


Introduction
Radiotherapy is the primary treatment modality of nasopharyngeal carcinoma (NPC) mainly due to its deep-seated anatomical location and relatively high radiosensitivity. Conventional radiotherapy (ConRT), which employs coplanar or non-coplanar stationary beams with fixed aperture, has been used to treat NPC for decades. These techniques treat patients in phases and deliver total doses of about 66 and 60 Gy to the primary NP tumour and cervical lymphatics, respectively.Reference Teo, Ma and Chan 1 , Reference Luo, Ye, Yu, He, Li and Liu 2 Despite the local control rate remaining satisfactory for early diseases, radiation-induced complications such as xerostomia, oral mucositis and hypothyroidism have been reported.Reference Zhang, Mo, Du, Wang, Liu and Wei 3 , Reference Lee, Ng and Hung 4 Recently, ConRT has been gradually replaced by the more advanced intensity-modulated radiotherapy (IMRT), which uses dynamic multi-leaf collimator (MLC) to create intensity modulated beams. IMRT usually employs seven to nine beams and delivered target doses of 70–72 Gy and 60–66 Gy to NP and cervical nodal regions, respectively. Because IMRT is able to produce more conformal high dose distribution to the targets that offers a better sparing of organs at risk, relatively higher target dose can be prescribed.Reference Kam, Chau, Suen, Choi and Teo 5 , Reference Peng, Wang and Yang 6 Nevertheless, as the NP is anatomically surrounded by many critical normal structures, post-radiotherapy (post-RT) complications are still common regardless of the radiotherapy techniques.
The parotid gland, which is situated laterally to the NP, is one of the organs at risk (OARs) and is often inadvertently irradiated during radiotherapy.Reference Porter, Scully and Hegarty 7 , Reference Tribius and Bergelt 8 Radiation-induced xerostomia has been reported in patients treated by both ConRT and IMRT,Reference Zheng, Han and Xiao 9 , Reference Wu, Ying and Kwong 10 although the latter presented with a lower incidence. Xerostomia usually starts from the mid-stage of radiotherapy course and persists after the treatment, and its severity is dose dependent.Reference Kam, Chau, Suen, Choi and Teo 5 , Reference Zheng, Han and Xiao 9 Although saliva flow may slowly recover after radiotherapy, full recovery is unlikely and xerostomia can develop into a life-long problem.Reference Dirix, Nuyts and van den Bogaert 11 , Reference Saarilahti, Kouri and Collan 12
Although IMRT has been reported with reduced severity of xerostomia in NPC patients relative to ConRT due to relatively lower mean dose to the parotid gland,Reference Peng, Wang and Yang 6 , Reference Saarilahti, Kouri and Collan 12 , Reference Nutting, Morden and Harrington 13 the pattern of radiation induced geometric changes of the parotid gland, which is associated with the parotid gland function,Reference Wu, Ying and Kwong 10 has not been fully studied. Therefore, the aim of this study was to investigate the differences in the pattern of parotid gland radiologically determined geometric changes during and shortly after radiotherapy between ConRT and IMRT, which was related to the difference in total dose delivered to the parotid gland.
Methods
This was a retrospective study. A total of 56 adult NPC patients, half of them treated by ConRT (n=28) and the other half by IMRT (n=28) between 2011 and 2013 in an oncology department, were randomly retrieved from the patient database. The choice of the radiotherapy techniques was mainly based on the oncologists’ preference and the financial condition of the patients. For the ConRT group, the patients were either treated with three to five coplanar or non-coplanar beams to the NP region, and an anterior cervical beam was used to cover the neck lymphatics. The radiation beams were stationary with fixed apertures using 6 MV photons. The treatment was delivered in two phases in which the second phase treated the clinical target volume with a reduced margin. Prescribed doses of 66–68 Gy and 60–66 Gy in 30–33 fractions were given to the NP and cervical nodal targets, respectively. For the IMRT group, inverse planning was used in which the patients were treated with seven to nine coplanar beams to the facio-cervical region using 6 MV photons. Dynamic MLC were used to generate intensity modulated beams. The clinical target volumes and planning target volumes of both primary tumour and neck lymphatics were treated by simultaneous integrated boost; 70–72 Gy and 60–66 Gy to the clinical target volumes of NP and neck lymphatics, respectively, in 32–35 fractions were prescribed. Both groups of patients were treated in supine head straight position and immobilised with the thermoplastic shell and head rest.
For each patient, planning computed tomography (CT) scan of the head and neck region in the treatment position were performed in the CT-simulator before radiotherapy. Four repeated kilovoltage CT scans were carried out at intervals around 10th, 20th and 30th fractions, and at 3 months after completion of treatment with the patients in the treatment position. After obtaining the CT images, the parotid glands of each patient in the planning CT were contoured in the Eclipse treatment planning system (Version 11; Varian Medical Systems, Palo Alto, CA, USA) for the generation of treatment plan. For the contouring of the parotid glands in the second to last CT sets, deformable registration between the planning CT and subsequent CTs (intervals at 10th, 20th and 30th fractions, and 3 months after radiotherapy) was carried out using MIM software (Version 6.3.4; MIM Software Inc., Cleveland, OH, USA). All the contouring was performed by the same operator who had been trained to conduct parotid gland delineation using CT images. The total mean dose delivered to the parotid glands for each patient was calculated from their respective treatment plans using the treatment planning system.
For the assessment of parotid gland changes, percentage change of volume (Δ%V) and dice similarity coefficient (DSC) were obtained. DSC, which indicated the spatial overlap between two volumes,Reference Zou, Warfield and Bharatha 14 was defined by (V o, V s)=2|V o∩V s| / |V o|+|V s|, where V o and V s were the volumes of original parotid gland and subsequent parotid gland at various time intervals, respectively, and ∩ was the intersection. A value of 1·0 would indicate perfect volume match between the two volumes, whereas 0 would imply no overlapping of volume. Translational displacements in x, y and z axes and total vector displacement (TVD), which was the three-dimensional displacement of the centroid, were obtained by comparing the parotid gland in each subsequent CT with that of the original planning CT using the MIM software. In addition to the parotid gland measurement, the change in lateral dimension of the patient’s head (ΔD L) was also measured which was an indication of the patient’s size. The lateral dimension of the patient’s head was defined as the width of the line perpendicular to the mid-line in the CT slice at level of the superior tip of the odontoid process (Figure 1).Reference Cao, Luo and Xu 15 The average values of each measured parameter for the ConRT and IMRT groups were calculated and compared. Normality test was conducted in each set of data. Independent t-test or Mann–Whitney test was conducted dependent on the normality of the data. All statistical tests were performed using Statistical Package for Social Science version 22 (IBM).
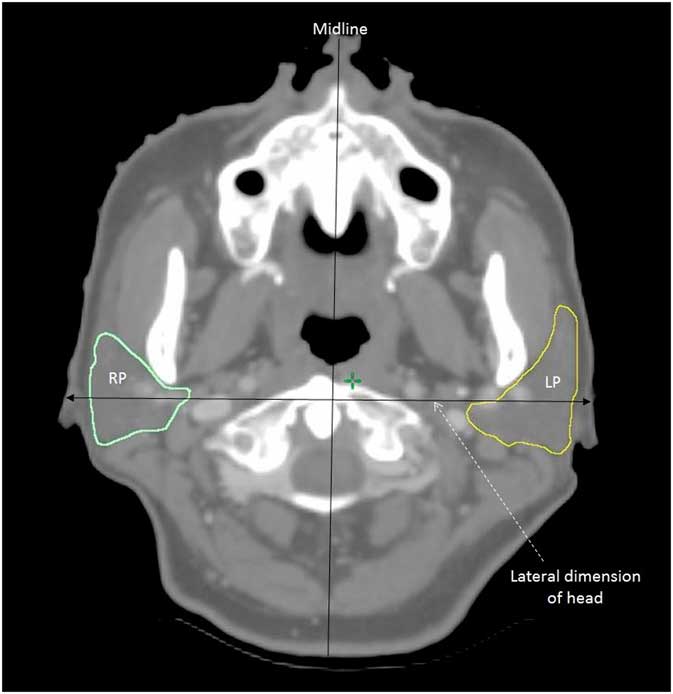
Figure 1 A transverse computed tomographic (CT) slice at the level of the tip of odontoid process showing the measurement of lateral dimension of the head.
Results
Patient characteristics
The age range and gender proportion of the two study groups were similar (Table 1). Over 75% of the patients belong to Stage III and IV (AJCC 2010 system) in both groups. The baseline mean parotid gland volume in the IMRT group was similar to that of the ConRT group (Table 2). The mean parotid gland doses in the ConRT and IMRT groups were 49·1±7·4 Gy and 37·5±9·5 Gy, respectively. The difference in mean parotid gland dose between the two groups was statistically significant (p<0·001).
Table 1 Patient characteristics
Abbreviations: ConRT, conventional radiotherapy; IMRT, intensity-modulated radiotherapy; AJCC, American Joint Committee on Cancer 2010 staging system.
Table 2 Comparison of the baseline (Pre-RT) parotid gland volume between the conventional radiotherapy (ConRT) and intensity-modulated radiotherapy (IMRT) groups
Lateral head dimension
For both ConRT and IMRT groups, the mean lateral head dimension decreased continuously during the radiotherapy course and reached a minimum at 30th fraction interval (Figure 2). Their differences between the ConRT and IMRT group were not significant until at 3 months after radiotherapy where the IMRT group demonstrated smaller ΔD L value than the ConRT group (p=0·017).

Figure 2 Comparison of the mean change of lateral dimension of head between conventional radiotherapy (ConRT) and intensity-modulated radiotherapy (IMRT) plans over the radiotherapy course up to 3 months post-treatment. Note: The horizontal lines indicate the error bars.
Percentage parotid volume change
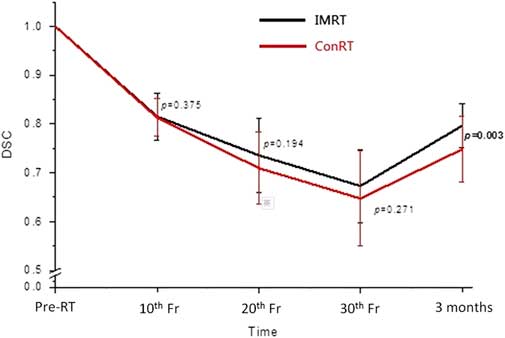
The mean parotid volume in both groups decreased with a maximum reduction of 35% at the 30th fraction (Figure 3). There were no significant differences between the ConRT and IMRT groups from 10th to 30th fractions. Volume recovery was observed in both groups at 3 months following RT with significantly greater recovery in the IMRT group (p=0·007). The trend of DSC was similar to that of the volume change. It decreased from pre-treatment to 30th fraction and partially recovered at 3 months after treatment (Figure 4). Significant difference between ConRT and IMRT was only noted at the 3 months post-RT interval with the IMRT group demonstrating a better restoration of the original shape (p=0·003).
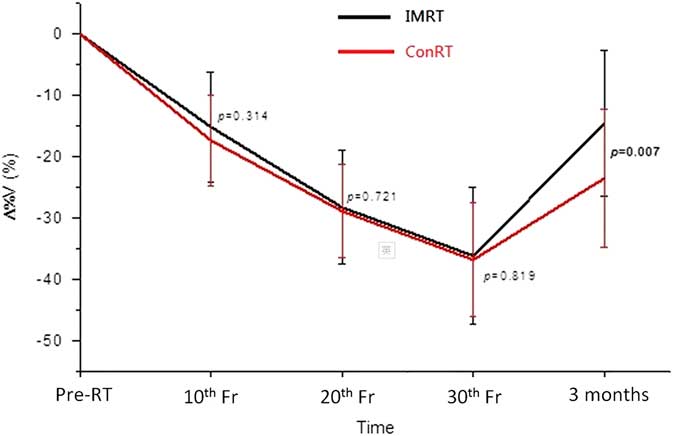
Figure 3 Comparison of the mean percentage change of volumes of parotid glands between conventional radiotherapy (ConRT) and intensity-modulated radiotherapy (IMRT) plans over the radiotherapy course up to 3 months after treatment. Note: The horizontal lines indicate the error bars.
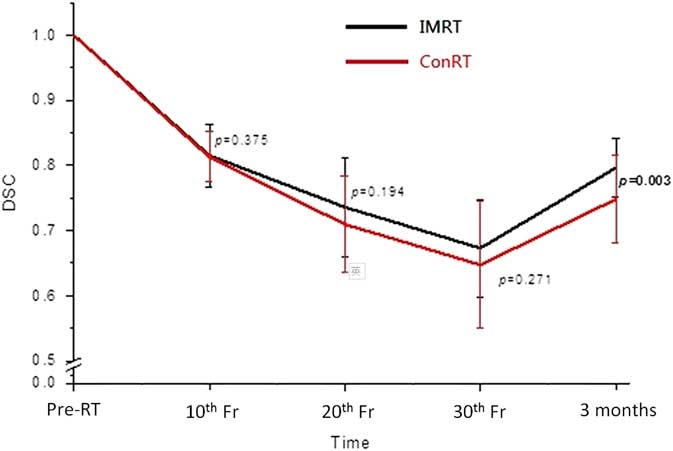
Figure 4 Comparison of the mean dice similarity coefficients (DSC) of parotid glands between conventional radiotherapy (ConRT) and intensity-modulated radiotherapy (IMRT) plans over the radiotherapy course up to 3 months after treatment. Note: The horizontal lines indicate the error bars.
Displacement of parotid gland
The centroid of the parotid gland demonstrated movement during the treatment course, in which the displacement in x- (medio-lateral) direction was the greatest followed by the z- (supero-inferior) and y- (antero-posterior) directions (Table 3). At 30th fraction, the centroid had moved medially, superiorly and posteriorly from the original position. This pattern was demonstrated by both ConRT and IMRT groups, and there were no significant differences in displacement between the two groups. For both groups, the TVD of the centroid demonstrated an increasing deviation during the treatment course, and then moved back to some extent at 3 months after treatment (Figure 5). The ConRT group showed greater TVD than the IMRT group, but their differences did not reach statistical significance except at 3 months post-RT interval (p<0·001).
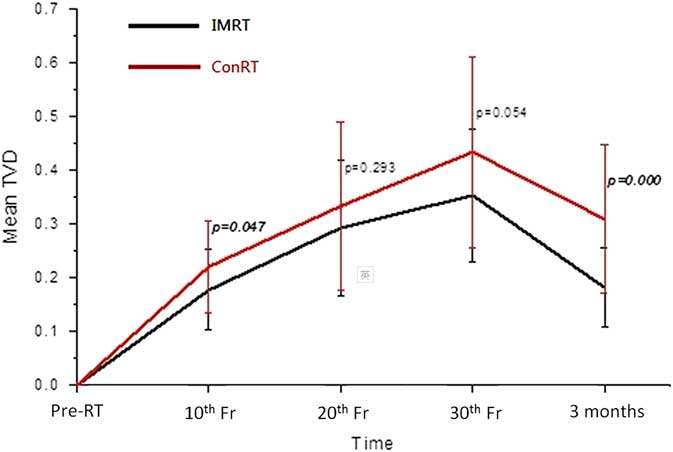
Figure 5 Comparison of the mean total vector displacement (TVD) of centroid of parotid glands between the conventional radiotherapy (ConRT) and intensity-modulated radiotherapy (IMRT) plans over the radiotherapy course up to 3 months after treatment. Note: The horizontal lines indicate the error bars.
Table 3 Displacement of the centroid of the parotid gland along the x, y and z axes at 30th fraction for the conventional radiotherapy (ConRT) and intensity-modulated radiotherapy (IMRT) groups
Notes: Δx=deviation along the x-direction (medio-lateral): -ve=towards mid-line; +ve=away from mid-line.
Δx=deviation along the y-direction (antero-posterior): -ve=towards posterior; +ve=towards anterior.
Δx=deviation along the z-direction (supero-inferior): -ve=towards inferior; +ve=towards superior.
Discussion
With regard to the geometric changes of the parotid gland during radiotherapy, our study demonstrated that there were no significant differences between patients treated by ConRT and IMRT. For both groups of patients, the parotid gland demonstrated continuous shrinkage and medial migration during the treatment course. They were reflected by the increase of Δ%V, DSC and TVD from pre-treatment to 30th fraction, respectively. The shrinkage of parotid glands during radiotherapy has been reported in previous studiesReference Barker, Garden and Ang 16 , Reference Zhang, Lin and Wu 17 and it was mainly caused by the loss of gland parenchyma and acinar cell atrophy due to high dose radiation.Reference Radfar and Sirois 18 , Reference Wang, Yan and Zhang 19 The volume reduction of the parotid gland subsequently changed its shape and therefore resulted in a similar trend in DSC as for Δ%V. This medial migration of the parotid gland during radiotherapy was caused by the shrinkage of radiosensitive NP tumour, which was situated medially to the parotid gland and created space for the parotid gland to move in. Another associated factor could be due to the weight loss of the patients, whose head size became smaller leading to the lateral structures moved closer to the mid-plane. Actually such medial movement of the parotid gland during radiotherapy course has been reported by some studies.Reference Fung, Wu and Teo 20 , Reference Barker, Garden and Ang 21 Our study has shown that NPC patients generally had gradual weight loss during a course of radiotherapy. This was reflected by the reduction of the lateral head dimension. The phenomenon of weight lost, however, may vary across other institutions depending on nutritional support given. This is a common phenomenon for head and neck cancer patients as a result of poorer nutritional status due to radiation induced oral mucositis and xerostomia. The effect would be compounded with concurrent chemotherapy, which is commonly applied for stage II disease or above for NPC patients.
Due to the better target dose conformity in IMRT plans, they were more effective in sparing the parotid gland than the conRT plans in NPC patients. This was proven in our study in which the average mean parotid dose of the IMRT group was about 12 Gy lower than that of the ConRT group. This was also the reason that higher prescribed dose to the target could be given in IMRT than in ConRT plans, which subsequently led to better tumour control.Reference Au, Ngan and Ng 22 , Reference Yan, Cao and Wang 23 Although the geometric changes of the ConRT group appeared relatively greater than that of the IMRT group during the radiotherapy course, their differences did not reach significance. This implied that the extra dose delivered by the ConRT to the parotid gland did not lead to significant geometric change during the treatment course. The possible reasons were because the mean doses of both groups had already exceeded the recommended tolerance mean dose of 25 Gy,Reference Deasy, Moiseenko and Marks 24 the extra dose delivered by the ConRT would not cause significant increase of parotid gland damage. Nevertheless, the results obtained at 3 months after treatment demonstrated that IMRT plans showed better recovery of parotid gland volume, shape and centroid position. For instance, the mean parotid volume returned to 85% of pre-treatment volume in IMRT group, compared with 75% in ConRT group. This indicated that although the rate of parotid gland damage was similar during the course of radiotherapy, the rate of recovery after completion of treatment was different between the two techniques. It has been reported that parotid recovery took place after completion of radiotherapyReference Hey, Setz and Gerlach 25 which were in line with the geometric changes obtained in our study. In addition, study by Hey et al.Reference Hey, Setz and Gerlach 25 reported that the recovery process of the parotid gland could be dose dependent. It was also proposed in some studies that stem cells in the parotid gland were responsible for the post-RT repair if they were not eliminated in the treatment course.Reference Feng, van der Zwaag, Stokman, van Os and Coppes 26 As the more conformal IMRT plans are better equipped to limit the high dose to a smaller volume, and deliver lower mean dose to the gland, it can help to preserve more stem cells in the gland and facilitate better recovery. The improved recovery of the parotid gland in the IMRT cohort may be attributed to this improved opportunity for stem cell recovery.
This study is the first to demonstrate that in radiotherapy of NPC patients, the geometric changes of parotid gland started at around the 2nd week of the radiotherapy course. Despite the changes in ConRT and IMRT during the radiotherapy course remain similar, patients in the IMRT group showed better parotid gland recovery after treatment. One limitation of this study was that the use of the parotid gland size as a surrogate measure for its function has not been proven, although there have been studies reported that the geometric changes of the parotid gland was associated with saliva production.Reference Wu, Ying and Kwong 10 , Reference Teshima, Murakami and Tomitaka 27 Another limitation of this study was that we could not conduct examinations after 3 months post-RT and changes of the parotid gland at later stages was not assessed. Therefore, studies with longer follow-up duration are suggested to evaluate the long-term difference between the two techniques. In addition, assessment of the salivary flow rate and patient xerostomia condition feedback at a longer follow-up time would reveal more information.
Conclusion
In the radiotherapy of NPC patients, both ConRT and IMRT demonstrated similar degree of parotid gland shrinkage and shifting during the radiotherapy course. However, the recovery of the parotid gland volume after treatment was more significant in the IMRT group. Our study demonstrated lower parotid dose from the IMRT technique brought about better volume recovery of the gland shortly after completion of radiotherapy.
Acknowledgements
None.
Financial support
None.
Conflict of interest
None.
Ethical standards
All procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committee of Sun Yat-sen University Cancer Center.








 Open access
Open access