's autonomy. significantly more
than child.
1 2 3 4 5
Validation
Validation refers to a combination of affect and content cues that a parent utilizes to encourage, support, or comfort the participant. Validative affect includes positive or empathetic facial expressions, affectionate or warm tone of voice, and relaxed, open body positioning. Parent should be reactive through expression and body positioning (nodding, laughing). A high-validation parent will show support for the participant's ideas, feelings, or concerns, summarize or repeat participant's words, and compliment or flatter the participant. Acknowledging stress or worry should also be included as signs of validation. Physical contact may be considered validation if it is initiated or provided as a source of emotional support. Frequency of validation cues may vary within clips as it is performed as a reaction to the participant, meaning a lack of support seeking by the participant may yield a lack of validation cues. Thus, validation should be measured as a response, rather than an initiated action. If the participant does display some support seeking cues and the parent explicitly ignores or invalidates those cues, or the parent displays validation content cues with a negative affect, the parent should be given a score between 1 and 2, depending on frequency and intensity of the parent response. If the participant displays support seeking cues and the parent responds with validation, or if the parent initiates validation cues, the parent should be given a score between 4 and 5, dependent on the frequency and intensity of the validation cues. When the participant displays no support seeking cues and the parent does not initiate validation, the parent should be given a score of 3. A score of 3 may also be awarded when the parent displays a mix of validation and invalidation cues throughout the clip. Validation scores should reflect a balance between both content and affect cues, so that a parent who scores high in validation should express both validation affect and content.
Low Validation High Validation
Parent does not acknowledge Parent encourages
participant's ideas or feelings, participant ideas,
does not empathize with empathizes with
participant, appears participant, appears
uninterested or disengaged. invested in
participant's success
1 2 3 4 5




 Open access
Open access