


Introduction
Poverty, non-availability of medicines, equipment, personnel, etc. are often cited as obstacles to adequate access to health-care services in developing countries. However, in some instances when these constraints are removed, they continue to experience low patronage of available health services (e.g. immunization, growth monitoring, antenatal care, etc). This is a disturbing development. What might be contributing to this is unclear and thus underscores the need to identify and assess the impact of innovative experiments targeted at overcoming these access and patronage hurdles. Furthermore, promoting primary health care as the basis for the provision of quality and sustainable health care and making it accessible to the majority of the population is currently the prime concern and focus of the health delivery systems. In line with this, the Catholic Relief Services (CRS) spearheaded a Development Assistance Programme (DAP) for the 2004–08 financial year in the northern sector of Ghana. The ultimate goal of the programme was to improve food security in the northern sector of Ghana – an area beset with both transitory and chronic food insecurity.
The programme had three main components, namely education, health and nutrition and safety net. The health and nutrition component focused on improving and maintaining child health and nutrition through child survival (CS) activities. The aim was to improve the quality, coverage and utilization of health and nutrition services in rural communities in Northern Ghana.
Strategies adopted to reach the health sector goals were the implementation of comprehensive behavioural change interventions to address sub-optional household health and nutritional behaviour. In the case of poor utilization of key health and nutrition services, interventions focused on the promotion of improved care-seeking behaviour, accessibility of health services and improved quality of health services.
The programme was evaluated in August 2008. In this paper, we present data to highlight the processes and actions taken to improve the utilization of key health and nutrition services and their impact on the growth of children. The improved utilization of health and nutrition services is without doubt one area that will be of much interest to health managers in many developing countries. This paper is therefore relevant for an international audience.
Purpose and objectives of the evaluation
The evaluation sought to assess the extent to which the programme objectives were achieved. More specifically, the evaluation assessed and analysed the following issues among others:
• Achievements of the programme as detailed in the project document as well as unintended outcomes associated with the interventions.
• Changes in key indicators between baseline and final evaluation.
• Level of contribution and/or ownership of the projects by beneficiary communities and partner institutions.
• Effectiveness of food as an incentive to attract mothers to child welfare clinic sessions.
• Relationships with, and appropriateness and capacity of, partners to sustain the gains thus made over the DAP period.
• Best practices and lessons learnt to date that will benefit other United States Agency for International Development (USAID) cooperating sponsors implementing Title II-funded development interventions.
Programme description
Relevance
Food insecurity resulting from vagaries of the weather and natural disasters such as droughts and floods continue to impede efforts at improving the nutritional status of children in the northern part of Ghana. Poverty and little nutritional knowledge are other challenges that need to be addressed before significant improvement in child and maternal nutrition can be achieved. The programme was thus relevant in view of the fact that maternal and child malnutrition is responsible for more than one-third of mortality in children under five years of age (Black et al., Reference Black, Allen, Bhutta, Caulfield, De Onis, Ezzati, Mathers and Rivera2008).
Target groups
The beneficiaries of the programme were primarily women and children living in food-insecure households in rural farming communities. Focus communities are located in select districts in the three northern regions of the country. The programme covered 221 beneficiary communities.
The strategic objectives
a) To improve CS by reducing chronic malnutrition (stunting).
b) To improve sub-optional household health and nutritional behaviours.
c) To improve accessibility and utilization of quality health and nutrition services by: 1) strengthening and support for the Community Health Planning and Services (CHPS) initiative; 2) empowering individuals and communities to improve their own health status; and 3) strengthening service delivery points as a prerequisite to attracting mothers/clients.
Programme activities
The specific programme activities carried out with support from the non-governmental organizations (NGOs) included the following:
i) Promoting infant feeding practices (eg, exclusive breastfeeding, appropriate complementary feeding practices and micronutrient supplementation.
ii) Promoting health-seeking behaviours at the community level and enhancing the quality of care through the training of health workers (eg, midwives, community health nurses) and community health volunteers.
iii) Effective case management of common childhood illnesses, including diarrhoea and pneumonia, by strengthening the ability of caregivers to prevent, recognize and treat or seek care especially for diarrhoea, dehydration and pneumonia through health and nutrition education.
iv) Expanded Programme on Immunization (EPI), with an emphasis on providing transport support and other logistics (including fuel) for district-level staff to deliver quality EPI services, run more outreach points and mobilizing communities to participate in childhood immunization and growth-monitoring sessions.
v) Improving geographical access to health services by supporting the construction of improved food storage facilities and growth monitoring centres.
vi) Supply of food assistance to beneficiary communities
vii) Provision of promotional materials, such as T-shirts and calendars, to the partners and the implementing staff (eg, community volunteers).
viii) Support of community-level health promotion activities including support of mothers’ support groups and holding of health campaigns, growth monitoring, etc.
ix) Institution of a rigorous and sustained monitoring of planned activities.
Expected outcomes
The intended changes expected from programme implementation were categorized as short term, intermediate and long term. The long-term goal was to improve food security of the targeted population in the three regions of Northern Ghana. Food security, according to USAID, refers to physical and economic access to sufficient food by all people at all times in order to meet their dietary needs for a productive and healthy life (USAID, 1995). For simplicity, food security is seen to consist of three components, namely food availability, food access and food utilization. Effective utilization of food (through improved sub-optimal care and feeding practices and improved access to health services) was expected to improve the health and nutritional status of beneficiary children.
Materials and methods
Evaluation design
A pre-test/post-test design involving two cross-sectional surveys at baseline and follow-up surveys were used to determine the outcome/impact of the programme. The same clusters and data collection methods were used for the baseline and final surveys.
Setting
The study was conducted in three intervention regions in Northern Ghana where chronic malnutrition is high. Baseline data were collected from 17 to 28 November 2003 and the final evaluation took place from 22 July to 18 August 2008.
Study population and sampling
The study population comprised young children (6–59 months) and women of childbearing age (15–45 years). Only women aged 15–45 years, whose children were aged 0–36 months and found within sample households, were eligible for interviewing. Assuming an effect size of 10.0% and a prevalence of 22.0% chronic malnutrition at baseline with 90% power, Type I (false-positive) α = 0.05 and 10% non-response rate, the sample size (n) estimated was 471.
Sample size was determined based on the 30 × 16 cluster methodology. The evaluation team selected 30 clusters (ie, sub-populations defined as sections of a community or whole community) and 16 interviews were conducted in each cluster (n = 480) in order to meet the sample size requirements. However, in the baseline survey, 10 interviews per cluster (n = 300) were conducted.
Selection of sample clusters
A two-staged cluster sampling methodology was used for both baseline and final evaluation surveys with 30 cluster samples for each of the two surveys. Probability proportionate to size was used to select the clusters. In follow-up surveys, it is generally recommended to retain the same clusters used in the baseline survey while choosing a new sample of households in each cluster (Food and Nutrition Technical Assistance Project (FANTA), 1997). This approach allows for sampling efficiency and provides the opportunity of detecting real programme impact.
Selecting the starting household using the EPI method
Using the EPI sampling methodology, the first household was selected from the centre of each cluster. In each cluster, the supervisor together with the interviewer chose a starting location by going to a central location in the cluster. At the centre of the cluster, a travel direction is selected at random by spinning a pen. The team then moved in a straight line in a chosen direction, counting all of the households until the end of the cluster was reached. The team then randomly chose a number between ‘one’ and the number of houses counted as the starting point for the survey. The number randomly chosen therefore corresponded to the starting house.
Selection of subsequent households
The random walk procedure was followed until such time that the required number of households had been interviewed. Every third household from the previously selected household formed the basis for selecting respondents for interviewing. This approach to selecting households has been reported to reduce similarity in responses by the interviewees (ie, reduced homogeneity; Bennett et al., Reference Bennett, Radalowicz, Vella and Tomkins1994).
Procedure for selecting individual survey subjects
Women of children aged 0–36 months found within sample households were eligible for interviewing. In each household, only one eligible respondent was randomly selected for interviewing, but for anthropometric assessment, all children aged less than five years in the household were selected.
In order to ensure adequate numbers for assessing exclusive breastfeeding, six interviews were conducted with mothers whose children were less than six months of age and 10 with mothers whose children were aged more than six months but less than or equal to 36 months.
Data collection
Interviews were conducted using pre-designed questionnaires. In order to ensure reliability and validity of the data collected, all data enumerators were given training. The content of the training included standard measurement procedures, data recording, recruitment, administration of questionnaires and supervision.
Main outcome indicators
Outcomes of the programme were assessed at the individual as well as the community or institutional level. To assess the nutritional status of pre-school children, both weight and height (length or stature) were measured alongside the administration of household health and nutrition questionnaires.
The anthropometric indicators used in assessing the nutritional status in the study population included height-for-age (HA), weight-for-age (WA) and weight-for-height (WH). Z-scores for WA (WAZ), HA (HAZ) and WH (WHZ) were calculated by using the World Health Organization (2006) growth standards. Although there are several ways of expressing the distribution of these indices at the population level, the WHO favours the use of Z-scores in assessing the level of malnutrition (WHO working group, 1986; Gorstein et al., Reference Gorstein, Sullivan, Yip, de Onis, Trowbridge, Fajans and Clugston1994). The Z-score cut-off point recommended by the WHO, Centre for Disease Control, to classify low anthropometric levels is 2 SD units below the reference median for the three indices.
Other key outcome indicators included the following:
• Complementary feeding rate
• Initiation of breastfeeding rate
• Exclusive breastfeeding rate
• Expanded access to health services
• Improved quality of health services.
Data management and analysis
Data were checked for completeness and consistency by field supervisors in the field and during data entry in order to ensure good quality. The data were coded for statistical analysis using SPSS for windows 11.5 (SPSS Inc, Chicago, IL, USA). Z-scores of HAZ, WAZ and WHZ were calculated with EPI-INFO software. The calculated Z-scores were checked for implausible values before being categorized. For example, WHZ less than −5 or more than +3 were removed from the data set.
In situations where the equivalent baseline data were not collected, some of the final evaluation indicators were compared to national coverage estimates obtained from the Ghana Demographic and Health Survey (GDHS), which was conducted in 2008 (Ghana Statistical Service (GSS) et al., 2009).
In assessing the statistical significance of observed changes, 95% CI were constructed for the difference between the two proportions (that is, baseline and final evaluation), using the following formula (Sarriot et al., Reference Sarriot, Winch, Weiss and Wagman1999):
![\[ \% \,{\rm{CI}}\,{\rm{for}}\,({{p}_1}\,{\rm{ - }}\,{{p}_2})\, = \,({{\hat{p}}_1}\,{\rm{ - }}\,{{\hat{p}}_2})\, \pm \,{{Z}_{{\alpha \mathord{\left/ {\vphantom {\alpha 2}} \right. \kern-\nulldelimiterspace} 2}}}\sqrt {\frac{{{{p}_1}{{q}_1}}}{{{{n}_1}}}\, + \,\frac{{{{p}_2}{{q}_2}}}{{{{n}_2}}}} \]](https://static.cambridge.org/binary/version/id/urn:cambridge.org:id:binary:20160107074211177-0767:S1463423610000411_eqnU1.gif?pub-status=live)
where Zα = the Z-score corresponding to the degree of confidence with which it is desired to be able to conclude that an observed change of size (p 2 − p 1) would not have occurred by chance (α – the level of statistical significance).
Ethics and informed consent
For purposes of informed consent of respondents, the aims and objectives of the survey were discussed and agreed with the NGO and the Ghana Health Service (GHS). Information about the evaluation was then communicated to the Regional Health Directorate of the three northern regions, which then communicated the information to the District Directors of the beneficiary districts.
At the community and household levels, consent was also sought from community leaders and heads of households before the data collection exercise. They were also assured of confidentiality and anonymity
Results
Nutritional status of children
Among children aged 0–59 months, the prevalence of underweight remained unchanged and global acute malnutrition increased by 2.5 percentage points, whereas the overall rate of chronic malnutrition reduced by 7.7 percentage points at the end of the project (Table 1).
Table 1 Comparison of malnutrition rate among children aged 0–59 months at baseline and final evaluation

WAZ = Z-score for weight-for-age; WHZ = Z-score for weight-for-height; HAZ = Z-score for height-for-age.
Infant feeding practices
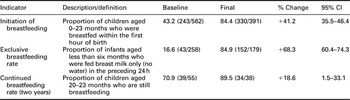
There were some significant changes in infant feeding practices in the beneficiary programme communities (Table 2).
Table 2 Comparison of key household health and nutrition behaviours/practices at baseline, midterm and final evaluation
Childhood immunization and growth monitoring coverage
Although no baseline data on childhood immunization were collected from the programme communities, the overall impact indicator for the EPI activities (ie, percentage of fully immunized children) showed that the coverage of immunization at the end of the project period in the programme districts was high compared to the figures of the 2008 GDHS (Table 3). There were significant differences in regular attendance at growth-monitoring sessions in the programme districts (χ 2 = 46.617, P = 0.001) besides the achievement of full immunization (χ 2 = 27.752, P = 0.015).
Table 3 Comparison of selected programme outcome variables and national coverage figures
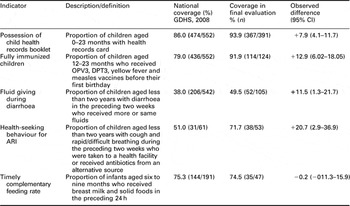
GDHS = Ghana Demographic and Health Survey; ARI = acute respiratory infection; OPV3 = oral polio vaccine (third dose); DPT3 = diphtheria-pertussis-tetanus (third dose).
Management of common childhood diseases
There was a 20.3 percentage point increase (49.5–29.2%) in the number of children under two years of age who had experienced diarrhoea in the preceding two weeks and had received either the same or more fluids (Table 4).
Table 4 Case management of diarrhoea and ARI

ARI = acute respiratory infection.
Maternal and newborn care
Out of the 480 women who were interviewed, 222 (46.3%) possessed antenatal care (ANC) cards that were sighted by the interviewer. Of the 219 antenatal cards examined at the household level, 149 (68.0%) received at least one tetanus toxoid injection, whereas 41 (18.7%) never received any injection for the last pregnancy. The proportion of mothers who received at least one tetanus toxoid injection (as recorded on a maternal health card) therefore increased from 17.2% at the beginning of the programme to 68.0% by the end of the programme.
Evidence from mothers who possessed ANC cards showed that 76.1% attended ANC at least four times. Skilled supervised delivery (ie, delivery conducted by a trained midwife/doctor/nurse) in the programme communities was still as low as 32.9%. Traditional birth attendant (TBA) deliveries declined from 58.9% at baseline to 53.6% at the end of the project life.
Supplementary food assistance
Interviews with key stakeholders revealed that the provision of food aid to target groups in the communities and institutions did help mitigate the effects of household food insecurity, although it could not completely eliminate household food insecurity.
Although some community members felt that the CRS could continue to provide food assistance forever, some were of the opinion that if the conditions in the country are such that the government continues to receive other forms of foreign assistance, for example, credits and loans, then what prevents the continuous supply of food aid to the most vulnerable groups? They argued that food aid is just another form of foreign support for the growth and development of the economy. This group of respondents, however, was fast to add that they would be willing to provide their own food if and only if assistance in the form of irrigation facilities improved seeds, fertilizers, farm inputs such as tractors, and ‘soft’ loans were guaranteed. It is these constraints that impede local food production.
Areas of sustainability
Sustainability of the programme was evaluated through key informant interviews in the following areas:
• Capacity of health workers to provide quality health care.
• Capacity of health committees and community-based management teams to operate effectively when the CRS finally withdraws.
• Promotion and adoption of desirable health behaviours and practices.
• Community capacity to develop and manage health activities through community-based mechanisms such as Centre management committees.
• Outreach health services delivery
It was gathered that with sustained health services in the communities, adoption of healthy behaviours/practices were most likely to continue. Sustainability of supplementary feeding, however, was not possible.
Infrastructural and logistic support
With support from the CRS, a total of 44 Food Assisted Child Survival (FACS) Centres were constructed at the beginning of the programme and this increased to 212 by the end of the programme.
The CRS also supported the expansion of the community-based CHPS by training community health Officers (CHOs) who man the CHPS Centres. In addition, the CRS provided logistics support to CHOs.
Discussion
The discussion focuses on the main areas of achievements, sustainability issues and lessons learnt from the programme.
Childhood nutritional status
There was a 7.7 percentage point (ie, 1.5%/year) reduction in chronic malnutrition in the programme area. The nutrition-related millennium development goals (MDGs) aim at reducing child malnutrition rates to less than 20% by 2010 and to less than 15% by 2015 (Chhabra and Rokx, Reference Chhabra and Rokx2004). The level of reduction in malnutrition achieved under the CRS-sponsored programme implies that if similar programme activities are put in place, the nutrition related MDGs could be met. It is therefore important that health authorities in Ghana keep a close watch over these achievements and maintain the strategies and activities that were used to ensure continuous progress. Reduction in infant and child growth retardation is an essential condition for achieving the MDGs.
The reduction in chronic malnutrition under the programme was encouraging. However, the level of reduction attained confirms the general difficulty in eradicating malnutrition worldwide. In the past, only a few nutrition intervention programmes have made modest achievements. For example, the Tamil Nadu Integrated Nutrition Project-1 became well known in international nutrition circles during the 1980s as a ‘success story’, because it was able to reduce the prevalence of underweight to 1.5 percentage points/year in participating districts, twice the rate of non-participating ones (Shekar, Reference Shekar1991).
The achievements of the Ghanaian programme may be attributed to a number of factors, including the build-up of a strong partnership between integrated community-based programming and health service delivery. Similar programmes that have been organized along this kind of partnership in the past have equally yielded positive results. A typical example was reported from Thailand where a drastic reduction in malnutrition was realized in less than a decade (ACC/SCN, 1992). Apart from political commitment, good strategic and programme planning, sustained integrated action and systematic monitoring, fuelled by a process of social mobilization and growing community ownership contributed to this dramatic achievement (Gillespie and Tontisirin, Reference Gillespie and Tontisirin1999).In addition, community-based child nutrition programmes in Tanzania and Senegal have shown encouraging results ((Van Roekel et al., Reference Van Roekel, Plowman, Griffiths, Vivas de Alvarado, Matute and Calderon2002; Gillespie et al., Reference Gillespie, McLachlan and Shrimpton2003)
Coverage in child immunization and growth monitoring
The overall impact indicator for the EPI activities (ie, percentage of fully immunized children) showed that the coverage of immunization at the end of the project period in the programme districts was very high. The availability (ie, physical access) of immunization services in programme communities was also high, as 455 (94.8%) children in the study sample possessed vaccination cards.
Several key factors may have contributed to these impressive outcomes. The first was that food aid assistance attracted a high patronage of child health promotion activities. Second, the positive results may also be attributed to an increased awareness of the importance of child growth by mothers brought about through the delivery of targeted health messages to programme communities. Third, all project districts were supported with transport and other logistics that facilitated sustained outreach services to these communities. The CRS also supported community health mobilization and capacity building through community volunteers.
Adoption of appropriate health practices
The programme was successful in impacting positive infant feeding practices, including early initiation of breastfeeding within 1 h of birth, exclusive breastfeeding of children aged less than six months and timely complementary feeding. Improving the health status of any given population depends on the adoption of consistent, positive health behaviours. The rationale behind the educational component of the programme was therefore based on the premise that positive behavioural change (ie, increased health service utilization, improved health practices) is a prerequisite for improved health status (impact). Programme efforts were therefore geared towards improving health practices in beneficiary communities.
In Ghana, there are social and cultural barriers to service utilization, and a lack of motivation among individuals and community members to act on acquired knowledge and make appropriate health decisions. Empowering individuals and communities with the right information and decision-making tools enhanced their ability to adopt positive health behaviours and practices.
Maternal and newborn care
Access to maternal health services also increased significantly as a result of improved accessibility to child health and antenatal services. Evidence from mothers who possessed ANC cards showed that 76.1% attended ANC at least four times. It is a recommendation by the WHO that pregnant women attend ANC at least four times (UNICEF and WHO, 2003).
Coverage in some service areas (eg, skilled supervised delivery) was still low. Supervised delivery is a necessary service required to ensure safe delivery and avoid unnecessary peri- and neo-natal deaths. Skilled supervised delivery (ie, delivery conducted by a trained midwife/doctor/nurse) in the programme communities was still as low as 32.9%. The scarcity of the required trained personnel at the community level may account for the relatively low coverage. The programme did not have the capacity to drastically increase the number of specialized health personnel needed to perform this function satisfactorily.
It needs to be stressed, however, that the utilization of health services does not only depend on the availability of services, but also on factors such as client attitudes, perceptions and past experiences with those services. In some communities, there was the perception that a woman who delivers by herself at home is seen as ‘brave’. This kind of attitude perhaps worsened the effective utilization of the available delivery services.
The decline in TBA deliveries may be attributed to the change in policy in the GHS, which shifted emphasis from deliveries conducted by these TBAs. The policy in the GHS now is to promote skilled supervised deliveries and this excludes TBA deliveries.
Management of childhood diseases
The increased incidence of diarrhoea cases among children under three years of age may be explained by the fact that a baseline survey was conducted in the dry season (November), whereas the final evaluation was conducted during the rainy season (July/August). Diarrhoea is usually more common in the rainy season. Diarrhoea can cause the growth of a child to falter due to the child’s impaired ability to absorb and utilize nutrients. This makes it very important that mothers are able to manage diarrhoea effectively. Analysis on diarrhoea management was focused only on children who had had diarrhoea during the past two weeks.
The recommended treatment for diarrhoea involves three aspects, namely: providing ORS for the child during diarrhoea, providing increased fluids to the child during diarrhoea and providing the same or more quantity of food to the child during diarrhoea. The 20.3 percentage point increase in the number of children under two years of age who had experienced diarrhoea in the preceding two weeks and had received either the same or more fluids was therefore a positive development. In addition, few mothers gave less fluid at the end of the programme compared to what pertained at baseline.
There was a slight increase in infectious diseases such as acute respiratory tract infection at the follow-up survey, compared to that at baseline. The main factor that might account for this trend is the fact that the follow-up survey was carried out in the rainy season, a period when some children are exposed to cold weather conditions. Cold conditions usually bring about increased pneumonia cases, coughs, etc.
Utilization of child and maternal health services
The utilization of health services is related to the availability, quality and cost of services as well as the social structures, health beliefs and personal characteristics of the users (Becker et al., Reference Becker, Peters, Gray, Gultiano and Blake1993; Sarin, Reference Sarin1997). Unlike curative services, the need factors for preventive health services are often, most of the time, obscured to potential clients. Therefore, to maximize utilization of preventive services in particular, the enabling factors such as income and access to quality health services need to be within the reach of families (Fosu, Reference Fosu1994). The strategies used to improve the utilization of key health and nutrition services under this programme included the provision of supplementary dry food rations, promotion of improved care-seeking behaviours, improved accessibility and quality of health services.
Since utilization of health services is highly sensitive to the distance that must be travelled to the health facility, the programme made it possible for services to be brought closer to communities. This was done through the construction of FACS centres and ensuring that services were delivered to under-served areas through supporting outreach services and engaging the services of community-based health volunteers. The programme supported with transport and other incentives that facilitated a sustained outreach services to communities.
Access to health services expanded
Geographic barriers greatly contribute to the low utilization of health services. Access to health services was made easier through a number of strategies. First, the provision of community-based food-assisted CS centres were sources for community mobilization for health, capacity building and empowerment, especially in deprived environments. The centres served as leverage points for the mobilization of mothers for health services (eg, child immunization, antenatal services, delivery of health and nutrition messages). Without these structures, it was not possible to carry out antenatal services since palpation, for example, was not possible. Furthermore, the FACS centres provided shelter for health staff in times of rainfall, etc. The use of the FACS centres as outreach points made physical access to health services within easy reach.
The CRS also supported the expansion of the community-based CHPS by training CHOs who man the CHPS centres. With this support, access to health interventions was enhanced as the CHOs were able to make services more readily available (eg, ANC, routine immunization services, distribution of vitamin A, community-integrated management of childhood illnesses and malaria interventions).
The results of these efforts helped ensure that health services were available to individuals, families and communities at their convenience.
Sustainability issues
Sustainability involves two inter-related issues: 1) sustainability of outcomes or changes and 2) long-term programme viability or institutionalization of interventions (Glasgow et al., Reference Glasgow, Vogt and Boles1999; Carroll et al., Reference Carroll, Craypo and Samuels2000).
Programme sustainability or institutionalization has been identified as a key factor in helping to sustain individual as well as community- and policy-level changes resulting from an intervention. There are reports of many programmes that achieved moderate changes upon project completion, but those changes disappeared over time when the intervention itself was not maintained (Carroll et al., Reference Carroll, Craypo and Samuels2000; Agency for Healthcare Research and Quality, 2001). The planning for sustainability of this programme was a major concern for the stakeholders. In particular, the key facilitating factors as far as sustainability was concerned were the following:
• The programme goals were consistent with that of the implementing counterpart agency (ie, the Ghana Health Service).
• Community involvement and ownership were central to the continuity of health activities.
• There were motivated individuals within the implementing agency who championed and promoted the programme.
• The implementing institution (GHS) benefited from the programme in terms of logistic support.
Lessons learnt
The following were some of the lessons learnt from the implementation of the programme:
a) Patronage for preventive primary health-care services was enhanced when some form of motivation existed to propel families to do just that. One such enabling factor that increased patronage for maternal and child health services under the programme was the availability of food aid in the communities, which attracted mothers to service delivery points.
b) In selecting beneficiary communities for the FACS activities, due cognizance was given to communities in which the GHS was already running outreach services. This approach ensured uniformity, and therefore the CRS phase-out from those communities did not disrupt health service delivery in those areas.
c) Through training and other motivation, community volunteers can be a rallying force behind community health mobilization and capacity-building.
d) To a large extent, the sustainability of the CS activities in the communities will depend on the continued provision of quality health services and organized side attraction, including awards for well baby competitions, regular attendance at growth monitoring sessions, etc.
Limitations of the study
It was difficult to associate the changes observed to the programme because of the lack of control over external factors. For example, some of the changes observed are season dependent (eg, incidence of diarrhoea, malaria); baseline studies were conducted in the dry season and the final evaluation was in the rainy season. Although some scholars have suggested that greater emphasis should be placed on showing the contribution that a particular intervention may make towards programme outcomes (Carroll et al., Reference Carroll, Craypo and Samuels2000; Mayne, Reference Mayne2001); this is not easily attainable because of the complexities surrounding health promotion/nutrition interventions.
Acknowledgements
We wish to acknowledge the invaluable contribution of the assessment team, whose organization, determination and co-operation made it possible to collect reliable data from programme beneficiaries. They were actively involved in interviewing all eligible respondents. The data collection team greatly understood the critical elements and demands of the data collection methodology, which involved walking from house to house (sometimes long distances) to reach the selected participants in the survey communities. Our warmest compliments also go to all the women who participated in this study for their immense co-operation and understanding. The enthusiasm and community mobilization efforts of the village volunteers facilitated the evaluation exercise, and to them we say bravo. We sincerely acknowledge the zeal and support received from the CRS/Ghana collaborators (ie, GHS). We very much appreciate the input of the individuals of this organization who granted the evaluation team audience and readily provided secondary data for the evaluation. In particular, we wish to express our heart-felt and sincere gratitude to the District Health Management teams, sub-district teams and District Directors for the wonderful and laudable effort in the data collection. Finally, we wish to acknowledge the contribution of the staff in the CRS/Ghana Office and Ghana USAID Mission for providing the financing for the programme including the evaluation.




