



Introduction
Patients with advanced cancer have an inevitable and predictable trajectory of dying, which is described as a steady decline with expected death no matter what treatments are offered (Institute of Medicine (US) Committee on Care at the End of Life 1997). Thus, for patients with advanced cancer and their family members, issues about end-of-life (EoL) decision-making are unavoidable themes that they must face.
Processes of EoL decision-making are influenced by cultural backgrounds of different regions to a large extent (Al-Bahri et al. Reference Al-Bahri, Al-Moundhri and Al-Azri2017). In western countries, which prioritize patients’ autonomy, the process of medical decision-making is mainly based on the combination of patients’ preferences, best interest standards, and substituted judgment (Gilbar Reference Gilbar2011; Lin et al. Reference Lin, Pang and Chen2013; Shepherd et al. Reference Shepherd, Hood and Sheehan2018). However, in Asian regions influenced by Confucian collectivism, such as China, Korea, and Japan, the process of important medical decision-making is largely based on family autonomy and family members are the legitimate and ordinary persons to make the final decisions (Fan Reference Fan2011; Gu et al. Reference Gu, Chen and Liu2016; Ho et al. Reference Ho, Kwong and Song2022; Lin et al. Reference Lin, Pang and Chen2013; Mori and Morita Reference Mori and Morita2020). In China, making EoL decisions for advanced cancer patients is the family members’ responsibility which can protect the patients from psychological burden.
Family decision-making self-efficacy (FDMSE) refers to the confidence that family members perceived in making EoL decisions with or for their loved ones. This includes confidence in making the best decisions, making decisions about feeding, resuscitation, treatment for pain, and palliative care, meeting spiritual needs, maintaining family harmony, and talking with medical professionals (Nolan et al. Reference Nolan, Kub and Hughes2008).
Previous studies found that families of patients with cancer, critical illness, and amyotrophic lateral sclerosis in the US all reported relatively high levels of self-efficacy in EoL decision-making (Dionne-Odom et al. Reference Dionne-Odom, Ejem and Azuero2018; Nolan et al. Reference Nolan, Hughes and Kub2009; Pignatiello et al. Reference Pignatiello, Irani and Tahir2020). However, in China, topics associated with death are taboo in Chinese families, and family members are reluctant to talk about EoL issues with patients and physicians (Pun et al. Reference Pun, Cheung and Chow2020). Under this unique cultural background, little is known about Chinese families’ self-efficacy in making EoL decisions for advanced cancer patients.
According to Bandura’s self-efficacy theory, self-efficacy originates from 4 sources, with one of the most important being mastery experiences (Bandura Reference Bandura1977). Nolan had demonstrated that there was a difference in family members’ decision-making self-efficacy between families who had past experiences of making EoL decisions and those who did not (Nolan et al. Reference Nolan, Hughes and Kub2009). Other authors have also recognized that some demographic factors such as patient’s age, family members’ gender, financial status, relationship with their loved ones, and other factors such as past discussion of EoL preferences were associated with families’ self-efficacy in decision-making (Dionne-Odom et al. Reference Dionne-Odom, Ejem and Azuero2018; Piña-Escudero et al. Reference Piña-Escudero, García-Avilés and Fajardo-Juárez2019). Currently, little is known about factors associated with Chinese family members’ self-efficacy in EoL decision-making.
To sum up, within the context of mainland China, the pivotal role of family members in EoL decision-making for their loved ones is markedly pronounced. However, given the distinct cultural landscape of the region, there exists a notable scarcity of research delving into the confidence levels of these family members in EoL decision-making, as well as the factors associated with this confidence. Consequently, this study primarily investigates the self-efficacy of Chinese family members in making EoL decisions for relatives afflicted with cancer, alongside exploring the various factors that might impact their decision-making self-efficacy.
Methods
Participants
In this study, a cross-sectional, anonymous questionnaire was conducted from June to October 2021, utilizing convenience sampling to recruit eligible patients with cancer and their family members in a tertiary cancer hospital in Guangzhou, China. The inclusion criteria included the following aspects: patients aged 18 years and above who had been hospitalized and diagnosed with a stage III or stage IV cancer; and a family member was the self-proclaimed main proxy decision-makers for the patient, aged 18 years and above, and proficient in Chinese reading and writing to complete the questionnaire.
According to Kendall’s sample estimation method, 5–10 times the number of variables is taken as the sample size in this study (Kendall and Weber Reference Kendall and Weber1977). There were 16 variables in the demographic characteristics questionnaire, and 4 variables in the patients’ EoL preferences questionnaire, so a total of 20 variables needed to be analyzed. Considering an invalid questionnaire rate of 10%, the minimum sample size was 112 in this study.
Measurements
Participant characteristics
Demographic characteristics included patients’ age, gender, primary site of cancer, duration of disease, education level, employment status, marital status, health insurance, and family members’ age, gender, education level, employment status, marital status, relationships with patients, family per capita monthly income, and past experiences of EoL decision-making. These 16 demographic factors may influence family members’ perceived confidence in EoL decision-making.
Patients’ EoL preferences questionnaire
Patients’ EoL preferences include the patients’ awareness of their diagnosis, participation in EoL decision-making, attitude toward life-sustaining treatment, and expression of unfilled wishes. These 4 factors may influence family members’ confidence in making EoL decisions for or with their loved ones.
Family decision-making self-efficacy
Based on Bandura’s self-efficacy theory, the FDMSE Scale was developed by Nolan through in-depth interviews with bereaved family members and used to assess the degree to which family members felt confident in making EoL decisions with or for their loved ones (Bandura Reference Bandura1977; Nolan et al. Reference Nolan, Hughes and Kub2009). There are 2 versions of the FDMSE: a version for conscious patients and another for unconscious patients. Both versions consist of 13 items with a 5-point Likert Scale ranging from 1 (“cannot do at all”) to 5 (“certainly I can do”). The total score ranges from 13 to 65, with a higher score indicating higher levels of confidence of family members in EoL decision-making with or for their loved ones. The conscious version of FDMSE has been translated into Chinese with a Cronbach’s alpha of 0.86 and a content validity of 1.0 (Hu et al. Reference Hu, Peng and Zhao2022). The Chinese version was used in this study.
Statistical analysis
The data were collected and analyzed using the Statistical Package for the Social Sciences (SPSS, v. 25.0). We used descriptive statistics to analyze the demographic characteristics of the patients and the family members, the item score and the average score of the FDMSE, and the patients’ EoL preferences. The family members who self-perceived “confidence” in each item were defined as those who chose the item score ≥4 points (I can do). An independent t-test and 1-way analysis of variance were used to analyze the variation of the FDMSE average score according to demographic characteristics and patients’ EoL preferences. Least significant difference test was used for conducting pairwise comparisons between groups. Finally, multiple regression analyses were used to explore factors contributing to the total score of the FDMSE. We set the significance level to be included in the model as p < 0.05.
Results
A total of 147 questionnaires were collected from eligible family members. Two questionnaires were excluded because of missing data (over 50%). Thus, 145 questionnaires were analyzed with an effective response rate of 98.6%. The mean score on the item-level of the FDMSE among family members was 3.92 ± 0.53.
Characteristics of participants
The patients’ and their family members’ demographic characteristics are shown in Table 1. On average, the patients were 56.28 ± 10.59 years old, and their duration of disease was 18.61 ± 35.36 months. Male patients made up 60.0% (87/145) of the total. The majority of patients were high school or below (79.3%), unemployed (84.1%), married (89.7%), and had health insurance (92.4%); on average, family members were 37.63 ± 10.18 years old. Nearly half of them were male (55.9%), married (80%), college or above (51.7%), employed (57.2%), offspring of the patients (53.1%), and with a monthly family income per capita of over 5000 yuan (53.1%). Only 27 (18.6%; 27/145) family members had past experiences of EoL decision-making.
Table 1. FDMSE average score according to the characteristics of patients and their family members

FDMSE = family decision-making self-efficacy; ANOVA = analysis of variance; SD = standard deviation.
* p< 0.05, **p< 0.01.
a FDMSE average score have statistical differences between 4 and 6 months and the other groups.
b FDMSE average score have statistical differences between >12 months and 1–3 months.
Patients’ EoL preferences
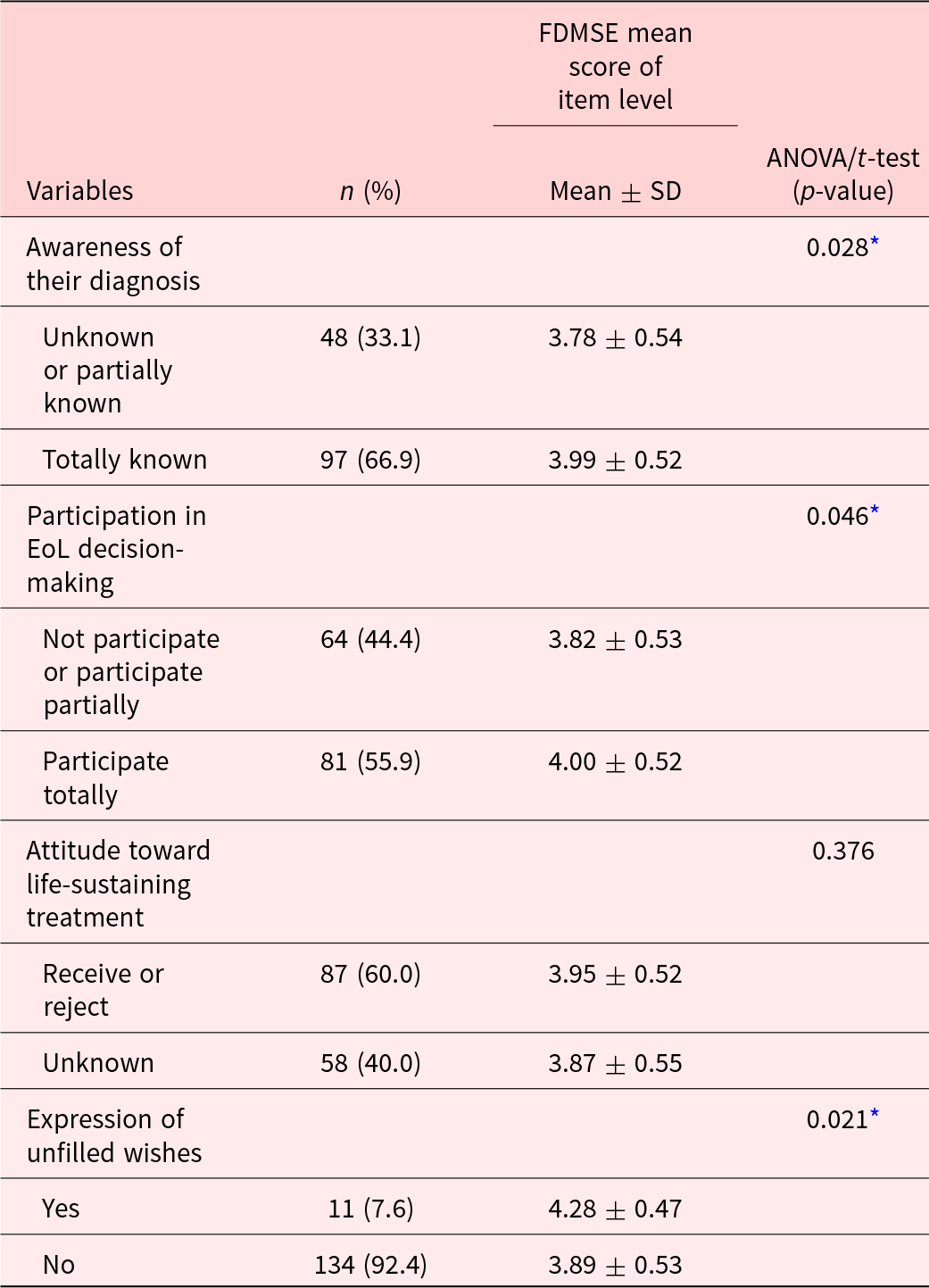
The patients’ EoL preferences are shown in the Table 2. A majority of patients were fully aware of their diagnosis (66.9%), totally participated in their EoL decision-making (55.9%), and had a clear attitude (receive or reject) toward life-sustaining treatment (60.0%); only 11 (7.6%; 11/145) of them had expressed their unfilled wishes.
Table 2. FDMSE average score according to patients’ EoL preferences
FDMSE = family decision-making self-efficacy; EoL = end of life; ANOVA = analysis of variance; SD = standard deviation.
* p;< 0.05, **p< 0.01.
Self-perceived confidence in EoL decision-making among family members
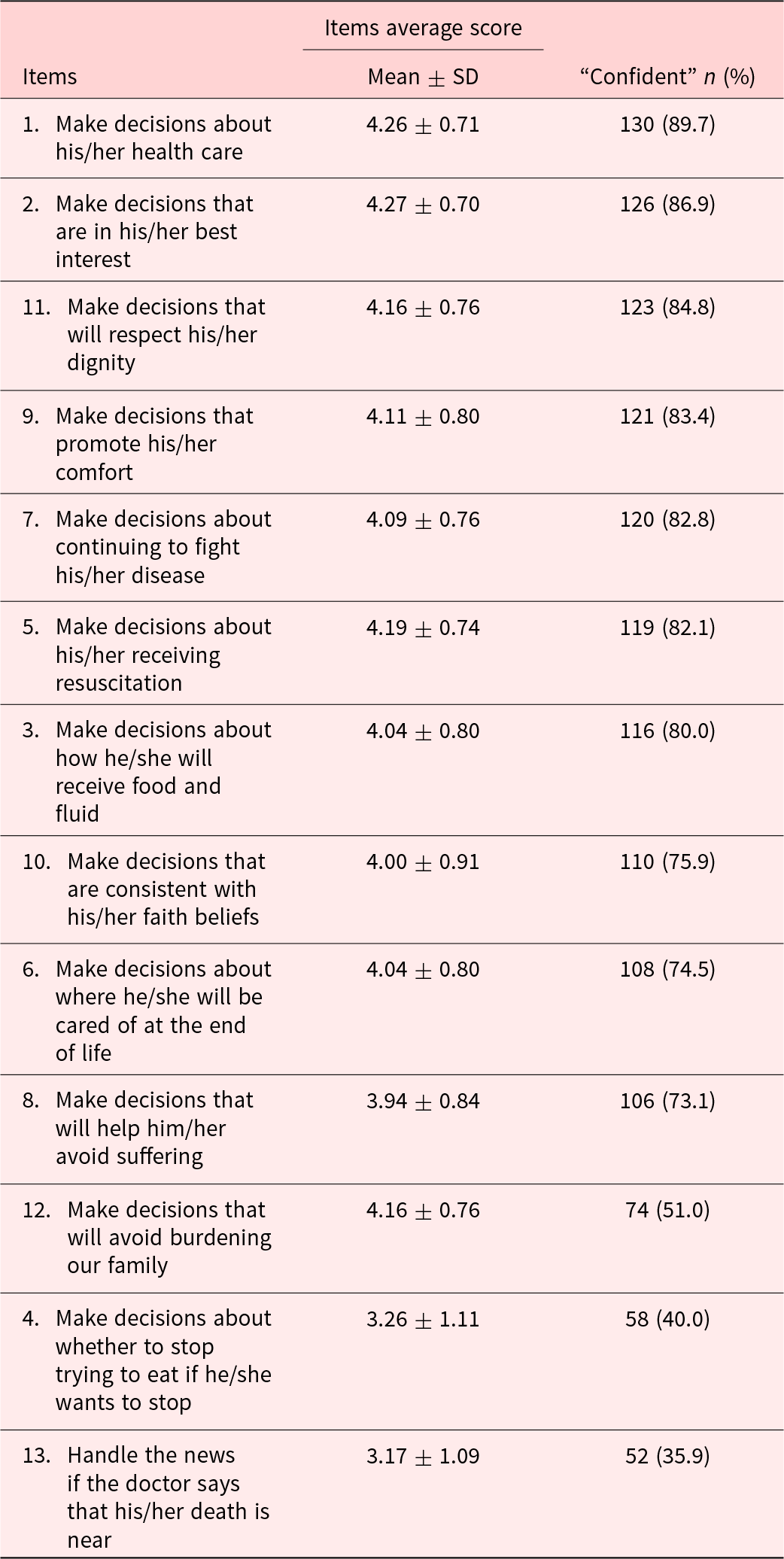
The 13 items were arranged in descending order by the percentage of the score equal to and greater than 4 points (I can do), as shown in Table 3. The item “Make decisions about his/her health care” was the highest; the item “Handle the news if the doctor says that his/her death is near” was the lowest.
Table 3. Items of FDMSE (mean ± SD) and the percentage of perceived confidence in EoL decision-making in descending order
FDMSE = family decision-making self-efficacy; SD = standard deviation.
Differences of FDMSE average according to demographic characteristics and patients’ EoL preferences
Table 1 presents the differences in FDMSE average score among demographic variables of patients and their family members. The FDMSE average score showed statistically significant differences among patients with different duration of disease (p < 0.001) and different health insurance (p = 0.017), and in family members who were unemployed (p = 0.002) and with lower monthly family income (p = 0.015).
As shown in Table 2, patients’ EoL preferences with statistical differences included patients’ awareness of their diagnosis, participation in EoL decision-making, and expression of unfilled wishes. FDMSE was lower in patients who did not know or knew their diagnosis partially (p = 0.028), did not participate or partially participated in their EoL decision-making (p = 0.046), and did not express their unfilled wishes (p = 0.021).
Predictors of FDMSE total score
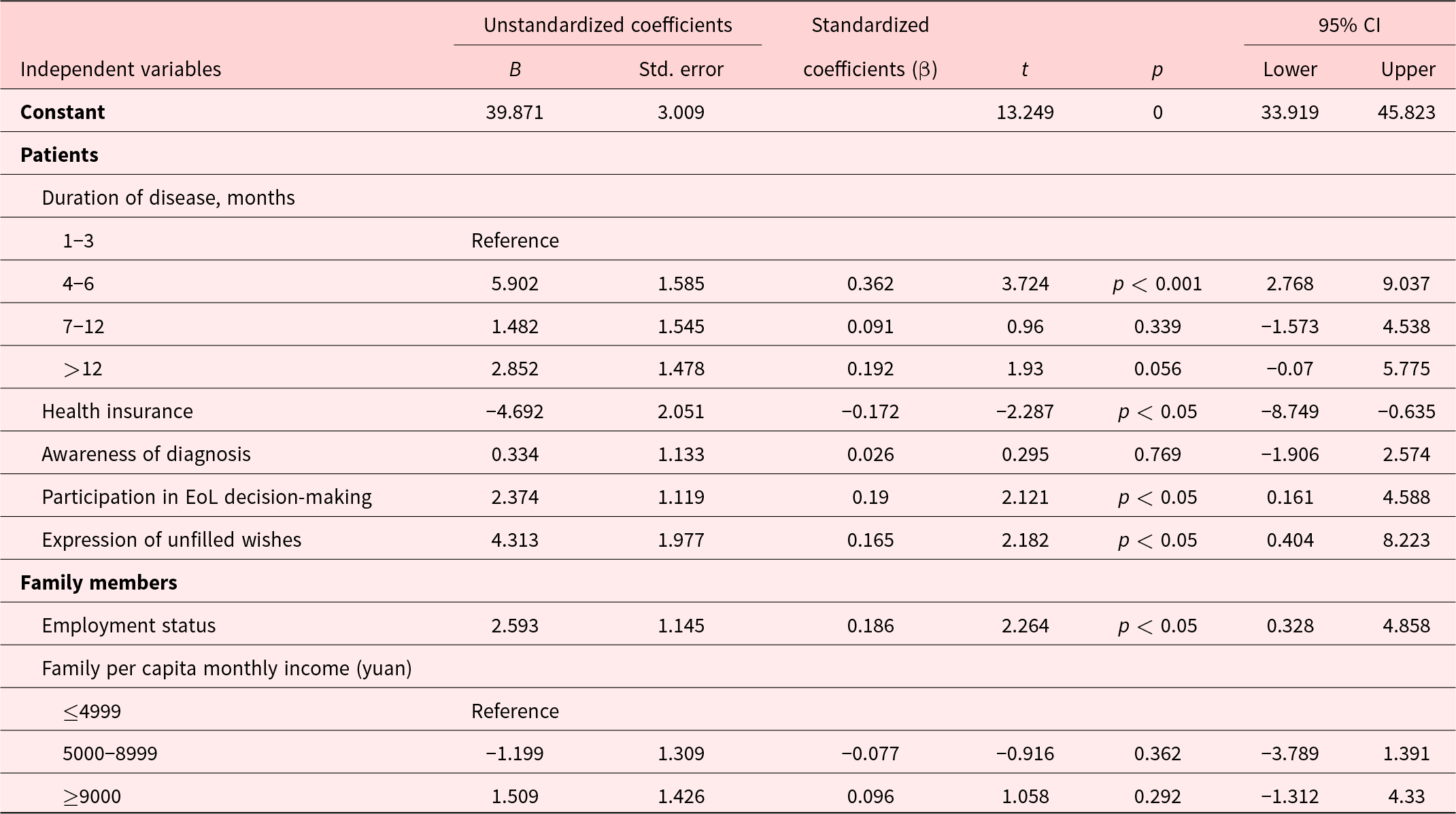
Using the FDMSE total score as the dependent variable, 7 variables with statistical significance in the univariate analysis (patients’ duration of disease, health insurance, awareness of their diagnosis, participation in EoL decision-making, expression of unfilled wishes, family members’ employment status, family per capita monthly income) were taken as the independent variables to conduct a multiple linear regression analysis, as shown in Table 4. Five factors entered the regression equation. The patients’ duration of disease (p < 0.01), health insurance (p < 0.01), participation in EoL decision-making (p < 0.05), expression of unfilled wishes (p < 0.05), and family members’ employment status (p < 0.05) served as predictors of the FDMSE total score of family members of patients with advanced cancer, which explained 27.6% (F = 5.119, p < 0.001) of the score variance.
Table 4. Multivariate linear regression model for prediction of FDMSE total score
CI = confidence interval; FDMSE = family decision-making self-efficacy.
Discussion
In this study, the family member’s self-efficacy in making EoL decisions for their loved ones with advanced cancer was found to be not high, that is, they were not confident enough to make EoL decisions. Also, several characteristics of patients and family members were found to be associated with family members’ confidence in making EoL decisions.
The averages score of Chinese FDMSE for advanced cancer patients in this study (3.92) was comparatively lower than those previously reported among American family members who made EoL decisions for cancer patients (4.50) (Dionne-Odom et al. Reference Dionne-Odom, Ejem and Azuero2018), critically ill patients undergoing mechanical ventilation (4.60) (Pignatiello et al. Reference Pignatiello, Irani and Tahir2020), and patients with amyotrophic lateral sclerosis (4.55) (Nolan et al. Reference Nolan, Hughes and Kub2009). This finding suggested that Chinese family members of advanced cancer patients encounter significant ethical dilemmas when making EoL decisions, resulting in reduced confidence (Lin Reference Lin2023). This phenomenon could be attributed to 2 reasons. First, the prevalent Chinese culture tended to avoid discussions about EoL care. In China, there is a pervasive silence surrounding EoL discussions among family members, which make them often lack both the readiness and awareness necessary for early discussions on EoL decision-making (Cheung et al. Reference Cheung, Au and Ip2020; Chiang et al. Reference Chiang, Wang and Hsieh2021; Pun et al. Reference Pun, Cheung and Chow2020; Tong and Spicer Reference Tong and Spicer1994). Second, support from health-care providers may not be sufficient. A recent survey in China revealed that a majority of Chinese family members received little information about EoL care from their physicians (Yao et al. Reference Yao, Chen and Lai2022). Several prior research indicated that engaging in conversations about EoL care can significantly bolster the confidence of surrogate decision-makers in handling EoL choices (Hickman and Pinto Reference Hickman and Pinto2014; Majesko et al. Reference Majesko, Hong and Weissfeld2012). In the future, the development of culturally tailored EoL communication strategies and the promotion of health-care providers’ initiative in providing information on EoL care are recommended for empowering Chinese cancer family members to participate in EoL care decision-making with enhanced confidence.
The current study showed that patients having medical insurance and family members being employed were associated with higher family members’ self-efficacy levels. Similarly, Hua et al. (Reference Hua, Cha and Ge2019) revealed that Chinese family members with less financial burden tend to have higher confidence in EoL decision-making. The cause may be attributed to the high medical expenditure incurred during the EoL period. A survey revealed that around 40% of the total health-care expenses for Chinese cancer patients are incurred in the final 3 months of their lives, which imposed heavy economic burdens in Chinese Cancer patients and their family (Leng et al. Reference Leng, Jing and Nicholas2019). This suggests that cancer patients’ family with worse financial status may be more likely to face the problem of lacking confidence in EoL decision-making.
The present study revealed that patients without expression of unfilled wishes and participation in EoL decision-making were correlated with a lower self-efficacy level of family members, which was consistent with the findings by Piña-Escudero’s et al.’s (Reference Piña-Escudero, García-Avilés and Fajardo-Juárez2019). Recently, Chen et al. (Reference Chen, Du and Cheng2023) demonstrated that terminal patients’ awareness regarding their prognosis yielded more benefits than harm for both Chinese patients and their family caregivers in terms of decision-making. However, previous studies have demonstrated that discussing EoL decisions in advance is not widely accepted among Chinese families, and most patients are excluded from the discussion (Xing et al. Reference Xing, Lin and Li2017). Therefore, culturally based advanced care planning is urgently needed to support physicians, patients, and their family members as a whole in clarifying the preferences of patients, and it may help promote the family members’ self-efficacy in making EOL decisions with or for patients with advanced cancer.
The current study also found that patients diagnosed within 3 months were associated with lower family members’ self-efficacy level. To the best of our knowledge, no existing studies have specifically addressed this correlation. Future longitudinal research is recommended to track the evolving trajectory of family members’ confidence in making EoL decisions for advanced cancer patients and determine the optimal timing for providing EoL decision-making support to family members.
Limitations
This study has some limitations. First, a convenience sample from 1 cancer center was adopted. Thus, there is a risk of selection bias, and the conclusions of this study may not be generalizable to other types of medical institutions. Second, the family members in this study were relatively young, with an average age of 37.63 ± 10.18 years, over half of whom had college-level education and a monthly family income above 5000 yuan. Thus, the findings may not be generalizable to families with different demographic characteristics.
Conclusions
To summarize, compared with studies in other regions, the Chinese family members in our study were relatively less confident about EoL decision-making for advanced cancer patients. We found that the factors associated with FDMSE included patients’ duration of disease, health insurance, expression of unfilled wishes, and family members’ employment status. The level of family members’ self-efficacy was lower when they had no source of income and had to face EoL decision-making for advanced cancer patients with a disease duration of less than 3 months, without health insurance, expression of unfilled wishes and participation of EoL decision-making. Therefore, we propose the development of cultural-tailored advanced care planning models to clarify patient preferences and to enhance the family members’ self-efficacy in making EoL decisions with or for patients with advanced cancer.
Acknowledgments
We express our great gratitude to the family members who participated in this study. Also, we are appreciative of the support and permission of this study from the hospital managers.
Author contributions
Yangfan Hu and Wenxia Wang contributed equally to this work.
Funding
This work was supported by the National Natural Science Foundation of China (grant No. 72004243) and the Fundamental Research Funds for the Central Universities, Sun Yat-sen University (grant No. 2021qntd33).
Competing interests
The authors declare that they have no conflict of interest.
Ethical approval
This research study was approved by the Ethical Committee of the School of Nursing, Sun Yat-sen University, Guangzhou, China (2021ZSLYEC-393), and the ethical committees of the medical institution participating in this study.




