


According to Imaizumi (Reference Imaizumi2015), the infant mortality rates (IMRs) for monozygotic (MZ) and dizygotic (DZ) twins decreased by one-half from 1995 to 2007 in Japan, where the rate was two times higher in MZ than in DZ twins. As for maternal ages, IMRs for both MZ and DZ twins were significantly higher at maternal ages of <20 years than in other maternal age groups. Similarly, the IMRs in MZ twins significantly decreased from 696 (per 1000 live MZ twin births) at gestational age (GA) <24 weeks to 3 at 37 weeks, except at 36 weeks. Corresponding IMRs in DZ twins significantly decreased from 589 at GA < 24 weeks to 1.9 at 39 weeks (except at 36–38 weeks) and significantly increased to 4.8 at ≥40 weeks.
According to Blickstein and Kalish (Reference Blickstein and Kalish2003), approximately 75% of live intrapair twins showed <15% birth weight discordance (BWD). Between co-twins (concordant), 20% were 15–24% (mildly) discordant, and approximately 5% were ≥25% (severely) discordant. Tobe et al (Reference Tobe, Mori, Shinozuka, Kubo and Itabashi2010) also reported these proportions using a nationwide obstetric database of Japanese twins from 2001 to 2005. In the Japanese population, severe discordance was 10%, a value that was two times higher than in the Caucasian population.
BWD is a risk factor for perinatal mortality in the USA (Branum & Schoendorf, Reference Branum and Schoendorf2003; Kim et al., Reference Kim, Caughey, Yee and Cheng2019), Japan (Kato & Matsuda, Reference Kato and Matsuda2006) and Canada (Jahanfar et al., Reference Jahanfar, Lim and Ovideo-Joekes2017). It is also a risk factor for neonatal mortality (Branum & Schoendorf, Reference Branum and Schoendorf2003; Demissie et al., Reference Demissie, Ananth, Martin, Hanley, MacDorman and Rhoads2002; Kim et al., Reference Kim, Caughey, Yee and Cheng2019; Mazhar & Kanwal, Reference Mazhar and Kanwal2010; Tobe et al., Reference Tobe, Mori, Shinozuka, Kubo and Itabashi2010).
The present study examines the relationship between IMRs and BWD levels among MZ and DZ twins. It also examines the effects of GA groups (<28 weeks and ≥28 weeks) and between two periods (1995–2001 and 2002–2008) on the relationship between IMRs and BWD levels.
Materials and Methods
Data Sources
Data on live births and infant deaths between 1995 and 2008 were obtained using Japanese vital statistics records. The Statistics and Information Department, Ministry of Health, Labour and Welfare (Tokyo, Japan) maintains records covering the entire Japanese population. Records in the form of live birth certificates include details about the nationality, sex, birth date, address, GA, birth weight (BW), parental birth dates and ages, single or twin births and birth order of twins. Death certificates contain the same information as live birth certificates (excluding paternal age) as well as the date of infant death.
Data Analysis
In the present study, 154,578 live-born twin pairs (309,156 live-born twins) were estimated using the Weinberg (Reference Weinberg1901) method as 128,236 MZ and 180,920 DZ twins. These data were used as denominators to compute the IMRs according to BWD levels. Intrapair BWD was computed as follows: higher BW minus lower BW divided by higher BW and multiplied by 100. This formula is also used to compute infant deaths. Number of infant deaths consists of two categories: live intrapair twins with both infant deaths (2Ds) and a surviving twin with an infant death (D). The former infant deaths were 553 twin pairs (1106 infant deaths) and the latter were 2372 infant deaths. Using the Weinberg method, these numbers of infant deaths (3478) were estimated as 1858 in MZ and 1620 in DZ twins. BWD levels were classified into the following seven groups: <5%, five groups from 5–9% to 25–29%, and ≥30%. The relationship between IMRs and BWD levels was computed for both types of twins. The relationship was also computed among two GA groups (<28 and 28 weeks≥) and for two periods (1995–2001 and 2002–2008).
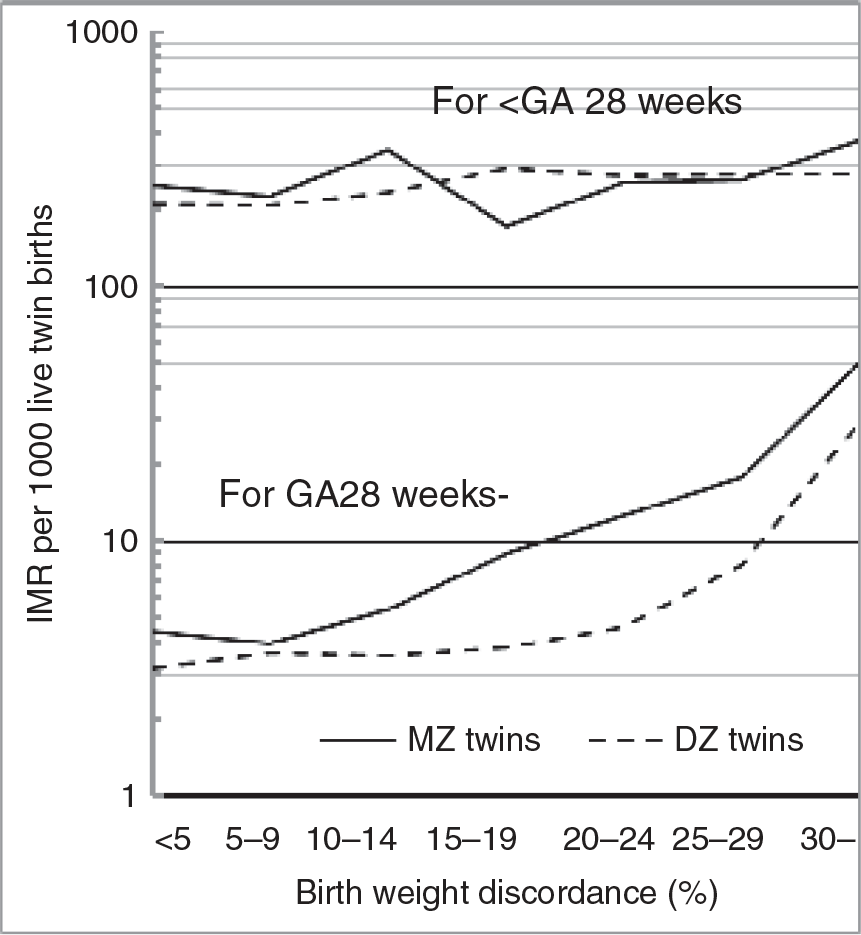
Fig. 1. Relationship between infant mortality rate (IMR) for zygotic twins and discordance levels among two gestational age groups (GA < 28 weeks and GA ≥ 28 weeks).
Results
Frequencies of BWD among Live-Born Twin Pairs
Table 1 shows the distribution of BWD among live twin births during the period 1995–2008. The frequencies of BWD at <5% were 32% in MZ and 26% in DZ twins. The corresponding proportions were at 5–9% for 25% and 24%, at 10–14% for 17% and 19%, at 15–19% for 10% and 13%, at 20–24% for 6% and 8%, at 25–29% for both 4%, and at ≥30% for both 5%, respectively. These proportions decreased with BWD levels, except at ≥30% for both MZ and DZ twins.
Table 1. Live twin births according to birth weight discordance in MZ and DZ twins, 1995–2008
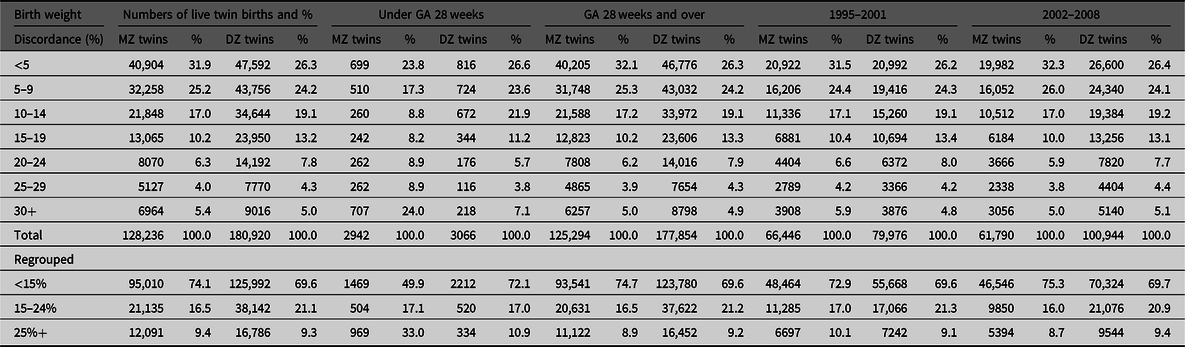
Note: GA = gestational age.
The total number of live-born twins was divided into two GA groups. For births that took place at <28 weeks, the proportions at <5% and at 30%≥ in MZ twins were 24%. In contrast, the corresponding values in DZ twins were 27% and 7%, respectively. The value for MZ twins at ≥30% was 3.7 times higher than that for DZ twins. For births at ≥28 weeks, the value at ≥30% was 5% for both MZ and DZ twins.
The total number of live twin births was divided into two periods: 1995–2001 (old) and 2002–2008 (recent). For the old versus the recent periods, concordant BWD levels at <15% were 73% and 75% in MZ twins. The corresponding values in DZ twins were 70% for both periods. In contrast, severely discordant BWD levels at ≥25% were 10% versus 9% in MZ twins. The corresponding values were 9% for both periods in DZ twins.
Relationship between IMRs and BWD in Twins
Table 2 shows the relationship between IMRs and BWD levels for both MZ and DZ twins according to the survival states of twin pairs: 2Ds, D and total (2Ds plus D). For the 2Ds category, the lowest IMR was at 5 − 9% in MZ (2.4 per 1000 live twins) and in DZ (1.8) twins. The IMRs were significantly higher in MZ than in DZ twins except at two BWD levels (5–9% and 15–19%). The lowest IMR in MZ twins significantly increased with BWD except at 15 − 19% (2.8). Conversely, the lowest IMR in DZ twins only significantly increased at 10 − 14% (2.7). Specifically, the IMRs in DZ twins were similar for each BWD level except at <5% and 10 − 14%.
Table 2. Infant mortality rates for MZ and DZ twins according to birth weight discordance levels, 1995–2008
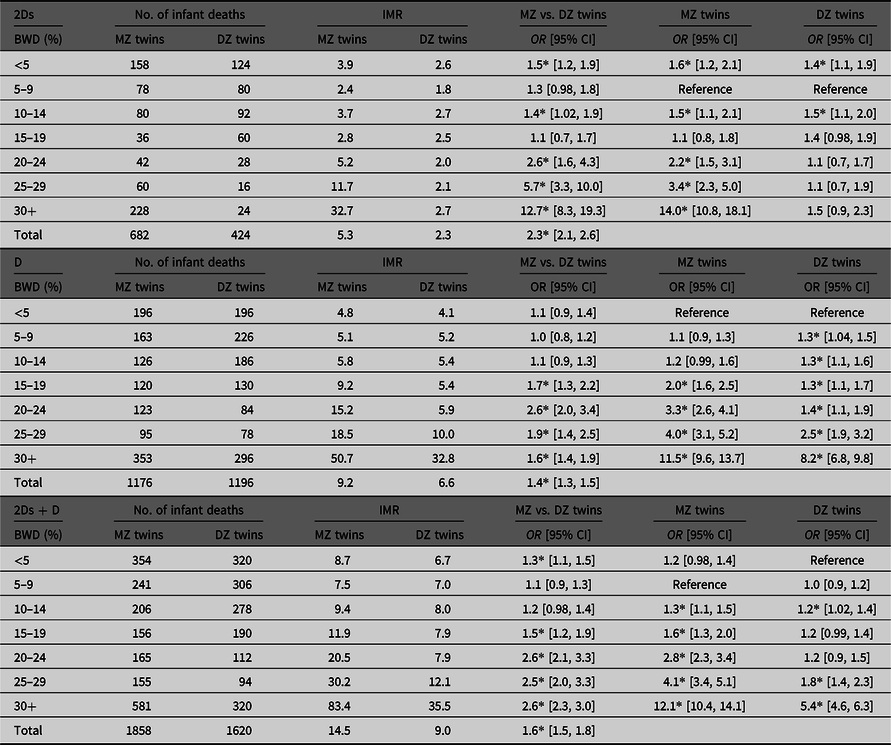
Note: 2Ds are twin pairs with live births and infant deaths. D is a twin pair with live births but only one infant death. IMR (infant mortality rate) is the number of infant deaths per 1000 live twin births. BWD = birth weight discordance. OR = odds ratio. CI = confidence interval.
* p < .05.
For the D category, the lowest IMR was at <5% in MZ (4.8) and in DZ (4.1) twins. IMRs were significantly higher in MZ than in DZ twins from 15–19% (9.2 vs. 5.4) to ≥30% (50.7 vs. 32.8). Among MZ twins, the lowest IMR significantly increased with BWD from 15–19% to ≥30%. In contrast, the lowest IMR in DZ twins significantly increased with BWD from 5–9% to ≥30%.
For total number of infant deaths (2Ds plus D), the lowest IMRs were at 5–9% (7.5) in MZ twins and at <5% (6.7) in DZ twins. IMRs were significantly higher in MZ than in DZ twins except at 5–9% and 10–14%. For MZ twins, the lowest IMR significantly increased with BWD level from 10–14% (9.4) to ≥30% (83.4). For DZ twins, the lowest IMR significantly increased at 10–14% (8.0) and from 25–29% (12.1) to ≥30% (35.5).
Relationship between IMRs and BWD Levels in Two GA Groups
Table 3 shows the relationship between IMRs and BWD levels for both types of twins according to the two GA groups. Table 2 shows the proportions of 2Ds and D among the total infant deaths were 36.7% (682/1858) and 63.3% (1176/1858) in MZ twins. The corresponding values were 26.2% (424/1620) and 73.8% (1196/1620) in DZ twins.
Table 3. Relationship between infant mortality rates in MZ and DZ twins and discordance levels among two gestational age groups, 1995–2008

Note: 2Ds are both twin pairs with live births and infant deaths. D is both twin pairs with live births but only one infant death. BWD = birth weight discordance. IMR is infant mortality rate per 1000 live twin births. GA = gestational age. CI = confidence interval.
* p < .05.
For the group with GA < 28 weeks, the IMRs among the 2Ds category were the lowest at 15–19% (66.1) in MZ and at ≥30% (91.7) in DZ twins. IMRs were significantly higher in MZ than in DZ twins for BWD levels at 10–14% (184.6 in MZ and 107.1 in DZ twins) and at ≥30% (212.2 in MZ and 91.7 in DZ twins). In contrast, IMRs were significantly lower in MZ than in DZ twins at 15–19% (66.1 vs. 151.2) and 20–24% (91.6 vs. 159.1). The lowest IMR in MZ twins was significantly lower than the other values for BWD levels except at 20–24%. Among DZ twins, the lowest IMR was obtained at ≥30%. Therefore, BWD among the 2Ds category was not the risk factor for IMR for both MZ and DZ twins.
For the D category, the IMRs were the lowest at 15–19% (107.4) in MZ and at <5% (93.1) in DZ twins and were similar between twins in each BWD level. Although IMRs in MZ twins were similar in all BWD levels except at ≥30% (164.1), they increased in DZ twins with BWD levels at 10–14% (128.0), 15–19% (139.5) and ≥30% (183.4).
For overall infant deaths (2Ds plus D), the IMRs were the lowest at 15–19% (173.6) in MZ and at 5–9% (207.2) in DZ twins and were significantly higher in MZ than in DZ twins at 10–14% and ≥30%. Conversely, IMRs were significantly lower in MZ than in DZ twins at 15–19%. The lowest IMR in MZ twins was significantly increased at 20–24% and thereafter. In contrast, the lowest IMR in DZ twins was only significantly increased for two BWD levels at 15–19% (290.7) and ≥30% (275.2).
For the group with GA ≥ 28 weeks, IMRs among category 2Ds were the lowest at 5–9% in MZ (0.6) and in DZ (0.3) twins. IMRs were significantly higher in MZ than in DZ twins in each BWD level. The lowest IMR in MZ twins was significantly increased with BWD after 10–14% (1.5), while the lowest IMR in DZ twins was significantly increased at 10–14% (0.6). This suggests that BWD is not a risk factor for IMR among category 2Ds in DZ twins.
For category D, IMRs were the lowest at <5% in MZ (2.9) and DZ (2.6) twins and were significantly higher in MZ than in DZ twins at 15–19% and thereafter. IMRs were significantly increased with BWD level at 10–14% and thereafter in MZ twins and at 5–9% and thereafter, except at 10–14% in DZ twins.
For the overall infant deaths, the IMRs were the lowest at 5–9% (3.9) in MZ and at <5% (3.2) in DZ twins and were significantly higher in MZ than in DZ twins except at 5–9%. As for MZ twins, the lowest IMR significantly increased with BWD from 10–14% (5.4) to ≥30% (50.3), while the lowest IMR in DZ twins significantly increased with BWD from 20–24% (4.6) to ≥30% (29.6).
For births at <28 weeks, the proportions of 2Ds versus D were 0.52 (432/826) versus 0.48 (394/826) in MZ and 0.49 (352/720) versus 0.51 (368/720) in DZ twins. The corresponding proportions for birth at ≥28 weeks were 0.24 (250/1032) versus 0.76 (782/1032) in MZ and 0.08 (72/900) versus 0.92 (828/900) in DZ twins. This suggests that for births at <28 weeks, the proportion of the two categories (2Ds vs. D) was similar among both MZ and DZ twins, whereas for births at ≥28 weeks, the proportions had an effect on the IMRs among MZ twins. See Figure 1.
Relationship between IMRs and BWD Levels between Two Periods
Table 4 shows the relationship between IMRs and BWD levels for MZ and DZ twins between two periods: 1995–2001 and 2002–2008. The proportions of infant deaths for old and recent periods were 59% (1100/1858) and 41% in MZ twins, respectively. The corresponding values were 52% (844/1620) and 48% in DZ twins. Then the ratios decreased by 7% in MZ and increased in DZ twins during the two periods. Decreased proportions of infant deaths in MZ twins led to a reduction in the total IMRs in the overall number of twins.
Table 4. Relationship between infant mortality rates in zygotic twins and discordance levels for 1999–2001 and 2002–2008
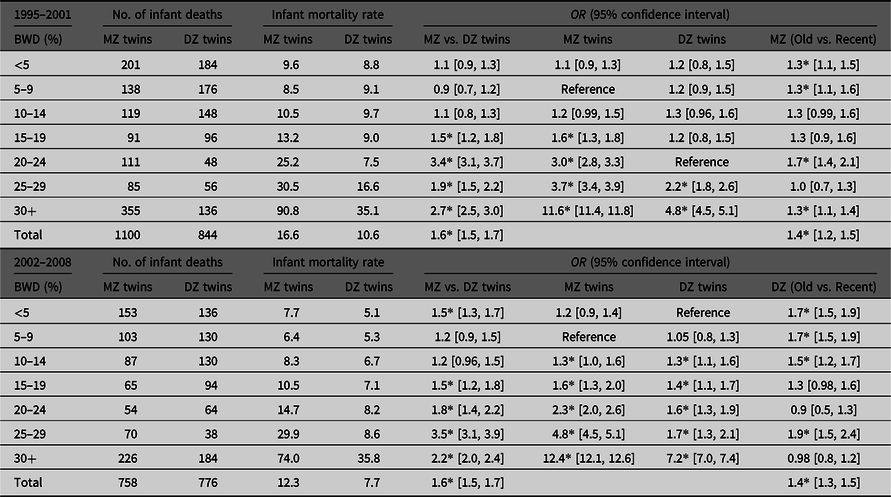
Note: 2Ds are both twin pairs with live births and infant deaths. D is both twin pairs with live births but only one infant death. BWD = birth weight discordance. OR = odds ratio. Infant mortality rate is the number of infant deaths per 1000 live twin births. Old is 1995–2001 and new is 2002–2008.
*p < .05.
IMRs were significantly higher in MZ than in DZ twins in each BWD except at three BWD levels (<15%) in the old period, whereas IMRs were significantly higher in MZ than in DZ twins in each BWD except at 5–9% and 10–14% in the recent period. The lowest IMR in MZ twins was at 5–9% (8.5 for old and 6.4 for the recent period). IMRs were significantly increased with BWD at 15–19% and thereafter in the old period and at 10–14% and thereafter in the recent period. In contrast, the lowest IMR in DZ twins was at 20–24% (7.5) for the old and at <5% (5.1) for the recent period. IMRs were significantly increased with BWD at 25–29% and ≥30% for the old period and were increased with BWD at 10–14% and thereafter in the recent period. As for comparison between the old and the recent periods, the IMRs significantly decreased in the recent than in the old period except at 10–14%, 15–19% and 25–29% in MZ twins and at 15–19%, 20–24% and ≥30% in DZ twins.
Discussion
In Caucasians, approximately 75% live intrapair twins showed BWD of <15% between co-twins (concordant), 20% were 15–24% (mildly) discordant and approximately 5% were ≥25% (severely) discordant (Blickstein & Kalish, Reference Blickstein and Kalish2003). Tobe et al (Reference Tobe, Mori, Shinozuka, Kubo and Itabashi2010) reported that severe discordance was 10.2% from 2001 to 2005 in the Japanese population, a value that was two times higher than that found in Caucasians. Table 1 shows that severe discordance was estimated as 9.4% in MZ, 9.3% in DZ and 9.3% in overall twins. Similarly, mild discordance was 19.2% and concordance was 71.5% for the overall Japanese population. Blickstein and Kalish (Reference Blickstein and Kalish2003) reported proportions of mild discordance that were similar to the results of the present study. In contrast, the proportion of severe discordance was two times higher in Japanese infants than in Caucasian infants, as shown in the results of Tobe et al. (Reference Tobe, Mori, Shinozuka, Kubo and Itabashi2010) and the present study.
Table 2 shows that BWD and adverse IMR in MZ twins were obtained at 10–14% and thereafter. As for DZ twins, the same association was obtained at 10–14%, 25–29% and ≥30%. In contrast, at GA < 28 weeks, shown in Table 3, the relationship between BWD levels and adverse IMRs was obtained at 20–24% and thereafter in MZ twins, whereas the relationship in DZ twins was only obtained at 15–19% and ≥30%. This suggests that at GA < 28 weeks, a short GA may be a risk factor for IMRs in DZ twins rather than BWD.
Tables 2 and 3 show that the proportions of infant deaths at GA < 28 weeks were 44.5% (826/1858) in MZ and 44.4% (720/1620) in DZ twins. Similarly, the corresponding proportions at GA ≥ 28 weeks were 55.6% (1032/1858) and 55.5% (900/1620), respectively. As for GA ≥ 28 weeks, the relationship between BWD and adverse IMR in MZ twins was obtained after 10–14% in MZ twins and after 20–24% in DZ twins.
Table 4 shows that the IMR in MZ twins at ≥30% was significantly higher in the old (90.8) than in the recent (74.0) period, whereas the corresponding rates in DZ twins were the same (35–36). According to Sago (Reference Sago2008), over 300 babies with twin-to-twin transfusion syndrome were treated with fetoscopic laser photocoagulation until April 2008 in Japan. After the operations on these babies, the proportion of survival rate at 6 months was 52% (75/144). The reduced IMRs in MZ twins during the two periods may be associated with the treatment with fetoscopic laser photocoagulation and medical care at <5%, 5–9%, 20–24% and ≥30%. For DZ twins, IMRs significantly decreased at <5%, 5–9%, 10–14% and 25–29% during the two periods which may be associated with medical care.
Acknowledgments
The author is grateful to the staff of Statistics and Information Department, Ministry of Health, Labour and Welfare in Japan.






 Open access
Open access