



Introduction
Head and neck squamous cell carcinoma (SCC) is the sixth most common cancer in the world.Reference Schenker, Arnold and Bauer1 The larynx is the second most common subsite for head and neck SCC.Reference Doobaree, Landis, Linklater, El-Hariry, Moller and Tyczynski2 Approximately half of patients present with advanced stage disease, with around 60 per cent receiving palliative intent from the outset.Reference Begbie, Douglas, Finlay and Montgomery3,Reference Timon and Reilly4 Half of all head and neck SCC patients die from their disease and will require palliative input in some form.Reference Schenker, Arnold and Bauer1,Reference Nilsen and Johnson5 Of the variable subsites of head and neck SCC, laryngeal cancer has been reported as having the best five-year survival rate.Reference Berrino and Gatta6
Predicting outcomes in patients with head and neck SCC treated with palliative intent is fraught with difficulty because of the variable nature of why the decision to embark on the palliative pathway has been taken. Often reported outcomes are for patients with head and neck SCC as a single group,Reference Begbie, Douglas, Finlay and Montgomery3,Reference Timon and Reilly4 which therefore need to be interpreted with a degree of caution as head and neck cancers can include a range of subsite primaries and cancer pathologies. Reported survival has been reported to range from days to years.Reference Begbie, Douglas, Finlay and Montgomery3,Reference Timon and Reilly4,Reference Kowalski and Carvalho7
There are several palliative interventions available to patients with laryngeal cancer, including open and trans-oral surgery, radiotherapy, chemotherapy and multi-modal interventions. A wide range of supportive measures are available to maintain and facilitate nutrition and communication, and manage symptom control. Any intervention will have risks that can negatively impact the patient's quality of life, including prolonged hospital stay or surgical complication. It is important to ensure a patient-centred plan is adopted and to ensure the patient's perspective and wishes are at the centre of the decision-making process.
This study aimed to elucidate our local practice and outcomes with regard to patients with laryngeal SCC managed with palliative intent from the outset. It is intended that this will better equip clinicians to communicate with patients regarding the palliative management of laryngeal SCC.
Methods
A retrospective analysis of all patients with a new diagnosis of laryngeal SCC presented between July 2010 and June 2016 at the South Glasgow and Clyde head and neck cancer multidisciplinary team (MDT) was undertaken. Patients whose treatment outcome was recorded as palliative intent were identified, and their electronic case records and case notes were reviewed. Clinical and demographic data were recorded. Patients who had undergone initial curative intent treatment but had subsequently been found to have residual disease on re-presentation to the MDT were excluded. Strengthening the reporting of observational studies in epidemiology reporting guidelines were followed for the study.
Participants
A total of 406 patients with laryngeal SCC were referred to the South Glasgow and Clyde head and neck cancer MDT over the study period. Sixty-five patients had outcomes recorded indicating palliative intent treatment following initial MDT discussion and were included in the study.
Results
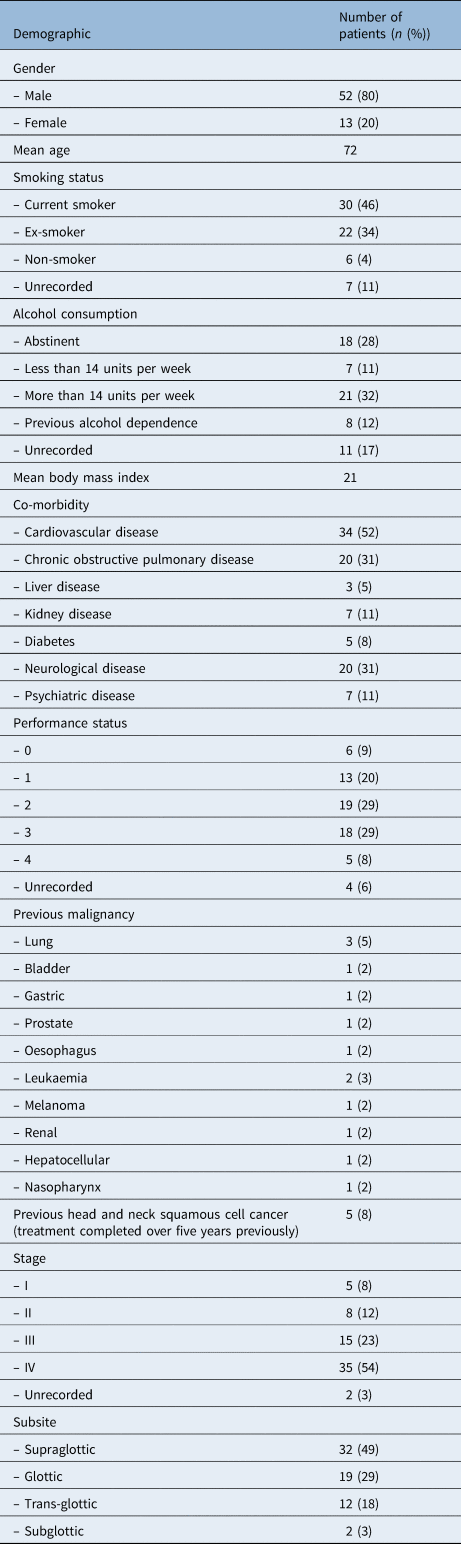
The demographic data for patients were collected and are displayed in Table 1. In total, 80 per cent of patients (n = 53) were male with a mean age of 72, 46 per cent (n = 30) were current smokers and 32 per cent (n = 21) drank more than 14 units per week. The majority of patients had cardiovascular co-morbidities (n = 34, 52 per cent) and a performance status of 2 or more (n = 42, 65 per cent). In addition, 77 per cent of patients (n = 50) had advanced disease, stage III or IV, at MDT presentation.
Table 1. Patient demographics
Survival
At the time of the data collection one patient was still alive and the status of one patient was unknown. Mean survival time from presentation at the head and neck MDT was 211 days (standard deviation (SD) = 279; range, 1–1609 days). With the removal of outliers mean survival time was 143 days (SD = 148.2; range, 1–566 days).
Palliative management
All patients received best supportive care. Nine patients (14 per cent) were offered curative intent treatment, but following discussion with the patient, they declined this. Seventeen patients (26 per cent) had cancer which was deemed incurable and 10 (15 per cent) had a potentially curable cancer, but because of the presence of a second incurable malignancy were deemed palliative. In addition, 29 patients (45 per cent) had potentially curable disease, but because of medical co-morbidities they were not candidates for curative intent treatment.
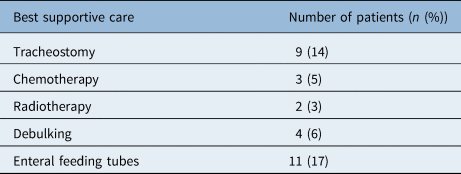
Table 2 outlines the interventions that were used for best supportive care. Nine patients (14 per cent) underwent tracheostomy and 3 (5 per cent) required their tracheostomy prior to discussion at the MDT. The mean time from tracheostomy to discharge was 48 days (range, 11–90 days). The mean time from tracheostomy insertion to death was 201 days (range, 42–232 days). The overall survival time from MDT for patients who underwent tracheostomy was a mean of 278 days (range, 63–1031 days). Four patients (6 per cent) underwent debulking surgery, with mean survival of 214 days and mean hospital stay of 1 day.
Table 2. Best supportive care treatment
Discussion
Over the course of the study period, 16 per cent of patients referred to the MDT with laryngeal SCC embarked on a palliative pathway from the outset. This is comparable to other studies reporting rates of 20.8 per cent for oral cancer, 25 per cent for hypopharyngeal cancer and 21.5 per cent for head and neck cancer.Reference Begbie, Douglas, Finlay and Montgomery3,Reference McMahon, Robertson, Liew, McManners, Mackenzie and Hislop8,Reference Pracy, Loughran, Good, Parmar and Goranova9 The patients’ co-morbidities had an impact on the decision-making process. Furthermore, 60 per cent of patients (n = 39) had potentially curative disease, but ultimately had palliative treatment due to significant co-morbidities or synchronous malignancies.
Overall, 54 per cent of patients (n = 34) presented with American Joint Committee on Cancer stage IV disease. This is lower than the reported rates for head and neck cancer as a whole.Reference Begbie, Douglas, Finlay and Montgomery3,Reference Ledeboer, Van der Schroeff, Pruyn, de Boer, de Jong RJ and van der Welden10 This may be because whilst in head and neck cancer the presenting symptoms can be non-specific, in laryngeal cancers, many patients present with voice change. There have been significant efforts to educate referring physicians of the potential for voice change to be a symptom of sinister pathology. Data from the English National Cancer audit have shown that hoarseness as a sole presenting symptom in laryngeal cancer reflected around 70 per cent of stage I–III disease,Reference Koo, Swann, McPhail, Abel, Elliss-Brookes and Rubin11 therefore early referral of patients with persistent hoarseness may identify laryngeal cancer at a less advanced stage.
Risk factors for laryngeal cancer include smoking and alcohol consumption, which are also risk factors for respiratory and cardiovascular disease. It was found that 80 per cent of patients (n = 52) in this study were current or ex-smokers and most patients had cardiovascular co-morbidities (n = 34, 52 per cent). The treatment modalities for laryngeal SCC carry significant consequences and risk of complication. It is paramount that prior to embarking on a curative treatment pathway, the possible survival benefits are weighed up against the potentially negative impact on quality of life for the patient. Interruption to radiotherapy has been shown to be associated with a poorer prognosis in the treatment of head and neck cancer because it is thought that cancer cells may initially accelerate regrowth after the start of radiotherapy.Reference Duncan, MacDougall, Kerr and Downing12
Synchronous primaries were identified in 17 per cent of patients, with the most common being lung malignancy. This is consistent with other published dataReference Nikolaou, Markou and Petridis13 and is perhaps expected with the common risk factors between laryngeal cancer and lung cancer.
Mean survival was 210 days. This is slightly longer than the mean survival times published for head and neck cancers as a whole.Reference Begbie, Douglas, Finlay and Montgomery3,Reference Ledeboer, Van der Schroeff, Pruyn, de Boer, de Jong RJ and van der Welden10 There was a wide range of survival times, which is most likely due to the heterogeneity of the reasons behind embarking on a palliative route. This illustrates the need for well-established support systems to be in place to help these patients through their journey.
Tracheostomy is an intervention that can secure the airway and provide symptomatic relief in airway obstruction. Our data show a longer mean survival in patients who had a tracheostomy, but also a mean hospital stay of 48 days following tracheostomy, with the associated long-term care consequences. In some of the non-tracheostomy cases, tracheostomy was deemed either inappropriate or the patient had refused tracheostomy. A common reason for patients to refuse tracheostomy was the concern that they may not be able to return home and would require either a care placement or to remain in hospital. In this case series, 8 of the patients (89 per cent) were discharged home or to a relative following their tracheostomy placement.
• It was found that 16 per cent of patients with laryngeal squamous cell cancer were treated with palliative intent from the outset
• In this study population, 54 per cent of patients presented with American Joint Committee on Cancer stage IV disease
• Forty-five per cent of patients in this study group treated with palliative intent had potentially curable disease
• Tracheostomy extended mean survival in the patient group, but necessitated a mean hospital stay of 42 days following tracheostomy insertion
• All potential interventions have an impact on a patient's quality of life and the patient must therefore be at the centre of the decision-making process
Debulking surgery had a mean hospital stay of 1 day and has been shown to negate the need for tracheostomy, with a low complication rate.Reference Paleri, Stafford and Sammut14,Reference Chan, To, Wong and Wei15 Debulking surgery can be considered in patients with palliative laryngeal cancer who wish to minimise their hospital stay. It must be emphasised to the patient that this is a temporary measure due to tumour regrowth. In patients suitable for debulking, it is important to carry out careful decision making and a shared airway plan with anaesthetic colleagues.
Conclusion
Realistic medicine is the principle of putting the patient at the centre of the decision-making process. Patients should be involved in the decision-making process where they are able, and all efforts should be taken to provide them with the information needed to make informed decisions. This can be difficult as there is a lack of consensus on how best to manage patients with laryngeal cancer with palliative intent and there is a lack of research in this area. This, coupled with the fact that conversations about end-of-life and palliative care can be challenging and complex, means that the management of patients with palliative laryngeal cancer can be difficult. This case series demonstrates the management of laryngeal SCC in our centre and may help to inform clinicians and patients when making challenging decisions in the palliative setting.
Acknowledgments
Ms Moira Brook and Ms Eva Carson, MDT Coordinators, South Glasgow MDT.
Competing interests
None declared


