


Psychiatric disorders are common in general practice and the general practitioner has a pivotal role in the recognition and subsequent treatment of psychiatric disorders. Although psychiatric attention tends to focus on anxiety and depressive disorders, these disorders are not the most prevalent in general practice. Fink et al (Reference Fink, Sorensen and Engberg1999) reported a prevalence of somato-form disorders as high as 30.3%. The comorbidity of somatoform disorders with anxiety and depressive disorders is high (Reference Maier and FalkaiMaier & Falkai, 1999) and the burden of illness may be substantial (Reference Kroenke, Spitzer and de GruyKroenke et al, 1997). A critical review demonstrated that cognitive–behavioural therapy can be effective in treating patients with somato-form disorders (Reference Kroenke and SwindleKroenke & Swindle, 2000). Few comprehensive studies have focused on an accurate quantification of clinically relevant disorders. The aim of the present study was to quantify the prevalence of somatoform disorders and comorbidity with anxiety and depressive disorders in primary care using DSM–IV criteria (American Psychiatric Association, 1994), with a particular emphasis on functional impairment.
METHOD
Study design
The somatisation study of the University of Leiden (SOUL study) was designed as a two-stage prevalence study. In the initial stage, screening questionnaires were used to identify high-risk patients. In the second stage, all high-risk patients and a sample of 15% of the low-risk patients were invited for a psychiatric diagnostic interview. After a follow-up of 6 months, participants with a somatoform disorder will be included in a subsequent controlled treatment study of cognitive–behavioural therapy given by their own general practitioner (not reported here).
Setting
The study took place in eight university-affiliated general practices in The Netherlands. The age and gender distributions are comparable to those of the Dutch population. The electronic medical records of all patients were available through the central database (Registratie Netwerk Universitaire Huisartspraktijken Leiden En Omstreken (RNUH-LEO)) of the family practice registration network of Leiden (13 practices). The database contains diagnostic codings according to the International Classification of Primary Care (ICPC; Reference Lamberts and WoodLamberts & Wood, 1990) for each consultation.
Patients
Between April 2000 and December 2001 a sample of 1778 attendees, aged 25–80 years, was sent the screening questionnaires by mail. After 2 weeks those who had not responded were sent a reminder, including the questionnaires. For each general practice the sample consisted of all consecutive patients on 13–30 arbitrary days within a 3-month period. To avoid problems with language, the study was limited to Dutch natives. Patients were not included if they were unable to participate in an interview because of difficulties such as deafness, aphasia or cognitive impairment. A total of 1046 patients (59%) returned the questionnaire and indicated that they were willing to participate. Data from the RNUH-LEO database allowed fairly detailed analyses of non-response characteristics. Non-response analyses showed that male patients of 25–44 years of age in particular were less willing to participate (response of 46%). When comparing reasons for consultation in the 3 months prior to selection, non-responders did not have more psychological problems (ICPC classification chapter P: 14%) than responders but they did have slightly more social problems (ICPC classification chapter Z: 7% v. 4%). Approximately 50% of both non-responders and responders consulted a general practitioner five or more times in the year prior to selection. Logistic regression modelling showed that after correction for age and gender (which both still have a significant effect) the only other variable with a significant effect was a social reason for encounter (odds ratio=0.6). Social problems are mainly problems in the relationship with a partner or other, mourning and problems related to the work situation.
Questionnaires
Participants completed the SF–36 functional limitation questionnaire (Reference Aaronson, Muller and CohenAaronson et al, 1998) as a measure of functional impairment, the Hospital Anxiety and Depression Scale (HADS; Reference Zigmond and SnaithZigmond & Snaith, 1983) as a measure of anxiety and depression and the Physical Symptom Checklist (PSC; available from the authors on request) to quantify the number of reported physical symptoms.
The first two questionnaires have been validated extensively and described sufficiently elsewhere. In general medical out-patients the total HADS scale has been validated for detecting psychiatric disorders: a cut-off point of 15 gave a sensitivity of 74% and a specificity of 84% (Reference Spinhoven, Ormel and SloekersSpinhoven et al, 1997). The PSC is a checklist of 55 physical symptoms that were mentioned in the DSM–III classification (American Psychiatric Association, 1980) and includes a broad array of symptoms covering most organ systems. The presence of symptoms is rated on a severity scale of 0–3 for the preceding week. A symptom is rated as present for scores 2 and 3. The total score represents the sum of the number of symptoms that are endorsed. In previous studies physical symptoms were a useful severity indicator of somatoform disorders and a fair predictor of medical utilisation (Reference Van Hemert, Hengeveld and BolkVan Hemert et al, 1993; Reference Kroenke, Spitzer and WilliamsKroenke et al, 1994; Reference Speckens, Van Hemert and BolkSpeckens et al, 1996).
High-risk sample
A total score of 15 or more on the HADS or a score of 5 or more on the PSC defined the high-risk sample, which is 48% of the total sample. Of the 506 high-risk patients, 190 patients screened positive on both the HADS and the PSC, 265 patients screened positive only on the PSC and 51 patients screened positive only on the HADS. The choice of instruments and cut-off values for the high-risk sample are somewhat arbitrary because a sample of low-risk patients was interviewed as well. The procedure merely aimed at increasing the number of interview positives for a subsequent treatment study without affecting the prevalence estimate.
Diagnostic interview
Of all the high-risk patients, 80% (404/506) participated in the diagnostic interview. Of the 540 low-risk patients, 15% were invited for diagnostic interview and 84% (69/82) participated. We tried several times to contact non-responders by mail or by telephone. Non-responders to the diagnostic interview were somewhat younger and scored 1.5 points higher on the HADS anxiety sub-scale (possible range 0–21): no differences were found in the number of physical symptoms or functional impairment (SF–36 sub-scales).
The Schedules for Clinical Assessment in Neuropsychiatry (SCAN 2.1; World Health Organization, 1999) were used by World Health Organization-certified psychologists for the psychiatric diagnostic interviews. Throughout the study we held regular sessions with the interviewers to maintain diagnostic standards. During the interview patients were asked about concurrent physical illnesses, and the interviewers made the clinical decision on whether symptoms were ‘unexplained’ or not. The researcher (I.A.A.) supervised all interviews for medical diagnostic data. Whenever necessary, medical diagnostic data concerning symptoms were obtained from the individual general practitioners. When doubt remained, the symptom was regarded as ‘explained’. The scoring algorithm needed to be modified slightly to allow separate and accurate diagnoses of hypochondriasis and somatisation disorder according to the criteria of DSM–IV. The modifications were reported to the World Health Organization task force that is developing the SCAN. Because the overlap between somatoform disorders and anxiety and depressive disorders is the object of this study, hierarchical rules between these disorders were not applied. Within the DSM–IV chapters the hierarchical rules were preserved. All chronic somatoform disorders were diagnosed (duration of at least 6 months): both acute pain disorder and somatoform disorder not otherwise specified were excluded.
An important modification of DSM–IV (compared with its predecessors) is that a severity criterion of ‘significant clinical distress or functional impairment’ has been included in most Axis I disorders. The distinction between Axis I and Axis V has become blurred. From a clinical point of view this modification is well justified, but from an epidemiological point of view the modification introduces an element of subjectivity in the diagnostic process and comparisons with previous studies may have become hampered. We took meticulous care to rate this item separately for each diagnosis throughout all interviews. To analyse the influence of this criterion, the prevalence rates were re-analysed using all criteria of symptoms and duration, with the exception of the severity criterion.
Analyses
Of the 404 high-risk patients interviewed, 116 had a DSM–IV somatoform disorder, 40 had an anxiety disorder and 34 had a depressive disorder. Of the 69 low-risk patients, 3 had a somatoform disorder and 1 had an anxiety disorder. All prevalence estimates and confidence limits were weighted for the sampling procedure (Reference CochranCochran, 1997). To quantify the overlap of somatoform disorders and anxiety and/or depressive disorders, the weighted prevalence and confidence limits for the combinations are given. In addition, we calculated the ratio that represents the factor by which comorbidity exceeds chance expectations: by taking the observed prevalence and dividing it by the prevalence expected by chance. Analyses were conducted using SPSS for Windows 11.0 and MsExcell 97 software.
RESULTS
Prevalence estimates
An estimated prevalence of DSM–IV somatoform disorders of 16.1% was found in a Dutch general practice consulting population (Table 1). The most common somatoform disorder was the undifferentiated somatoform disorder, with a prevalence of 13.1%. These patients suffer from one or more unexplained physical symptoms (e.g. fatigue, headache or gastrointestinal symptoms) that cause clinically significant distress or impairment for at least 6 months. The prevalence of current anxiety disorders was 5.5% and of current depressive disorders was 4.1%. When the new DSM–IV criterion of moderate to severe clinical impairment was ignored (for all diagnoses), the prevalence of somatoform disorders increased from 16.1% to 21.9%, the prevalence of anxiety disorders increased from 5.5% to 7.0% and the prevalence of depressive disorders increased from 4.0% to 6.8%. It must be noted that patients who had no symptoms because of effective medical treatment were not diagnosed. This was a substantial group of patients: use of antidepressants without current significant symptoms was present in 7.4% (95% CI 4.8–9.9) of patients and use of anxiolytics without current significant symptoms was present in 4.5% (95% CI 2.5–6.4) of patients.
Table 1 Estimated prevalence (weighted percentages) of DSM-IV somatoform disorders and anxiety and depressive disorders (with current symptoms) in a consulting population of general practices
| Estimated prevalence: DSM-IV criteria | Estimated prevalence: DSM-IV, including disorders with no or mild impairment | |||
|---|---|---|---|---|
| % | 95% CI | % | 95% CI | |
| Somatoform disorders 1 | ||||
| Somatisation disorder (300.81) | 0.5 | 0.0-0.9 | 0.5 | 0.0-0.9 |
| Undifferentiated somatoform disorder (300.81) | 13.0 | 9.8-16.2 | 17.7 | 13.9-21.6 |
| Pain disorder, chronic (307.××) | 1.6 | 0.7-2.4 | 2.3 | 1.3-3.3 |
| Hypochondriasis (300.7) | 1.1 | 0.4-1.8 | 1.4 | 0.6-2.2 |
| Body dysmorphic disorder (300.7) | - | - | - | - |
| Conversion disorder (300.11) | 0.2 | 0-0.6 | 0.2 | 0-0.6 |
| Total | 16.1 | 12.8-19.4 | 21.9 | 18.0-25.8 |
| Anxiety disorders | ||||
| Panic disorder with or without agoraphobia | 2.72 | 0.9-4.4 | 2.7 | 0.9-4.4 |
| Agoraphobia without history of panic disorder | 0.52 | 0.0-0.9 | 0.5 | 0.0-0.9 |
| Specific phobia | 1.8 | 0.9-2.7 | 3.0 | 1.9-4.1 |
| Social phobia | 0.8 | 0.2-1.5 | 1.4 | 0.6-2.2 |
| Obsessive-compulsive disorder | 0.5 | 0.0-0.9 | 0.8 | 0.2-1.5 |
| Post-traumatic stress disorder | 0.2 | 0.0-0.6 | 0.23 | 0.0-0.6 |
| Generalised anxiety disorder | 0.8 | 0.2-1.5 | 0.8 | 0.2-1.5 |
| Total | 5.5 | 3.5-7.6 | 7.0 | 4.6-8.8 |
| Depressive disorders | ||||
| Major depressive disorders, single or recurrent | 2.9 | 1.7-4.0 | 3.9 | 2.7-5.2 |
| Bipolar disorder | 0.4 | 0.0-0.8 | 0.4 | 0.0-0.8 |
| Dysthymia | 0.8 | 0.2-1.4 | 2.5 | 0.8-4.3 |
| Total | 4.1 | 2.7-5.3 | 6.8 | 4.7-8.9 |
The age and gender distributions of the prevalence figures are summarised in Table 2. The estimated prevalence of somatoform disorders was much lower in patients aged 65 years and over. The same was found for anxiety disorders and depressive disorders. Women tended to have more somatoform disorders (no significant difference). We found no gender differences for anxiety disorders. Depressive disorders were slightly but not significantly more prevalent in females.
Table 2 Patient characteristics and prevalence of somatoform disorders, anxiety disorders and depressive disorders in a consulting population of general practices: disorders to DSM-IV (i.e. moderate to severe clinical impairment) and DSM-IV disorders including disorders with no or mild impairment
| Patient characteristics | No. of patients interviewed (n=473) | Somatoform disorders Weighted prevalence (s.e.) | Anxiety disorders Weighted prevalence (s.e.) | Depressive disorders Weighted prevalence (s.e.) | |||
|---|---|---|---|---|---|---|---|
| DSM-IV | DSM-IV including no/mild | DSM-IV | DSM-IV including no/mild | DSM-IV | DSM-IV including no/mild | ||
| Age group (years) | |||||||
| 25-44 | 169 | 21.8 (15.3-28.3) | 27.8 (20.3-35.2) | 8.7 (4.0-13.4) | 10.4 (5.5-15.2) | 4.1 (1.9-6.3) | 5.7 (3.2-8.3) |
| 45-64 | 234 | 15.3 (10.4-20.2) | 22.4 (16.2-28.7) | 4.2 (2.3-6.1) | 5.8 (3.7-8.0) | 4.9 (2.9-6.9) | 9.7 (5.1-14.3) |
| 65-79 | 70 | 5.4 (1.3-9.5) | 7.2 (2.5-11.8) | 1.8 (0.0-4.2) | 1.8 (0.0-4.2) | 0.9 (0.0-2.6) | 0.9 (0.0-2.6) |
| Gender | |||||||
| Male | 127 | 11.1 (4.6-17.5) | 14.0 (7.4-20.6) | 5.9 (0.0-11.9) | 7.0 (0.9-13.1) | 3.7 (1.5-5.9) | 4.5 (2.1-6.9) |
| Female | 346 | 18.6 (14.7-22.5) | 25.5 (20.7-30.3) | 5.7 (3.8-7.5) | 7.2 (5.2-9.3) | 4.2 (2.6-5.9) | 7.9 (5.1-10.7) |
| Total | 473 | 16.1 (12.8-19.4) | 21.9 (18.0-25.8) | 5.5 (3.5-7.6) | 7.0 (4.8-9.1) | 4.1 (2.8-5.4) | 6.8 (4.7-9.0) |
Comorbidity and functional impairment
The comorbidity of DSM–IV somatoform disorders and anxiety or depressive disorders is considerable (Fig. 1). The observed comorbidity of somatoform disorders and anxiety/depressive disorders was 4.2% (95% CI 2.9–5.5). The expected percentage of comorbidity occurring only by chance was 1.3% (95% CI 1.9–7.2). The observed/expected ratio was 3.3 (95% CI 1.8–6.1). Of all patients with a somatoform disorder, 26% (95% CI 23–28) also had an anxiety and/or depressive disorder: 17% (95% CI 12–23) had an anxiety disorder and 17% (95% CI 12–23) had a depressive disorder. Of all patients with an anxiety and/or depressive disorder, 54% (95% CI 48–60) also had a somatoform disorder.
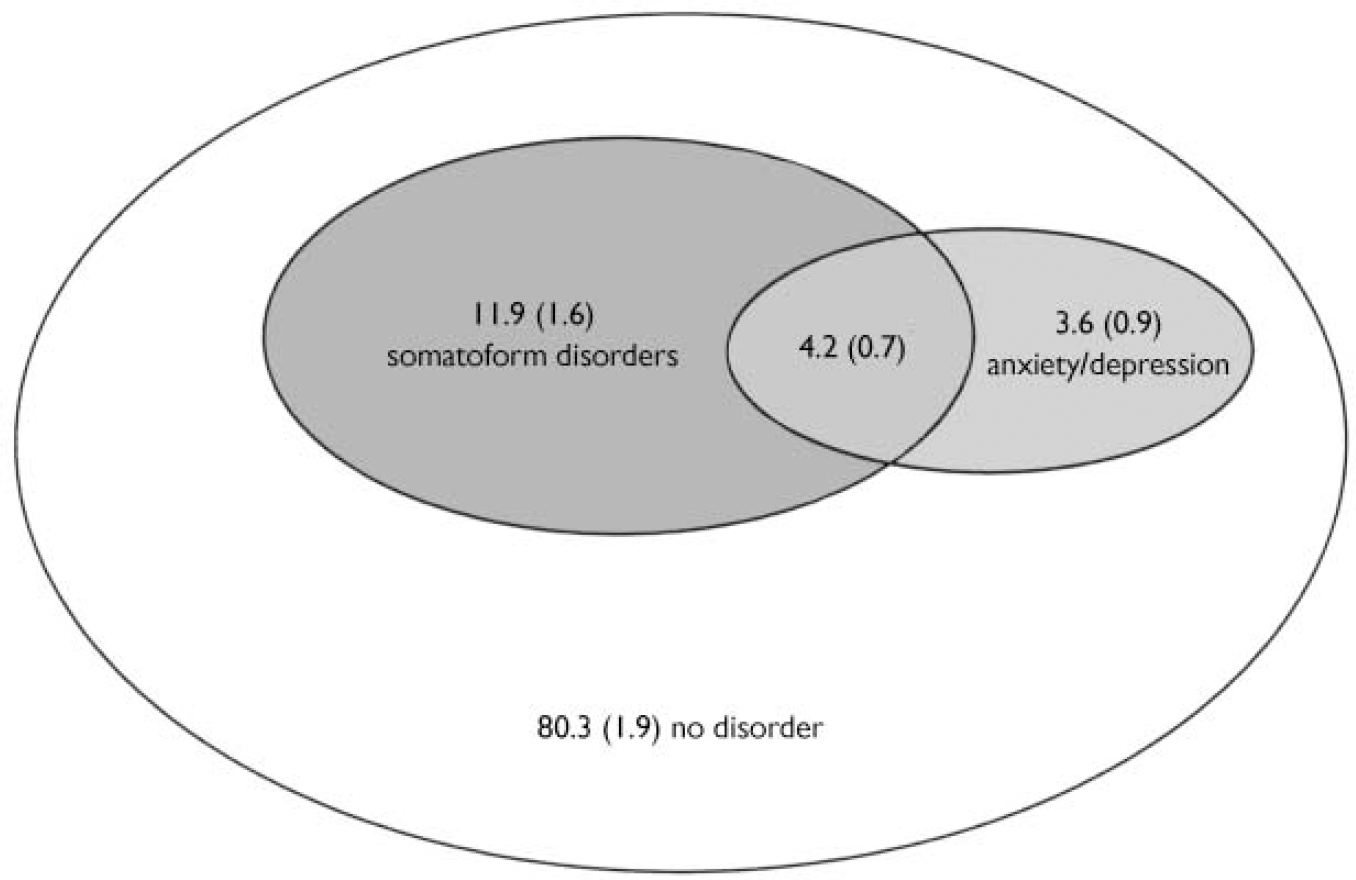
Fig. 1 Overlap between somatoform disorders and anxiety or depressive disorders: weighted prevalence (s.e.). Observed comorbidity, 4.20%; expected comorbidity, 1.26%; ratio=3.3. Within somatoform disorders: 26% anxiety and/or depressive disorders; within anxiety and/or depressive disorders: 54% somatoform disorders.
The symptoms and functional limitations of patients with a somatoform disorder together with an anxiety or depressive disorder are more severe: they add up when comorbidity is present (Table 3). In comparison with patients without disorders, the rating on the PSC was 5.1 (95% CI 2–8) points higher for patients who only had an anxiety or depressive disorder and 5.4 (95% CI 4–7) points higher for patients who only had a somatoform disorder. For the patients with comorbid somatoform and anxiety or depressive disorders the rating was 10.2 points higher (95% CI 7–13), which approximately equals the sum of the increase due to the separate categories. The same applied to the HADS depression scale, whose rating increased by 4.8, 2.2 and 6.9 points, respectively. For the HADS anxiety scale the increase in rating in the subgroup with comorbid disorders (6.5) was less than the sum of the increase in the separate subgroups (5.9 and 2.7, respectively). Functional impairment according to the SF–36 showed a different pattern for somatoform compared with anxiety or depressive disorders. In comparison with patients without psychiatric diagnoses, patients with only anxiety or depressive disorders were most severely limited in their social functioning and in their role functioning because of emotional problems. Patients who only had somatoform disorders were limited in all areas covered by the SF–36. Patients with comorbid disorders were more limited in all areas, and when compared with patients with only somatoform disorders their scores were significantly worse for social functioning, role functioning because of emotional problems and subjective health.
Table 3 Symptoms and functional limitations in patients with or without somatoform disorder (S) and with or without anxiety/depressive disorder (AD): weighted means with 95% confidence intervals
| S- | S- | S+ | S+ | |
|---|---|---|---|---|
| AD- | AD+ | AD- | AD+ | |
| (n=329) | (n=25) | (n=84) | (n=35) | |
| Symptoms | ||||
| No. of physical symptoms1 | 4.4 (4-5) | 9.4 (7-12) | 9.8 (8-11) | 14.7 (12-18)** |
| HADS depression score | 3.3 (3-4) | 8.0 (6-10) | 5.4 (5-6) | 10.2 (9-11)** |
| HADS anxiety score | 4.8 (4-5) | 10.7 (9-13) | 7.4 (7-8) | 11.3 (10-13)** |
| Functional limitations2 | ||||
| Physical functioning | 80 (78-83) | 76 (66-87) | 73 (69-78) | 66 (57-75) |
| Social functioning | 80 (77-82) | 53 (44-62) | 60 (55-65) | 45 (36-53)** |
| Role functioning: physical problems | 66 (61-70) | 53 (35-71) | 34 (25-42) | 29 (16-41)** |
| Role functioning: emotional problems | 84 (79-86) | 33 (17-49) | 51 (41-60) | 22 (11-33)** |
| Pain | 71 (68-73) | 66 (57-76) | 55 (50-60) | 58 (50-66) |
| Subjective health | 66 (64-68) | 56 (48-65) | 54 (50-58) | 44 (38-49)** |
DISCUSSION
Main findings
Our study demonstrates that somatoform disorders are among the most prevalent psychiatric disorders in general practice. A somatoform disorder was diagnosed in 16.1% of consecutive consulting patients. The prevalence of anxiety or depressive disorders was 4.0% and 5.5%, respectively. Comorbidity of somatoform disorders and anxiety or depressive disorders was 3.3 times more likely than could have been expected by chance. More than half the patients with an anxiety or a depressive disorder fulfilled the criteria of a comorbid somatoform disorder. All patients were, by definition, at least moderately impaired owing to their symptoms. Somatoform disorders as well as anxiety or depressive disorders were associated with substantial functional impairment. In patients with comorbid disorders the symptoms and functional limitations increased proportionally, which resulted in a substantially higher burden of illness for patients with comorbid disorders.
Strengths and weaknesses of the study
This is a comprehensive study of the prevalence of strictly defined DSM–IV somato-form disorders, anxiety disorders and depressive disorders in a consulting general practice population, with special emphasis on functional impairment.
The 59% response rate, although not uncommon in primary care, was fairly low for a prevalence study. Selectivity of the responding sample could, in theory, invalidate our prevalence estimates. We addressed this issue with a detailed nonresponse analysis using registered data from the RNUH-LEO database. The response selection was independent of frequency of consultation and of psychological problems, as seen by the general practitioner. Response was comparatively low in the younger males (46%). If they were the healthier subjects, this may have resulted in some overestimation of disorders. On the other hand, social problems were slightly underrepresented in the responding sample, which could have affected the rates towards some underestimation.
The exclusion of somatic disorders as a potential explanation of symptoms is one of the unsolved problems in studies of somato-form disorders. Some form of clinical judgement will have to be involved. In the present study we adopted a cautious approach. The interviewers and the supervising general practitioner made an initial judgement of information provided by the patients. If there was any doubt about the possibility of a somatic disorder as an explanation of the presenting symptoms, additional information was sought from the general practitioner treating the patient. When doubt remained over whether a diagnosis of somatoform disorders was justified, the symptom was regarded as ‘explained’. This may have resulted in an underestimation of the prevalence of somatoform disorders.
Prevalence estimates
When comparing our study with previous prevalence studies, our estimates are relatively low. For DSM–IV somatoform disorders a prevalence estimate of 30% has been found (Reference Fink, Sorensen and EngbergFink et al, 1999). For current depressive disorders previous prevalence estimates were 8% (DSM–IV; Reference Olfson, Fireman and WeissmanOlfson et al, 1997), 11.1–26% (DSM–III–R; Reference Coyne, Fechner-Bates and SchwenkCoyne et al, 1994; Reference Linzer, Spitzer and KroenkeLinzer et al, 1996; Reference Tiemens, Ormel and SimonTiemens et al 1996) and 11.7% (ICD–10; Reference Sartorius, Üstün and LecrubierSartorius et al, 1996). Prevalence estimates for current anxiety disorders were 11.6% (DSM–IV; Reference Olfson, Fireman and WeissmanOlfson et al, 1997), 14.4–18% (DSM–III–R; Reference Coyne, Fechner-Bates and SchwenkCoyne et al, 1994; Reference Linzer, Spitzer and KroenkeLinzer et al, 1996; Reference Tiemens, Ormel and SimonTiemens et al, 1996) and 10.2% (ICD–10; Reference Sartorius, Üstün and LecrubierSartorius et al, 1996). Prevalences rather resembled the rates found in community surveys, for example in Italy (Reference Faravelli, Salvatori and GalassiFaravelli et al, 1997) and The Netherlands (Reference Bijl, Ravelli and van ZessenBijl et al, 1998).
Our lower estimates are most likely due to our strict definition of the disorders. The SCAN interview is known as a high-threshold diagnostic interview with a comparatively strong emphasis on clinically relevant symptoms (Reference Simon, Maier and ÜstünSimon et al, 1995; Reference Brugha, Jenkins and TaubBrugha et al, 2001). In addition, we took meticulous care to rate the criterion of functional impairment that was introduced in most Axis I disorders in the update from DSM–III–R to DSM–IV. It has been demonstrated recently that adherence to clinical significance criteria may reduce the prevalence estimates of anxiety and depressive disorders by approximately one-third (Reference Narrow, Rae and RobinsNarrow et al, 2002). Another explanation for our low estimates could be found in the use of psychotropic medication, which may vary between populations. It is theoretically possible that the prevalence rates could be reduced by 50% or more in a population with optimal treatment. So far, other studies have not reported any figures concerning psychotropic treatment.
Surprisingly, no differences were found by gender for prevalence rates of anxiety disorders, and gender differences for depressive disorders were minimal. This could be due to limited statistical power, because confidence limits, especially in men, were rather large. Another possibility is that our emphasis on impairment contributed to this finding. For depressive disorders (but not for anxiety disorders) the gender differences increased when the DSM–IV criterion of moderate to severe clinical impairment was ignored.
Comorbidity
A high comorbidity of somatoform disorders and anxiety or depressive disorders has been a common finding in previous studies (Reference Barsky, Wyshak and KlermanBarsky et al, 1992; Reference Ormel, Von Korff and UstunOrmel et al, 1994; Reference Escobar, Gara and SilverEscobar et al, 1998; Reference Maier and FalkaiMaier & Falkai, 1999). Functional somatic syndromes are also related to (but not fully dependent on) anxiety and depression (Reference Henningsen, Zimmermann and SattelHenningsen et al, 2003).
Kroenke et al (Reference Kroenke, Spitzer and de Gruy1997) showed that anxiety disorders, depressive disorders, multi-somatoform disorder and somatoform disorder not otherwise specified have independent effects on functional limitations. This study confirms that the symptoms and functional limitations of the disorders can be summated, with the most prevalent somatoform disorders in the present study being undifferentiated somatoform disorder. Patients who have anxiety or depressive disorders are particularly limited in social functioning, role functioning because of emotional problems and subjective health. Patients with somatoform disorders are limited in all areas that are measured by the SF–36. In patients with comorbidity the impairments are summated.
Implications of the study
The findings on comorbidity have implications for the focus of treatment. To engage patients in treatment it is of primary importance to distinguish clearly whether the patient initially presents with psychological or physical symptoms. Patients with a somatoform presentation tend to attribute their symptoms primarily to a physical disorder. The initial motivation for treatment of psychological symptoms will be limited. To engage subjects in a psychologically oriented treatment the somatoform presentation of symptoms should be recognised and dealt with (Reference Sharpe, Hawton and SimkinSharpe et al, 1996; Reference Kroenke and SwindleKroenke & Swindle, 2000). Patients might accept that psychological distress is a consequence of persistent somatic symptoms, or that the relationship is circular (symptoms lead to distress, which, in turn, exacerbates the symptoms).
With DSM–V on the horizon, discussion again has started about the classification of somatoform disorders (Reference Wise and Birket-SmithWise & Birket-Smith, 2002). It has been argued that somatoform disorders are not psychiatric disorders in a strict sense. Indeed, it is not very clear that unexplained physical symptoms are caused by psychological factors. It is clear, however, that there is a strong relationship with anxiety and depression, given that half of the patients in general practice with anxiety or depression suffer from a somatoform disorder as well. The relationship could be due to anxiety and depression causing (awareness of) physical symptoms, or physical symptoms causing anxiety and depression, or there may be a more complex relationship such as a circular causality. Furthermore, a third factor, such as consulting behaviour, could be related to both. In addition to patients with comorbid disorders, many more patients suffer from a somatoform disorder without anxiety or depression. From our study it is evident that both somatoform disorders and anxiety and depression come with substantial functional impairment and that the combination is even worse. A somatoform presentation seems to result from a complex interplay of perception and attribution of symptoms, resulting in unproductive illness behaviour. It has been demonstrated repeatedly that a cognitive–behavioural approach can be effective in alleviating this burden (Reference Kroenke and SwindleKroenke & Swindle, 2000). The inclusion of a well-defined category of somatoform disorders in DSM–V is needed to facilitate further research on the effective treatment of such patients.
Burden of illness and primary care
Somatoform disorders have a major impact on the burden of psychiatric illness. At least one out of six patients seen by a general practitioner has a somatoform disorder. Furthermore, our findings demonstrate that when somatoform disorders occur in combination with anxiety or depressive disorders, symptoms and impairments can be summated. To engage patients in an effective psychological treatment it is important to recognise the somatoform presentation of symptoms. General practitioners should have a strong working knowledge of the principles of diagnosis and treatment of somatoform disorders, as well as of anxiety and depressive disorders.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ Somatoform disorders are among the most prevalent psychiatric disorders in general practice.
-
▪ More than half of the patients with an anxiety or depressive disorder fulfilled the criteria for a comorbid somatoform disorder, which should have implications for the engagement of patients in treatment.
-
▪ In patients with comorbid disorders the physical symptoms, depressive symptoms and functional limitations can be summated.
LIMITATIONS
-
▪ Given a response rate of 59%, selective non-response may have affected our prevalence estimates.
-
▪ In a primary care setting the presence of somatic disorders cannot be ruled out entirely.
-
▪ Comparisons are based on dichotomous groups, with DSM–IVdisorders present or absent. Analyses using a dimensional approach might give more insight into the relationship between depression/anxiety and somatoform disorders.
Acknowledgements
The Netherlands Organization for Health Research and Development (ZON-MW) funded the study. The interviewers were J. E. Piederiet and B. M. Brouwer, with data assistance from L. Hoogenboom and G. Driebergen. We thank J. Ormel. for his comments on an earlier version of this manuscript.





eLetters
No eLetters have been published for this article.