


Trends in disease incidence are important for conceptualising disease aetiology and planning health services. Several studies have used meta-analysis to determine whether eating disorder incidence has changed over time, although these have largely focused on anorexia nervosa. Prior results indicate a small global increase in the incidence of anorexia nervosa throughout the 20th century (Reference Keel and KlumpKeel & Klump, 2003), with a stable European incidence since the 1970s (Reference Hoek and van HoekenHoek & van Hoeken, 2003). Only three studies have specifically focused on trends in the incidence of bulimia nervosa, owing to its later recognition as a diagnostic category and the tendency to report prevalence rather than incidence. However, prior work found a threefold increase in the UK primary care incidence of bulimia nervosa between 1988 and 1993 (Reference Turnbull, Ward and TreasureTurnbull et al, 1996). This leaves two important questions: has the incidence of anorexia nervosa remained stable, and is the incidence of bulimia nervosa continuing to rise as dramatically as previously reported?
METHOD
We analysed the annual incidence rates of eating disorders within a primary care setting, extending the work done by Turnbull et al (Reference Turnbull, Ward and Treasure1996). The General Practice Research Database (GPRD; http://www.gprd.com) was searched for newly recorded cases of anorexia and bulimia nervosa between 1994 and 2000 inclusive. This database covers approximately 280 general practitioners and over 3 million patients (about 5% of the total UK population). Although inner-London and smaller practices are slightly underrepresented, the patients are broadly representative of the UK population with respect to age and gender. Diagnostic information was recorded using a modified version of the Oxford Medical Information System (OXMIS) or Read classification system (depending on the year in question). The high quality of data recording has been previously validated (Reference Walley and MantganiWalley & Mantgani, 1997; Reference Jick, Kaye and Vasilakis-ScaramozzaJick et al, 2003).
The GPRD was searched for first-time diagnoses of anorexia and bulimia nervosa made between 1 January 1994 and 31 December 2000. Annual incidence rates were calculated for women aged 10-39 years. This cohort represents the vast majority of registered cases, and was the group considered in the previous study (Reference Turnbull, Ward and TreasureTurnbull et al, 1996). Incidence rates were calculated by dividing the number of eating disorder cases diagnosed annually by the total number of people in this age group registered with a general practitioner (GP) in that year. These annual incidence rates were then compared with figures collected using an identical method from the years 1988-1993 (Reference Turnbull, Ward and TreasureTurnbull et al, 1996). In addition, incidence for the total population was calculated for the year 2000, and stratified by age group and gender.
During the period studied there have been changes to the formal diagnostic criteria for bulimia nervosa. However, the GPRD uses general practitioner rather than psychiatric diagnoses, minimising the effect of these changes. In addition, concurrent notes and referral letters for cases from the year of peak incidence were compared with those from the most recent year available to determine whether there had been changes in diagnostic habits.
RESULTS
Over the period studied, annual incidence rates for diagnosed anorexia nervosa remained stable for females aged 10-39 years (Fig. 1). The rate in 1988 was 18.5 per 100 000 (95% CI 10.2-26.9) and in the year 2000 the rate was 20.1 per 100 000 (95% CI 15.0-25.2), with minimal variation in the intervening years. In 2000 the age- and gender-adjusted incidence of anorexia nervosa diagnosed in primary care was 4.7 per 100 000 population (95% CI 3.6-5.8). The incidence rate varied dramatically according to the age-gender group (Table 1). The incidence rate for females was 8.6 per 100 000 (95% CI 6.5-10.6) compared with 0.7 per 100 000 (95% CI 0.1-1.3) for males. This translated to a relative risk for females to males of 12:1. The highest incidence, 34.6 per 100 000 population (95% CI 22.0-47.1), was found in females aged 10-19 years.
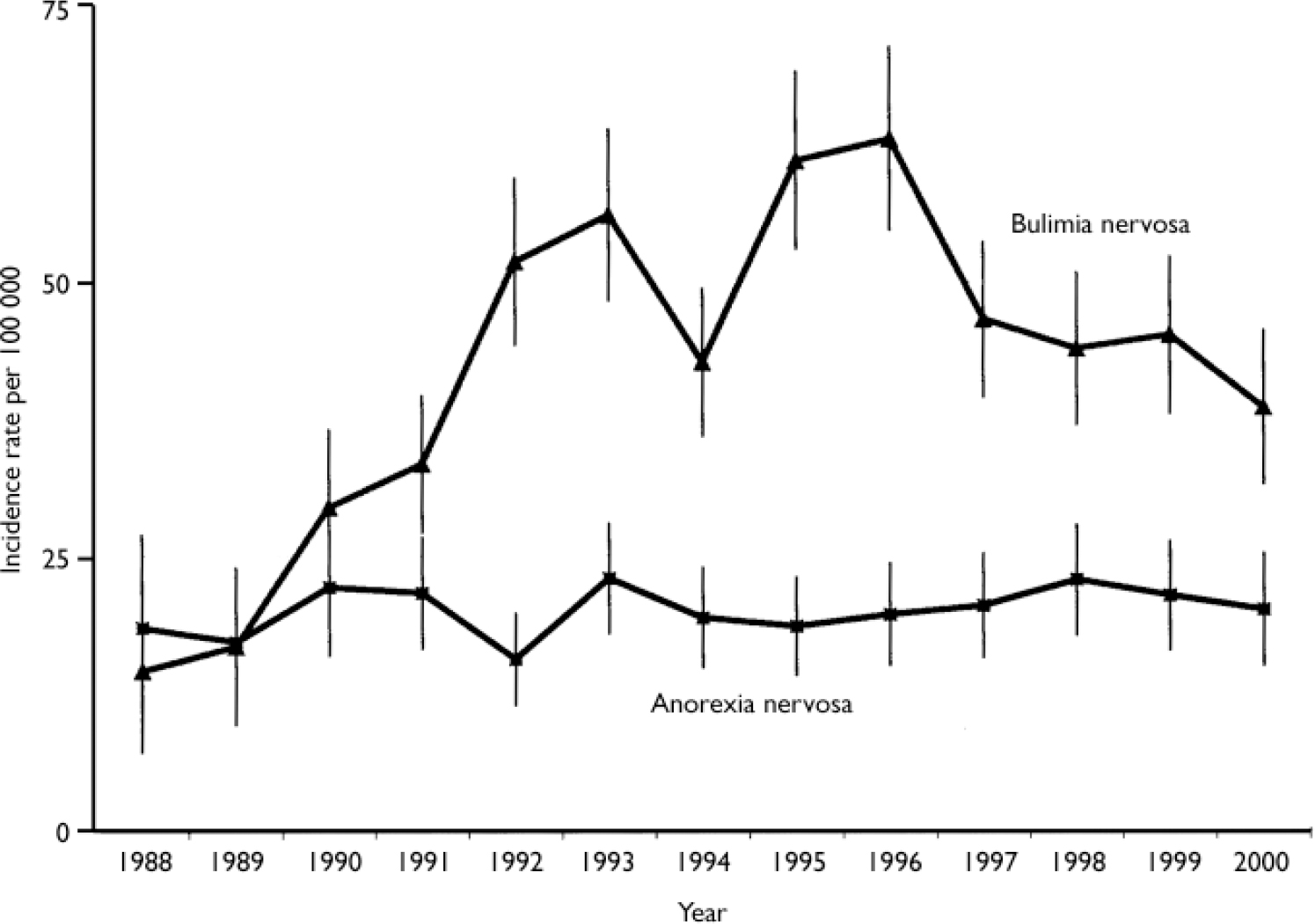
Fig. 1 Annual incidence of anorexia and bulimia nervosa in women aged 10-39 years from 1988 to 2000 (error bars represent 95% CI).
Table 1 Incidence of anorexia nervosa per 100 000 population for the year 2000
| Age (years) | Females | Males | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Cases n | Registered population n | Incidence (95% CI) | Cases n | Registered population n | Incidence (95% CI) | Cases n | Registered population n | Incidence (95% CI) | |
| 0-9 | 0 | 91 168 | 0 | 0 | 95 646 | 0 | 0 | 186 814 | 0 |
| 10-19 | 29 | 83 866 | 34.6 (22.0-47.1) | 2 | 88 092 | 2.3 (0-5.4) | 31 | 171 958 | 18.0 (11.7-24.4) |
| 20-39 | 22 | 209 761 | 10.5 (6.1-14.9) | 1 | 209 525 | 0.5 (0-1.4) | 23 | 419 286 | 5.5 (3.2-7.7) |
| 40+ | 14 | 374 150 | 3.7 (1.8-5.7) | 2 | 342 503 | 0.6 (0-1.4) | 16 | 716 653 | 2.2 (1.1-3.3) |
| Total | 65 | 758 945 | 8.6 (6.5-10.6) | 5 | 735 766 | 0.7 (0.1-1.3) | 70 | 1494711 | 4.7 (3.6-5.8) |
The results for bulimia nervosa are very different. As demonstrated by Turnbull et al (Reference Turnbull, Ward and Treasure1996), the early 1990s showed a marked increase in primary care incidence for women aged 10-39 years which continued until 1996. Although there was an overall increase in reported cases of bulimia nervosa from 1988-2000, the incidence rate has fallen by 38.9% since this peak (Fig. 1). In 2000 the age- and gender-adjusted incidence of bulimia nervosa in primary care was 6.6 per 100 000 (95% CI 5.3-7.9). The incidence rate for females was 12.4 per 100 000 (9.9-14.9) compared with 0.7 per 100 000 (95% CI 0.1-1.3) for males. This represents a relative risk for females to males of approximately 18:1. The highest incidence, 35.8 per 100 000 (95% CI 23.0-48.6), was in females aged 10-19 years.
To control for the changing criteria applied to bulimia nervosa, diagnostic validity was analysed in a subgroup of cases randomly selected from the years 1996 (n=26) and 2000 (n=19). There are considerable difficulties associated with a retrospective validation of diagnoses owing to the limited information available. Cases were defined as ‘probable bulimia nervosa’ if all but one of the DSM-IV criteria (American Psychiatric Association, 1994) were mentioned in the case history. Seventeen of the cases (37.3%) had insufficient information available to validate diagnoses. Of the remaining cases, a similar proportion of cases in 1996 and 2000 were either ‘full’ or ‘probable’ bulimia nervosa (82.3% and 81.8%, respectively). It is important to note that all of the remaining cases were considered to be eating disorder cases (either ‘not otherwise specified’ or anorexia nervosa).
Table 2 Incidence of bulimia nervosa per 100 000 population for the year 2000
| Age (years) | Females | Males | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Cases n | Registered population n | Incidence (95% CI) | Cases n | Registered population n | Incidence (95% CI) | Cases n | Registered population n | Incidence (95% CI) | |
| 0-9 | 0 | 91 168 | 0 | 0 | 95 646 | 0 | 0 | 186 814 | 0 |
| 10-19 | 30 | 83 866 | 35.8 (23.0-48.6) | 3 | 88 092 | 3.4 (0-7.3) | 33 | 171 958 | 19.2 (12.6-25.7) |
| 20-39 | 60 | 209 761 | 28.6 (21.4-35.8) | 2 | 209 525 | 1.0 (0-2.3) | 62 | 419 286 | 14.8 (11.1-18.5) |
| 40+ | 4 | 374 150 | 1.1 (0-2.1) | 0 | 342 503 | 0 | 4 | 716 653 | 0.6 (0-1.1) |
| Total | 94 | 758 945 | 12.4 (9.9-14.9) | 5 | 735 766 | 0.7 (0.1-1.3) | 99 | 1494711 | 6.6 (5.3-7.9) |
DISCUSSION
The incidence rate of anorexia nervosa in primary care has remained extremely stable over the 12 years studied. In contrast, reported cases of bulimia nervosa increased during the same period. However, the peak in bulimia cases seen in 1996 was followed by a subsequent decline for the remainder of the study. This decline was almost entirely explained by the decrease in incidence rates for females aged 20-39 years. In 1993 the incidence rate for this group was 56.7 per 100 000 (95% CI 49.2-64.3) (Reference Turnbull, Ward and TreasureTurnbull et al, 1996), but by 2000 it had fallen to 28.6 per 100 000 (95% CI 21.4-35.8). In contrast, the incidence of bulimia nervosa in women aged 10-19 years has remained relatively stable: 41.0 per 100 000 in 1993 compared with 35.8 per 100 000 in 2000 (Reference Turnbull, Ward and TreasureTurnbull et al, 1996).
CONTEXT OF FINDINGS
The stability of anorexia nervosa incidence is consistent with reports from a review by Hoek & van Hoeken (Reference Hoek and van Hoeken2003), and the age- and gender-adjusted incidence is comparable with that found in another primary-care study (Reference Hoek, Bartelds and BosveldHoek et al, 1995). Our data suggest that the previous trend of increasing incidence of bulimia nervosa in primary care has not continued, and therefore the age- and gender-adjusted incidence reported here is lower than other comparable figures (Reference Hoek, Bartelds and BosveldHoek et al, 1995; Reference Soundy, Lucas and SumanSoundy et al, 1995). This finding, that young women aged 10-19 years have the highest risk of both anorexia and bulimia nervosa, corresponds with other epidemiological evidence that eating disorders emerge in late adolescence (Reference Soundy, Lucas and SumanSoundy et al, 1995; Reference Lucas, Crowson and O'FallonLucas et al, 1999; Reference Lewinsohn, Striegel-Moore and SeeleyLewinsohn et al, 2000).
A major strength of our study is the use of a nationally representative primary care database. Because of the structure of the UK health system most patients will pass through the care of a GP, even if later referred to specialist services. Additionally, 20% of patients with anorexia nervosa and 40% of patients with bulimia nervosa are treated exclusively in primary care (Reference Turnbull, Ward and TreasureTurnbull et al, 1996). Moreover, time trends were assessed using the same method over the entire study period, rather than depending on meta-analysis. However, the use of a primary care database is itself a limitation, in that the reported figures represent clinically meaningful cases rather than those meeting DSM-IV criteria. This parallels the picture seen in other studies of clinical cases. Several specialist services consistently report that the most common diagnosis is ‘eating disorders not otherwise specified’, and these cases are no less severe in presentation or illness duration than those meeting full diagnostic criteria (Reference MillarMillar, 1998; Reference Ricca, Mannucci and MezzaniRicca et al, 2001; Reference Fairburn and HarrisonFairburn & Harrison, 2003; Reference Turner and Bryant-WaughTurner & Bryant-Waugh, 2004). A second limitation is that only those identified by their GP are reported in this study; therefore, this study cannot estimate the true community incidence of these disorders. This limitation is shared by all epidemiological studies that use service registers.
CHANGES IN BULIMIA NERVOSA
There are several potential explanations of the peak in incidence of bulimia nervosa seen in the 1990s and its subsequent decline. It is possible that patients may now seek help from different sources. During the study period, the UK-based Eating Disorder Association (http://www.edauk.com) has experienced a dramatic increase in demand for its web-based messaging and e-mail service (S. Ringwood, Eating Disorder Association, personal communication, 2004). Perhaps patients are now turning to a range of different support services, rather than relying primarily on their GP. Another possible explanation relates to changes in professional or public attention to eating disorder symptoms. The earlier period of rising incidence of bulimia might have been the result of increased recognition and detection efforts given to a new and ‘fashionable’ diagnosis. In line with this theory, the decrease in identified cases mirrors a decline in eating disorder research publications. Between the years 1960 and 2000 the number of references about eating disorders in general - and bulimia in particular - grew proportionately much faster than the total number of Medline citations (Reference TheanderTheander, 2002). However, during the 1990s this rate slowed, and eating disorder literature is now published at a slightly lower rate than general medical literature. Perhaps during the period of intense academic interest, clinicians were more attuned to eating disorder diagnoses and symptoms. This would have specific implications for bulimia nervosa as it is typically a hidden illness, whereas anorexia nervosa is more instantly recognisable.
Intense UK press coverage of bulimia during the 1990s might also have contributed to the apparent rise in incidence. For example, the first reports of Princess Diana's battle with bulimia appeared in Andrew Morton's 1992 book Diana: Her True Story (Reference MortonMorton, 1992), and subsequent media interest might have focused attention on bulimic symptoms and improved public awareness of the disorder. It is notable that the Princess's death in 1997 coincided with the beginning of the decline in bulimia incidence. Greater familiarity has been implicated in the increased incidence of other diseases, including autism and repetitive strain injury (Reference Brogmus, Sorock and WebsterBrogmus et al, 1996; Reference Kaye, del Mar Melero-Montes and JickKaye et al, 2001). Identification with a public figure's struggle with bulimia might have temporarily decreased the shame associated with the illness, and encouraged women to seek help for the first time. This would suggest that some of the 1990s peak might have been caused by the identification of long-standing cases, rather than a true increase in community incidence. The finding that the recent decline is largely due to a reduction in incidence in the older group (women aged 20-39 years) supports this conclusion.
FUTURE WORK
Further research is needed to determine whether the reported incidence of bulimia nervosa will continue to decline in the UK, or whether this is the beginning of a stabilisation that echoes the stable incidence observed for anorexia nervosa. This work suggests a need for increased recognition and treatment efforts, especially for adolescent women. Even subclinically disordered eating behaviour during adolescence elevates the risk of a broad range of physical and mental health problems during early adulthood (Reference Johnson, Cohen and KasenJohnson et al, 2002) and eating disorder symptoms in adolescence confer a strong risk of eating disorders in young adulthood (Reference Kotler, Cohen and DaviesKotler et al, 2001). In addition, the National Institute for Clinical Excellence (2004) has recently called attention to the lack of research in adolescents with bulimia nervosa. Given that this age group now shows the highest incidence of bulimia in primary care, there needs to be renewed emphasis on research in this area.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ The incidence of anorexia nervosa detected by general practitioners has remained stable for the years 1988-2000, whereas the incidence of bulimia was marked by a dramatic increase in the 1990s and now appears to be falling.
-
▪ Special detection and treatment efforts should be aimed at young women aged 10-19 years, as this is the age group with the highest risk of both anorexia and bulimia nervosa.
-
▪ General practitioners need more information about the presentation of eating disorder symptoms and the treatments available, to allow early and effective intervention.
LIMITATIONS
-
▪ Only those approaching their general practitioner for treatment could be detected; this study cannot estimate the number in the community who do not seek help for their condition.
-
▪ Incidence is calculated from general practitioners' clinical diagnoses rather than DSM-IV criteria.
-
▪ It cannot yet be determined whether the decline in bulimia nervosa incidence during the last 4 years of our study represents a true decrease in disease incidence or is due to other changing circumstances.




eLetters
No eLetters have been published for this article.