


Schizophrenia is a severe mental disorder that results in a significant disability for the patient. In China, more than 50% of mental disabilities in adults are caused by schizophrenia.Reference Li, Chen, Du, Song, Zhang and Zheng1 From a life-course perspective, increasing amounts of evidence have indicated that prenatal maternal stress (PNMS) has a lasting effect on mental health, including increasing the risk for schizophrenia in later life.Reference Clair, Xu, Wang, Yu, Fang and Zhang2,Reference Babenko, Kovalchuk and Metz3 However, the association between prenatal exposure to earthquake and risk of adult schizophrenia has yet to be examined. The present study, using the Great Tangshan Earthquake (GTE) in 1976 as a natural experiment, was designed to capture the potential long-term effect of prenatal exposure to earthquake on the risk of schizophrenia in adulthood, using the difference-in-difference (DID) method, established by examining the regional variations of earthquake exposure across birth cohorts. The findings contribute to the literature by testing the fetal origins hypothesis, particularly regarding the effect of PNMS on adult schizophrenia from a nationwide perspective.
Method
The China National Sample Survey on Disability
The most recently released individual-level data were drawn from the China National Sample Survey on Disability (CNSSD), conducted in 2006. The aim of the survey was to investigate the prevalence, types, severity and causes of disabilities, as well as the living conditions and health service needs of populations with disability in China.
The sampling population of this survey was a household population in all province-level administrative regions of mainland China. Following standard procedures for complex samples, a multistage, stratified random cluster sampling with probability proportional to size was used to obtain the nationally representative samples in households. Each family member of the selected households was interviewed by trained field interviewers. In total, 2 526 145 people in 771 797 households were investigated from 5964 sites, 2980 towns, 734 counties and 31 provinces, representing 1.93 people per 1000 residents of China.
Ethical approval
The survey was approved by the State Council of China (approval no. 20051104) and conducted within the legal framework governed by the Statistical Law of the People's Republic of China (1996 Amendment). All survey respondents provided their informed written consent to participate in this survey.
The GTE
The GTE, occurring on 28 July 1976, is one of the largest and heaviest unpredicted earthquakes of the 20th century, with a magnitude of 7.8 on the Richter magnitude scale and more than 240 000 deaths. The epicentre of the earthquake was near Tangshan city in Hebei province, China, and the areas most affected were cities and counties of at least 14 provinces. The news was broadcasted at home and abroad by Xinhua News Agency of China later that day. Given the heavy magnitude and casualties of the GTE, it can be assumed that almost all of the Chinese people living at that time were aware of it and were affected by the earthquake in some way.
Analytical samples
In the present study, the term ‘prenatal exposure’ refers to maternal exposure to the GTE during the roughly 300 days from periconception to delivery. We restricted our analysis to the four birth cohorts pre-earthquake, earthquake, post-earthquake and reference, according to the birth time of participants relative to the time of the GTE. Individuals born between August 1975 and May 1976 had postnatal exposure to the earthquake during the first year of life, and were defined as the pre-earthquake cohort. The other three cohorts born in the same month period (August to May) in different years were used for analysis to minimise the differences caused by the month of birth. Those born between August 1976 and May 1977 were exposed to the earthquake strike in gestation, and thus were defined as the earthquake cohort. Those born between August 1977 and May 1978 and those born between August 1978 and May 1979 were not exposed to the earthquake in gestation or life, and they were defined as the post-earthquake cohort and as the reference cohort, respectively. The earthquake cohort was further divided into first (born between March 1977 and May 1977), second (born between November 1976 and February 1977) and third (born between August 1976 and October 1976) trimester subgroups, based on the timing of exposure during pregnancy. In addition, we assumed that all adult participants were living where their mothers were living at the time of their births, and excluded migratory adults according to the household registration information because their prefectures reported in the survey time were different from their birth prefectures. As a result, 94 410 adults born between August 1975 and May 1979 were used for analysis, aged 26–30 years during the survey time. Figure 1 illustrates the derivation of our analytical samples.
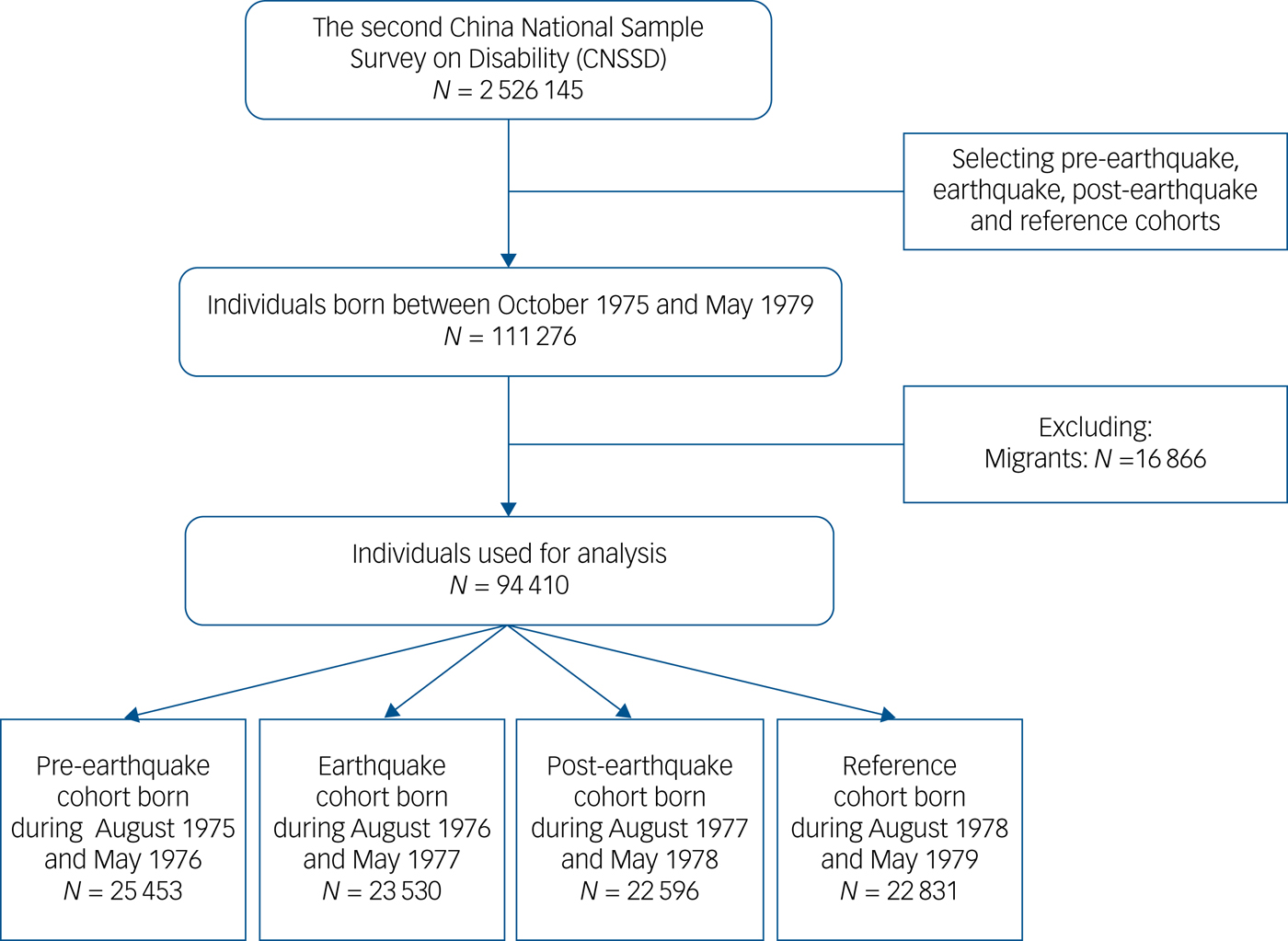
Fig. 1 Flowchart of samples.
Measures
Schizophrenia
The survey first identified individuals with psychiatric disability and then diagnosed schizophrenia from that subgroup. Psychiatric disability was defined as any mental disorders of over 1-year duration, manifesting as a cognitive, affective or behavioural disorder affecting the daily life and social participation of the patient, according to the World Health Organization's International Classification of Functioning, Disability and Health.4 During the survey, each family member of the selected households was interviewed by trained interviewers from local primary care institutions, using a screening questionnaire for disability according to the 2001 Guidelines and Principles for the Development of Disability Statistics, recommended by the United Nations. The questionnaire has been tested in three pilot studies and showed very good validity.Reference Zhang5 For those who could not provide valid information, a proxy who knew the most about the person answered the questions. The questions to detect psychiatric disability among adult individuals examined (a) forgetfulness, (b) difficulty concentrating, (c) inability to control moods, (d) out-of-the-ordinary behaviour and (e) addiction to alcohol or drugs.
Those who screened positive were referred to psychiatrists with at least 5 years of clinical experience to confirm diagnosis of disability and the detailed mental disorders. The World Health Organization's Disability Assessment Schedule, Version II,6 which has been validated among in a schizophrenic population,Reference Ulug, Ertugrul, Gögüs and Kabakcı7 was first administered to evaluate social function limitations. Individuals scoring 52 or higher were identified as with psychiatric disability and were assigned to subsequent diagnostic procedures for psychiatric disorders. The ICD-10 symptom checklist for mental disorders was administered to diagnose schizophrenia.8 The psychiatrists followed the instructions of the F0–F6 categories to fill out the checklist and diagnose schizophrenia. The ICD-10 diagnostic criteria had been widely used in the ascertainment of schizophrenia among Chinese people and has good validity in China.Reference Clair, Xu, Wang, Yu, Fang and Zhang2,Reference Xiang, Ma, Cai, Li, Xiang and Guo9
Earthquake severity
Earthquake severity was measured by seismic intensity, a preferred metric to evaluate how strongly an earthquake affects a specific place. The seismic intensity of the GTE in different regions of the country was identified according to the New Chinese Seismic Intensity Scale in 1957,Reference Hsieh10 and varied from I (not felt) to XI (disastrous). We implemented an ordinal category of the intensity in prefecture level by dividing the prefectures into three groups: destructive, felt and not felt. Destructive zones comprised prefectures where the intensity was destructive to disastrous (V–XI). Felt zones included prefectures where the earthquake was only felt by a few persons at rest to felt indoors by many (II–IV). Not felt zones encompassed prefectures where earthquake was not felt (I). Supplementary Figure 1, available at https://doi.org/10.1192/bjp.2019.114, depicts the geographical distribution of seismic intensity at the prefecture-level in China. This category is consistent with the original macroscopic observation record of the GTE (see Supplementary Figure 2) by the China Earthquake Administration.
Control variables
Control variables in this study included age (continuous variable), gender (male or female), area of residence (rural or urban according to the Hukou status of individuals), education level (primary school and below, junior high school or senior high school, or university and above), ethnicity (Han or other), marital status (married or single) and annual household income per capita (top, middle and bottom by tertiles 0–1999 RMB yuan, 2000–3999 RMB yuan or ≥4000 RMB yuan). We used province dummies to capture the provincial fixed effects.
Statistical analyses
We used the DID method, exploiting both cohort and geographical variations in earthquake exposure to estimate the effects of the GTE. Let Y ijk denote a schizophrenia outcome for participant i born in intensity j (1 = felt, 2 = destructive) and cohort k (1 = pre-earthquake cohort, 2 = earthquake cohort, 3 = post-earthquake cohort). X ijk denotes the control variables and ε ijk denotes random error; a logit regression model with DID estimator can be obtained from:
 $$\eqalign{ Y_{ijk} & = \alpha _0 + \mathop \sum \limits_{\,j = 1}^2 \theta _j{\rm Intensit}{\rm y}_j + \mathop \sum \limits_{k = 1}^3 \gamma _k{\rm Cohor}{\rm t}_k \cr & + \mathop \sum \limits_{ \,j = 1}^2 \mathop \sum \limits_{k = 1}^3 \beta _{jk}\lpar {{\rm Intensit}{\rm y}_j \times {\rm Cohor}{\rm t}_k} \rpar + \delta X_{ijk} + \varepsilon _{ijk},} $$
$$\eqalign{ Y_{ijk} & = \alpha _0 + \mathop \sum \limits_{\,j = 1}^2 \theta _j{\rm Intensit}{\rm y}_j + \mathop \sum \limits_{k = 1}^3 \gamma _k{\rm Cohor}{\rm t}_k \cr & + \mathop \sum \limits_{ \,j = 1}^2 \mathop \sum \limits_{k = 1}^3 \beta _{jk}\lpar {{\rm Intensit}{\rm y}_j \times {\rm Cohor}{\rm t}_k} \rpar + \delta X_{ijk} + \varepsilon _{ijk},} $$where β jk, the coefficients of the interaction between birth cohorts and earthquake zone, is the estimated effect of prenatal exposure to earthquake on later-life schizophrenia.
To estimate the earthquake effects on schizophrenia by different pregnancy trimesters, we also calculated the β jk for the cohort variable with subgroups (1 = pre-earthquake, 2 = first trimester, 3 = second trimester, 4 = third trimester, 5 = post-earthquake).
We estimated two models for each outcome variable. The first model did not include control variables and the second model controlled for age, gender, residence, education level, ethnicity, marital status, household income per capita and province fixed effects. The odds ratio, adjusted odds ratio and 95% CI were calculated. All data were entered into a customized database and analysed by Stata version 13 for Windows. Statistical significance was set at a two-sided P value <0.05.
Data availability
Data cannot be shared publicly because of legal restrictions, as the data contains potentially sensitive information. The State Council of China imposed the restrictions according to the Statistical Law of the People's Republic of China (1996 Amendment). A de-identified minimal data-set of the quantitative data is available upon request to researchers who meet the criteria for confidential information. Please send any requests to the Data Access Committee of Institution of Population Research, Peking University, no. 5 Yi He Yuan Lu, Beijing 100871, China (contact email: [email protected]).
Result
Characteristics of study participants by birth cohort
The study comprised 94 410 Chinese adults, with an average age of 28.38 ± 1.19 years during the survey time. Among the analytical samples, all four cohorts were similar in terms of gender composition (49.84–50.84% were men), residence area (71.40–72.29% resided in rural area) and ethnicity (85.02–85.75% were Han). Among our analytical samples across the nation, 10.86% were in prefectures of destructive earthquake intensity and 28.99% were in the felt prefectures. Table 1 reports the cohort-specific descriptive statistics of characteristics of study participants by birth cohorts.
Table 1 Characteristics of study participants, by birth cohort
Prenatal exposure to earthquake and risk of schizophrenia in adulthood
Among the study adults, 371 (0.39%) were experiencing schizophrenia at the survey time. Rate of adult schizophrenia following prenatal exposure to the GTE was 0.42%. Without further stratifying each cohort by prefecture, differences between cohorts in schizophrenia were not statistically significant (Table 1).
Table 2 shows the DID estimates of the prenatal earthquake effect on adulthood schizophrenia. We found that the earthquake cohort with any prenatal exposure to felt earthquake had higher odds (odds ratio, 3.59; 95% CI 1.50–8.59) of schizophrenia as compared with the reference cohort in the unadjusted model. This effect was partially mitigated but remained significant (odds ratio, 3.38; 95% CI 1.43–8.00) after controlling for multiple covariates.
Table 2 Prenatal earthquake exposure and risk of schizophrenia in adulthood, by earthquake cohort

AOR, adjusted odds ratio estimated from models controlling for age, gender, residence, education level, ethnicity, marital status and household income per capita.
Table 3 shows the effect of prenatal exposure to earthquake on schizophrenia by trimester of pregnancy. After controlling for covariates, prenatal exposure to felt earthquake during the first trimester of pregnancy increased the risk of adulthood schizophrenia significantly (odds ratio, 7.45; 95% CI 2.83–19.59). By contrast, we did not find a significant effect of prenatal exposure to earthquake during the second or third trimester of pregnancy on adulthood schizophrenia.
Table 3 Prenatal earthquake exposure and risk of schizophrenia in adulthood, by trimester of pregnancy
AOR, adjusted odds ratio, estimated from models controlling for age, gender, residence, education level, ethnicity, marital status and household income per capita.
Sensitivity checks
Similar to the pattern shown in Tables 2 and 3, when another cohort (born during June 1978 and March 1979, immediately following the aftermath of the GTE) was used as the reference group, we could still observe significant effects of any prenatal exposure to felt earthquake during gestation (odds ratio, 2.64; 95% CI 1.25–5.58) and during the first trimester of pregnancy (odds ratio, 5.84; 95% CI 2.71–12.57) on adult schizophrenia (see Supplementary Table 1).
With a priori knowledge that the urban population experienced much higher earthquake mortality ratios depending on the effective population size during the GTE,Reference Gutierrez, Taucer, De Groeve, Al-Khudhairy and Zaldivar11 we examined the potential heterogeneity of earthquake stress response across the population by fitting the same models to the urban sample and rural sample respectively. As a result, we found the effect of any prenatal exposure in the rural sample to felt earthquake during gestation (odds ratio, 3.35; 95% CI 1.06–10.64) and during the first trimester of pregnancy (odds ratio, 5.29; 95% CI 1.36–20.55) on adulthood schizophrenia in the adjusted models, which is similar to the total sample. However, we did not find effects in the urban sample (see Supplementary Table 2).
Discussion
According to the fetal origins hypothesis, the origins of many adults' physical and mental health outcomes can be traced back to the in utero period, when rapid changes in the structure and function of the fetal brain and body take place based on the intrauterine and extrauterine environments.Reference Glover12 In this study, we identified for the first time that any prenatal exposure to earthquake during gestation has an enduring deleterious effect on schizophrenia in adulthood, using the GTE as a natural experiment. Data for this study were gleaned from a large representative sample of the most recent national population-based survey on disability in China. Our findings provide an epidemiological verification in the large population of China, using robust methodology.
Based on the life-course model of health, the resulting deleterious effect on mental conditions may have a long latency period before its manifestation in adulthood.Reference Ben-Shlomo and Kuh13 Our result is consistent with the findings of prior studies on the association between earthquakes and mental health in China,Reference Wang, Shi, Zhang, Ma, Jiang and Sun14,Reference Cai, Zhu and Sun15 although causal processes are not sufficiently documented in the existing literature. Our findings of the earthquake effects are also supported by studies on other disaster-related PNMS, such as exposure to ice storm,Reference King, Dancause, Turcotte-Tremblay, Veru and Laplante16 floodReference Selten, van der Graaf, van Duursen, Gispen-de Wied and Kahn17 and terror attacks,Reference Weinstein, Levav, Gelkopf, Roe, Yoffe and Pugachova18 which suggest these stress experiences during gestation exert long-term consequences on future risk of schizophrenia.
Furthermore, in our study, we found that individuals who experienced the earthquake during the first trimester of pregnancy had significantly higher risk of adulthood schizophrenia. This is consistent with prior research on maternal stress in trimesters of pregnancy and schizophrenia in later life, which suggests that the first trimester is a particularly critical period for a variety of stressors that have been associated with an increased risk for neurodevelopmental disorders, including schizophrenia.Reference Khashan, Abel, McNamee, Pedersen, Webb and Baker19,Reference Palmer, Evans, Broughton, Huddart, Drayton and Rankin20 Our findings indicate that the first trimester may be especially crucial as the fetus is particularly vulnerable to PNMS, an adaptive response to demands of the environment.Reference Babenko, Kovalchuk and Metz3
Generally, exposure to prenatal stress may increase the susceptibility to adult schizophrenia through neuroendocrine mechanism, epigenetic modifications and alteration of the hypothalamic-pituitary-adrenal axis (HPA-axis).Reference Babenko, Kovalchuk and Metz3,Reference Wadhwa, Culhane, Rauh and Barve21 During the first trimester, the neurogenesis and self-renewal of neural stem cells vigorously occur; disturbance of the neuronal proliferation and migration during this period may underlie the increased susceptibility to schizophrenia.Reference Udagawa and Hino22 Stress can also affect the epigenetic modifications, such as DNA methylation and histone modification. They are critical mechanisms for regulating gene expression and are associated with an increase in susceptibility to schizophrenia when affected.Reference Babenko, Kovalchuk and Metz3,Reference Udagawa and Hino22 Furthermore, fetal programming by glucocorticoids is known to occur early in gestation. The changes in HPA-axis programming through glucocorticoids as a result of antenatal stress may program a trajectory of abnormal brain growth, from fetal brain development through puberty and into adulthood.Reference Khashan, Abel, McNamee, Pedersen, Webb and Baker19
In terms of earthquake severity, in contrast to the Chile Tarapaca Earthquake Study that found a significant effect of high-intensity earthquake on preterm delivery, our study reports that only felt earthquake (similar to moderate intensity in the Chile study) exposure during gestation was statistically significant in the deleterious effect on adult schizophrenia. We speculate that mortality selection effect could shape this phenomenon. Extreme negative adversity often results in excess mortality, with the least healthy members of the population being affected the most.Reference Seltzer and Jablon23 Consequently, the surviving cohorts may be healthier than other cohorts that were not subject to such seismic shock. The mortality selection hypothesis thus predicts a positive or null link between early-life exposure to severe shocks and later health outcomes.Reference Mu and Zhang24 The GTE killed 242 769 persons, according to official figures, and almost all of them were in the destructive zone when the earthquake struck. In comparison, the Tarapaca Earthquake killed 11 persons, although the moment magnitude scale of the two earthquakes were similar. The mortality selection effect is also reflected in the results of urban and rural sub-population analysis in our study. As mentioned above, compared with the rural population, the urban population experienced much higher earthquake mortality ratios with more effective population size during the GTE.Reference Gutierrez, Taucer, De Groeve, Al-Khudhairy and Zaldivar11 Therefore, the different results we found between urban and rural population infer the presence of both a significant earthquake effect of exposure from the deleterious results in rural samples and a positive mortality selection effect from the null results in urban samples. Consistent with prior studies on famine and war,Reference Seltzer and Jablon23,Reference Mu and Zhang24 our results of earthquake suggest that, for the mental health outcome as measured by schizophrenia, the mortality selection effect offsets the fetal origins effect in urban GTE survivors.
A wealth of data exists on the prevalence of schizophrenia in different parts of the world. A recent review reported that the 10–90% quintiles for the point prevalence of this disease ranged from 0.19% to 1%, with a median of 0.6%.Reference McGrath, Saha, Chant and Welham25 Our prevalence estimation of 0.39% falls within this range. However, since we excluded individuals with schizophrenia not experiencing disability from our estimation and disability was self-reported during screening, the prevalence estimates are likely lower than when we included all affected persons.
Limitations
The current study has several limitations. First, the strategy of using a natural disaster as an exogenous source of stress rests on the exclusion restriction assumption that there are no alternative paths of influence other than that stress. Although we have considered the effect of mortality, alternative pathways of influence cannot be fully ruled out. In addition, this study was not able to account for the differences in maternal access to social and instrumental support, personal resilience or coincidental stressors that might be worsened by the GTE, including violence perpetrated by an intimate partner. Moreover, earthquake is an acute population-level stressor, so the generalisability to chronic or individual-level sources of stress remains a question. Additionally, the CNSSD seems a little outdated (although our main objective was not the recent prevalence of schizophrenia) and people living in institutions such as dormitory or army are not represented in this household survey. Despite these limitations, our findings contribute to an emerging body of evidence showing that maternal stress, particularly in early pregnancy, substantially affects the risk of schizophrenia in early adulthood after a major disaster. Further studies will focus on other disaster-related PNMS that were not well studied in China, such as exposure to flood and other mental disorders, to further validate the findings.
In conclusion, this study explored the long-term effect of prenatal exposure to earthquake on the risk of adult schizophrenia based on data from a nationally representative survey, using robust methods. Currently, the Chinese Government is developing the Healthy China Plan as a national strategy to promote health up to 2030, in which health promotion for the entire population and throughout the total life cycle is the main theme. This policy provides great opportunities to engage in population health research from a perspective of the life cycle, to prevent adult diseases and disabilities in early life. Our findings indicate that early life health investment is not only an imperative pathway, but also a sufficient condition for the realisation of the Healthy China Plan. This study contributes to the literature on prenatal and early-life exposure to stress and calls for potential health practice strategies in a non-Western context.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjp.2019.114.
Funding
This work was supported by the National Social Science Foundation of China (grant number 18CRK005, awarded to C.G.). However, the funder had no role in the design, analysis, interpretation or decision to submit this paper.
Acknowledgements
The authors are grateful to Richard Liang, a medical intern at Cedars-Sinai Medical Center and Master's candidate at Fielding School of Public Health of University of California, Los Angeles, for the review of the manuscript.







 Open access
Open access
eLetters
No eLetters have been published for this article.