



Family-centred rounds have become the gold standard for inpatient paediatric rounding. 1 Previous work suggests family-centred rounds reduce harmful errors, increase nursing engagement, and improve staff and family satisfaction. Reference Khan, Spector and Baird2–Reference Mittal4 Despite widespread adoption of family-centred rounds in general paediatrics, it is understudied and poorly described in subspecialty settings including paediatric cardiology. Reference Kipps, Albert, Bomher, Cheung, Feehan and Kim5 Patient and unit-based factors differ between cardiology and general paediatrics units including team census, patient acuity and chronicity, nursing ratios, and use of high acuity therapies. As such, it is reasonable to hypothesise that rounds may function differently on an acute care cardiology unit and that family-centred rounds may have different benefits and barriers to implementation. Reference Hoerst, Bakar and Cassidy6–Reference Harahsheh, Kipps and Hart8 Many heart centres are developing dedicated acute care cardiology units, Reference Anderson, Chowdhury and Connor9 presenting opportunities to develop and study rounding models and impact of family-centred rounds. Known limitations of family-centred rounds Reference Anttila, Rappaport, Tijerino, Zaman and Sharif10,Reference Parente, Stark and Key-Solle11 may also be addressed as acute care cardiology units develop dedicated practices. Reference Gal, Char, Anderson, Cooper and Madsen12 Self-reporting of use of family-centred rounds in acute care cardiology units is high; however, the definition of family-centred rounds and approach to rounds in these centres remains unknown. Reference Hoerst, Bakar and Cassidy6 Within acute care cardiology, local quality improvement efforts increased nursing and family presence during rounds, Reference Kipps, Albert, Bomher, Cheung, Feehan and Kim5 suggesting such efforts could improve family-centred rounds as well.
Within the acute care cardiology unit at Cincinnati Children’s Hospital Medical Center, families have been variably involved in daily rounds but many principles of family-centred rounds are not employed, likely limiting the true benefits of family-centred rounds. Reference Destino, Shah and Good3 Therefore, we sought to use quality improvement methods to improve the family-centredness of our rounds by increasing family presence and participation in daily rounds.
Materials and methods
Setting
This project was conducted in a 29-bed acute care cardiology unit at a tertiary care children’s hospital housing patients under a heart failure/transplant service and a general cardiology service. The project was limited to the general cardiology service due to availability of staff for data collection. The rounding team consists of nurse practitioners, paediatric residents, a categorical cardiology fellow and intermittently an advanced acute care cardiology fellow, a cardiology attending, a pharmacist, a dietician, and case managers. Ancillary staff members, including social workers, therapists (respiratory, occupational, speech, and physical), as well as subspecialty cardiology (e.g. electrophysiology, adult congenital) and other medical consult services are present during rounds depending on patient need. Bedside nurses initiate rounding encounters reporting objective and overnight data. Rounds are conducted in the hallway outside of patient rooms. Families at the bedside are often invited to listen and ask questions, but there was no systematic approach to families at the bedside joining rounds nor an established means for families to join virtually when away from the bedside. The timing of rounds is variable. Families are not provided a specific time estimate of when their rounds will occur.
Intervention
We formed a multidisciplinary improvement team of nurses, nurse practitioners, attending physicians, a nursing manager, and a family representative. We established operational definitions for family presence and family participation during rounds. Family presence was defined as the family joining the rounding encounter, physically or via telecommunication. Families who were at bedside but did not join the rounding encounter (e.g. sleeping, working, engaged in other conversation/discussion, opted not to join) were not counted. Family participation was defined as the family asking any question or making any comment during the rounding encounter aside from standard greetings and closures. Baseline family presence and participation were manually counted from 28 August, 2021 to 5 January, 2022. This informed our SMART aim: to increase family presence from a mean of 43–75% and family participation from a mean of 81–90%, both by 30 May, 2022. Following the Institute for Healthcare Improvement Model for Improvement, we created a key driver diagram (Supplemental Figure 1) to identify potential interventions for iterative plan-do-study-act cycles. Between January and May 2022, plan-do-study-act cycles were run targeting different failures of the baseline system.
Education to the multidisciplinary team
The improvement team provided education related to benefits of family-centred rounds to unit nurse practitioners and attendings. The education highlighted the American Academy of Pediatrics statement on family-centred care 1 and research supporting the use of family-centred rounds in general paediatrics. It also mirrored the rounding training paediatric residents receive at the hospital level. Bedside nurses were engaged and made aware of the initiative through nursing members on the improvement team. After initial education was completed, attendings and nurse practitioners were periodically given informal reminders of the benefits and value of family-centred rounds verbally or via text messages.
Interventions to improve family presence among families unable to be at bedside
Early failure analysis revealed common reasons for families not being at bedside were caring for other children or family members, inability to miss work, difficulty with transportation, prioritising sleep because of admission-related fatigue, and missing rounds inadvertently because of lack of knowledge of when rounds would occur. We tailored interventions to attempt to address these challenges.
As families report high satisfaction with telehealth solutions when unable to be in person, Reference Rogers, Lynch, Toth and Weisgerber13 we introduced an intervention to call families and use speakerphone for those unable to be at bedside during rounds. This required adaptations related to which individual would call and what phone would be used. Ultimately, the primary provider calls families when approaching the room using a secure mobile application which displays the hospital phone number on the receiving phone. The provider briefly explains the reason for the call after which they proceed with the rounding encounter as usual with the family on speakerphone. A script was also developed for providers to leave a voicemail if the family does not answer.
Scheduling interpreters, when needed, was introduced as another intervention to improve family presence and participation. Patients requiring interpreters are flagged at an evening huddle and the charge nurse, who also makes the rounding schedule, places a request through interpreter services. We utilise in-person interpreters when able, as this is associated with improved caregiver satisfaction during family-centred rounds. Reference Anttila, Rappaport, Tijerino, Zaman and Sharif10,Reference Kosack, Carson and Montenegro14
Interventions to improve family participation:
Historically, nurses initiated rounding encounters followed by the frontline provider presentation, after which families had the opportunity to ask questions. To better align with standard, accepted approaches for family-centred rounds Reference Destino, Shah and Good3 and to improve family participation, we restructured rounding encounters to have families open rounds. This intervention also required small adaptations. Initial attempts often resulted in families being asked to open rounds with closed ended questions such as “How did the night go?” which did not achieve the true aim of family participation. Additional instruction was provided for nurse practitioners around using open-ended, non-threatening questions such as “What concerns do you have?” or “What is on your mind today?”, improving family participation.
Contextual considerations
No concurrent initiatives were felt to impact family presence or participation. A new building opened during the project splitting patients between two physical units (though still cared for by the same team and not changing rounding structure). Changes in unit leadership and staffing occurred throughout the project with a new medical director, new nursing manager, significant turnover in bedside nurses, and turnover in the nurse practitioner group. Floating bedside nurses received just-in-time education on rounding processes. Heart failure/transplant team census fluctuation sometimes impacted the start time of general cardiology rounds.
Study of intervention, measures, and analysis
Family presence, participation, and census were counted manually during baseline and testing periods by a team member who observed rounds while all attendings were on service. Our process measure, percent family presence was calculated by dividing the number of encounters for which family presence was positive by the total number of rounding encounters. Our outcome measure, percent family participation was calculated by dividing the number of encounters during which families participated by the number of encounters during which families were present. Data were visualised using p-charts charts with annotation of introduced plan-do-study-act ramps and relevant contextual information. We assessed for signs of special cause variation using standard rules and examined the relationship between variation and interventions. Reference Benneyan, Lloyd and Plsek15 Using median and interquartile ranges for the general cardiology team census, we created a definition for high census and created control charts for family presence and participation during times of high census. Throughout the process, we used qualitative data through verbal feedback from members of the rounding team and families to assess the impact of interventions on staff and family satisfaction and assess for unintended consequences.
Several balancing measures were considered. We hypothesised rounds might be prolonged with increased family participation; however, duration of rounds was not measured. This was partly due to challenges with data collection and partly because we did not consider this a sufficiently negative outcome that would prevent adoption of improved family-centred rounds. Prolongation of rounds related to family participation may inconvenience the medical team but has also been thought of as an investment with the dividends being improved communication with families and nursing, resulting in fewer clarifications throughout the day. Reference Muething, Kotagal, Schoettker, Gonzalez del Rey and DeWitt16 Instead, we asserted that delays in patient care and flow due to prolonged rounds would be unacceptable. Therefore, we used time of arrival on our unit for patients transferring from the ICU as well as hospital length of stay as our balancing measures. We used X-MR charts to monitor time of transfer and length over the project period.
Ethical considerations
The institutional review board determined that the project was exempt from review.
Results
Baseline data reflecting 71 days of pre-intervention rounding revealed mean family presence of 43% and mean family participation of 81% (Fig 1). During high census days, baseline mean family presence was 37% and baseline mean family participation was 70% (Supplemental Figure 2).

Fig. 1 Statistical control charts of process and outcome measures. Panel A demonstrates two occurrences of special cause variation in percent families present for rounds; the first occurring shortly after education related to family-centered rounds was provided for nurse practitioners and attendings and the second after the secure calling application was installed on nurse practitioner phones. Panel B shows one instance of special cause variation which occurred following education to providers.
Process and outcome measures
During the project, family presence increased to a mean of 83% and family participation increased to a mean of 96%. There were two instances of special cause variation in family presence during the project period, each meeting criteria of having 8 consecutive points above the prior centreline of the p-chart. The first instance of special cause variation in family presence occurred after the education intervention, with the mean increasing from 43 to 66%. The second instance of special cause variation occurred after introduction of the interventions to call families and schedule interpreters, resulting in a further increase in mean family presence to 83%. Special cause variation occurred once for family participation, corresponding temporally to the education intervention. During the project, family presence increased to a mean of 83% and family participation increased to a mean of 96%. There were two instances of special cause variation in family presence during the project period, each meeting criteria of having 8 consecutive points above the prior centreline of the p-chart. The first instance of special cause variation in family presence occurred after the education intervention, with the mean increasing from 43 to 66%. The second instance of special cause variation occurred after introduction of the interventions to call families and schedule interpreters, resulting in a further increase in mean family presence to 83%. Special cause variation occurred once for family participation, corresponding temporally to the education intervention.
High census subanalysis
Median census during the project period was 13 (interquartile range 11–15). There were 26 days with census greater than 15 (range 16–21) which were deemed high census days. When assessing only high census days, family presence and participation both improved (37–61 and 70–93% respectively), though family presence notably did not improve to the same level as all census days (Supplemental Figure 2). Both family presence and family participation had special cause variation but, interestingly, timing of the improvement preceded introduction of interventions.
Balancing measures
There was no change in time of transfer or length of stay between the baseline period and testing periods (Fig 2).
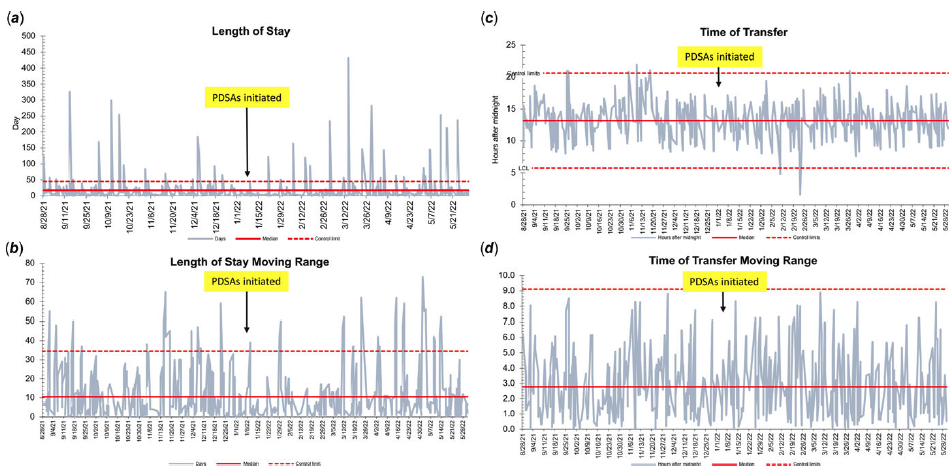
Fig. 2 Statistical control charts of balancing measures included in project. Panels A and B show no special cause variation in length of stay or in the moving range of length of stay. Panels C and D show no special cause variation in time of transfer from the intensive care unit or in the moving range of time of transfer.
Discussion
With this work, we demonstrate how a multidisciplinary team can utilise quality improvement methodology to significantly increase family presence and participation in daily rounds on a paediatric acute care cardiology unit. Education on family-centred rounding, alignment with institutional practice, and use of technology to virtually connect families with the care team were leveraged to achieve this improvement. Even during times of high census, family presence and participation improved. There were no significant care delays noted, with time of transfer and length of stay remaining stable throughout the improvement period.
Family-centred rounding is associated with improved clinical outcomes and improved family and staff experience, but it also has limitations including concerns related to duration of rounds. Reference Destino, Shah and Good3 We used length of stay as a balancing measure due to concern that prolonged rounds could delay appropriate patient care and subsequently increase length of stay. However, some theorise that family-centred rounds could actually shorten length of stay through improved communication with patients related to anticipated discharge timing, education, durable medical equipment training, and other aspects of transition to home. Reference Christianson, Kalinowski and Bauer17–Reference Wrobleski, Joswiak, Dunn, Maxson and Holland19 Christianson et al. showed no change in length of stay when incorporating increased discussion of discharge criteria during family-centred rounds, while Oshimura et al. found a modest reduction in length of stay from pre to post family-centred rounds eras at their institution. Wrobleski et al. found that patients who had a family-centred approach to discharge planning were less likely to contact healthcare providers, visit the emergency department, or require readmission because of unexpected complications. These studies demonstrate that benefits of family-centered rounds may extend beyond rounding encounters and even beyond acute hospitalisation.
Benefits of family-centred rounds should be distributed equitably. We included interventions specifically designed to achieve family presence for families with barriers to being at the bedside during daily rounds, some of which are known social determinants of health. Reference Lopez, Baker-Smith and Flores20 Social determinants of health continue to impact children with heart disease; improved outcomes have not been achieved uniformly and systemic and institutional practices reinforce inequity. Reference Davey, Sinha, Lee, Gauthier and Flores21,Reference Demianczyk, Behere and Thacker22 Intuitively, families with economic and/or housing instability, limited education and/or literacy, fewer community and family support structures in place, and a myriad of other social determinants of health are less able to remain at a hospitalised child’s bedside and engage with a rounding medical team. In general paediatrics, Black, Latinx, and caregivers of colour experience barriers to inclusion in family-centred rounds relative to White caregivers. Reference Parente, Stark and Key-Solle11 By including interventions such as improved utilisation of interpreters during rounds and calling families unable to be at bedside due to challenges with transportation, inability to have time away from work, or being a caregiver for someone other than the admitted child, we are attempting to address some of the institutional inequity that has existed in the rounding process.
Improvement efforts utilising low-reliability interventions, such as the ones we employed, are particularly vulnerable to failure. Reference Resar23 Therefore, we chose to monitor our system during times of stress, which we defined as high census. When unit-based pressures are high, low-reliability interventions, such as calling families not at bedside, may be more cumbersome. Such pressures likely contribute to the low baseline rates of family presence and participation during high census compared to normal census. Interestingly, the improvement in our measures on high census days occurred prior to interventions, possibly due to the Hawthorne effect as rounding team members were aware of baseline data collection and the project. Reliable, equitable interventions to engage families even during periods of high census are needed.
A clear next step in improving family presence on rounds is family-facing communication surrounding the timing of their rounds. Rounding schedules improve family presence in acute care cardiology. Reference Kipps, Albert, Bomher, Cheung, Feehan and Kim5 Schedule-based rounding also improves nursing presence, a tenet of family-centred rounds. Reference Khan, Spector and Baird2,Reference Destino, Shah and Good3,Reference Kipps, Albert, Bomher, Cheung, Feehan and Kim5 Implementation of schedule-based rounding requires workflows that, unfortunately, could not be supported in the course of this work. Unit leadership is currently testing technology solutions that allow implementation of schedule-based rounding and further facilitate telehealth options for families not at bedside. Family participation has not been assessed with schedule-based rounding, but our data suggest improved family presence, in and of itself, facilitates family participation. Technology solutions for schedule-based rounds would also have higher level of reliability and likely facilitate sustained improvement. Reference Weick and Sutcliffe24
There are limitations to the generalisability of this work. Institutional variation surrounding rounding practices and the lack of clear definitions complicate implementation of family-centred rounds. Reference Destino, Shah and Good3 Other institutions may not have existing systems to support interventions designed to improve family presence and participation. Regional variation may also challenge certain interventions. Hospitals caring for more families requiring interpreters may experience larger impact on rounding processes by utilising interpreters during rounds, though these hospitals may also have more robust interpreter services. Reference Kosack, Carson and Montenegro14 We did not measure how many patients required use of interpreter services at baseline or after interventions. Additionally, changes we experienced in unit staffing may also limit generalisability. As new personnel were onboarded, it was challenging to provide ongoing education, but these providers did not have entrenched practices and may have been more open to change. Incorporation of new tasks related to project interventions may have felt stressful to some team members. We did not formally measure the impact of our work on provider stress but acknowledge that changes to longstanding processes can be difficult. Lastly, it remains to be seen whether we will sustain these improvements, particularly as we relied upon relatively low level of reliability interventions.
Conclusions
Within a paediatric acute care cardiology environment, we increased both family presence and participation during daily rounds without major negative unintended consequences. Other subspecialty and cardiology environments, such as the cardiac ICU, may also be able to improve family participation in rounds, consistent with the gold standard for inpatient paediatric rounds. Improving family-centredness of rounds may be an avenue for institutions to address social determinants of health and systemic issues that continue to fuel inequity and differential outcomes. Future work is needed on our unit to increase the reliability of our interventions and thus sustain our improvement.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951123001063.
Acknowledgements
Special thanks to the Intermediate Improvement Science Series offered by Cincinnati Children’s Hospital, James M. Anderson Center for Health Systems Excellence, and Sheryl Bloomer for assistance in this project.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interest
None.




