


Clostridium difficile is the principal infectious cause of antibiotic-associated diarrhea and colitis,Reference Paredes-Sabja, Shen and Sorg 1 accounting for an estimated 20%–30% of cases.Reference Kelly, Pothoulakis and Lamont 2 The burden of disease is substantial—in a multistate point prevalence study on healthcare-associated infections in 2011, C. difficile infection (CDI) accounted for 12% of all healthcare-associated infections.Reference Magill, Edwards and Bamberg 3 In the same year, the national burden of disease was projected at 453,000 incident infections with 83,000 recurrent cases and 29,300 deaths resulting from these recurrences. 4 Mortality estimates suggest attributable mortality of 6.9% and 16.7% at 30 days and 1 year, respectively.Reference Dubberke and Olsen 5 This health burden also comes with a profound economic toll, estimated at greater than $1 billion per year,Reference Scott 6 further highlighting the urgency for strategies to prevent CDI.
To devise and adopt prevention strategies in inpatient settings, an understanding of the risk factors for CDI is essential. Several conventional risk factors include older age, antibiotic exposure, prolonged hospitalization, immunocompromising condition, or serious underlying illness. 7 Recent literature has demonstrated an association between proton pump inhibitor (PPI) use and increased risk of CDI. A proposed biologic mechanism is that PPI suppresses gastric acid, which is an important host defense mechanism to prevent germination of ingested C. difficile spores.Reference Biswal 8 PPI use may also result in deleterious changes in the human gut microbiome, increasing the risk of CDI.Reference Clooney, Bernstein and Leslie 9 , Reference Seto, Jeradlo, Orenstein, Chia and DiBaise 10
Due to the observed association and plausible biologic mechanisms, the US Food and Drug Administration released a drug safety announcement in 2012 regarding the association between C. difficile and the use of PPIs and concluded that PPIs were associated with increased risk of CDI. 11 Despite concerns for adverse effects, PPI use remains ubiquitous.Reference Gawron, Feinglass, Pandolfino, Tan, Bove and Shintani-Smith 12 , 13 Understanding the magnitude of risk for hospital-acquired CDI with PPI use would inform the potential impact of interventions to optimize PPI prescribing on hospital-acquired CDI rates. We undertook a systematic review to examine the relationship between PPI use and hospital-acquired CDI.
This systematic review evaluates the literature to answer 2 questions: (a) Are PPIs associated with an increased risk of hospital-acquired CDI? (b) If so, what is the magnitude of this association?
METHODS
We conducted this analysis using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis framework.Reference Moher, Liberati, Tetzlaff and Altman 14 We registered this review at the international prospective register of systematic reviews known as PROSPERO on June 21, 2015 (registration number: CRD42015023690).
Data Sources and Searches
Two reviewers (V.A. and A.B.) independently searched MEDLINE (PubMed), Web of Science, Cumulative Index to Nursing and Allied Health Literature, Cochrane Central Register of Controlled Trials, University of York Center for Reviews and Dissemination, and Clinicaltrials.gov. These bibliographic databases were searched for articles published from January 1, 1980, through July 30, 2015. The Web of Science search facilitated the capture of most conference abstracts or proceedings. For completeness, we searched BIOSIS databases for conference proceedings. Details of the search strategies are available in the Online Supplemental Appendix A.
We also searched for ongoing systematic reviews or meta-analyses of studies with the terms “Proton Pump Inhibitor” and “Clostridium difficile infection” at the Cochrane Library Online as of June 11, 2015. Two studiesReference Kwok, Arthur, Anibueze, Singh, Cavallazzi and Loke 15 , Reference Deshpande, Pant and Pasupuleti 16 were identified; however, neither focused solely on hospital-acquired CDI. All medical subject headings of “proton pump inhibitors” and “Clostridium difficile” were searched in the MeSH database available from PubMed’s homepage. Twenty-five and 19 subheadings were found for the term “proton pump inhibitors” and “clostridium difficile,” respectively. Generic brand names of proton pump inhibitors such as “omeprazole,” “lansoprazole,” “dexlansoprazole,” “esomeprazole,” “pantoprazole,” “rabeprazole,” “ilaprazole” were added to the search. Studies with different type, dose, and duration of the adopted proton pump inhibitor(s) were included.
To assess articles by relevance, abstracts were screened for the following inclusion criteria: (1) studies were observational studies or clinical trials, (2) risk of hospital-acquired CDI after taking PPI was evaluated, (3) reported data were quantitative, (4) the article was published in a peer-reviewed journal, and (5) the study presented data in such a way that allowed for calculation of risk or odds ratio. No language restrictions were used. Exclusion criteria consisted of the following: (1) studies evaluated the risks in community-onset CDI cases, community-associated CDI cases, indeterminate-onset CDI cases, and unknown outpatient cases after taking PPI, (2) reported data were qualitative, (3) the article was published as a dissertation, (4) the study population had recurrent CDI defined as relapse of the original infection (ie, endogenous persistence of the same strain) or reinfection (ie, acquisition of a new strain from an exogenous source)Reference Depestel and Aronoff 17 that occurred less than or equal to 8 weeks after the onset of a previous episode,Reference Warny, Pepin and Fang 18 , Reference Walker, Eyre and Wyllie 19 and (5) studies were pediatric, animal-, or lab-based studies.
Study Selection
One reviewer (V.A.) merged search results using a reference management software which facilitated removal of duplicate records. Two independent reviewers (V.A. and A.B) screened all abstracts identified in the initial search.
Data Extraction and Quality Assessment
Our search, conducted on July 2, 2015, yielded 700 articles. Of these, we retrieved 493 abstracts and full-text articles that met eligibility criteria. Fifty-nine duplicate records were removed. A total of 434 articles were screened at the abstract level and 83 full-text articles were screened for eligibility (inclusion and exclusion criteria). Complete search terms, strategy, and results are described in Appendix A. Reviewers identified 23 full-text articles from which data were extracted, as shown in Figure 1. Two reviewers (V.A. and J.T.) independently extracted data from the articles. Any disagreement or discrepancy was settled in consensus with a third investigator (N.S.). Reviewers extracted data using a standard electronic data sheet (Excel; Microsoft). Data extracted included study methods (study design, total study duration, methodology), participants (demographic characteristics, location, diagnostic criteria), exposure (PPI definition, regimen, dose), CDI outcome (definition, measurements), and results.
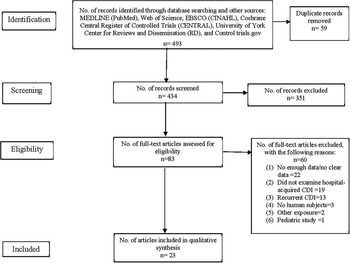
FIGURE 1 Flow diagram of study selection criteria in Preferred Reporting Items for Systematic Reviews and Meta-Analysis framework. CDI, Clostridium difficile infection; CINAHL, Cumulative Index to Nursing and Allied Health Literature.
The quality of case-control and cohort studies was assessed independently by 2 reviewers (V.A and A.B) using the Meta-analysis of Observational Studies in Epidemiology guidelines.Reference Stroup, Berlin and Morton 20
Outcomes
The primary outcome of interest was hospital-acquired CDI, defined in studies by positive stool toxin assay, clinical diagnosis, or International Classification of Disease, Ninth Revision, codes. For our analysis, we extracted data regarding sample size and case frequency, as well as reported odds ratios and risk ratios. Descriptive statistics were used to define the study population. Subgroup analysis was performed to determine how CDI case definition may impact risk of PPI.
Data Synthesis and Analysis
The relationship between PPI and CDI was examined using Review Manager software, version 5.3 (Rev Man; Cochrane Collaboration). We calculated the Cochran χ2 and the I2 statistic to evaluate existence and degree of heterogeneity. A P<.1 for χ2 was used as the cutoff to determine significance of heterogeneity. Significant heterogeneity would mean utilizing a random effects model, whereas a χ2 that was not significant would suggest that a fixed effect model would be adequate.
Assessment of Publication Bias
To assess for publication bias, funnel plots were generated by Rev Man. Funnel plots are used to check for asymmetry in distribution of study results, which aids in identification of studies prone to bias. If bias is present, plots of study variability or sample size against effect size are skewed and asymmetrical.Reference Sterne and Egger 21 Small studies are more likely to have a poor quality and be prone to bias; thus, the trim and fill method of Duval and TweedieReference Duval and Tweedie 22 was followed to detect and correct for any publication bias present.
RESULTS
Study Characteristics
A total of 23 studies assessing the relationship between PPI and CDI were included in this review. Table 1 shows the general characteristics of component studies in the meta-analysis.Reference Al-Tureihi, Hassoun, Wolf-Klein and Isenberg 23 – Reference Wang, Cai, Yu, Huang and Zong 45 Of the 23 component studies, 19 studies were case-control studies, and 4 employed retrospective cohort designs. There were no randomized controlled trials that evaluated the relationship between PPI and CDI and no conference proceedings or abstracts met eligibility criteria. CDI case definitions varied, with the most common case definition being a positive stool toxin assay with associated symptoms (10 studies) or without documented symptoms (11 studies). Two studies defined cases by International Classification of Disease, Ninth Revision, codes.Reference Barletta and Sclar 25 , Reference Pakyz, Jawahar, Wang and Harpe 41
TABLE 1 General Characteristics of Studies Included in Meta-analysis of PPI Use and Hospital-Acquired CDI
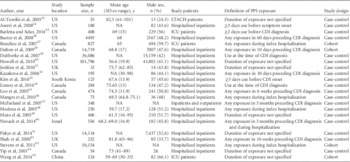
NOTE. CDI, Clostridium difficile infection; ICU, intensive care unit; LTACH, long-term acute care hospital; NA, not available; PPI, proton pump inhibitor.
Sample sizes in studies ranged from 32 to 101,796 hospitalized patients, totaling 186,033 cases. Amongst these studies, 10,307 CDI cases were reported. Studies were from centers around the world: 12 from the United States, 6 from Canada, 2 in the United Kingdom, and 1 each in South Korea, Israel, and China. The mean age of patients amongst the 16 studies that allowed for this calculation was 69.9 years The proportion of males in included studies ranged significantly, from as few as 24.5% to 66.1%. All studies were in hospitalized patients, and 3 studiesReference Barletta and Sclar 25 , Reference Beaulieu, Williamson and Pichette 27 , Reference Wang, Cai, Yu, Huang and Zong 45 were conducted exclusively in ICU patients.
Definition of Exposure
There was no standard definition of PPI exposure. Exposure varied from use of PPI at the time of CDI diagnosis,Reference Baxter, Ray and Fireman 26 to exposure during index hospitalization,Reference Beaulieu, Williamson and Pichette 27 , Reference Manges, Labbe and Loo 36 , Reference Modena, Bearelly, Swartz and Friedenberg 38 , Reference Stevens, Dumyati, Brown and Wijngaarden 43 to any exposure in the previous 90 daysReference McFarland, Clarridge, Beneda and Raugi 37 , Reference Novack, Kogan and Gimpelevich 40 (Table 1). Only 1 study commented specifically upon which PPIs were used.Reference Novack, Kogan and Gimpelevich 40 In this study, PPIs used were omeprazole, lansoprazole, and pantoprazole.
Relationship Between PPI and CDI
Fourteen studies identified a significant association between CDI and PPI, while the association was not statistically significant in the remaining 9. Of these 9, sixReference Beaulieu, Williamson and Pichette 27 , Reference Jenkins, Teoh, Simpson, Dave, Simpson and Breusch 31 , Reference Loo, Poirier and Miller 35 , Reference Manges, Labbe and Loo 36 , Reference Yip, Loeb, Salama, Moss and Olde 44 , Reference Wang, Cai, Yu, Huang and Zong 45 had a trend toward a positive association—that is, an increased risk of CDI with PPI exposure. The remaining threeReference McFarland, Clarridge, Beneda and Raugi 37 , Reference Novack, Kogan and Gimpelevich 40 , Reference Shah, Lewis, Leopold, Dunstan and Woodhouse 42 had nonsignificant odds ratios less than 1 (0.82–0.86).
Our main analysis was performed in 2 subgroups: the 4 cohort studies and the 19 case control studies, as detailed in Figure 2. All cohort studies showed an increased risk of CDI in patients exposed to PPI, with 2 of 4 demonstrating statistical significance. All but 3 case control studies demonstrated a positive association between PPI and CDI, with 12 reaching statistical significance in this relationship. Pooled analysis of cohort studies demonstrated a odds ratio of 1.97 (95% CI, 1.29–2.98), which was statistically significant. Analysis of case control studies revealed an odds ratio of 1.77 (95% CI, 1.46–2.14), which was also significant. There was no difference of overall effect between the subgroups (P<.00001). Pooled odds ratio for all 23 studies was 1.81 (95% CI, 1.52–2.14).

FIGURE 2 Forest plot of the association between proton pump inhibitor (PPI) and Clostridium difficile infection (CDI). The vertical line corresponds to the no-difference point between 2 groups. Horizontal lines represent the 95% CIs. Studies are listed by first author and year.
Subgroup Analysis by Definition of CDI
Subgroup analysis was performed to determine whether CDI case definition altered the strength of association with PPI, as detailed in Figures 4 and 5. In the 10 studies that included symptoms in the CDI case definition, the pooled odds ratio was 1.42 (95% CI, 1.07–1.88). In the 13 studies that did not require symptoms for CDI case definition, the pooled odds ratio was 2.15 (95% CI, 1.74–2.66).
Effect of Confounding Factors on Relationship Between PPI and CDI
Most studies took into consideration one or more of the most common risk factors for CDI: exposure to antibiotic therapy or H2 blockers, renal failure, diabetes mellitus, immunosuppression, malignancy, and gastrointestinal disease. In addition, most studies identified sex, age, and additional comorbidities, such as respiratory illness and length of hospitalization, as potential confounding variables. Given the disparate study designs, patient populations and study locations, we did not attempt to control for the numerous confounding variables identified in component studies. Confounders identified in each of the included studies are detailed in Table 2.
TABLE 2 Intrastudy Risk of Bias, According to Guidelines for Meta-analysis of Observational Studies in Epidemiology, and Confounders Identified in Component Studies

NOTE. In all studies, the study population, outcome, and outcome assessment were clearly defined. APACHE, Acute Physiology and Chronic Health Evaluation; C. difficile, Clostridium difficile; CDAD, C. difficile–associated diarrhea; COPD, chronic obstructive pulmonary disease; H2RA, histamine receptor 2 antagonist; IBD, inflammatory bowel disease; ICU, intensive care unit; LOS, length of stay; NGT, nasogastric tube; PPI, proton pump inhibitor.
Assessment of Heterogeneity and Publication Bias
Significant statistical heterogeneity was found (I2 = 82%), as shown in Figure 3, which was not adequately explained by subgroup analyses to identify sources. Clinical heterogeneity was also present given the differing definitions across studies of exposure as well as confounding variables.

FIGURE 3 Funnel plot to assess the potential impact of publication bias.

FIGURE 4 Forest plot of the association between proton pump inhibitor (PPI) and Clostridium difficile infection (CDI) in those studies defining CDI cases in the presence of symptoms. Studies are listed by first author and year.

FIGURE 5 Forest plot of the association between proton pump inhibitor and Clostridium difficile infection (CDI) in those studies not requiring symptoms for CDI case definition. Studies are listed by first author and year.
By applying trim and fill, it was determined that no apparent publication bias was present.
DISCUSSION
Although several reviews and studies have demonstrated an association between PPI use and CDI, PPIs continue to be widely used among CDI-susceptible populations. Our results show a significant association between PPI use and the incidence of hospital-acquired CDI, lending further evidence to PPI as a risk factor for CDI. Using the relevant available literature, we calculated a pooled odds ratio of 1.81, as shown in Figure 2.
Four previous systematic reviews of similar methodology have studied this question. Tleyjeh and colleaguesReference Tleyjeh, Adbullhak and Riaz 46 performed a meta-analysis of 51 observational studies examining both community- and healthcare-associated CDI, all of which demonstrated a positive association between PPI and CDI, with a pooled odds ratio of 1.65 (95% CI, 1.47–1.85). They estimated the number needed to harm amongst patients receiving PPI concurrent with antibiotic therapy at 50 (95% CI, 31–97); this is significant given the high volume of patients exposed to both classes of medications during a hospitalization. Deshpande et alReference Desphande, Pant and Pasupluleti 47 in 2012 examined the role of PPI in the development of CDI and specifically recurrent CDIReference Deshpande, Pasupuleti and Throta 48 in both the inpatient and outpatient setting. In the review of 30 observational studies by Deshpande et al,Reference Desphande, Pant and Pasupluleti 47 pooled meta-analysis demonstrated greater odds of developing CDI amongst those on PPI (odds ratio, 2.15 [95% CI, 1.81–2.55]). This review also performed subgroup analysis to examine the effect of concomitant antibiotic use on the relationship between PPI and CDI. They found that the higher risk of CDI among PPI users persisted across each subgroup, regardless of the frequency of antibiotic use reported on component studies. In 2015, Deshpande performed a meta-analysis examining the relationship between PPI and recurrent CDI; the pooled risk ratio from 8 studies was 1.58 (95% CI, 1.13–2.21). Garey et alReference Garey, Sethi, Yadav and DuPont 49 found a similar relationship when examining the association between any anti-ulcer medication (PPI and H2 blocker) and recurrent CDI, with a statistically significant pooled odds ratio from 3 studies of 2.149 (95% CI, 1.13–4.08). Previous data have also demonstrated increased risk of severe or severe-complicated CDI in patients receiving PPI.Reference Khanna, Aronson, Kammer, Baddour and Pardi 50
Significant heterogeneity existed across studies, which limited our ability to perform additional analysis regarding potential confounders and CDI outcomes. Despite this heterogeneity, all but 3 studies demonstrated a positive association between PPI use and CDI—that is, PPI exposure appears to increase the risk of CDI significantly. Several confounders were proposed in included studies, many known to be conventional risk factors for CDI: old age, use of antibiotics, prolonged hospital course, immunosuppression, and underlying chronic disease.
Inclusion of symptoms in CDI case definition appears to impact the relationship with PPI, with a less robust association when symptoms were required for CDI case identification. This may suggest colonization is an important mediator in the association between CDI and PPI. Data regarding the proportion with clinically apparent disease in the studies that did not include symptoms in the CDI case definition are not available. Without these data, we cannot comment further on the frequency of colonization in these studies and the contribution to the association between PPI and CDI. The pooled odds ratio in this group remained significant, however, in line with our remaining results and previous studies demonstrating an association between CDI and PPI. Given colonization with toxigenic C. difficile greatly increases the risk of clinical infection,Reference Zacharioudaks, Zervou, Pliakos, Aiakas and Mylonakis 51 reducing risk of colonization is an important aspect of an infection prevention program.
Overuse of PPIs is widespread. In 1 study, 59% of general medical patients receiving PPI did not have a clear indication for use.Reference Reid, Keniston, Heller, Miller, Medvedev and Albert 52 These numbers are similar amongst critically ill patients, with Farrell and colleaguesReference Farrell, Mercogliano and Kuntz 53 citing 68.1% of patients on gastric acid suppression for stress ulcer prophylaxis did not have identifiable risk factors for stress-related mucosal bleeding. Our study highlights the importance of optimizing PPI use as an important component of a CDI reduction program. Barriers to reducing unnecessary PPI use in the inpatient setting should be studied to inform interventions to combat overuse or misuse. With the results of our meta-analysis and the results of the others on this topic, it should now be possible to predict the impact PPI optimization may have on reduction in hospital-acquired CDI rates. Intervention studies in this area are now needed.
Our study has several limitations. First, our results suffer the limitations of the component studies, such as potential selection bias when selecting controls. Secondly, studies were quite heterogeneous in their methods and outcome reporting. Given this heterogeneity, we were not able to independently adjust for potential confounders in the relationship between PPI and CDI. We attempted to control for any significant outliers by developing a priori inclusion and exclusion criteria and applying these stringently. Third, included studies used varying case definitions for CDI infection, potentially contributing to misclassification bias. We have addressed this by performing subgroup analysis. Finally, publication bias is always a potential concern in meta-analyses, and it is possible that studies demonstrating either no association or a negative association between PPI use and CDI are less likely to be published. However, we assessed this using the trim and fill method for publication bias assessment, and publication bias was not identified in our review.
In conclusion, our results provide further evidence that PPIs increase the risk of CDI in hospitalized patients. Given the reported overprescription of PPIs,Reference Reid, Keniston, Heller, Miller, Medvedev and Albert 52 , Reference Buckley, Park and Anderson 54 , Reference Tasaka, Burg and VanOsdol 55 optimization of PPI use in the inpatient setting should be a focus of infection prevention programs. Minimizing inappropriate use may have a significant impact on rates of hospital-acquired CDI.
ACKNOWLEDGMENTS
Financial support. Veterans Health Administration National Center for Patient Safety of the US Department of Veterans Affairs; Veterans Affairs MERIT award (no. I01CX000391 to N.S.); and National Institutes of Health pre-doctoral traineeship (awards UL1TR000427 and TL1TR000429 to A.B.).
Potential conflicts of interest. All authors report no conflicts of interest relevant to this article.
Disclaimer: The views expressed in this article are those of the author(s) and do not represent the views of the US Department of Veterans Affairs or the United States Government.
SUPPLEMENTARY MATERIAL
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/ice.2016.194









