



Introduction
Prostate cancer (PC) is the second most frequent malignant neoplasia in the world among men. Approximately 1.3 million new cases of PC were expected in 2018 (Reference Bray, Ferlay, Soerjomataram, Siegel, Torre and Jemal1). In Brazil, 65,840 new cases of prostate cancer were expected each year of from 2020 to 2022 (2).
The higher incidence of PC has been associated with increased use of the prostate-specific antigen (PSA) test, especially in asymptomatic individuals (Reference Bray, Ferlay, Soerjomataram, Siegel, Torre and Jemal1;Reference Hamdy, Donovan and Lane3;Reference Moyer4). Male ageing (Reference Lunenfeld5) and the increased survival of patients with distant spread (metastasis) (Reference Bandini, Pompe and Marchioni6) also contribute to a higher prevalence of PC. As more men live with PC, there is a significant economic impact on public and private health services (Reference Sennfalt, Carlsson, Thorfinn, Frisk, Henriksson and Varenhorst7). Roehrborn and Black (Reference Roehrborn and Black8) conducted a review of the literature that showed the same trend in costs throughout PC treatment in Europe, the United States, Canada, and Australia. The highest cost is associated with the end stage of the disease (metastasis), primarily from the high cost of oncologic treatments (e.g., chemotherapy) and the great expense of hospital admissions, medical appointments, loss of productivity, and other supportive care at the end of life (EOL) (Reference Yabroff, Lund, Kepka and Mariotto9).
The results from studies on the cost of PC are heterogeneous (EUR 3,171–EUR 5,851) (Reference Roehrborn and Black8), which can be attributed to the differences in methodology, epidemiology, diagnosis, and treatment in each country. Though not usually addressed, another important limiting factor is the nature and accuracy of costing methods used in economic studies on PC. In general, studies use different costing methods, with no established standard (Reference Molinier, Bauvin and Combescure10). Time-driven activity-based costing (TDABC) is an innovative method for estimating costs. Proposed by Kaplan and Anderson (Reference Robert and Kaplan11;Reference Robert and Kaplan12), TDABC has already been used in industrial areas to estimate the cost of services (Reference Hoozée and Bruggeman13), and its benefit stems from its high accuracy (Reference Keel, Savage, Rafiq and Mazzocato14).
To the best of our knowledge, there are few cancer cost studies using TDABC; existing studies mainly evaluated only one type of treatment or diagnosis in the patient's care (Reference Alves, da Silva Etges, Neto and Polanczyk15). Thus, these studies do not estimate the total cost of the disease. Evaluation of the entire patient care chain is necessary to estimate the overall cost (Reference Jo16). TDABC is robust and allows the generation of accurate data. There is thus a growing trend of its use globally in cancer cost studies (Reference Keel, Savage, Rafiq and Mazzocato14;Reference Beriwal and Chino17). The method has been applied in several recent microcosting studies in health care (Reference da Silva Etges, Cruz and Notti18); in many, it is possible to discuss and measure waste reduction opportunities or process of care efficiency increases (Reference da Silva Etges, Ruschel, Polanczyk and Urman19). For those who applied the methods, limitations in the information technology available and the opportunity to collect quality time data are frequent challenges (Reference da Silva Etges, Ruschel, Polanczyk and Urman19).
Despite these challenges in method application, costs estimates for metastatic PC are needed to achieve better healthcare planning in the public health system (PHS). Thus, the aim of this study was to estimate the cost of advanced PC (metastatic) from the perspective of a philanthropic hospital in southern Brazil and to identify determinants of costs.
Methods
Study Design and Sample
This is a retrospective study using secondary data. All data were collected from patients who had received at least one cycle of chemotherapy using docetaxel (the only available therapy at the time of the study) and from patients whose treatment had been paid for by the Brazilian PHS at Hospital Santa Rita (HSR). Patients who received any treatment for their disease using the private system were excluded from the study. HSR only provides care for cancer patients from southern Brazil. The temporal horizon consisted of the time interval between diagnosis of metastasis until the death of the patient. The study period was from September 2012 to May 2017. The Research Ethics Board from Irmandade da Santa Casa de Misericórdia de Porto Alegre approved the research protocol (No. 2,157,033).
Costs
The costs were classified according to Horngren (Reference Horngren, Foster, Datar, Madhav and Rajan20). The total cost for each patient came from the sum of the direct medical costs extracted by applying the TDABC microcosting method. Costs of any other nature that did not relate to PC were not included in the study. All costs were estimated from the perspective of a philanthropic hospital. In Brazil, philanthropic hospitals are private, non-profit institutions that provide services to the PHS. Brazilian currency (Brazilian Real) was converted to 2018 United States dollars (USD).
Tasy© software (2012 Koninklijke Philips Electronics N.V.) was used for extraction of direct medical costs. The actual costs of general medications, oncologic medications, hospital supplies, inputs, and exams (imaging and laboratory) were extracted from the patients’ accounts.
Application of the TDABC Method
TDABC is considered the gold standard method in microcosting and value analysis in health care (Reference da Silva Etges, Cruz and Notti18;Reference da Silva Etges, Ruschel, Polanczyk and Urman19;Reference da Silva Etges, Polanczyk and Urman21). Motivated by that, in 2020, a group of researchers introduced TDABC in the Healthcare Consortium that congregated guides to apply the TDABC method (Reference da Silva Etges, Polanczyk and Urman21). In our study, the application of TDABC followed the guidelines of Everaert and Bruggeman (Reference Everaert, Bruggeman, Sarens, Anderson and Levant22) and da Silva Etges et al. (Reference da Silva Etges, Cruz and Notti18) according to the following steps.
-
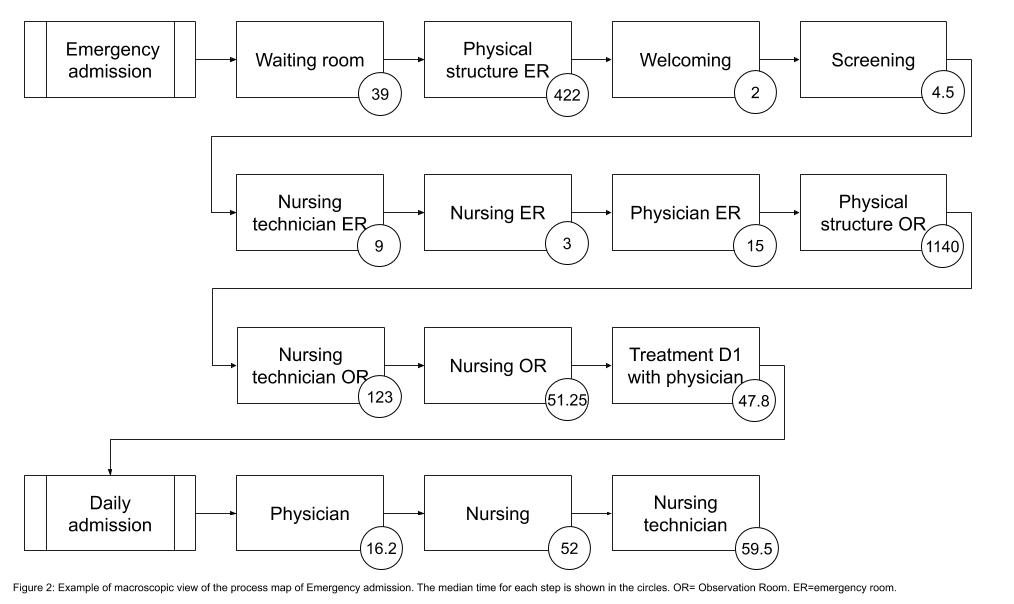
Step 1: Develop process maps for each activity in patient care delivery.
Patient accounts and electronic medical records were evaluated to identify the departments that the patients most frequently attended from September 2012 to May 2017. These departments were selected to estimate the costs using the TDABC method. The main activities of each department were mapped (Supplementary Material).
-
Step 2: Identify the resources involved in each activity and department.
Resources were divided into personnel (physicians, nurses, technicians, and auxiliary administrative) and structural (water, energy, and office supplies) categories. Interviews were conducted with physicians and nurses to identify the professionals involved in each activity. The workload data for each professional involved in the activities were retrieved after consultation with the hospital's personnel department. The resources involved with the structure were extracted from the Tasy© software report.
-
Step 3: Estimate the total cost for each activity and department.
The total cost of each activity was calculated according to the consumption of the necessary resources noted in step 2. The total accumulated cost in 2016 was considered for the analysis.
-
Step 4: Estimate the practical capacity of each resource and calculate the practical capacity cost rate (CCR).
The CCR is the ratio of the costs of the resources (labor or department structures) and the practical capacity of each resource, which represents the actual capacity (minutes worked in one year) of the resources used to perform the activity. CCR is presented in BRL/minutes.
The practical capacity of the care workforce was calculated based on the monthly workload information of the employees. The practical capacity of the department structures was calculated based on the working hours and resources available for clinical appointments, such as clinical offices and hospital beds. A practical capacity adjustment of 80 percent was considered for calculating the actual practical capacity, as recommended by Kaplan and Anderson (Reference Robert and Kaplan11).
-
Step 5: Estimate the time consumption of each resource used in a specific activity.
The estimate of the average time that patients made use of each resource in each activity (chrono-analysis) was performed as suggested by Kaplan and Anderson (Reference Robert and Kaplan11). Chrono-analysis was performed with the direct observation of patients. Two study resource groups had time data collected in the chrono-analysis: assistance (related to the assistance labour force) and administrative (referring to the consumption of resources of the administrative structure).
-
Step 6: Estimate the total (indirect) cost of each patient.
The average time to perform each activity was multiplied by the specific CCR of each activity. The sum of the products of each activity resulted in the total cost of the process. The costs of outsourced procedures to the hospital were added to the cost of the activities, which were imaging and laboratory exams, as well as the cost of drugs and materials. For these procedures, the hospital acquisition cost was attributed as the cost per procedure.
Statistical Analysis and Outcomes
SPSS® (SPSS for Windows 18.0) was used for analyses. Data are presented as the frequency and/or percentage (%), mean ± standard deviation. The costs were classified as follows: outpatient clinic visits, exams (laboratory and imaging), hospital admission, systemic treatment (oncologic), radiotherapy, and emergency. The EOL cost was calculated considering the expenditures from the time of the last cycle of chemotherapy to death. The cost data are presented in two ways: the total cost with the distribution of resource consumption by department and the monthly cost per patient. The monthly cost was calculated by dividing the cost per patient by time (months) of the follow-up period. The monthly cost is presented in medians and interquartile ranges. High-cost patients were defined as those who presented a median cost above the 75th percentile (outcome). Univariate analysis was performed to determine factors (age, metastases at diagnosis, Gleason score, previous local treatment, and the use of adjuvant GnRh analogue) associated with high-cost patients. Variables significantly associated with the outcome (p ≤ .20) in univariate analyses were included in the multivariate analysis. Poisson regression with robust variance was applied using stepwise backward selection of variables, starting with all the eligible variables and removing those with a p-value > .05. The results of the regression analysis were expressed as relative risk (RR) and confidence intervals of 95 percent (95% CIs).
Overall survival was assessed using the Kaplan–Meier survival curve, considering the date of the diagnosis of metastases as the beginning of the observation and the date of death as the end. Cases in which there was no death record until the end of the collection (May 2017) were classified as censored. We considered p < .05 as statistically significant.
Results
We had access to data from fifty-nine patients. However, data from sixteen patients were excluded because these patients migrated to private assistance. The final sample was composed of data from forty-three patients. The mean age of these patients was 62.2 ± 8.34 years at the time of diagnosis of metastasis (Table 1). The median overall survival was 1.87 years (95% CI 1.45–2.30), and the median of the EOL period was 4.7 months (95% CI 1.3–8.0). Regarding the treatment of chemotherapy with docetaxel, the median of the sample cycles was 7 (minimum of 1 and maximum of 31).
Table 1. Clinical characteristics (n = 43)a

a Data are presented as mean and SD = standard deviation, number (%).
b Extent of disease during the evaluated period.
c Median (minimum − maximum).
d Radiotherapy for pain control.
e Surgery for bleeding control, spinal cord compression, and pathological fracture.
The total cost of the sample was BRL 917.000 (USD 250,878) and the monthly cost per patient was BRL 20.201 (USD 5,526) (Table 2). Twenty-six percent of the total cost was estimated through TDABC. The costs of systemic oncological treatment (34%), exams (30%), and hospital admission (26%) contributed most to the total cost. The EOL cost per patient was BRL 5.151 (USD 1,409).
Table 2. Cost per patient and resources consumption (2018)

a Median (p25; p75).
Clinical variables and their impact on high-cost outcomes (costs above the 75th percentile) are described in Table 3. In the univariate analysis, the variables metastatic stage at initial diagnosis and previous local treatment were associated with high cost. In the multivariable model, only the previous local treatment variable showed an association with the high cost of the patient. Patients without previous local treatment presented thirteen times more risk of having a high cost than patients who received local treatment (RR = 13.01; 95% CI 2.04–83.02).
Table 3. Clinical variables and their impact on the high costa

a Median cost higher than the 75 percentile — BRL 26.160 (USD 7,156).
b Poisson regression.
c Previous local treatment = treatment of primary tumor with surgery and/or radiotherapy.
In the exploratory analysis, it was observed that patients who had undergone previous local treatment had a lower median cost than those without local treatment: BRL 15.064 (USD 4,121) versus BRL 25.331 (USD 6,930) (p = .004), respectively. Moreover, the pattern of resource consumption was different. When comparing the distribution of the total cost between the two groups (those with and without previous local treatment), there was a higher tendency of resource consumption in hospitalization (34%) and exams (31%) for patients without local treatment. In contrast, among patients with previous local treatment, the consumption of hospitalization resources and exams accounted for 15 percent and 29 percent, respectively (data not shown).
Discussion
This article presents the cost of metastatic PC based on real-world data from patients of the PHS in a philanthropic hospital in southern Brazil. The total cost of patient care in the sample evaluated was BRL 917.000 (USD 250,878), and the cost per patient per month of overall survival was BRL 20.201 (USD 5,526).
There are a few economic studies of prostate cancer in Brazil (Reference Campolina, Yuba and Decimoni23); however, none of them is on the economic burden of metastatic PC in the Brazilian PHS (SUS). Asano et al. (Reference Asano, Soo, Kim, Carvalho Del Aguila, Navarro and Fernandes24) carried out a study on the economic burden of PC with bone metastases between 2010 and 2015, but the study was conducted in the supplementary health scenario. The cost per patient was BRL 118.183 (USD 32,333), and 56 percent of this cost was derived from medications. Although it is hard to compare our results with this study, it is important to note that the resource consumption behaviors seem to be similar to those we observed, as there is a concentration of resources in direct costs, especially on medications.
Using accurate tools to assess costs can benefit the development of economic models to evaluate the cost-effectiveness of treatment. For instance, a study carried out in Brazil by Aguiar et al. (Reference Aguiar, Tan, Simko, Barreto, Gutierres and Giglio25) developed a descriptive analytical model to evaluate the cost-effectiveness of adding abiraterone or docetaxel to androgen deprivation in comparison to androgen deprivation alone. The costs used in Aguiar et al.'s model were lower than those from our study. For example, the EOL cost per patient was BRL 1.034 (95% CI 827–1,240) in Aguiar et al., while the same cost in our study was BRL 5.151 (USD 1,409).
Another strength of our study is the fact that we identified clinical variables that can predict high costs in patient care and can inform the decision-making process. When the clinical variables and their relation to the total cost were evaluated, it was observed that patients who did not have their primary tumor treated previously had a higher risk of presenting the outcome (high cost). It is known that the local progression of PC may result in invasion of adjacent structures, urinary retention, hematuria (bladder invasion), intestinal obstruction, and fistulas (Reference Leonel Almeida and Jorge Pereira26). These are serious complications that demand hospital care, explaining the high cost in the group with no previous local treatment. Retrospective studies show that local treatment of PC reduces the incidence of these local complications (Reference Won, Gurney, Marx, De Souza and Patel27;Reference Heidenreich, Porres and Pfister28). Therefore, it is plausible that reducing the risk of local progression would result in a different profile of complications and in a different amount of resource consumption. Our results suggest this possibility, as patients without local treatment presented a higher proportion of expenditures on hospitalization.
On the other hand, our results should be considered with some caution. The data presented are limited to a specific scenario and time. We performed a cost estimate in a philanthropic hospital, which is a type of hospital that relies on some level of academic activity. Some processes are developed by training professionals (resident physicians), which is not the reality of most hospitals. The fact that we present a perspective of the provider (philanthropic hospital) means that no intangible costs and costs related to loss of production were evaluated. Moreover, the sample was small and composed of a very specific population: patients with metastatic prostate cancer who underwent chemotherapy at a referral hospital with its own pre-established routines. The retrospective design and the need to perform chrono-analysis prospectively in another sample for some activities are limitations as well.
It is also important to mention that the TDABC methodology is recent and not yet widespread. There were only seven studies in the oncology domain that used TDABC as a tool for estimating the costs of treatments (Reference Alves, da Silva Etges, Neto and Polanczyk15) before 2016. Therefore, there are limitations in comparing the results of the present study with the results of studies in which other methodologies were used. Variations in the epidemiology of PC, treatment patterns, and evaluated perspectives (Reference Yabroff, Lund, Kepka and Mariotto9;Reference Molinier, Bauvin and Combescure10) are other variables that limit generalizability.
Despite the limitations noted above, evidence obtained from real-world data is of paramount importance to raise awareness about disease management and to shed some light on the economic impact of this management. Advanced methods of estimating costs such as TDABC also allow us to accurately identify the economic impact that different patient flows represent and to generate rich information to improve actions in favor of quality assurance of health services (Reference Keel, Savage, Rafiq and Mazzocato14).
It is also important to highlight that, to the best of our knowledge, this is the first study on the economic burden of metastatic PCs in the Brazilian PHS using the TDABC costing evaluation method. Our results show evidence that the TDABC methodology can be applied in health scenarios and can help to better predict the healthcare costs of metastatic PC.
Value in health is commonly defined as the ratio between benefits/outcomes and costs related to the burden of a specific disease (Reference Lee, Matthew Austin and Pronovost29). The American Society of Clinical Oncology (ASCO) (Reference Schnipper, Davidson and Wollins30) and the European Society for Medical Oncology (ESMO) (Reference Cherny, Sullivan and Dafni31) developed guidelines to evaluate cost/benefit ratios. However, discussion is still more focused on determining outcomes. Other pharmacoeconomics guidelines follow the same trend (Reference Jacobs and Barnett32;Reference Frappier, Tremblay, Charny and Cloutier33). Therefore, we believe it is important to shed light on the need for accurate tools to assess costs in health care, especially for the decision-making process in developing countries with limited resources.
We believe that future studies could focus on the development and improvement of costing methods. Neglecting health cost information or using low-accuracy cost methodologies can result in skewed interpretations, mainly in economic analysis studies. We also believe that Porter and Kaplan's (Reference Porter34;Reference Kaplan and Porter35) proposal for considering important outcomes for patients in the cost estimate is of great importance and should be considered in future studies.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0266462321000271.
Acknowledgements
We thank Cristiane Pieri Ferreira for her valuable contribution to data extraction.








 Open access
Open access