


The effect of compulsory community treatment on health service use is controversial. Two randomised controlled trials in the USA showed negative results (Reference Steadman, Gounis and DennisSteadman et al, 2001; Reference Swartz, Swanson and WagnerSwartz et al, 2001), differences only emerging in post hoc analyses of non-randomly selected subsamples (Reference Swartz, Swanson and WagnerSwartz et al, 2001). Both trials also excluded patients with a history of violence, although dangerousness is often the reason for compulsory treatment in hospital or in the community (Reference Sensky, Hughes and HirschSensky et al, 1991; Reference Lansing, Lyons and MartensLansing et al, 1997). Finally, court-ordered treatment in the USA is different from compulsory community treatment prescribed by a mental health professional, the intervention used in Australasia (Reference McIvorMcIvor, 1998) and Canada (Reference Gray and O'ReillyGray & O’Reilly, 2001), and proposed for England and Wales (Department of Health, 2000). Although epidemiological studies may minimise selection bias, two trials in Australia were unable to control for confounders such as forensic history or illness severity (Reference Vaughan, McConaghy and WolfVaughan et al, 2000; Reference Preston, Kisely and XiaoPreston et al, 2002). This epidemiological study compares the readmission rate of patients receiving compulsory community treatment with that of two control groups, taking into account socio-demographic factors, clinical features, previous psychiatric history and forensic history.
METHOD
Data sources
We gathered information on all patients ordered to receive compulsory community treatment in the first year of implementation of these orders, from the following sources:
-
(a) the Police Offenders database of all offences and convictions in Western Australia;
-
(b) the Mental Health Information System record of all in-patient, out-patient and community contacts with psychiatric services in the state;
-
(c) the Mental Health Review Board database of all involuntary treatment in the state.
Western Australia is well suited for population-based record linkage studies as it has a well-maintained, comprehensive administrative database linking together records of all private and public hospital separations (patient discharges, transfers to another facility or deaths), contacts with state mental health services (including public out-patient clinics), death registrations and several other sets of health data for the entire state (Reference Holman, Bass and RouseHolman et al, 1999). This linked database was set up in 1980, and is one of only a small number of such comprehensive record linkage systems in the world. Components of the database, such as the Mental Health Information System used in this study, were established in 1966 (Reference Lawrence, Holman and JablenskyLawrence et al, 2001). They have been widely used for epidemiological studies in psychiatry (Lawrence et al, Reference Lawrence, Holman and Jablensky1999, Reference Lawrence, Jablensky and Holman2000, Reference Lawrence, Holman and Jablensky2001, Reference Lawrence, Holman and Jablensky2003; Reference Preston, Kisely and XiaoPreston et al, 2002; Reference Kisely, Lawrence and PrestonKisely et al, 2003) and other medical fields (Reference Norman, Semmens and Lawrence-BrownNorman et al, 1998; Reference Semmens, Norman and Lawrence-BrownSemmens et al, 1998).
These three linked components of the database enabled us to assess the psychiatric and forensic history of all patients who had been assigned to compulsory community treatment in Western Australia. We used a two-stage design of matching and multivariate analyses to take into account socio-demographic factors, clinical features, case complexity, previous psychiatric history and forensic history. We selected these variables because previous studies have shown their association with compulsory treatment in in-patient or community settings. Patients receiving compulsory community treatment are generally no more than 40 years old (Reference Reicher, Rossler and LofflerReicher et al, 1991; Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Vaughan, McConaghy and WolfVaughan et al, 2000; Reference Steadman, Gounis and DennisSteadman et al, 2001), male (Reference Malla, Norman and HelmesMalla et al, 1987; Reference Reicher, Rossler and LofflerRiecher et al, 1991; Reference CallanCallan, 1996; Reference Sanguineti, Samuel and SchwartzSanguineti et al, 1996; Reference Takei, Persaud and WoodruffTakei et al, 1998; Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Vaughan, McConaghy and WolfVaughan et al, 2000), single (Reference Reicher, Rossler and LofflerReicher et al, 1991; Reference Vaughan, McConaghy and WolfVaughan et al, 2000), non-White (Reference CallanCallan, 1996; Reference Commander, Cochrane and SashidharanCommander et al, 1999; Reference Bhui, Stansfeld and HullBhui et al, 2003) and unemployed (Reference Vaughan, McConaghy and WolfVaughan et al, 2000). They are less likely to have a higher level of education (Reference Swartz, Swanson and WagnerSwartz et al, 1999) and are more likely to have a mental disorder, such as schizophrenia, and comorbidity, including substance use (Reference Geller, Grudzinskas and McDermeitGeller et al, 1998; Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Steadman, Gounis and DennisSteadman et al, 2001). Previous health service use and forensic history, particularly of crime against persons, also predict compulsory community treatment (Reference Scheid-CookScheid-Cook, 1987; Reference Sensky, Hughes and HirschSensky et al, 1991; Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Vaughan, McConaghy and WolfVaughan et al, 2000).
Because of the way these databases are organised, we first had to identify cases and controls from the Mental Health Information System, and then link their records to the other two databases. An initial matching stage was necessary because of the large number of potential confounding variables, and to reduce the possibility of type I error in the multivariate analyses. We could not match for variables such as forensic history and involuntary treatment status because we were able to link the Police Offenders and Mental Health Review Board databases to the Mental Health Information System only after we had drawn our cases and controls. Of necessity, these variables were controlled for in the multivariate analyses.
The current Mental Health Act of Western Australia was implemented in November 1997 (Government of Western Australia, 1996). As in other parts of Australia and New Zealand, it provides for involuntary treatment in the community through the introduction of a community treatment order (CTO). The order is made out by a qualified mental health specialist, who must specify which medical practitioner is to supervise the patient's treatment or care, where the patient is to receive care, the frequency at which the medical practitioner is to report to the specialist and the duration of the order, which must not exceed 3 months in the first instance. The Mental Health Review Board must conduct a review 4–6 months after instigation of the order. A lawyer, a psychiatrist and a lay person make up the review board and hear evidence from both treating doctors and patients.
Selection of cases
We selected cases on the basis of the date that the community treatment order was made – the ‘index date’. From orders made between 13 November 1997 (the date of implementation of the Mental Health Act 1996) and 31 November 1998, we identified 265 patients who were ordered to receive compulsory community treatment. As Western Australia has a population of 1.8 million, this is equivalent to 15 per 100 000 of the general population (95% CI 13.8–17.5). Of these, 41 (15%) were given a CTO while living in the community; the remainder had a CTO imposed on discharge from hospital.
Selection of controls
We selected two control groups. The matched control group consisted of patients who were matched to each case on gender and aboriginal ethnicity, and with an age difference of less than 2 years. We also matched on whether the person had received a CTO while in the community or on discharge from hospital. The index date for the matched control patients was the discharge date from an authorised mental health hospital closest to the index date of their matched CTO case. In the case of patients placed on a CTO, we matched on the date of commencement of an episode of care. We also matched on place of birth, diagnosis and health service use (Table 1). Of 7881 matched controls selected in the first stage of the matching process, 265 were determined as the final matched controls. There was no significant difference between members of the CTO group and the matched control group in terms of socio-demographic and clinical characteristics or health service use, except that the CTO group had significantly more bed-days and out-patient attendances 12 months prior to the index date than did those in the matched control group (Table 1). The second group, the consecutive control group, was matched on date of discharge from in-patient care with the 224 patients given CTOs while in hospital (n=224). The index date for patients in the consecutive control group was the same as the index date of their matched CTO case. The data-set was complete for all variables in the three groups.
Table 1 Comparison of risk factors between the community treatment order (CTO) group and the matched control group (MCG)
| Risk factor | CTO group (n=265) | MCG (n=265) | P (CTO v. MCG) |
|---|---|---|---|
| Age (years): mean (s.d.) | 37.4 (12.8) | 37.4 (12.4) | 0.9992 |
| Gender: n (%) | 1.0002 | ||
| Male | 171 (64.5) | 171 (64.5) | |
| Female | 94 (35.5) | 94 (35.5) | |
| Aboriginality: n (%) | 0.8612 | ||
| Aborigine | 18 (6.8) | 17 (6.4) | |
| Non-aborigine | 247 (93.2) | 248 (93.6) | |
| Diagnosis:1 n (%) | 0.1292 | ||
| Schizophrenia/psychosis | 179 (67.5) | 161 (60.8) | |
| Mood disorder | 1 (0.4) | 4 (1.5) | |
| Other disorder | 85 (32.1) | 100 (37.7) | |
| Personality disorder: n (%) | 0.5062 | ||
| No | 200 (75.5) | 191 (72.1) | |
| Yes | 65 (24.5) | 74 (27.9) | |
| Country of birth: n (%) | 0.7512 | ||
| Australia | 190 (71.7) | 182 (68.7) | |
| Not Australia | 75 (28.3) | 83 (31.3) | |
| Placement on CTO: n (%) | 1.0002 | ||
| On discharge from hospital | 224 (84.5) | 224 (84.5) | |
| In a community facility | 41 (15.5) | 41 (15.5) | |
| In-patient admissions (references): n (%) | 0.062 | ||
| 0 | 43 (16.2) | 54 (20.4) | |
| 1 or 2 | 171 (64.5) | 144 (54.3) | |
| 3 and over | 51 (19.2) | 67 (25.3) | |
| Bed-days1: mean (s.d.) | 66.4 (61.0) | 45.0 (48.0) | <0.0013** |
| Number out-patient attendances1: mean (s.d.) | 56.4 (75.0) | 32.0 (46.0) | <0.0013** |
| Mental illness history (years): mean (s.d.) | 11.4 (8.2) | 11.5 (8.2) | 0.7933 |
Data preparation
Some of the data elements for our study had categorical values (e.g. gender, marital status) and others were continuous (illness duration, total length of stay during the 12 months prior to the index date). After testing various model configurations, we needed to reduce the number of value categories for some of the variables. If the continuous variable was skewed, we transformed the values into three levels: values smaller than the 25th percentile being the first level (usually taken as a reference category), values between the 25th and 75th percentiles being the second level and values greater than the 75th percentile being the third level. We did this because the distributions of these variables were still not normal after log-transformation. This method also makes the results easier to interpret.
Survival analysis
We compared time to readmission using Kaplan–Meier survival and Cox regression analyses. Initially, we used Kaplan–Meier survival analysis to compare the risks of admission between the three study groups in the year after the index date. All non-psychiatric admissions to hospital were ignored in the survival function. The survival function was generated using the actuarial method by dividing the time period into 365.25 days. We defined censored cases as being those in which the person did not require psychiatric hospital admission during the course of the study. Readmission periods were calculated in daily observations from the index date. We compared the survival curves using the log-rank test.
We performed life table analysis on each group to evaluate the percentage of group members who required readmission throughout the 12-month period. The numbers and percentages of patients admitted at each daily interval from among those remaining in the study were computed.
Cox regression analysis of predictors of hospital admission
We performed a Cox regression analysis to examine contributors to hospital admission. Contributing variables (in addition to receiving compulsory community treatment) reflected patient characteristics, clinical features and forensic history. Patient characteristics included age, gender and aboriginal ethnicity. Marital status was dichotomised into ‘always single’ v. ‘ever having been in a relationship’, with the latter as the reference category. Country of birth was divided into Australia v. elsewhere. Educational level was classified as completing primary, secondary or tertiary studies. Location of residence was divided into metropolitan v. rural or remote area, with metropolitan area as the reference variable. In terms of illness severity, complexity and diagnosis, we divided cases according to psychiatric diagnosis into ‘schizophrenia or other psychosis’ and ‘other disorders’, with the latter as the reference category. We also considered the number of three-digit primary or secondary ICD–9 psychiatric diagnoses (World Health Organization, 1978), including substance use in the year prior to the index date (termed psychiatric comorbidity) and whether the patient had ever been diagnosed as having a personality disorder. We assessed health service use prior to the index date in terms of admission rates, in-patient bed-days, out-patient contacts and whether the patient had ever received ‘after-care’ treatment (suspended or conditional discharge) in the year prior to the index date. Forensic history included whether the person had an offence recorded, had been imprisoned, and number of offences recorded 1 year prior to the index date. Lifetime history of any imprisonment was also included. We also examined the type and severity of offence (antisocial, or against property or person), and the most serious offence that had occurred in the previous year. We used the Statistical Package for the Social Sciences for Windows version 11.01 for the analyses.
RESULTS
Kaplan–Meier survival analysis of time to admission
Of 754 study subjects, two-thirds (n=496) were admitted to hospital in the subsequent year. The risks of admission for the three groups were 72% for the CTO group, 65% for the matched controls and 59% for the consecutive controls, these differences reaching statistical significance (log-rank χ2=4.7, P=0.03). Separate survival analyses between the groups indicated that patients having compulsory community treatment were significantly more likely to be admitted than those in the consecutive control (log-rank χ2=9.64, P=0.002) and the matched control groups (log-rank χ2=5.31, P=0.02). There was no significant difference in admission rates between the consecutive control and the matched control groups (log-rank χ2=1.01, P=0.316).
Cox regression analysis
Table 2 shows risk factors that were associated with significant changes to the risk of being admitted. A risk ratio of more than 1 indicates an increased risk of admission; 95% confidence intervals represent the possible ranges of the risk ratio at the 0.05 significance level. For continuous variables the ratios represent the added risk per unit of measurement, such as year of life, bed-day or out-patient contact. Probability values also reflect the significance of a level relevant to its reference category.
Table 2 Crude and adjusted risk ratios for admission
| Risk factor at baseline | Admitted (n=496) | Not admitted (n=258) | Risk ratio | |
|---|---|---|---|---|
| Crude (95% Cl) | Adjusted (95% Cl) | |||
| Gender: n (%) | ||||
| Male | 301 (60.7) | 158 (61.2) | 1.01 (0.84-1.25) | 1.06 (0.87-1.26) |
| Age (years): mean (s.d.) | 36.9 (13.2) | 42.8 (13.8) | 0.98 (0.97-0.99) | 0.98 (0.97-0.99)** |
| Aboriginality: n (%) | ||||
| Aborigine | 38 (7.7) | 10 (3.9) | 1.37 (1.01-1.80) | 1.54 (1.05-2.16)* |
| Single: n (%) | ||||
| Always single | 313 (63.1) | 137 (53.0) | 1.27 (1.05-1.52) | 1.12 (0.89-1.40) |
| Residence: n (%) | ||||
| Rural | 57 (11.5) | 35 (13.6) | 0.89 (0.65-1.14) | 0.85 (0.63-1.14) |
| Work, study or home duties: n (%) | ||||
| Yes | 195 (39.3) | 104 (40.3) | 1.00 (0.77-1.10) | 0.91 (0.75-1.10) |
| Country of birth: n (%) | ||||
| Not Australia | 152 (30.6) | 77 (29.8) | 1.03 (0.83-1.28) | 1.13 (0.93-1.38) |
| Personality disorder: n (%) | ||||
| Yes | 159 (31.7) | 55 (21.3) | 1.45 (1.20-1.76) | 1.46 (1.89-1.79)** |
| Education: n (%) | ||||
| Primary (reference) | 104 (20.5) | 50 (19.2) | ||
| Secondary | 325 (66.0) | 175 (68.0) | 0.88 (0.70-1.10) | 0.88 (0.70-1.12) |
| Tertiary | 67 (13.5) | 33 (12.8) | 0.92 (0.68-1.25) | 0.85 (0.61-1.18) |
| Diagnosis: n (%) | ||||
| Other (reference) | 208 (42.0) | 105 (41.0) | ||
| Schizophrenia | 288 (58.0) | 153 (59.0) | 0.92 (0.77-1.10) | 0.99 (0.97-1.01) |
| Illness duration (years): mean (s.d.) | 11.5 (8.2) | 14.2 (9.4) | 0.98 (0.97-0.99) | 0.99 (0.98-1.01) |
| Comorbidity: n (%) | ||||
| Present | 253 (51.0) | 90 (35.0) | 1.56 (1.29-1.84) | 1.21 (0.98-1.49) |
| Admissions1: n (%) | ||||
| 0 (reference) | 102 (21.0) | 87 (34.0) | ||
| 1 or 2 | 271 (55.0) | 143 (55.0) | 1.43 (1.14-1.79) | 1.27 (0.99-1.64) |
| 3 and over | 123 (25.0) | 28 (11.0) | 2.38 (1.82-3.01) | 1.81 (1.32-2.47)** |
| Bed-days1: mean (s.d.) | 55.1 (58) | 43.0 (55.0) | 1.003 (1.002-1.004) | 1.002 (1.001-1.004)** |
| Number of out-patient contacts1: mean (s.d.) | 48.3 (73.5) | 40.5 (66.5) | 1.001 (1.00-1.002) | 1.001 (0.99-1.002) |
| Involuntary treatment status1: n (%) | ||||
| Yes | 385 (77.6) | 194 (75.2) | 1.06 (0.86-1.31) | 0.82 (0.64-1.04) |
| Number of after-care contacts: mean (s.d.) | 5.17 (7.4) | 4.9 (7.0) | 1.00 (0.99-1.01) | 1.01 (0.99-1.03) |
| Offence committed1: n (%) | ||||
| Any offence | 46 (9.3) | 26 (10.1) | 1.11 (0.91-1.39) | 0.94 (0.73-1.20) |
| Any offence on a person | 15 (3.0) | 7 (2.7) | 1.07 (0.63-1.78) | 0.91 (0.51-1.77) |
| Lifetime offences: n (%) | ||||
| Ever convicted | 115 (23.0) | 54 (21.0) | 0.91 (0.67-1.23) | 0.73 (0.52-1.07) |
| Ever imprisoned | 19 (3.8) | 16 (6.2) | 0.73 (0.48-1.20) | 0.80 (0.48-1.33) |
| Cases v. controls: n (%) | ||||
| CTO cases (reference) | 191 (38.8) | 74 (28.7) | ||
| Consecutive controls | 132 (26.6) | 92 (35.7) | 0.71 (0.57-0.88) | 0.82 (0.64-1.04) |
| Matched controls | 173 (34.9) | 92 (35.7) | 0.80 (0.65-0.98) | 0.74 (0.59-0.93)** |
We initially examined the relationship between the variables of interest and admission using crude or unadjusted ratios (Table 2). This shows that patients in the matched control and consecutive control groups were significantly less likely to be admitted in the subsequent year than those in the CTO group. Apart from the community treatment order, factors that were associated with a significantly greater risk of admission were aboriginal ethnicity, younger age, lifetime single status, psychiatric comorbidity in the previous year, the presence of personality disorder at any time, a shorter psychiatric history, and health service use prior to the index date (admissions, and bed-days but not out-patient contacts).
Factors in the 12 months prior to the index date that had no significant effect on the risk of admission included place of residence, diagnosis and involuntary status. Gender, educational level, work status and forensic history also had no influence (Table 2). Table 2 also shows risk ratios for each variable adjusted for all other variables. Patients receiving compulsory community treatment still had an increased chance of being admitted in comparison with the matched control group (Table 2, Fig. 1), and no less a chance than those in the consecutive control group (Table 2). Other factors associated with admission included younger age, aboriginal ethnicity, the presence of personality disorder at any time, and health service use prior to the index date (admissions and bed-days, but not out-patient contacts; Table 2). We found the same results when using a stepwise Cox regression, and when comparing the CTO group with the other two groups in separate two-way analyses of variables not controlled for in the respective matching (further information available from the author upon request).
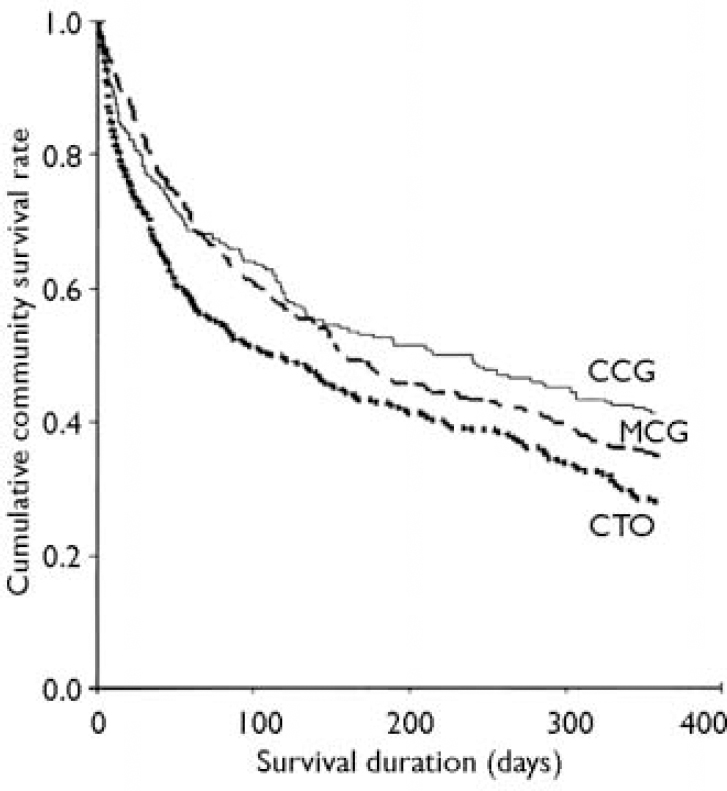
Fig. 1 Cumulative survival rates in the community of the three cohorts (n=265 for the community treatment order (CTO) and matched control (MCG) groups, n=224 for the consecutive control group (CCG))
DISCUSSION
Limitations of the study
To our knowledge this is the first study to evaluate the use of compulsory community treatment using an epidemiological sampling frame and survival analysis of linked mental health and offender databases. We were also able to perform a two-stage design of matching and multivariate analysis to control for socio-demographic variables, clinical features, case complexity and psychiatric history. We selected these variables because previous studies have shown their association with compulsory treatment in in-patient or community settings. Where matching was possible, we were able to demonstrate that there was no significant difference between CTO cases and matched controls in respect of most variables that have been shown to be associated with CTO placement. Where matching was not possible, we controlled for confounders such as forensic history, or bed-days in the previous 12 months, with multivariate analyses. However, there might have been additional factors that we could not control for in the analysis. These include social disability, aggression not resulting in a criminal record, medication type (including the use of depot preparations) and characteristics of the primary clinician, treating team or service. It would be difficult to collect this information across an entire jurisdiction such as Western Australia, which is the size of western Europe. Inevitably, a study that took these factors into account would be restricted to one or two services, with consequent loss of statistical power and the dangers of selection or referral bias. Furthermore, our study was able to adjust for more service-use confounders than others that have shown positive effects of compulsory community treatment (Reference BindmanBindman, 2002).
As this was an epidemiological study, we could not study quality of life and patient or carer satisfaction. We also do not know if compulsory treatment orders improve social outcome.
The use of community treatment orders and the overall admission rate in the 12 months after the index date were both higher than rates reported in other studies (Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference O'Reilly, Keegan and EliasO’Reilly et al, 2000; Reference Swanson, Swartz and WagnerSwanson et al, 2000; Reference Vaughan, McConaghy and WolfVaughan et al, 2000; Reference Steadman, Gounis and DennisSteadman et al, 2001). This requires further investigation, and may limit the generalisability of our findings to other settings. However, it is also possible that an epidemiological study with a large database better reflects clinical reality than do small studies that might have had careful selection criteria.
In common with other studies, we only followed up patients for 12 months after the index date (Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Swanson, Swartz and WagnerSwanson et al, 2000; Reference Steadman, Gounis and DennisSteadman et al, 2001). This meant we could compare our results with those of other authors. Although it is possible that the effects of compulsory community treatment may only become apparent in the longer term, we were concerned that factors such as subsequent life events, or interventions other than a community treatment order, might confound the results over longer periods. We would need further information on these possible confounders if we wished to assess outcome beyond 12 months.
A randomised controlled trial would address many of these problems but would also raise medico-legal and ethical difficulties. Where mental health legislation is implemented at a state, provincial or national level, randomisation within a jurisdiction is difficult to achieve. The only two such trials in this area were of involuntary out-patient treatment in the USA (Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Swanson, Swartz and WagnerSwanson et al, 2000; Reference Steadman, Gounis and DennisSteadman et al, 2001). Potential medico-legal problems were addressed in one of these by state legislation (Reference Steadman, Gounis and DennisSteadman et al, 2001). In addition, both trials explicitly excluded patients with a history of violence (Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Swanson, Swartz and WagnerSwanson et al, 2000; Reference Steadman, Gounis and DennisSteadman et al, 2001); this limits their applicability, as recent dangerousness – particularly violence against others – is often the reason for compulsory treatment in hospital or the community (Reference Sensky, Hughes and HirschSensky et al, 1991; Reference Lansing, Lyons and MartensLansing et al, 1997). It is because of these limitations that analysis of routine databases has been recommended as a way of minimising bias (Reference BindmanBindman, 2002). This is what we have done in this study.
Strengths of the study
Advantages of our study included its size, and the use of an epidemiological sampling frame that spanned the introduction of compulsory community treatment and covered all patients given a CTO. Our sample was therefore more representative of patients given such an order, and less subject to referral or selection bias. The Cox regression modelling allowed multivariate examination of a wide range of predictors of admission to hospital, for both case and control groups. We were able to control for the effects of case complexity and forensic history, including violence against others. Use of the Police Offenders database meant we were not reliant on self-report or information from health records that could be subject to reporting bias (Reference Sensky, Hughes and HirschSensky et al, 1991).
Another strength of this study is the consistency of our findings irrespective of survival analysis method and of whether we compared patients in the CTO group with the two different control groups separately, or in combination.
Comparison with other studies
The use of compulsory community treatment in Western Australia (15 per 100 000 (95% CI 13.8–17.5)) was similar to that reported in New South Wales (Reference Vaughan, McConaghy and WolfVaughan et al, 2000) but higher than rates reported from Canada (5 per 100 000; Reference O'Reilly, Keegan and EliasO’Reilly et al, 2000) or the USA (3 per 100 000; Reference Ridgely, Borum and PetrilaRidgely et al, 2001). Differences in the nature of compulsory community treatment are unlikely to be the only explanation, as the legislation in Canada and Australia is very similar (Reference O'Reilly, Keegan and EliasO’Reilly et al, 2000; Reference Gray and O'ReillyGray & O’Reilly, 2001; Reference Preston, Kisely and XiaoPreston et al, 2002). Some of this variation may be explained by the use of alternative provisions such as extended release in some jurisdictions (Reference Torrey and KaplanTorrey & Kaplan, 1995).
Like several other authors (Reference BurstenBursten, 1986; Reference Geller, Grudzinskas and McDermeitGeller et al, 1998; Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Steadman, Gounis and DennisSteadman et al, 2001), we found that compulsory community treatment does not reduce the overall risk of hospital admission compared with controls, even after adjusting for possible confounders on multivariate analyses. As our data come from the first year following the introduction of CTOs, it is possible that psychiatrists were unfamiliar with the use of such orders, and that with greater experience the intervention would produce better results. It is unlikely that our findings are attributable to the legislation in Western Australia giving insufficient powers to treating psychiatrists compared with other jurisdictions, as the Act includes the power to give treatment in the community, which is absent from similar legislation in North America.
One interpretation of our findings is that increased surveillance of patients given CTOs ensured that they were admitted if they deteriorated, and that through such earlier admissions, health service use would be reduced in the longer term. If this were the case, it might be expected that patients treated under a CTO would have shorter periods of admission. However, our previous study showed that having a CTO did not reduce the number of days spent in hospital over the subsequent 12 months (Reference Preston, Kisely and XiaoPreston et al, 2002).
Research implications
Proponents of compulsory community treatment argue that it is less coercive than compulsory admission to hospital (Reference Pinfold and BindmanPinfold & Bindman, 2001). However, our findings suggest that compulsory community treatment remains unproved as a way of reducing hospital admission rates. Even where changes in outcome have been shown, such as lower out-patient attendance rates or a decrease in violent behaviour (Reference Swartz, Swanson and WagnerSwartz et al, 1999; Reference Swanson, Swartz and WagnerSwanson et al, 2000), we still do not know whether these are due to the legislative framework, use of depot medication or greater intensity of contact (McIvor, Reference McIvor1998, Reference McIvor2001). For example, Swartz et al (Reference Swartz, Swanson and Wagner2001) in a post hoc analysis of their results suggested that compulsory community treatment had to be maintained for at least 180 days and combined with at least seven out-patient contacts a month to reduce admission rates. We require further studies to establish whether it is intensity of treatment or its compulsory nature that may affect outcome. Further research may also determine whether there are particular types of patient or legislative framework that give the best outcomes. In addition to quantitative research, qualitative techniques may give further insights into the effect of compulsory community treatment on patients, carers and health care professionals (Reference O'ReillyO’Reilly, 2001).
Policy implications
In spite of the lack of evidence for the effectiveness of compulsory community treatment, governments in jurisdictions such as Nova Scotia and parts of the UK are actively considering similar legislation. In England and Wales, this will increase the circumstances in which someone might be assessed and subjected to compulsory treatment, and reduce the opportunities for discharge (Reference MoncrieffMoncrieff, 2003). There are several dangers to this. Aside from the effect on individual liberties, such initiatives give the impression that legislators are addressing the needs of patients and their carers, while actually doing very little. Legislation in this area may also detract from the introduction of interventions known to be of benefit to individuals with severe mental disorders, such as assertive community treatment (Reference Marshall and LockwoodMarshall & Lockwood, 2003), but which are more expensive than legislative solutions to the problem.
Health service planners, clinicians, patients and carers should question the rationale for compulsory community treatment and advocate more effective treatments. If governments continue to introduce this type of legislation, without further evidence of effectiveness, some evaluation of outcome should at least be included.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ Community treatment orders in isolation do not reduce hospital admission rates.
-
▪ Community treatment orders may not be an effective alternative to assertive community treatment programmes. We require further studies to establish whether it is intensity of treatment or its compulsory nature that may affect outcome.
-
▪ Evaluation of outcome should be included if this type of legislation is introduced.
LIMITATIONS
-
▪ There may have been additional factors such as social disability that we could not control for in the analysis.
-
▪ As this was an epidemiological study, we could not study clinical or social outcomes, or patient and carer satisfaction.
-
▪ The study relied on routine administrative data.
Acknowledgement
The Medical Research Foundation of Fremantle Hospital provided funding for. the study.




eLetters
No eLetters have been published for this article.