



Introduction
Emergency Medical Services (EMS), through the Emergency Call Centers (ECCs), have been one of the main entrance points for patients into the health system during the coronavirus disease 2019 (COVID-19) pandemic, affecting their activity Reference Castro Delgado, Cernuda Martínez, Romero Pareja, Cuartas Álvarez and Arcos González1 and patient outcomes. Reference Kurosaki, Okumura, Nunokawa, Yao, Murasaka and Inaba2 Since the start of the COVID-19 pandemic, EMS in Spain through telephone numbers 112/061, in addition to daily emergency calls, received calls from citizens who required urgent health care due to COVID-19 compatible symptoms or requesting information in relation to the pandemic. This situation overwhelmed ECCs with the potential risk of delay in daily care and response to emergencies, so that in the EMS, parallel flows of calls were created using new telephone numbers for requests for specific information due to COVID-19. Reference Al-Wathinani, Hertelendy and Alhurishi3 These health information telephone numbers have also been useful in early identification of a disease outbreak, over-riding other surveillance systems. Reference Handberry, Bull-Otterson and Dai4 In this way, EMS tasks may not be limited to providing a specific health response, Reference Cabañas, Williams, Gallagher and Brice5 but also to complement the epidemiological surveillance systems and act as a predictor for other levels of care. Reference Castro Delgado, Delgado Sánchez, Duque del Río and Arcos González6–Reference Arcos González, Pérez García and Castro Delgado8
The pandemic scenario in the field of prehospital care was affected by several circumstances. The high demand for calls to the ECC in relation to COVID-19 (both informative and care), and the fact that emergency and prehospital providers had an increase of sick leave that caused delays in the initial telephone service, Reference Rubí-Alzugaray, Rubio-Roca and Álvarez-Franco9 caused a special impact on those patients who required emergency medical care. Reference Yu, Liu and Chen10 In addition, the uncertainty generated fears by citizens of a possible contagion when going to health centers. Reference Galmiche, Rahbe and Fontanet11 For this reason, it is necessary to know the impact of the pandemic on EMS activity to improve EMS planning for future pandemics. Reference Lerner, Newgard and Mann12 In addition, knowing if there is any change in patient profile before and during the pandemic can show its indirect consequences, given that many patients have delayed or missed different medical appointments at different levels of care, which could cause a change in the type of treatment and EMS activity.
The main objective of this study was to find out if there were differences in the profile of patients treated by the Servicio de Asistencia Médica Urgente (SAMU)-Asturias Advanced Life Support (ALS) units, the EMS of the Principality of Asturias, between the pre-pandemic period (2019 – prior to the start of the pandemic) and the pandemic period (2020 – onset of the COVID-19 pandemic).
Methodology
This was a descriptive, cross-sectional, observational, and retrospective study that included all patients treated by ALS units of SAMU-Asturias in the period of time between January 1, 2019 and December 31, 2020, both days inclusive. Patients not treated by ALS units were excluded from the study, as well as interhospital transport. Data were obtained from the electronic clinical record of SAMU-Asturias, where all patients have to be registered by law. No sample size was calculated as all patients were extracted in the period of time. Data were extracted by software responsible of the health services following appropriate internal procedures. No missing data were reported.
Since the pandemic in Spain began in March 2020, the months of January and February 2020 were considered in the pre-pandemic period. Asturias is located in the northern part of Spain with nearly one million people, 90% of them covered by ALS units belonging to the public health system during the study period. All patients were treated by SAMU-Asturias ALS. Interhospital transport was excluded from this study. The variables studied have been: number of patients, type of activation, prehospital times, and patient resolution. Activation codes, patient resolution, the demographic characteristics of the patients, and prehospital times were analyzed.
Quantitative variables were presented as means (standard deviations [SD]). Qualitative variables were presented in absolute numbers and percentages. Student’s t-test was used to compare means. The X Reference Kurosaki, Okumura, Nunokawa, Yao, Murasaka and Inaba2 test was used to assess the association of qualitative variables and the odds ratio (OR) with its 95% confidence interval (CI) was used to assess the magnitude of the association. Data analysis was performed using the SPSS Statistics (Version 27.0.1.09; IBM statistical program; Armonk, New York USA). The study was approved by the Research Ethics Committee of the Principality of Asturias, Spain (ref.: 2021.597).
Results
During the years 2019 and 2020, a total of 17,032 patients were treated by ALS units in the study area. In the pandemic period (from March 15, 2020 through December 31, 2020), a total of 5,563 patients were treated, and in the pre-pandemic period (from January 1, 2019 through March 14, 2020), a total of 11,469 patients were treated. Average age of the population studied was 58.98 years (SD = 26.7). The activation code “common disease” was the most frequent in both periods (81.5% pre-pandemic and 81.46% in pandemic), and in terms of patient resolution, the code “transfer arrival alive” was the most frequent (75.16% pre-pandemic and 72.29% in pandemic). The daily average number of services was 23.3 (SD = 5.5). During the pre-pandemic period, the daily average number of services was 24.7 (SD = 5.3), and in the pandemic period, the average was 21.2 (SD = 5.2) with a reduction of 14.2% (P <.000). Figure 1 and Table 1 show the distribution in the number of services by month in 2019 and 2020. They show a reduction in the number of services in the pandemic months (with the exception of the month of June) compared to the same months of 2019. Regarding gender, no statistically significant differences had been observed in the pre-pandemic period in relation to the pandemic. Statistically significant differences (P = .03) were found in age between the different study periods, although with a minimal difference (pre-pandemic the average age was 59 years, and in the pandemic, the average age was 60 years); Table 2. Regarding the analysis of the activation code, no significant individual differences were found between the pandemic and the previous situation (Table 3). Analyzing the resolution codes (Table 4), transfer by own means increased from 0.5% in pre-pandemic to 1.0% in pandemic (P = .008). In the rest of the causes of resolution, no significant differences were found. Regarding prehospital times, an increased on-scene time and total prehospital time were observed (Figure 2 and Table 5).
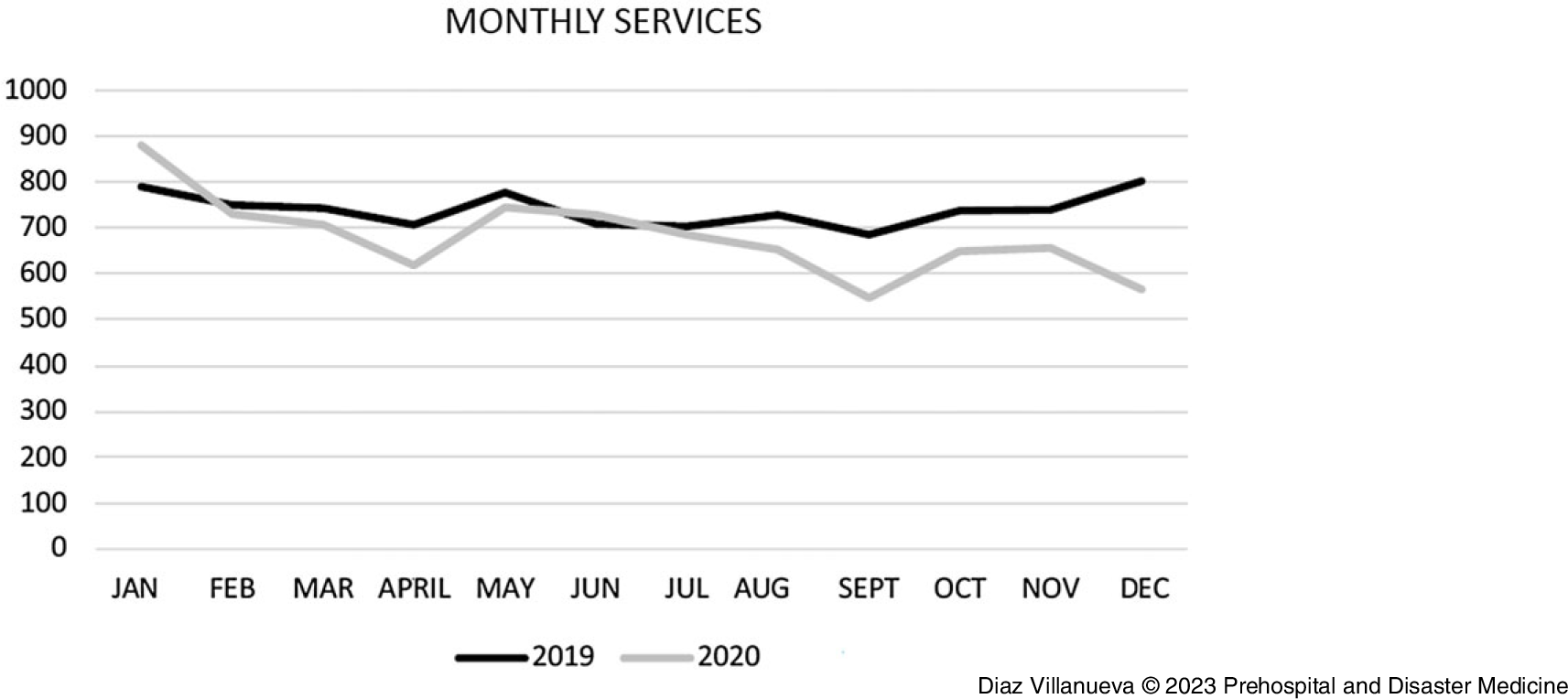
Figure 1. Distribution of SAMU-Asturias ALS Services by Year and Month.
Abbreviations: ALS, Advanced Life Support; SAMU, Servicio de Asistencia Médica Urgente.
Table 1. Distribution of Patients Treated by ALS of SAMU-Asturias by Year and Month
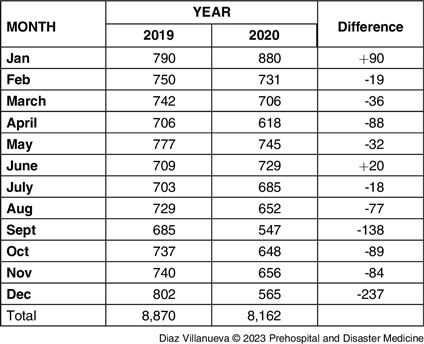
Abbreviations: ALS, Advanced Life Support; SAMU, Servicio de Asistencia Médica Urgente.
Table 2. Gender and Age Differences

Table 3. ALS Activation “Codes” (Reason for Activation)
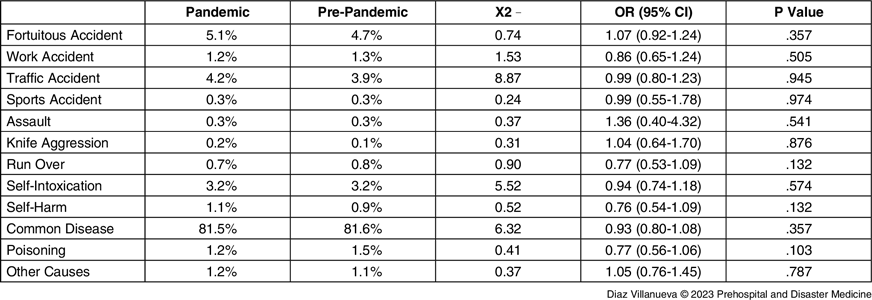
Abbreviation: ALS, Advanced Life Support.
Table 4. Patient Resolution of SAMU-Asturias ALS
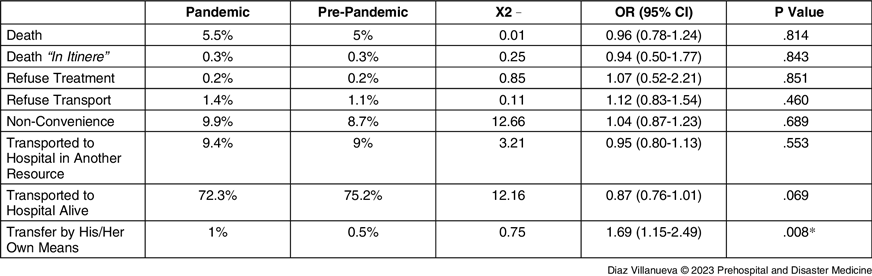
Abbreviations: ALS, Advanced Life Support; SAMU, Servicio de Asistencia Médica Urgente.
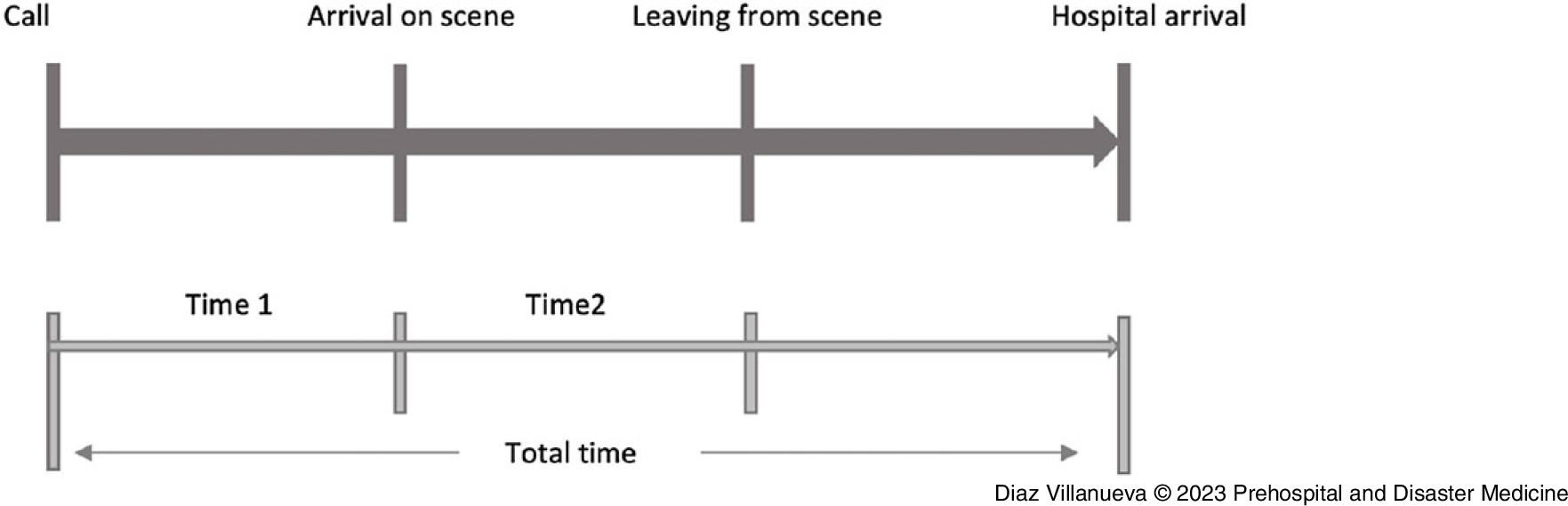
Figure 2. Diagram of Prehospital Times Analyzed.
Table 5. Prehospital Times Pre- and In-Pandemic

Discussion
According to studies published to date, in general terms, the number of interventions by the EMS since the start of the pandemic compared to the year 2019 was lower, Reference Handberry, Bull-Otterson and Dai4,Reference Hughes, Hughes and Morbey13,Reference Penverne, Jenvrin and Montassier14 similar to these results. These data could be justified by the fact that a state of alarm was established in Spain for approximately the first two months after the declaration of the pandemic, followed by different types of restrictions such as county closures that led to a decrease in social life and activities at all levels. Regarding the data collected in this study, in relation to the number of services per month, a decrease was found in these if each month was individually compared with the corresponding month of the previous year, with the exception of the months of January and June. Given that the pandemic became official in March and the restrictions also began this month, it is quite coherent to think, and this is reflected in these data, that January would not be affected by the trend of the rest of the year, which probably is not the case in February because, although the pandemic had not been made official, media was already informing people about a viral pneumonia of Chinese origin. With respect to June, it should be noted that it meant a month with daily life practically the same as the pre-pandemic period since the confinement had meant a significant reduction in all the epidemiological parameters on which the restrictions were active; therefore, during this month, these were very lax or non-existent, which is why EMS activity recovered. Months in which this drop in the number of services is most evident is in April and September. The first month coincides with the full confinement of the entire Spanish population, which reflect, as mentioned above, a restriction of activity at all levels. On the other hand, in September, new restriction measures were implemented, which again generates less social activity.
In this study, it was observed that the average age of the patients treated by the SAMU-Asturias ALS units had increased by one year in the pandemic period with respect to the pre-pandemic period, a fact that was assumed to be related to the results of other studies that described the relationship between the increase in age and the greater morbidity of COVID-19. Reference Mitchell, O’Reilly, Mitra, Smit, Miller and Cameron15 Regarding gender, no differences were found between the different study periods.
During the first months of the pandemic, previous published studies show some striking changes compared to the previous year. Risk factors for the deterioration of mental health have increased in parallel with the decrease in protective factors, generating changes in population mental health. Reference Petersen, Dantoft and Jensen16 In addition, there was an increase in the sales of alcoholic beverages in 2020 compared to 2019, mainly in susceptible populations (eg, middle age, low socioeconomic level, or mental disorders), as well as a change in the places of consumption, given the restrictions taken by the respective authorities. Reference Ogeil, Scott and Faulkner17
It would also make sense to consider that the number of accidents, both at work and road traffic, as well as in sports or at school, would have been significantly reduced, since a very large part of the population was at home most of the time. Although one might think that domestic accidents would rise, it seems unlikely that they could equal those mentioned above. It was expected that similar results to those described would be obtained. However, no significant differences were found between the two periods in the reasons for the activation of the SAMU-Asturias ALS units. These discrepancies could be attributed to the fact that the database only includes calls for ALS units. However, the rest would be transported by Type B ambulances (Basic Life Support [BLS] and primary health care). Therefore, it is likely that the variability in the rest of the activation codes was evident in non-urgent care and not in that included in the object of this study. This coincides with the results of previously published studies, in which a marked reduction was observed in the non-urgent category, in contrast to the immediate care category, which remained at similar levels. In fact, according to some studies, the odds that a call handled by EMS would be prioritized as severe doubled during the pandemic period. Reference O’Connor, Hannah and Burnor18 Focusing on the context of mental health and substance abuse and the contrast between these results and those of other studies, the most probable explanation is that, although alcohol consumption could have increased, this would not be the case in youth recreational consumption, an important cause of acute alcohol intoxication, and it would be in the chronic drinker/alcoholic profile, which would probably lead to health complications in the medium-long term. In addition, although patients susceptible to pharmacological poisoning continued to be able to purchase medications, the rest of the main substances causing overdose/poisoning (eg, cocaine and amphetamines) probably suffered a decrease in their consumption, secondary to the absence of ludic activity and the difficulty in obtaining it due to mobility restrictions. All cases would be grouped either within the category “intoxication” or alternatively in “self-intoxication” and at the time of prehospital care, it could be difficult to distinguish between both. Finally, it was expected to be observed an increase during the pandemic period in the activation code called “common disease,” since it was believed that this was where all patients treated as a result of COVID-19 would be included, but this increase was not observed.
Regarding the resolution of the services, an increase was observed in the category “transfer by your own means.” This could be due, on the one hand, to the promotion by EMS staff of this type of transfer in mild patients to avoid possible contamination of the ambulance in case of being positive, or to a refusal of the patient to be transferred in an ambulance for fear of contagion. Initially, the idea was to find an increase in non-convenience patients, since the hospital collapse at certain times could force the EMS to carry out a more exhaustive selection of patients who were candidates for hospital transfer, leaving patients at home who, in other circumstances, would have been referred to a hospital. However, this category did not undergo significant changes. Otherwise, different reviewed studies revealed an increase in the number of deaths attended by EMS and attributed it to the generalized fear on part of the population to COVID-19 infection, which generated a delay in the demand for health care. Some studies have shown a decrease in the proportion of patients who required care for acute myocardial infarction, Reference Sung, Paik, Lee and Kang19 as well as in other situations, such as: decompensated heart failure, renal failure, and exacerbations in patient’s lung diseases, Reference Gulen, Satar and Acehan20 which could cause a serious exacerbation of chronic disease that resulted in death. Likewise, these studies have observed an increase in the percentage of patients who refused to be transferred to the hospital, not only because of the fear described above, but also due to the fact that being admitted to a hospital meant being isolated from family members given the protocols established in that moment, which is why many people would make such a decision. For this same reason, it was expected to be found in the analysis of the variable under study “resolution” an increase in the category “rejects transfer” that was not finally verified.
Lastly, and as a noteworthy piece of information, prehospital times increased in the pandemic period due to longer on-scene time. This may be due to two factors: on the one hand, the use of the personal protective equipment (PPE), and on the other hand, the fact that the assessment of the patient and the performance of certain techniques with PPE was more laborious and could thus increase on-scene treatment time.
Limitations
These results may help EMS policy makers to develop strategic response plans to future pandemics and improve EMS surge capacity to adapt to needs. The main limitation of this study is that it included ALS calls, and results must be interpretated in this way. Total calls or total BLS activations were not analyzed, as these were not the objective.
Conclusion
In this study, it was observed that the pandemic has had an impact on the activity of SAMU-Asturias, which has been observed in a 9.2% decrease in daily ALS services during the pandemic, an increase in prehospital times during the pandemic period, and a slight increase in the mean age of patients seen during the pandemic in relation to pre-pandemic. No differences were found between the reasons for activation or between the resolution of the patients.
Conflicts of interest/funding
None declared. The authors have no financial or other interest that should be known by readers related to this document.








 Open access
Open access