



Introduction
Individuals who are exposed to natural disasters have a higher likelihood of reporting posttraumatic stress disorder (PTSD; Cénat et al., Reference Cénat, McIntee and Blais-Rochette2020; Chen et al., Reference Chen, Qi, Ke, Qiu, Xu, Zhong, Lu and Chen2022), especially children and adolescents, in whom the prevalence ranges from 8.4% to 32.9% (Shi et al., Reference Shi, Zhou, Geng, Li, Zhou, Lei, Chen, Chen and Fan2018). Extensive research has focused on interventions for children with PTSD from the perspective of individuals, social groups, and schools (Zhou, Reference Zhou2020). However, in some children, PTSD symptoms persist or increase over time following disasters (Lai et al., Reference Lai, Lewis, Livings, Greca and Esnard2017). This may be attributed to the lack of interventions focused on families, which are important for children’s recovery following traumatic events because parental trauma exposure can have detrimental consequences for children (Hartzell et al., Reference Hartzell, Stenson, van Rooij, Kim, Vance, Hinrichs, Kaslow, Bradley and Jovanovic2022; Narayan et al., Reference Narayan, Lieberman and Masten2021). Therefore, posttrauma assistance for children may be limited if parents’ trauma-related outcomes are not considered, especially for families that experience traumatic events simultaneously. Recent research has revealed that parental PTSD adversely affects children’s PTSD (O’Toole, Reference O’Toole2022). However, previous studies have focused primarily on the overall level of PTSD (Shi et al., Reference Shi, Zhou, Geng, Li, Zhou, Lei, Chen, Chen and Fan2018; Zhou & Zhen, Reference Zhou and Zhen2022), which may lead to non-precise interventions because of the loss of important information due to treating all PTSD symptoms equally (Bartoszek et al., Reference Bartoszek, Hannan, Kamm, Pamp and Maieritsch2017). Thus, to promote targeted clinical interventions for children who develop PTSD following trauma, it is necessary to examine the association between parents’ PTSD symptoms and children’s PTSD symptoms.
Previous studies on the association between PTSD in parents and children have reported a sex difference between mothers and fathers. For instance, the intergenerational link between PTSD among mothers and children is stronger than that among fathers (Lehrner et al., Reference Lehrner, Bierer, Passarelli, Pratchett, Flory, Bader, Harris, Bedi, Daskalakis, Makotkine and Yehuda2014). Some studies have indicated that PTSD in fathers does not influence PTSD in children (Zerach et al., Reference Zerach, Levin, Aloni and Solomon2017), whereas others have posited that fathers’ PTSD increases the risk of their children developing PTSD (O’Toole et al., Reference O’Toole, Burton, Rothwell, Outram, Dadds and Catts2017). The same-sex matching effect model suggests that fathers and mothers have a greater influence on the developmental outcomes of their children of the same sex (Zou et al., Reference Zou, Wu and Li2020). For instance, Di Maggio and Zappulla (Reference Di Maggio and Zappulla2014) reported that fathers’ strictness was associated with internalizing problems and general satisfaction in boys but not girls, while Cross et al. (Reference Cross, Kim, Vance, Robinson, Jovanovic and Bradley2016) found that mothers who had experienced childhood sexual abuse showed a greater degree of emotional numbing and distance with respect to daughters but not sons. Moreover, Andersson (Reference Andersson2016) also found that fathers’ warmth during childhood was more significant for male adulthood health, and mothers’ warmth was more important to female adulthood health. On the basis of these findings, we hypothesized that mother’s PTSD symptoms could predict daughters’ PTSD symptoms and that father’s PTSD symptoms could predict sons’ PTSD symptoms.
The mechanism by which parents’ PTSD symptoms predict children’s PTSD symptoms is underexamined, although a large number of studies have indicated an association. In attempts to clarify this mechanism, previous studies have suggested several possible underlying factors. One factor is related to children’s sense of security. PTSD symptoms in parents can influence how they interact with their children (Jensen et al., Reference Jensen, Sezibera, Murray, Brennan and Betancourt2021; Monn et al., Reference Monn, Zhang and Gewirtz2018). For instance, parents with emotional numbing or behavior avoidance are likely to be less emotionally engaged and less expressive with their children (Sherman et al., Reference Sherman, Gress Smith, Straits-Troster, Larsen and Gewirtz2016). Moreover, parents with symptoms of negative cognitive and emotional alterations (NCEA) have negative cognitions regarding the world (Deng, Reference Deng2016), which are shown unconsciously during the communication process with their children, while parents with hyperarousal symptoms tend to overreact to their child’s behaviors (Sherman et al., Reference Sherman, Gress Smith, Straits-Troster, Larsen and Gewirtz2016) or display verbal or physical aggression toward their child (Taft et al., Reference Taft, Kaloupek, Schumm, Marshall, Panuzio, King and Keane2007). These interactive behaviors may affect a child’s sense of security because their family environment may unsafe, and they may begin to distrust other people and the world. A low sense of security can lead children to feel unsafe, less in control, and to have a decreased sense of belonging. In turn, this may trigger traumatic memories, an increase in negative beliefs, the avoidance of trauma-related stimuli, or overreactions concerning individual safety (Quan et al., Reference Quan, Zhen, Yao and Zhou2020), which can eventually lead to intrusion, avoidance, NCEA, and hyperarousal symptoms of PTSD. Thus, parental PTSD symptoms may exert a detrimental prediction on children’s PTSD symptoms via a lowered sense of security in children.
Another potential factor is related to catastrophization, which is a negative cognitive emotion regulation strategy in which previously experienced threatening or stressful life events are emphasized (Garnefski & Kraaij, Reference Garnefski and Kraaij2006). Individuals who catastrophize exaggerate their negative perceptions and cognitions of traumatic events. Parents with PTSD symptoms may experience considerable internal conflicts with previous belief systems because of shattered world assumptions, which can result in negative hypotheses regarding the worth of themselves, others, and the world (Janoff-Bulman, Reference Janoff-Bulman2010). For example, parents with intrusive and negative cognitions may find it difficult to stop thinking about traumatic events in a negative way, such as how worse the disaster is (Deng, Reference Deng2016). Moreover, parents who overreact to their surroundings may fear losing cognitive control (Kwon et al., Reference Kwon, Lee and Lee2021), which can result in negative appraisal and thoughts regarding the surrounding environment. Such negative thinking and cognitive appraisal of traumatic events by parents may be accepted and internalized by their children during parent–child interactions, which can contribute to catastrophization in the children (Neville et al., Reference Neville, Soltani, Pavlova and Noel2018). According to the cognitive model of PTSD (Ehlers & Clark, Reference Ehlers and Clark2000), the negative appraisal of traumatic events or their sequelae maintains a sense of persistent threat and can lead to subsequent threats of intrusions, arousal symptoms, and strong emotions. Specifically, thoughts such as, “bad things always happen to me,” can promote avoidance of particular situations or scenarios, and these continuous thoughts can serve as cues for children to recall traumatic events, which give rise to intrusion symptoms of PTSD (Ehlers & Clark, Reference Ehlers and Clark2000). Thoughts such as, “nowhere is safe,” or “how horrible it is to experience a disaster,” may heighten an individual’s vigilance regarding their surroundings and thus increase hyperarousal symptoms. Furthermore, catastrophizing thoughts can contribute to an individual’s overestimation of future threats, which can then facilitate the formation of negative beliefs (Gellatly & Beck, Reference Gellatly and Beck2016), resulting in NCEA symptoms. In light of the above findings, we predicted that parental PTSD symptoms would predict children’s PTSD symptoms by increasing catastrophization in children.
Children’s sense of security and catastrophization are possible mechanisms that may mediate the prediction of PTSD symptoms from parents to children. However, to date, their potential multiple mediating roles have been overlooked, despite the importance in establishing a broader theoretical framework. Therefore, in the present study, we focused on the multiple mediating roles of the sense of security and catastrophization. Individuals with a higher sense of security are more likely to seek help from others and to have greater courage and energy to cope with existing negative thoughts compared with those with a lower sense of security (Quan et al., Reference Quan, Zhen, Yao and Zhou2020). This can facilitate discussions with others, new insights, and the reconstruction of past appraisals (Zhen et al., Reference Zhen, Quan and Zhou2018), which may relieve catastrophizing thoughts. In contrast, a poor sense of security may aggravate catastrophization. Therefore, we also supposed that parental PTSD symptoms would positively predict children’s PTSD symptoms via a decreased sense of safety and amplification of catastrophization in children. Because of the supposed same-sex prediction from parents to children above, we assessed the mechanism among parent–child dyads.
The literature reviewed above indicates a prediction of PTSD symptoms from parents to children. However, in previous studies, this association was examined primarily using the total PTSD score (Shi et al., Reference Shi, Zhou, Geng, Li, Zhou, Lei, Chen, Chen and Fan2018; Zhou & Zhen, Reference Zhou and Zhen2022), which limits precise interventions (Bartoszek et al., Reference Bartoszek, Hannan, Kamm, Pamp and Maieritsch2017). Moreover, a considerable number of relevant studies focused mainly on families who had experienced the holocaust or war (O’Toole, Reference O’Toole2022). Thus, it remains unclear whether these previous findings can be applied to entire families affected by natural disasters (Marshall et al., Reference Marshall, Kuijer, Simpson and Szepsenwol2017). Moreover, the potential same-sex matching effect has not been explored in terms of different PTSD symptoms among parent–child dyads. In addition, whether the multiple mediating roles of the sense of security and catastrophization can be used to predict matching of parents’ PTSD symptoms and children’s PTSD symptoms is unknown.
To address this, we examined the same-sex matching effect in terms of the predictive paths from parents’ PTSD symptoms to those in their children by first comparing predictions among parent–child dyads (i.e., father–son, father–daughter, mother–son, and mother–daughter), and then examining the mediating role of children’s sense of security and catastrophization following Super Typhoon Lekima, using a longitudinal study design. Given the theoretical and empirical evidence discussed above, we predicted that the same-sex matching effect would be present for all predictive paths from parental PTSD symptoms to children’s PTSD symptoms by children’s sense of security and catastrophization, particularly among mother–daughter and father–son dyads.
Method
Participants and procedure
Super Typhoon Lekima occurred in China in August 2019. It affected 14.024 million people, caused 57 deaths and 14 disappearances, and resulted in an economic loss of CNY 53.72 billion (approximately 8416 million USD). In this study, we focused on Wenling city, which is located in the southeast of Zhejiang province. This coastal city, which faces the sea on three sides, was the center of Super Typhoon Lekima. The maximum wind force near the center was 16 level when the storm landed, and the city was directly and severely affected. Roads were blocked, water and electricity were cut off in large areas, and houses were severely damaged when the typhoon landed in Wenling. The study process was approved by the Research Ethics Committee of Department of Psychology and Behavioral Sciences, Zhejiang University, and was conducted 3 months and 15 months after the typhoon. To recruit parents and children, we requested assistance from educational agencies and informed them of our aims and the longitudinal design. Finally, two middle and high schools were selected for convenience sampling. With the help of the school teachers, all students in grades 7, 8, 10, and 11 (students in grades 9 and 12 did not participate because they were studying for their entrance examination) completed a self-report questionnaire in their classroom on the assessment date, with the supervision of trained psychology postgraduate students. The study purpose and voluntary nature of participation were highlighted before the students completed the survey. Written informed consent was obtained from all students and their guardians.
At the same time, the parents of the participating students also completed an electronic questionnaire, which was sent by teachers via WeChat (a free messaging and calling app widely used in China). The purpose of the study and voluntary nature of participation were explained in the recruitment information sent to the parents via WeChat, and written informed consent was obtained from parents who were willing to participate in the survey. All participants had access to psychological and counseling services via a family psychological service website, if required, following the completion of the questionnaire. A similar process was conducted for the second investigation.
A total of 1218 parent–child dyads completed the first assessment 3 months after Super Typhoon Lekima (T1, November 2019). The second assessment was conducted after an interval of 12 months (T2, November 2020). We matched data from T1 and T2 according to the school, grade, and class of the children, which resulted in 487 parent–child dyads who completed surveys at both timepoints. We removed data from divorced families to ensure a constant family situation, and focused on a single child within families. Finally, data from 447 parent–child dyads were included in the analysis. Of the 447 children, 44.1% (n = 197) were boys, and 55.9% (n = 250) were girls. The mean age was 13.40 years (standard deviation [SD] = 1.21 years). Of the 447 parents, 23.0% (n = 103) were fathers, and 77.0% (n = 344) were mothers. The mean age was 40.15 years (SD = 5.50 years), and 43 parents did not report their age. In terms of income, 149 (33.3%) families had a monthly income < 5,000 RMB, 187 (41.8%) had a monthly income of 5,000–10,000 RMB, and 111 (24.9%) had a monthly income ≥ 10,000 RMB. In terms of educational status, 95 (21.3%) parents had a primary school level education, 241 (53.9%) parents had a junior high school level education, and 111 (24.8%) parents had an educational level higher than senior high school. Finally, 161 (36.0%) parents had a single child, 265 (59.3%) had two children, and 21 (4.7%) had three children.
Measures
PTSD in parents and children
We assessed parental PTSD symptoms at T1 and children’s PTSD symptoms at T1 and T2 using a revised Chinese version (Zhou, Zhen, et al., Reference Zhou, Zhen and Wu2022 ) of the Weathers’ PTSD Checklist for the Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 (PCL-5; Weathers, Reference Weathers2013). The scale assesses the frequency of DSM-5 PTSD symptoms related to Super Typhoon Lekima and contains 20 items rated on a five-point scale ranging from 0 (not at all) to 4 (extremely). The scale assesses four symptoms: intrusion (5 items, e.g., “sad thoughts or images associated with typhoons pop into my mind”), avoidance (2 items, e.g., “I try not to remember, talk about, or feel emotions about the typhoon”), NCEA (7 items, e.g., “I feel emotional numbness, such as an inability to cry or cheer up”), and hyperarousal symptoms (6 items, e.g., “I feel restless or irritable”). In the current study, the scale had acceptable internal consistency (for parents at T1, Cronbach’s alphas were .870, .587, .874, and .892 for the intrusion, avoidance, NCEA, and hyperarousal subscales, respectively, and .956 for the entire scale; and those for children at T1/T2 were .788/.835, .539/.663, .801/.856, and .834/.885 respectively, and .919/.943 for the entire scale) and good construct validity (for parents at T1: χ 2(160) = 401.664, comparative fit index (CFI) = .926, Tucker–Lewis index (TLI) = .912, root mean square error of approximation (RMSEA) = .058, and standardized root mean residual (SRMR) = .044; for children at T1/T2: χ 2 (164/161) = 343.817/395.537, CFI = .910/.908, TLI = .896/.892, RMSEA = .050/.057, and SRMR = .061/.073). According to the DSM-5 diagnostic criteria for PTSD, children with a PTSD score ≥ 31 were considered to have probable PTSD (Foa et al., Reference Foa, Asnaani, Zang, Capaldi and Yeh2018), and adults with a PTSD score ≥ 34 were considered to have probable PTSD (Yang et al., Reference Yang, Wu, Gao, Wang, Quan and Zhou2020).
Children’s sense of security
We assessed the children’s sense of security at T1 and T2 using the modified Perceived Security Questionnaire (Quan et al., Reference Quan, Zhen, Yao and Zhou2020). It was developed by Liu et al. (Reference Liu, Tang, Zhang, Deng, Lei and Liu2009) according to the definition of Maslow and other questionnaires about security, and sense of security here involved sense of life safety, belonging, and control. The scale contains three corresponding subscales: sense of life security (4 items, e.g., “I am willing to continue living where I am”), sense of belonging (3 items, e.g., “I trust the people around me”), and sense of control (3 items, e.g., “We can rebuild our homeland by ourselves”). The 10 questionnaire items are rated on a five-point scale ranging from 1 (completely disagree) to 5 (completely agree). The scores for item 2, 4, and 10 were inverted. We used the total score, with a higher score indicating a higher sense of security for children. The questionnaire exhibited good reliability (Cronbach’s alpha = .836/.847 at T1/T2) and good construct validity (χ 2 (29/29) = 44.109/68.294, CFI = .988/.971, TLI = .982/.956, RMSEA = .034/.055, and SRMR = .027/.028 at T1/T2) in this study.
Children’s catastrophization
We assessed children’s catastrophization at T1 and T2 using a subscale of the Cognitive Emotion Regulation Questionnaire (Garnefski et al., Reference Garnefski, Kraaij and Spinhoven2002), which comprises 4 items (e.g., “I often think about how terrible what I have experienced is”). The items are rated on a five-point scale ranging from 0 (never) to 4 (always). A higher score indicates a higher level of catastrophizing cognitive coping. The scale exhibited good reliability (Cronbach’s alpha = .921/.947 at T1/T2) and good construct validity (χ 2 (2/2) = 6.013/3.720, CFI = .990/.994, TLI = .969/.983, RMSEA = .067/.044, and SRMR = .009/.010 at T1/T2) in the current study.
Data analysis
We used Little’s missing completely at random test to assess the randomness of missing data. The results showed that data were missing in a non-random way (χ 2 (91) = 125.188, p = .01); therefore, the data were handled using robust maximum likelihood estimates. To examine sex differences in long-term predictions of children’s PTSD symptoms by parents’ PTSD symptoms, we divided the data into four groups: father–son (n = 49), father–daughter (n = 54), mother–son (n = 148), and mother–daughter (n = 196) dyads. A single-group direct effect model was established to test the long-term prediction of children’s PTSD symptoms from parents’ PTSD symptoms for each group, using Mplus 8.0 (Muthén & Muthén, Reference Muthén and Muthén2017). Then, we used a multi-group model comparison to examine the statistical differences between mother–daughter dyads and other dyads.
Because of the limited sample size for the subgroups, we used the bootstrap method for all models, with 5,000 replications for more accurate results (Shrout & Bolger, Reference Shrout and Bolger2002). A 95% bootstrap confidence interval (CI) was used to examine the significance of path coefficients, instead of a p value. A path was considered significant if the 95% CI did not include 0. Moreover, given that the children in our study were nested in classes, we used the CLUSTER option to perform clustering by class. χ 2, CFI, TLI, RMSEA, and SRMR were used to evaluate the model fit. The cutoffs for the model indices were ≥ .90 for the CFI and TLI, and < .08 for the RMSEA and SRMR (Wen et al., Reference Wen, Hou and Marsh2004). We did not control for demographic variables (e.g., family income, parental education) in these models because they showed no significant differences in terms of the main variables (F (2, 193) = .09–3.14, p S > .05).
According to the results of the direct effect models for the four groups, we only used the data for the mother–daughter group in the subsequent analysis. Descriptive statistics and Pearson’s correlation analysis were conducted to calculate the means, SDs, and associations between the major variables (i.e., mothers’ PTSD symptoms at T1, and daughters’ PTSD symptoms, sense of security, and catastrophization at T1 and T2). We then built a multiple indirect effect model that included daughters’ sense of security and catastrophization at T2 according to mothers’ PTSD symptoms at T1 and daughters’ PTSD symptoms at T2, after controlling for daughters’ sense of security, catastrophization, and PTSD at T1. In addition, we added a path from daughters’ sense of security at T2 to catastrophization at T2. To avoid type-I errors, we combined the correlation paths within the four PTSD symptoms for mothers and daughters respectively.
Results
Direct prediction from parental PTSD symptoms to children’s PTSD symptoms
Based on the cutoff scores for adults and children, the prevalence of PTSD in fathers at T1, mothers at T1, sons at T2, and daughters at T2 was 14.6% (n = 15), 19.2% (n = 66), 10.7% (n = 21), and 14.8% (n = 37), respectively. We built a single-group direct effect model to test the predictive value of parental PTSD symptoms on children’s PTSD symptoms according to the different sex dyads (i.e., father–son, father–daughter, mother–son, and mother–daughter). All models showed good fit indices (χ 2 (0) = .00, CFI = 1.000, TLI = 1.000, RMSEA = .000 [90% CI: .000–.000], SRMR = .000). The results of the path analysis showed that the path coefficients for the father–son, father–daughter, and mother–son dyads were all non-significant (see Supplemental Materials Figure S1–S3), and only mothers’ PTSD symptoms significantly predicted daughters’ PTSD symptoms (Figure 1). Specifically, mothers’ intrusion symptoms positively predicted daughters’ intrusion (β = .38, bootstrap 95% CI [.06, .69]), avoidance (β = .40, bootstrap 95% CI [.10, .68]), and hyperarousal symptoms (β = .28, bootstrap 95% CI [.01, .54]); mothers’ avoidance symptoms positively predicted daughters’ avoidance symptoms (β = .27, bootstrap 95% CI [.06, .50]); and mothers’ hyperarousal symptoms negatively predicted daughters’ hyperarousal symptoms (β = −.34, bootstrap 95% CI [−.65, −.05]).
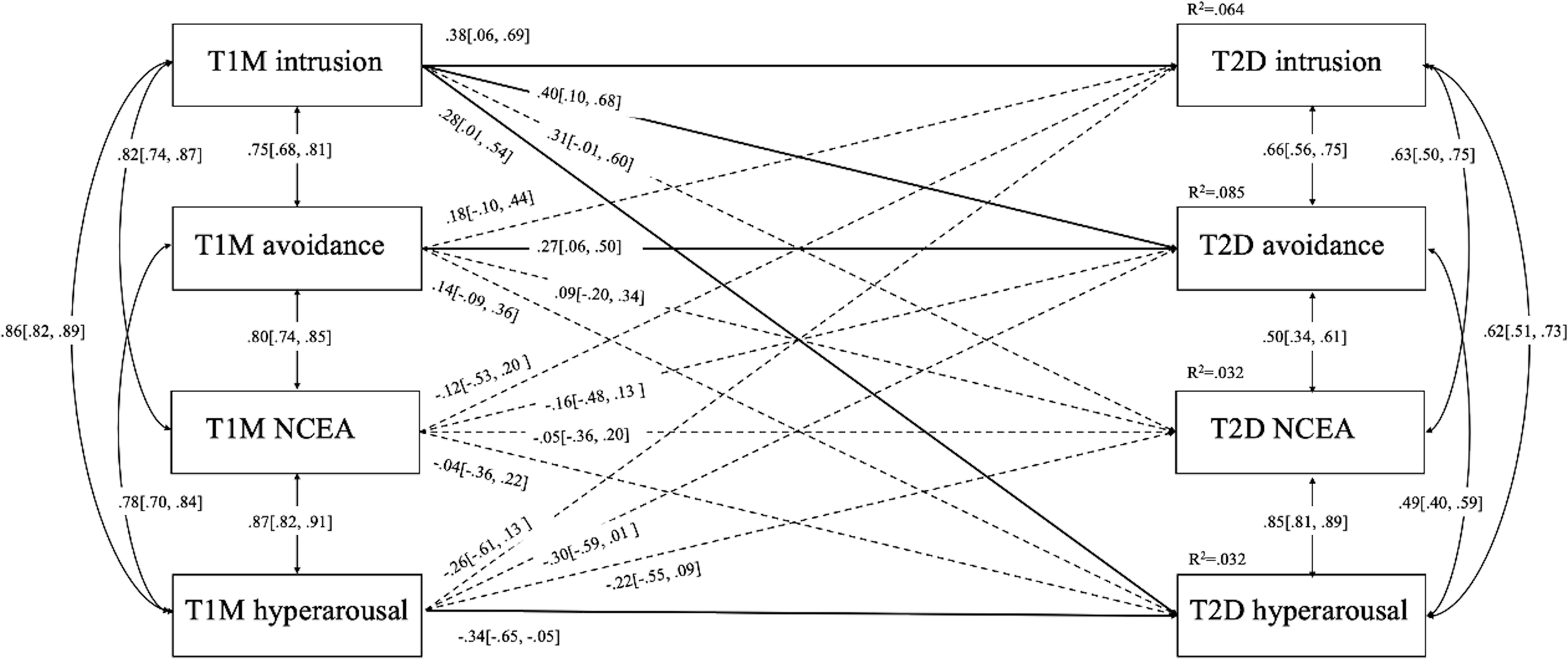
Figure 1. Direct Model for Mother–Daughter Dyads. Note. NCEA = negative cognitive and emotional alterations; M = Mother, D = Daughter; bootstrap 95% CI showed in the brackets; all parameters are standardized.
Next, we conducted a multi-group model comparison, wherein we generated a structural invariance model to compare the mother–daughter dyad with the other dyads using the MODEL TEST command (constraining the same path coefficients equally; Wang & Wang, Reference Wang and Wang2019). The Wald test showed a significant difference between the following groups: χ 2 = 33.22, df = 16, p = .007 for the mother–daughter dyad versus the mother–son dyad; χ 2 = 49.54, df = 16, p < .001 for the mother–daughter dyad versus the father–son dyad; χ 2 = 55.15, df = 16, p < .001 for the mother–daughter dyad versus the father–daughter dyad. The results indicated that there were sex differences in the predictive value of parental PTSD symptoms on children’s PTSD symptoms, such that only mothers’ PTSD symptoms predicted daughters’ PTSD symptoms.
Descriptive statistics and correlations between the main measures for mother–daughter dyads
Table 1 shows the descriptive statistics and correlations between mothers’ PTSD symptoms at T1 and daughters’ PTSD symptoms, sense of security, and catastrophization at T1 and T2. The results of the correlation analysis indicated that mothers’ intrusion and avoidance symptoms at T1 were significantly positively correlated with daughters’ intrusion and avoidance symptoms at T2 and catastrophization at T1; daughters’ sense of security at T1 and T2 was significantly negatively correlated with their own intrusion, avoidance, NCEA, and hyperarousal symptoms and catastrophization at T2, as well as the PTSD total score and catastrophization at T1; daughters’ catastrophization at T1 and T2 was significantly positively correlated with their own intrusion, avoidance, NCEA, and hyperarousal symptoms at T2, as well as the PTSD total score at T1; and daughters’ PTSD total score at T1 was significantly positively correlated with their own intrusion, avoidance, NCEA, and hyperarousal symptoms at T2. In addition, we found that the correlations within PTSD symptoms among mothers at T1 and daughters at T2 were positive respectively.
Table 1. Means, standard deviations, and correlations among the main variables for mothers and daughters
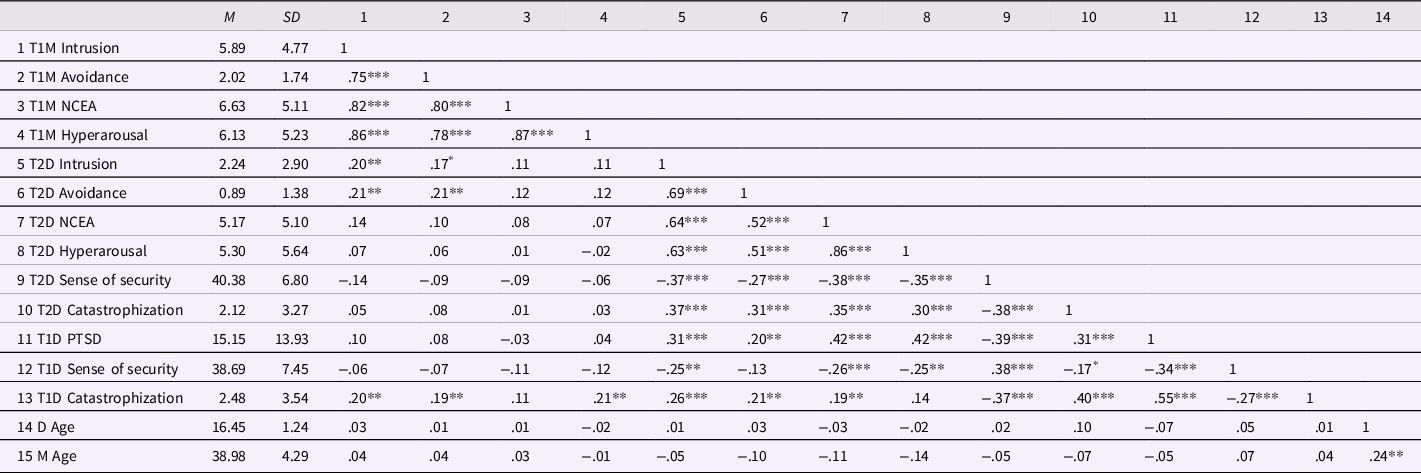
Note. NCEA = negative cognitive and emotional alterations, PTSD = posttraumatic stress disorder; M = Mother, D = Daughter;
* p < .05,
** p < .01,
*** p < .001.
Analysis of the indirect effect of mothers’ PTSD symptoms on daughters’ PTSD symptoms
According to the direct effect model of PTSD symptoms in mother–daughter dyad, we built an indirect effect model by adding daughters’ sense of security and catastrophization at T2 as mediating factors (Figure 2), after controlling for daughters’ sense of security, catastrophization, and PTSD at T1. The model had acceptable fit indices (χ 2 (15) = 45.67, CFI = .941, TLI = .774, RMSEA = .106 [90% CI: .072–.142], SRMR = .066). The results indicated that mothers’ intrusion symptoms at T1 indirectly positively predicted daughters’ NCEA and hyperarousal symptoms at T2 via daughters’ sense of security at T2, and indirectly positively predicted daughters’ four symptoms of PTSD at T2 via daughters’ sense of security at T2 and then daughters’ catastrophization at T2. Mothers’ hyperarousal symptoms at T1 indirectly negatively predicted daughters’ NCEA and hyperarousal symptoms at T2 via daughters’ sense of security at T2, and negatively indirectly predicted daughters’ four symptoms of PTSD at T2 via daughters’ sense of security at T2 and then daughters’ catastrophization at T2. The indirect path coefficients are shown in Table 2. Moreover, mothers’ avoidance symptoms at T1 directly positively predicted daughters’ avoidance symptoms at T2, but this was not via daughters’ sense of security or catastrophizing at T2. These results revealed that daughters’ sense of security and catastrophization played multiple mediating roles in the predictive value of mothers’ intrusion and hyperarousal symptoms for estimating daughters’ PTSD symptoms. The indirect effect of mothers’ intrusion and hyperarousal symptoms was the opposite.
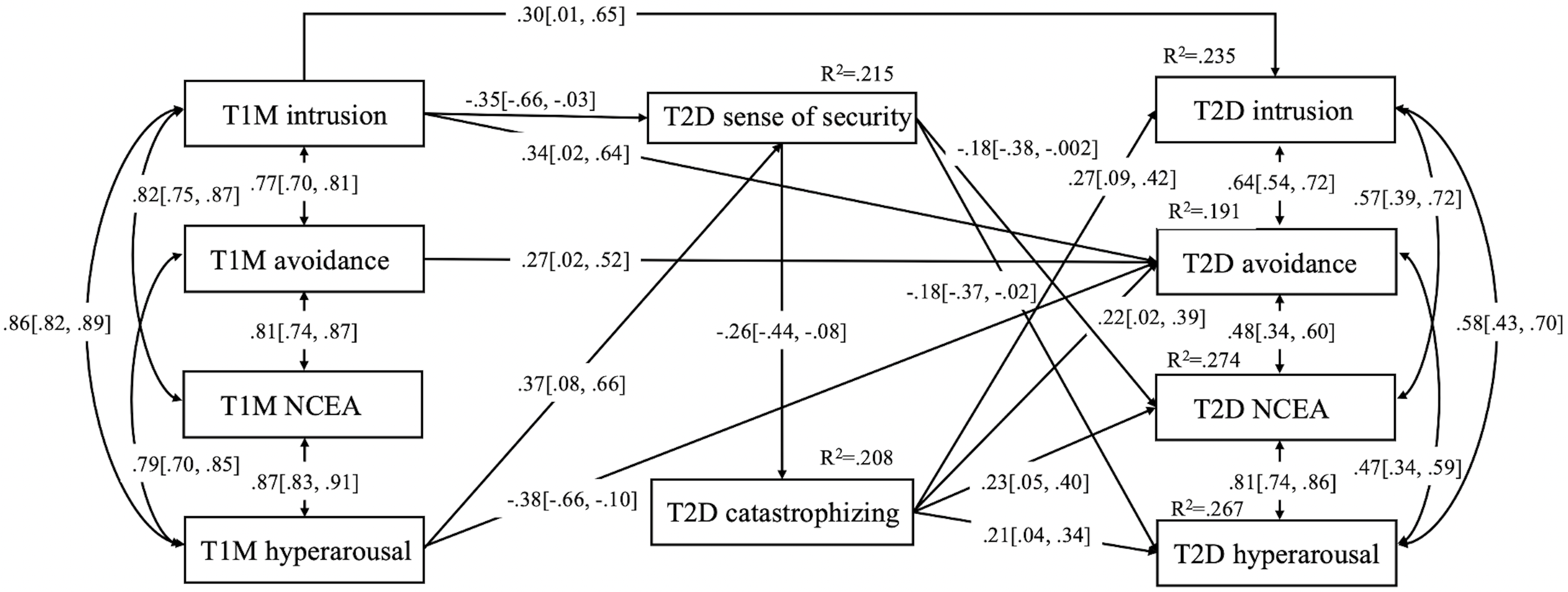
Figure 2. Mediation Model for Mother–Daughter Dyads. Note. NCEA = negative cognitive and emotional alterations; M = Mother, D = Daughter; the model has been controlled in terms of daughter’s sense of security, catastrophization, and PTSD at T1; bootstrap 95% CI showed in the brackets; all parameters are standardized.
Table 2. Bias-corrected bootstrap tests of the mediating effects for mother–daughter
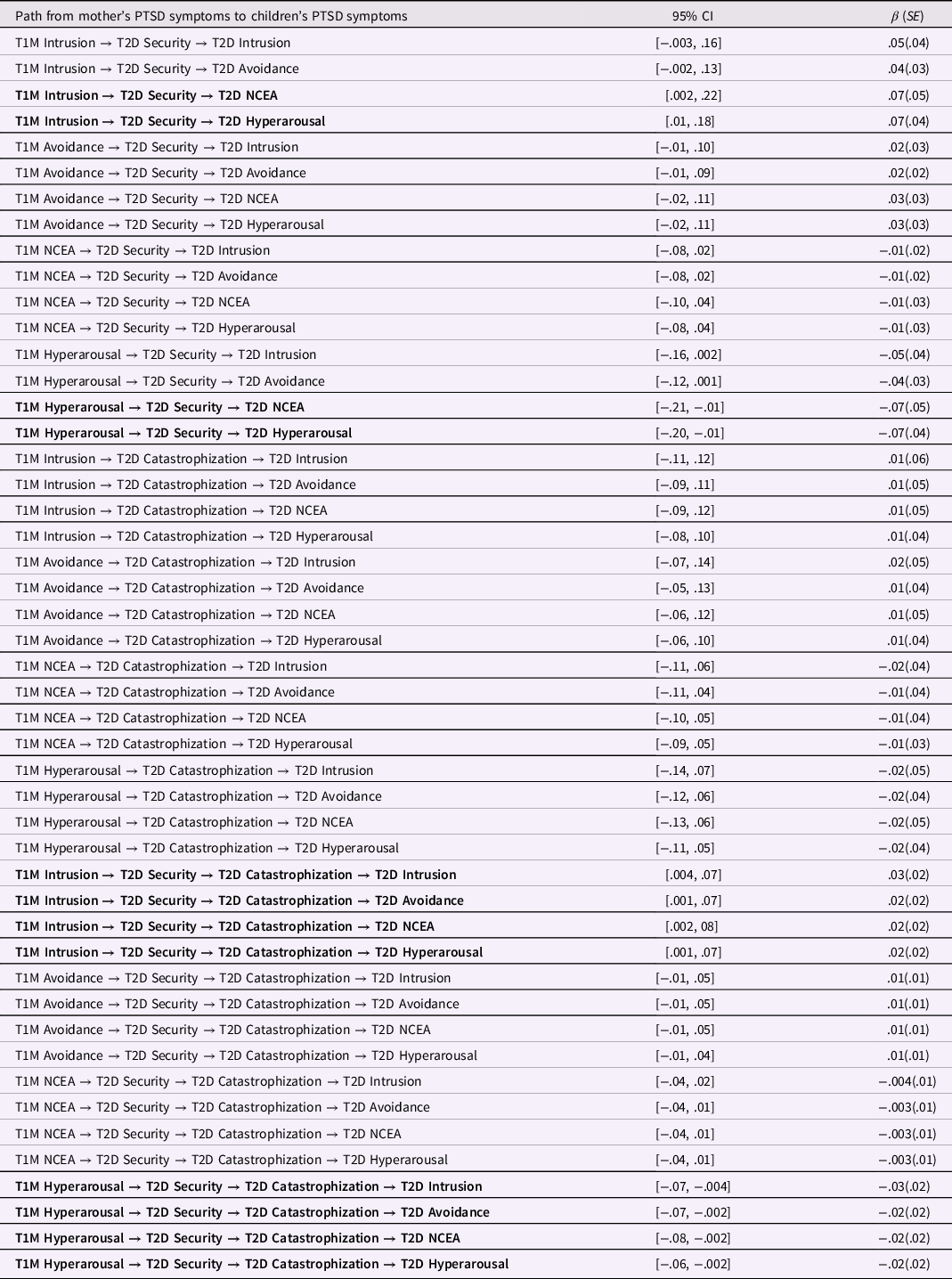
Note. NCEA = negative cognitive and emotional alterations; M = Mother, D = Daughter; If the 95% CI of the path coefficient does not include 0, the path is significant (shown in bold).
Discussion
This is the first longitudinal study to examine the same-sex matching effect in terms of the predictive value of parents’ PTSD symptoms for estimating children’s PTSD symptoms following Super Typhoon Lekima. We found that only mothers’ PTSD symptoms at T1 predicted daughters’ PTSD symptoms at T2. This long-term prediction was not observed in any of the other parent–child dyads. This finding suggests that there was a same-sex matching effect in the predictive value of parental PTSD symptoms for estimating children’s PTSD symptoms in females only. This may be attributable to the “strict mother, kind father” parenting style in China (Xu et al., Reference Xu, Liu, Li, Liu and Huntsinger2018). In subsequent analyses, we found that mothers’ intrusion and hyperarousal symptoms predicted daughters’ PTSD symptoms via daughters’ sense of security and catastrophization, the prediction of which showed the opposite effect. Mothers’ hyperarousal symptoms negatively predicted daughters’ PTSD symptoms, which could reflect Chinese cultural family dynamics. Specifically, in China, parental overprotection is perceived as an expression of caring for children (Xia et al., Reference Xia, Wang, Li, Wilson, Bush and Peterson2015). Thus, when mothers exhibit hyperarousal, and thus overprotective behaviors, daughters may feel less fear, panic, and hypervigilance with respect to the outside world, and have lower levels of catastrophization and PTSD symptoms because of an enhanced experience of security.
We found that the long-term prediction of specific PTSD symptoms was possible only in the mother–daughter dyad. This finding supports the same-sex matching effect among parent–child dyads (Zou et al., Reference Zou, Wu and Li2020) and expands this effect into PTSD symptoms, but only for females. This result may be attributed to sex differences in PTSD symptoms and differing parental roles in the family. A previous study found that girls were more likely to report PTSD symptoms than boys, even if they experienced the same type of traumatic event (Tolin & Foa, Reference Tolin and Foa2006). Thus, parental PTSD symptoms are more likely to predict PTSD symptoms in daughters versus sons because daughters are more likely to report PTSD symptoms. Mothers’ PTSD symptoms have also been more strongly related to children’s PTSD symptoms compared with fathers’ PTSD symptoms (Morris et al., Reference Morris, Gabert-Quillen and Delahanty2012). This may be because fathers are frequently less involved in parenting than mothers (Bastiaansen et al., Reference Bastiaansen, Verspeek and van Bakel2021). Given that they generally spend less time with their children, it is less likely that PTSD symptoms in fathers will influence their children. Moreover, the “strict mother, kind father” parenting style in China (Xu et al., Reference Xu, Liu, Li, Liu and Huntsinger2018), in which fathers limit displays of aggressive or conflictual behaviors towards children to maintain the “kind father” role, may limit the degree to which fathers’ PTSD symptoms transfer to children.
We discovered that higher levels of avoidance symptoms in mothers were associated with increased avoidance symptoms in daughters, and that higher intrusion in mothers was associated with higher intrusion, avoidance, and hyperarousal symptoms in daughters. This effect of avoidance symptoms could be attributed to similar behavior patterns between parents and children. Daughters may accommodate avoidance symptoms by facilitating avoidance behaviors because of mothers’ avoidance behaviors (Creech & Misca, Reference Creech and Misca2017). In terms of intrusion symptoms, mothers who have constant flashbacks and re-experience negative events may discuss their situation and related distress with their daughter. Such information may be stored in the daughter’s active memory and become intrusive memories (Joseph & Linley, Reference Joseph and Linley2005), activate stimuli-response connections, and decrease the sense of security regarding one’s surroundings, which could thus increase intrusion, avoidance, and hyperarousal symptoms in daughters.
Surprisingly, daughters whose mothers had higher hyperarousal symptoms showed fewer hyperarousal symptoms, which reflects the Chinese culture background. In China, parental control, such as overprotection and monitoring, is perceived as an expression of caring (Xia et al., Reference Xia, Wang, Li, Wilson, Bush and Peterson2015) and provides children with a greater sense of security. Mothers who have hyperarousal symptoms could be overprotective toward their daughters because they are hypervigilant about the surrounding environment. This could offer daughters a heightened sense of safety and reduce their fear of the surrounding environment, thus diminishing hyperarousal symptoms. Moreover, high feelings of safety may reduce the degree to which daughters negatively perceive the world, for example, reducing the sentiment that “nowhere is safe”, and thus decreasing vigilance regarding one’s surroundings.
When we added daughters’ sense of security and catastrophization to the direct model, we found that mothers’ intrusion and hyperarousal symptoms indirectly predicted daughters’ subsequent symptoms via daughters’ sense of security and catastrophization. Specifically, mothers’ intrusion symptoms positively predicted daughters’ NCEA and hyperarousal symptoms by decreasing daughters’ sense of security, and they predicted daughters’ four PTSD symptoms (i.e., intrusion, avoidance, NCEA, and hyperarousal symptoms) by decreasing daughters’ sense of security and then increasing daughters’ catastrophization. This may be attributed to the constant flashbacks and re-experiencing of the traumatic event induced by intrusion symptoms in mothers, which heightens their distress and hinders their ability to help and support their daughters to cope with disaster-related problems. Ultimately, this could reduce their daughters’ sense of security. Having a low sense of safety could increase daughters’ panic and hypervigilance with respect to their surroundings, which could lead to a hyperarousal state when exposed to trauma-related cues (Zhou, Huang, et al., Reference Zhou, Huang and Zhen2022). This lowered sense of security may heighten their fear of connecting with the outside world, which may lead to detachment and social alienation, resulting in the aggravation of NCEA. Furthermore, daughters with a decreased sense of security are likely to have a lower sense of control and belonging and to consider the world unsafe, which could increase their negative appraisal of the disaster and increase catastrophizing thoughts. According to the cognitive model of PTSD (Ehlers & Clark, Reference Ehlers and Clark2000), negative appraisal and thoughts about the disaster arouse cues to recall the traumatic event, generate vigilance regarding one’s surroundings, and contribute to the overestimation of future threats, which increases NCEA and intrusion, avoidance, and hyperarousal symptoms.
We found that mothers’ hyperarousal symptoms negatively predicted daughters’ NCEA and hyperarousal symptoms by increasing daughters’ sense of security alone, and they predicted daughters’ four symptoms by increasing daughters’ sense of security and then reducing catastrophization. Mothers with hyperarousal symptoms are likely to be more overprotective of their daughters because of hypervigilance. As mentioned, in China, this overprotective behavior is considered an expression of caring (Xia et al., Reference Xia, Wang, Li, Wilson, Bush and Peterson2015) and provides safety for daughters. This is likely to decrease daughters’ fear, panic, and hypervigilance with respect to the outside world and relieve NCEA and hyperarousal symptoms. Moreover, when daughters have a higher sense of security, they may be more courageous in expressing their feelings and thoughts, which could help with the acquisition of new insights through discussions with others (Zhen et al., Reference Zhen, Quan and Zhou2018) and the reduction of catastrophizing thoughts. In turn, this could weaken the connection between trauma-related cues and reactions (e.g., fear, flashbacks, and overreactions), reduce intrusion, avoidance, and hyperarousal symptoms, decrease negative cognitions regarding the disaster, and reduce NCEA symptoms.
This study has several limitations. First, it was difficult to avoid reporting bias because we used a self-report questionnaire to assess parents and children, as well as a chance of producing minuscule pseudo-significant results as we tested a large number of indirect effects in this study. Second, the study sample comprised parents and children exposed to a typhoon, which may limit the generalizability of our findings to other natural disasters. Unlike some other natural disasters such as earthquakes, typhoons can occur every year. Thus, victims may repeatedly be exposed to typhoons, which could affect the recovery of their sense of security and incur new PTSD symptoms. Third, we did not measure some variables that may influence the mediating effect, such as parenting behaviors, co-parenting. Thus, future studies could explore the mediating effects of the various variables from the perspective of families. Fourth, the inclusion of only one parent may not have captured a complete picture of entire families. It would be valuable to further examine the current findings using triadic mother–father–child data. Fifth, the study design, in which we conducted a one-time point assessment of parents and excluded the potential influence of subsequent typhoons, limited our ability to explore the bidirectional influence of parents and children, and to examine precise causal relationships. Future studies are needed to explore the bidirectional associations of PTSD symptoms in parents and children to obtain causal information, and to consider the potential influence of other natural disasters such as subsequent typhoons. Finally, although being in accordance with previous studies (e.g., Islam et al., Reference Islam, Ferdous, Sujan, Tasnim, Masud, Kundu, Mosaddek, Choudhuri, Kira and Gozal2022), the reliability of avoidance subscale in the PCL-5 is relatively low in this study because there are only two items on the avoidance symptom subscale.
Despite these limitations, we successfully examined sex differences in the predictive value of parents’ PTSD symptoms in estimating children’s PTSD symptoms following a typhoon. Our findings provide new and detailed insight regarding the PTSD symptoms from parents to children. We found that the same-sex matching effect from mothers to daughters was present for the intrusion and avoidance symptoms of PTSD but not the other two symptoms. Furthermore, this study shed light on the potential mechanism underlying the PTSD symptoms from mothers to daughters, and highlighted daughters’ sense of security and catastrophizing thoughts as key mediators. From a practical perspective, our findings suggest that addressing mothers’ PTSD symptoms is important for relieving daughters’ PTSD symptoms. Thus, clinical workers should consider the same-sex effect in females and directly manage mothers’ intrusion and avoidance symptoms to protect daughters from developing PTSD symptoms. Moreover, we revealed that daughters’ sense of security and catastrophizing thoughts play an important role in the predictive value of mothers’ PTSD symptoms for estimating daughters’ PTSD symptoms. Thus, interventions to improve daughters’ sense of security and reduce catastrophizing thoughts may be valuable in reducing the severity of PTSD in this population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579422001511
Acknowledgments
We are grateful to the parents and children for their participation for the research, and to school teachers who helped with the data collection.
Funding statement
This study was supported by the General Project for National Social Science Fund of China (Grant No. 20BSH167).
Conflicts of interest
None.






