


“Suicide should never be presumed, but must always be based on some evidence that the deceased intended to take his own life” (Reference Mathews and ForemanMathews & Foreman, 1993). The evidence that the coroner seeks to record a suicide verdict must indicate suicidal intent beyond reasonable doubt; when this is not the case, an open (also known as undetermined) or accidental verdict is returned. The inclusion of open verdicts in suicide studies acknowledges the fact that many cases of open verdicts are suicides and that ‘official’ suicide rates per se are underestimates of the real incidence. The Department of Health's (1999) Saving Lives: Our Healthier Nation includes all open verdicts in with suicides when setting national targets for suicide reduction. Thus, it is of importance to understand more clearly the relative contribution of open verdicts to epidemiological studies of suicide.
Our study compares open and suicide verdicts, excluding cases in which suicide was considered either impossible or unlikely. The process of exclusion and its significance is discussed.
METHOD
All cases from the Coroner's Office in Newcastle upon Tyne in which either a suicide or open verdict was recorded were extracted for the period 1985-1994. Information from the coroner's records was recorded in a semi-structured manner onto a data sheet, including social and demographic details, information about the circumstances of the death and relevant clinical background such as psychiatric and medical history.
All open verdicts were assessed by two of the authors (K.R.L. and K.S.) independently. Cases were classified as ‘probable suicide’, or ‘suicide impossible or unlikely’. The small number of cases in which assessment differed was jointly reviewed and, after discussion, a consensus category agreed. Examples of cases of ‘suicide impossible’ included cases of babies found dead, cases of malignant disease (with no suspicion of self-harm) and deaths immediately following surgery. The category of ‘suicide unlikely’ was allocated to cases such as that of a young man who in a state of solvent intoxication fell from a window and of an elderly lady with dementia and who was prone to wander, found drowned in a small stream. In these cases there was no suspicion of suicidal thinking before the event. We identified 188 suicide verdicts (139 males and 49 females) and 185 open verdicts. Of the latter, we excluded 26 cases (suicide unlikely or impossible), leaving a total of 159 open verdicts considered to be probable suicides (99 males and 60 females). The open:suicide verdict ratio (OSR) was 0.85.
RESULTS
Age, gender, civil status, physical health and social class
Of open verdicts, 37.7% were for females compared with 26.1% of suicide cases (χ2=5.45, d.f.=1, P<0.05). The mean age at death for open verdicts was 43.6 years (s.d.=17.3) and for suicide verdicts 47.12 (s.d.=19.2) (unpaired t=test, d.f.=345, P=0.076). There was no significant difference as regards marital status or physical health (χ2=6.59, d.f.=5, P=0.253 and χ2=0.004, d.f.=1, P=0.949, respectively) but there was a significant difference in social class distribution between the two groups (χ2=17.2, d.f.=4, P<0.01).
Psychiatric morbidity
This was recorded in a hierarchical fashion so that if someone had a history of previous in-patient care, out-patient attendance was not also recorded. No significant difference was found (see Table 1) but the high percentage in both groups who had received psychiatric treatment should be noted.
Table 1 Psychiatric morbidity
| Open verdict | Suicide verdict | Level of significance | |
|---|---|---|---|
| % | % | ||
| History of previous deliberate self-harm | 47.4 | 44.7 | NS |
| Psychiatric in-patient treatment (past or present) | 35.6 | 26.9 | NS |
| Psychiatric out-patient treatment (past or present) | 12.9 | 12.9 | NS |
| Psychiatric treatment (past or present) by general medical practitioner only | 9.5 | 15.6 | NS |
Alcohol consumption
Of those with documented alcohol levels (open verdicts, n=149; suicide verdicts, n=186), a significantly greater proportion of those given open verdicts had consumed alcohol at or around the time of suicide (50%, n=74 v. 38.7%, n=72) (χ2=4.04, d.f.=1, P<0.05). A significantly greater proportion of those given open verdicts were judged to be heavily intoxicated (18.1%, n=27), based on blood alcohol levels, than suicide verdicts (9.7%, n=18) (χ2=5.07, d.f.=1, P<0.05).
Suicide notes
Of the open verdicts, 11.3% (n=18) of persons had written a suicide note compared with 49.5% (n=93) in suicide verdicts (χ2=56.1, d.f.=1, P<0.01). As regards the content of the suicide notes in the open verdict cases, in seven cases there was no hint of any suicide intent and in a further seven such intent was not clearly stated but alluded to in a euphemistic manner such as ‘see you in another life’. Four cases stated their intent to kill themselves but three of these were heavily intoxicated and in the remaining case an audio tape with a suicide message was only discovered after the inquest. Among the open verdict cases who had left suicides notes, 55.6% (n=10) had blood alcohol levels indicating intoxication compared with only 13.0% (n=17) of open verdict cases judged intoxicated who had not written notes (χ2=19.34, d.f.=1, P<0.01).
Method of suicide
As can be seen from Fig. 1, there is a significantly higher frequency of hanging (χ2=15.4, d.f.=1, P<0.01) and carbon monoxide (CO) poisoning (χ2=11.3, d.f.=1, P<0.01) in the suicide verdict group, whereas drowning (χ2=6.9, d.f.=1, P<0.01) and ‘falling from a height’ (χ2=4.8, d.f.=1, P<0.05) occurred more frequently within the open verdict group.
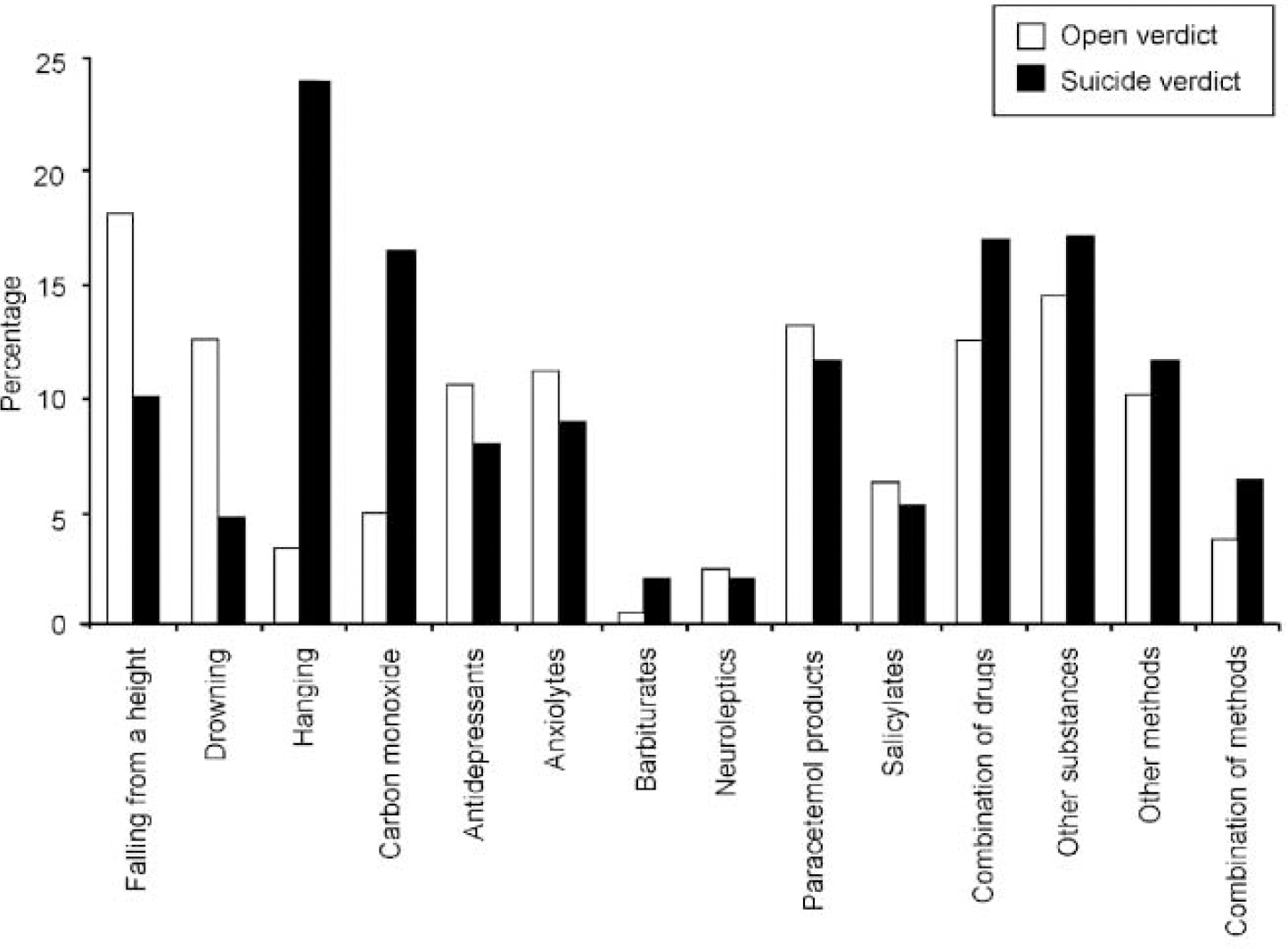
Fig. 1 Methods employed (as histogram).
Influence of exclusions
In Newcastle upon Tyne there has been a considerable change in the pattern of open verdicts recorded since 1961 (see Fig. 2). However, this graph illustrates all open verdicts. In our current series we excluded 26 cases (14%) of open verdicts from the analysis, judging them to be non-suicides. Examination of the 106 open verdicts recorded between 1961 and 1965 resulted in the exclusion of 53 cases (50%) as being ‘non-suicides’: a significant difference from the number excluded in this series (χ2=44, d.f.=1, P<0.01).
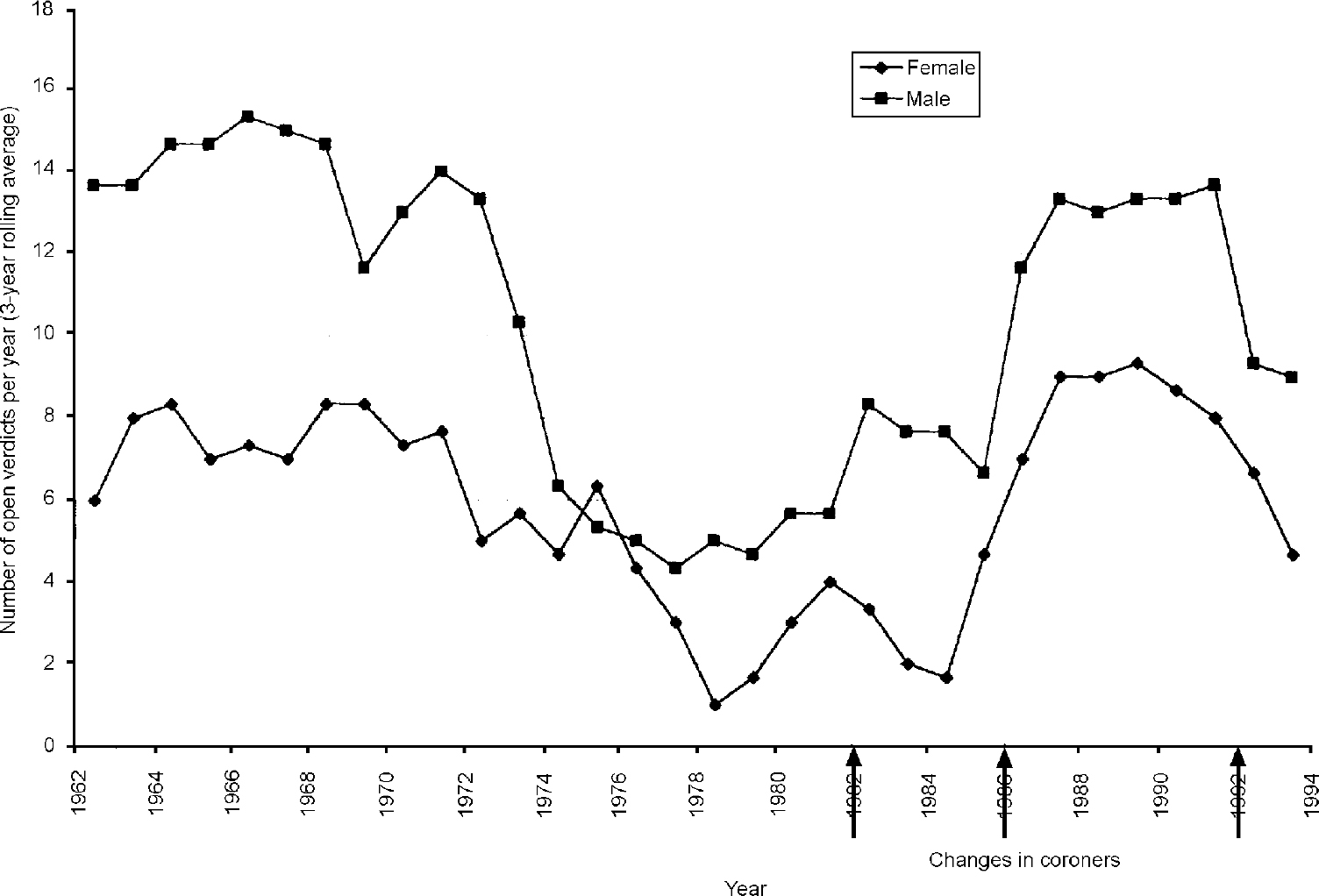
Fig. 2 Open verdicts in Newcastle upon Tyne, 1962-1994.
Discriminating variables
Logistic regression was undertaken to determine which variables were most accurate in discriminating between an open and suicide verdict. A forward stepwise model was used with an admission criterion of P<0.05 and rejection of P>0.1. The most accurate model achieved a correct prediction level of 76.5% (open verdicts 75.9%, suicide verdicts 77.1%). In this model, six variables contribute to the statistical differentiation between suicide and open verdicts (model χ2=111.6, d.f.=6, P<0.001). In descending statistical importance, the variables were: a suicide note, hanging, CO, age, ‘other substances’ and ‘other methods’. ‘Other substances’ refers to any substance ingested or injected not already included and would cover drugs such as insulin or chemicals such as paraquat. ‘Other methods’ refers to those not accounted for already, such as cutting. The number of correct predictions of 261 out of a possible 341 gives a moderate Cohen's κ value of 0.529. Given that 188 (58.3%) out of 347 suicide verdicts could have been predicted correctly by chance, the information available results in a moderate increase in accuracy of prediction.
DISCUSSION
Limitations of suicide research
Suicide rates based on suicide verdicts alone are clearly an underestimate of the true rate, yet including all open verdicts may equally be an approximation. A crucial problem of suicide research, therefore, is deciding which open verdicts to include. We excluded cases in which suicide was considered impossible (e.g. a baby found in a locker) and those in which suicide was unlikely on the grounds of probability. A surprising finding was the variation in the rate of exclusions from 14% (1985-1994) to 50% (1961-1965). This may reflect changes in coroners' practice in the type of case given an open verdict, such that more open verdict cases in the 1960s were genuinely not suicides. However, it is also possible that we experienced difficulty evaluating behaviour from three decades ago, even though we used the same principle (balance of probabilities) in deciding exclusions. We may have erred on the side of negating suicide motives in borderline cases, such as 10 cases of drowning where either heavy intoxication was evident or no information on the circumstances was given, or three cases of CO poisoning which were attributed to potentially faulty gas ovens. Had objective criteria been available, our findings may have been different.
Some papers do not exclude cases (Reference SalibSalib, 1997; Reference Hawton, Fagg and SimkinHawton et al, 1998) while others do not report the number of open verdicts excluded (Reference Vassilas and MorganVassilas & Morgan, 1997), exclusions here being decided on the basis of a panel of three psychiatrists. The precise criteria each used are not stated. Cooper & Milroy (Reference Cooper and Milroy1995) excluded 117 open verdict cases out of 330 (35%), judging them not to be suicides. They give a comprehensive list of criteria on which a decision was made. Appleby et al (Reference Appleby, Cooper and Amos1999) excluded 11.3% of open verdicts if “the coroner's records clearly indicated a suspected cause of death other than suicide”. It is difficult, therefore, to know whether or not different authors use the same criteria and how this affects the relative contribution of open verdicts on their findings. Such variation in practice underlines the need for operational criteria to help decide which open verdicts should be included as suicides, such as have been suggested by Jobes et al (Reference Jobes, Berman and Josselson1987). We are not aware, however, of any criteria which have been validated and assessed for reliability.
The increasing importance of open verdicts to suicide statistics
Nationally, there has been an increasing number of open verdicts. Neeleman & Wessley (Reference Neeleman and Wessely1997) found the OSR in England and Wales increased by a factor of 1.2 (males) and 1.15 (females) every 3 years from 1974 to 1991. However, open verdict cases where suicide was unlikely or indeed impossible were not excluded from their analysis. Moreover, the frequency of such exclusions may vary with the time period, as we have found in our study. The OSR for England and Wales during 1989-1991 was 0.65, making open verdicts a large contributor to suicide statistics. The OSR of 0.85 found in our study is greater than this national rate (and would of course be higher again if we had not excluded 26 open verdicts). This difference may reflect a relatively greater number who drowned or fell from a height in Newcastle, which has the River Tyne spanned by several bridges. Combining our open and suicide verdicts, 77 cases (22.2%) used one of these methods compared with 8% in England and Wales (Office for National Statistics, 1995). This suggests the relative importance of open verdicts varies considerably from area to area, as well as between time periods. As the OSR rises, it becomes increasingly important to ascertain correctly which open verdicts should be included as ‘probable’ suicides.
Comparison of open with suicide verdicts
The comparison of open with suicide verdicts revealed many similarities, although some differences were found. Can we explain these differences based on the fact that a coroner will only arrive at a verdict of suicide based on information which clearly indicates beyond reasonable doubt that the deceased intended to take their own life? A suicide note might be considered such evidence, as would the perceived lethality of the mode of death. Taylor (Reference Taylor1982) has considered these as primary ‘suicidal clues’. Our finding of suicide notes in 11.3% of cases is lower than that reported by Jacobson et al (Reference Jacobson, Bagley and Rehin1976) of 20% of cases, but similar to that of Neeleman et al (Reference Neeleman, Mak and Wessely1997) of 12.8% of cases. Analysis of the notes, however, failed to reveal clear suicidal intent, except in four cases, three of which had blood alcohol levels indicating intoxication. High blood alcohol levels were found in seven other cases of open verdicts where notes had been left. This may have influenced the coroner to regard intoxication as impairing the ability of the deceased to form suicidal intent. However, that this consideration is not a sole deciding factor is reflected by the finding that 9.7% of suicide verdict cases were judged to be intoxicated at the time of suicide.
Taylor (Reference Taylor1982) also refers to secondary suicidal clues, such as the deceased's psychological and medical history. Such ‘clues’, however, do not directly imply suicidal intent and so should not influence the coroner's decision. The similarities we have found between open and suicide verdicts in respect of these clues lends support to such a view.
Our findings are in agreement with similar studies using logistic regression analysis in that method used and suicide notes are the main discriminating factors between open and suicide verdicts. Salib's (Reference Salib1997) study of unexpected deaths in the elderly given either an open or suicide verdict, found the main determining factors influencing coroners' verdicts were: intimation of intent to die, method used and past psychiatric history. Platt et al (Reference Platt, Backett and Kreitman1988) found that the method used was the most powerful discriminator. Cooper & Milroy (Reference Cooper and Milroy1995) found certain modes of death such as drowning, jumping, poisoning, and self-immolation were more likely to receive an open verdict.
Variables such as age, gender, marital status and social class might be expected not to influence coroners' verdicts. We found that gender and social class distribution was different between the two verdicts. It is recognised, however, that different methods are used by the genders (Reference Charlton, Kelly and DunnellCharlton et al, 1992; Reference Cooper and MilroyCooper & Milroy, 1995) and, when controlled for, such a difference may disappear (Reference Holding and BarracloughHolding & Barraclough, 1978). Indeed, when using logistical regression analysis the influence of method is shown to be of prime importance and, when adjusted for, reduces the contribution of gender and social class to a non-significant level. We cannot readily explain the finding of age as a significant discriminating variable.
Implications for suicide research?
The marked similarities between the two groups lend support to the current practice of including cases of open verdicts in epidemiological suicide studies. However, the assumption that all open verdicts are suicides could substantially distort the ‘true’ suicide rate. This is particularly important at a time when the Government is setting targets for suicide reduction which include all open verdicts and an increasing number of unnatural deaths are given legally defined open verdicts.
It is important that a standardised assessment instrument be developed to help decide which open verdicts be included as suicides and which excluded, in order to produce a more reliable picture of the epidemiology of suicide. Such an instrument will permit more valuable comparisons between populations.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ The majority of open verdicts are, on the balance of probability, suicides and should therefore be included in studies of suicide.
-
▪ Not all open verdicts are suicides and the principle of probability should be applied and, if cases do not fall within these bounds, they should be excluded.
-
▪ Objective criteria should be developed to decide which open verdicts should be considered as suicides for research purposes.
LIMITATIONS
-
▪ Objective criteria for exclusion of some open verdicts were not applied; they are not as yet available.
-
▪ Information for each case was derived from coroners' records only.
-
▪ Changes in coroners' practice in Newcastle upon Tyne were not systematically evaluated.
ACKNOWLEDGEMENTS
We thank HM Coroner for Newcastle upon Tyne, Mr Leonard Coyle, for permission to examine records and the coroner's officers, Mr David Hopwood and Mr Jim MacDonald, for their most helpful cooperation; the A. & S. H. Burton Trust for financial support; and Professor D. W. K. Kay for helpful comments in the preparation of this paper.




eLetters
No eLetters have been published for this article.