


There is a considerable body of evidence indicating that both maternal depression and social adversity have a deleterious impact on the quality of the mother—infant relationship (Reference Murray and CooperMurray & Cooper, 1997). Infants from poor communities in the developing world are especially vulnerable in this regard since they are subject to parenting which is under the strain of both marked socio-economic hardship and high rates of depression (Reference HarphamHarpham, 1994). In a South African peri-urban settlement it has recently been found that one in three mothers has depression in the early post-partum period (Reference Cooper, Tomlinson and SwartzCooper et al, 1999), a rate three times higher than that which would be expected in developed countries (Reference Cooper and MurrayCooper & Murray, 1998; Reference O'Hara, Murray and CooperO'Hara, 1997). Furthermore, in this South African context, compared with women without depression, those with depression were found to be significantly less sensitively engaged with their infants, and, correspondingly, the infants of these mothers were significantly less positively engaged in interaction with their mothers. The question arises whether a mother—infant intervention could be of benefit in such indigent peri-urban populations. As a pilot to a possible controlled intervention study, a preliminary study was conducted in which a mother—infant intervention was delivered to a group of women in a South African peri-urban settlement and the outcome compared with that of a group who had not received the intervention.
METHOD
Study location
The study was carried out in Khayelitsha, a peri-urban settlement of around 350 000 people, on the outskirts of Cape Town. South Africa has seen a rapid urbanisation process since the abolition of the ‘pass’ laws in 1986 (Reference MashMash, 1998). This has resulted in a sharp increase in the number of people living in poor and overcrowded conditions in shanty towns on the periphery of established urban sites. Khayelitsha is one such settlement. It is predominantly informally organised, made up of serviced and unserviced shacks, with less than one in five of all dwellings classed as formal houses. There is considerable overcrowding. The population is highly unstable, partly because of steady migration from the rural areas, and partly because of sustained movement within Khayelitsha itself from unserviced to serviced shacks, from violent to less turbulent areas, and from flooded to drier areas. The vast majority of residents are migrants who were born in the eastern Cape (formerly known as the Ciskei and the Transkei). Two-thirds of the population are estimated to be unemployed. Of those in employment, the great majority earn less than the Household Subsistence level. Nearly a quarter of the population are functionally illiterate (Reference MashMash, 1998).
Sample recruitment
Over the course of a 6-month period in 1998, a sample of 40 pregnant women in a defined area of Khayelitsha (Makhaya) were approached and invited to receive an intervention in the context of a study of its efficacy. All agreed. Eight of the women either moved away within 2 months of the delivery or sent their infants to relatives in distant parts of the country within the same period.
Nature and delivery of the intervention
The intervention delivered was based on an adaptation of the Health Visitor Preventive Intervention Programme (further details available from the author upon request). This was adapted specifically for the Khayelitsha project by incorporating the key principles of the World Health Organization (1995) document Improving the Psychosocial Development of Children, and by extending the intervention until 6 months post-partum. The aim of the intervention was to provide the mother with emotional support and to encourage her in sensitive responsive interactions with her infant. A major aspect of the intervention was the use of particular items from the Neonatal Behavioural Assessment Schedule (NBAS; Reference Brazelton and NugentBrazelton & Nugent, 1995) to sensitise the mother to her infant's individual capacities and sensitivites. In addition, based on the findings of this assessment, specific advice was formulated concerning aspects of infant management (e.g. sleep regimen, crying, feeding).
The intervention was delivered by four community workers, who had been selected by a subset of the authors in consultation with the local community council. These women had no specialist qualifications and, indeed, had limited schooling. They received training in basic counselling skills as well as in the specific mother—infant intervention. They delivered this intervention to the women in their homes in sessions lasting approximately an hour. The intervention involved women being visited twice antenatally, twice weekly for 4 weeks postnatally, weekly for 8 weeks, fortnightly for a month, and then monthly for 2 months. Written records were kept of each intervention session and these were reviewed weekly as part of a group supervision process (under the supervision of M. L.). In addition, each community worker taperecorded all the sessions involved in their last two cases and a random selection of the sessions was transcribed and subjected to a content analysis.
Assessments
The women were assessed at 6 months post-partum following the intervention. A set of questions were drawn up to assess the mother's view of the help she had received from the community worker. (This was an adaptation of a questionnaire used in a study of health visitor intervention conducted in Reading in the UK. The questionnaire is available from the author upon request.) These questions were put to the mother in a standardised form by an independent assessor. Another independent assessor carried out three assessments. First, maternal mood was assessed, using a translated version of the major depression section from the Structured Clinical Interview for DSM-IV diagnoses (SCID; Reference First, Spitzer and GibbonFirst et al, 1996). The depression section of the SCID interview was translated into Xhosa, back-translated into English and then translated back into Xhosa. Second, basic anthropometric measures were taken of the infant. Finally, at the end of the intervention video recordings were made of the mothers and infants within the research base during two situations: free play and the mother feeding the baby. Each of these lasted 5-10 minutes. Following a viewing of a subset of these video recordings, a rating system was devised. The play interactions were coded on three variables: one concerned maternal sensitivity, one the overall quality of the interaction and one the infants' overall engagement in the interaction. The feeding interactions were also rated on three dimensions, all concerning the quality of the mothers' interactive behaviour: interactive engagement, affective expression and overall sensitivity. Each of these was rated on an eight-point scale. Two codes rated 19 of the interactions independently to assess reliability. Satisfactory reliability was achieved for three of the scales: maternal sensitivity during play (tau=0.62, P < 0.001), affective expression during feeding (tau=0.90, P < 0.001) and sensitivity during feeding (tau=0.74, P < 0.001).
The outcome at 6 months of the mothers and infants who had received the intervention was compared with a sample, selected by group-matching mothers and infants (i.e. on two of the following three variables: maternal age, parity and marital status) drawn from an epidemiological sample recruited and assessed in an adjacent area of Khayelitsha at the same time the interventions were being delivered (Reference Cooper, Tomlinson and SwartzCooper et al, 1999).
RESULTS
Evaluation of community workers
In order to establish whether the training had been successful and the intervention was being delivered as prescribed in the manual, the transcripts of the recorded sessions were coded by an independent rater to quantify the presence of the essential counselling, infant assessment, encouragement and provision of information skills required by the intervention programme. On the basis of ordinal ratings of global categories, all the community workers showed at least moderate to good performance in the implementation of the counselling skills, the infant assessment and the provision of information, with two of the four community workers being rated as excellent on all these dimensions of performance.
Demographic characteristics
The demographic characteristics of the 32 women who received the full intervention, together with the 32 comparison mothers, are contained in Table 1. The groups differed in terms of age and educational attainment. The women in the intervention group were older (χ2=8.90, d.f.=2, P=0.01) and better educated (χ2=6.74, d.f.=1, P=0.01) than the comparison group. The groups were comparable for the other demographic characteristics shown.
Table 1 Demographic characteristics
| Characteristic | Intervention group (n=32) % | Comparison group (n=32) % |
|---|---|---|
| Maternal age (years) | ||
| <28 | 19 | 37 |
| 28-33 | 28 | 41 |
| > 33 | 53 | 22 |
| Single | 29 | 44 |
| Primiparous | 10 | 25 |
| Educated to Standard 9 or above1 | 50 | 25 |
| Unserviced shack | 9 | 6 |
Virtually all the women in both groups initiated breast-feeding (i.e. 94% (30/32) of the intervention group and 97% (29/30)Footnote 1 of the comparison group), of whom around two-thirds were still breast-feeding by 6 months (i.e. 66% (21/32) and 70% (21/30), respectively).
Mothers' perception of the intervention
A questionnaire was used to assess whether the mothers found the intervention to be of help and the degree to which the mothers perceived the intervention to have enhanced their sensitivity to their infants' needs and capacities. Given a four-point choice of ‘strongly agree’, ‘moderately agree’, ‘slightly agree’ and ‘disagree’, 90% (29/32) of the mothers strongly or moderately agreed with the statement that the community worker had ‘really understood how I felt’, and 94% (30/32) strongly or moderately agreed with the statement that the community worker ‘made me feel supported’, with the statement that ‘I felt she was on my side’ and with the statement that ‘I felt that I could trust her and talk openly about myself to her’. Statements about the help given with caring for the infant were similarly positively endorsed. For example, 90% (29/32) of the mothers strongly or moderately agreed with the statement that the community worker ‘helped me to solve problems I was having with my baby’. Several statements concerned with enhanced maternal sensitivity to the infant were also positively endorsed. Thus, all the mothers strongly or moderately agreed with the statement that the community workers had ‘made me appreciate the things that my child can do’, and 90% (29/32) agreed with the statement that ‘she helped me understand my child's needs’ and the statement that ‘she showed me how to respond to what my child was doing’. Endorsement of negative statements was extremely rare.
Maternal mood
The rate of DSM-IV major depression (American Psychiatric Association, 1994) at 6 months post-partum was 19% (6/32) in the index group compared with 28% (9/32) in the comparison group. After controlling for age and level of education, using a Mantel—Haenszel test (Reference Armitage and BerryArmitage & Berry, 1996), this difference was found not to be significant (χ2 MH=2.00, d.f.=1, P=0.16).
Mother—infant engagement
The three reliable interaction variables were transformed into binary variables (i.e. none or little v. at least to a moderate degree). As can be seen from Fig. 1, there was evidence for a benefit of the intervention. Thus, after controlling for age and education, relative to the comparison group, in the play and feeding situations the index mothers showed greater sensitivity (χ2 MH=5.19, d.f.=1, P=0.02, and χ 2 MH=5.95, d.f.=1, P=0.1, respectively), and in the feeding situation there was an indication that they expressed more positive affect (χ2 MH=3.11, d.f.=1,P=0.08).
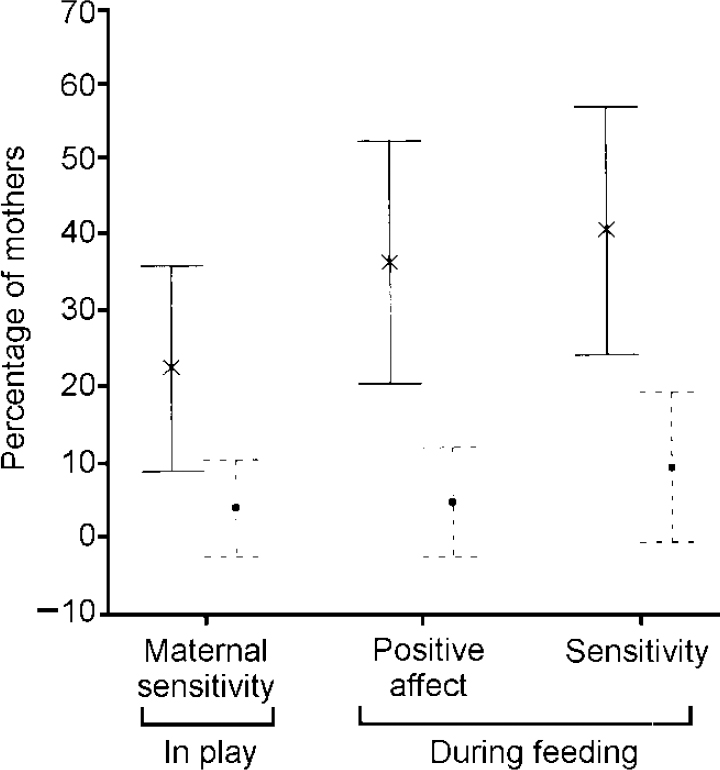
Fig. 1 Percentage of mothers (with 95% confidence intervals) showing interactions of at least moderate quality during play and feeding; solid lines, intervention group; dashed lines, comparison group.
Infant growth
Differences were observed between the two groups at 6 months in terms of infant physical development (Fig. 2). These differences were tested using the Mann—WhitneyU test. The infants in the intervention group were significantly heavier (P=0.01) and their weights were less variable than those of the comparison group infants, i.e. median=85th centile (IQR=34) and 66th centile (IQR=46) respectively. Height also differed significantly between the two groups (P=0.02), with infants in the intervention group being taller than those in the comparison group: median=75th centile (interquartile range, IQR=42) and 58th centile (IQR=61) respectively. No significant difference was found between the two groups for weight—length ratio (the median BMI was 18.2 (IQR=4) for the intervention group and 17.7 (IQR=2.5) for the control group) or for head circumference (Fig. 2).
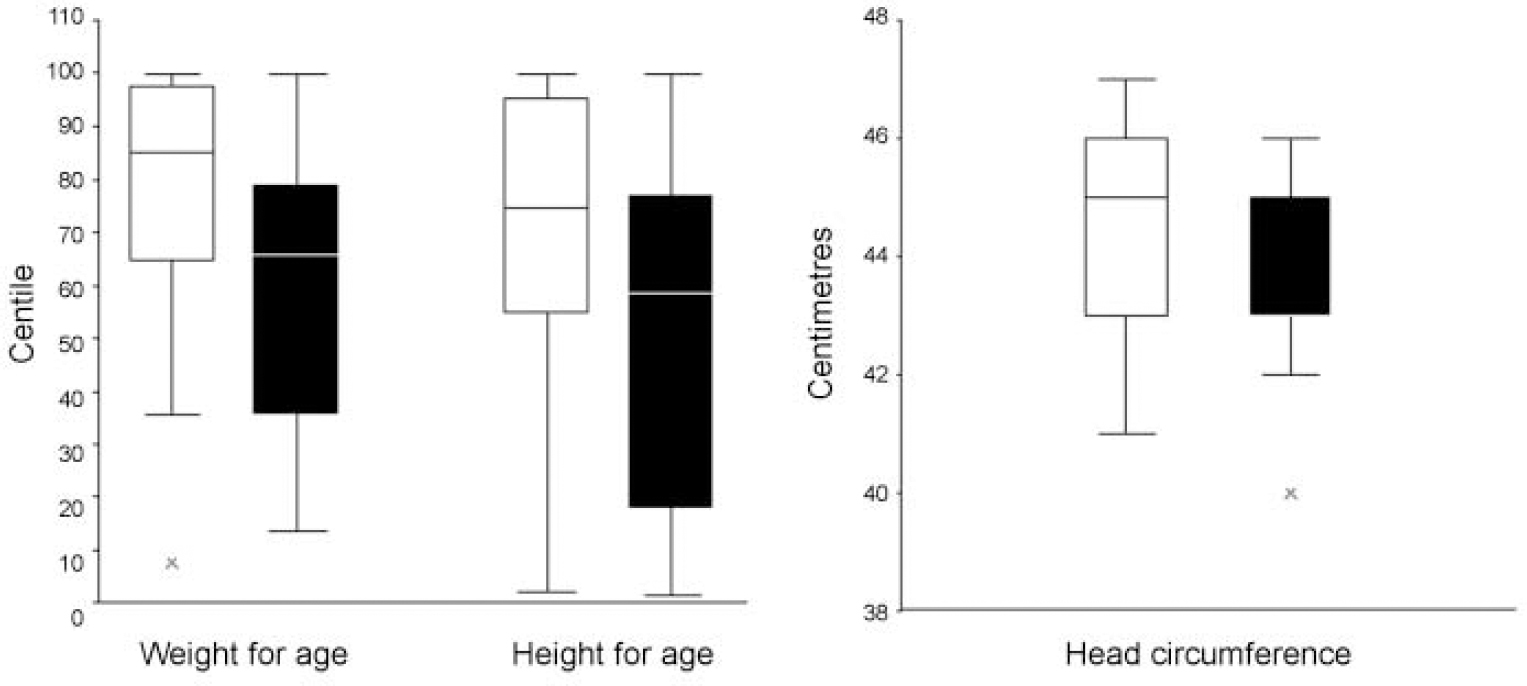
Fig. 2 Boxplots of anthropometric measures for infants in the intervention group (□) and comparison group (▪).
In order to determine whether any association between group membership and growth remained after controlling for the possible effects of breast-feeding persistence and maternal age, Cochran—Mantel—Haenszel tests were performed. Weight and height were both reduced to three class ordinal variables — below the 25th centile, 25-75th centile and above the 75th centile. For infant weight, taking account of both breast-feeding persistence and age, an indication of an intervention effect remained (χ2 MH=5.3, d.f.=2, P=0.07). For all age groups (i.e. <28, 28-33, >33 years), among those whose mothers were still breast-feeding at 6 months, a higher proportion of infants in the intervention group than the comparison group were found to have a weight above the 75th centile. For infants who were no longer being breast-fed, higher proportions above the 75th centile for weight were also seen in the intervention group than in the comparison group for the higher and the lower age groups. Of the six infants below the 25th centile, five were from the comparison group and only one from the index group. When infant height was considered, the effect of the intervention remained significant when account was taken of both breast-feeding persistence and age (χ2 MH=6.5, d.f.=2, P=0.04); both for those still breast-feeding at 6 months and those who had ceased breast-feeding, for the higher and lower age groups, higher proportions of infants in the intervention group than the comparison group were found to have a weight above the 75th centile. Of the nine infants below the 25th centile on height, seven were from the comparison group and only two from the index group.
DISCUSSION
Post-partum depression and child development
There is a considerable body of evidence indicating that the quality of the early mother-infant relationship is strongly related to the course of child cognitive and socio-emotional development. Indeed, the moderate and self-limiting depressions occurring after 10-15% of births in developed countries have been found to be associated with enduring adverse effects on child cognitive development (Reference Sharp, Hay and PawlbySharp et al, 1995) and behavioural adjustment (Reference Sinclair and MurraySinclair & Murray, 1998; Reference Murray, Sinclair and CooperMurray et al, 1999), especially in boys. Where examination has been made, it has been found that the disturbance in the quality of the early mother—infant relationship associated with the maternal affective disorder carried much of the predictive force in the adverse child outcomes. Notably, the experience of social adversity has been found to have an impact on the quality of early mother—infant engagement independent of maternal mood (Reference Murray, Fiori-Cowley and HooperMurray et al, 1996).
Post-partum depression in a South African peri-urban settlement
A high rate of post-partum depression has been reported in a South African peri-urban settlement (Reference Cooper, Tomlinson and SwartzCooper et al, 1999). It was also found that, as in Western samples (Reference Murray and CooperMurray & Cooper, 1997), there was a strong association between maternal depression and disturbances in the mother—infant relationship. This is a serious cause for concern. Not only is children's developmental progress likely to be compromised by the extreme levels of social and economic adversity which obtain in this South African context (and in similar situations around the developing world), but it is likely to be further jeopardised by the impact of such forces on the quality of care infants receive from their mothers. It is, therefore, of paramount importance that interventions are developed and evaluated to support mothers and families living in indigent peri-urban contexts in caring for young infants.
A study by Wendland-Carro et al (Reference Wendland-Carro, Piccinini and Millar1999) of a small, disadvantaged Brazilian sample found positive benefits from a brief intervention intended to enhance the quality of the early mother—infant relationship. The intervention was designed to motivate mothers to be involved with their infants and to promote affectionate handling of the infant. It consisted of just one session during which a video was shown of infant capacities (based on an administration of the NBAS; Reference Nugent and BrazeltonNugent & Brazelton, 1989), followed by a discussion with the mother emphasising the infant's potential to interact and the importance of affectionate and sensitive handling. This session was supplemented by written material. When mother—infant interactions were assessed 1 month later, in comparison with a group of mothers who did not receive this intervention, the index mother—infant dyads were found to have significantly more ‘synchronised interactions’, involving mutual gaze, vocalisations and smiles, and index mothers were more responsive to infant cries.
The findings of Wendland-Carro et al (Reference Wendland-Carro, Piccinini and Millar1999) are surprising and encouraging. Early family intervention programmes in the past have usually been intensive, long-term treatments (e.g. Reference Olds and KitzmanOlds & Kitzman, 1993; Reference Heinicke, Fineman and RuthHeinicke et al, 1999), lasting for at least 2 years. If brief programmes directed at the quality of mother—infant engagement can effect significant change in the mother—child relationship, then it is important to develop and evaluate such treatments, especially in high-risk populations.
The nature of the intervention
The pilot study described here was an evaluation of just such an intervention. A treatment developed for delivery by trained health visitors in Britain (further details available from the author upon request) was adapted for delivery by trained, but otherwise unqualified, community workers in the South African context. The training of the community workers in delivery of the treatment was preceded by several focus group meetings concerned with child-care beliefs and practices, and the community workers themselves were given considerable latitude to shape the intervention. Cultural norms surrounding the concept of infancy and child-care practices were taken into account in delivering the intervention. Although there were consequently differences in the implementation of the intervention in the African context as opposed to the original British setting, the central tenets of the intervention, which concern maximising the potential for sensitive mother—infant engagement, appear to be equally acceptable and appropriate for the two cultures.
Use of unqualified community workers
Questions have been raised about the appropriateness of using unqualified workers in home-based family interventions. Indeed Olds & Kitzman (Reference Olds and Kitzman1993) reported that of six intervention programmes that were effective in enhancing child cognitive development, five employed professional or highly trained staff. If the disappointing findings reported from developed-world studies using unqualified workers were to be replicated in the developing world, this would have grave implications. The skilled human resources are simply not available in such circumstances to provide a home-based service to more than a tiny proportion, if any, of the population (Reference Freeman, Pillay, Foster, Freeman and PillayFreeman & Pillay, 1997). Yet, as our South African epidemiological study revealed, in the context of the adversity which is endemic in these peri-urban circumstances, disturbances in the early mother—infant relationship are common. If a service is to be provided to meet the need, then it must necessarily be a service that can be provided by the community itself.
Mothers' perceptions of the intervention
An encouraging finding of the study was that the intervention was extremely well received by the mothers. Not only was it the common experience of the mothers to feel well supported by the community workers, but they also felt helped in the understanding and management of their baby. In no case was the intervention regarded by the mother or the wider family as an unwanted intrusion. This stands in contrast to home-based interventions in developed countries, where high-risk populations not uncommonly perceive the ministrations of a clinical or social agency as an intrusion (Reference Egeland and EricksonEgeland & Erickson, 1990).
Impact of the intervention on the mother—infant relationship
This study did not involve random assignment of participants to an intervention and a properly constituted control condition. Indeed, it is simply a comparison between two groups, one of which received an intervention. Therefore, the findings can only be regarded as preliminary and must be interpreted with caution. It is nevertheless encouraging that, based on the small sample of women and infants who received the index intervention, an advantage over the group who had not received it did emerge. In particular, the mothers of those who had received the intervention were rated as being more sensitive and more affectionate to their infants.
Two further findings require comment. First, although there was no reliable antidepressant effect of the index intervention, there was a suggestion that, assuming no pre-treatment difference obtained between the two groups studied, should the current findings be replicated in a larger controlled trial, an antidepressant effect might emerge. (If the 6-month post-partum rates in the current study are robust, with 80% power and α set at 0.05, two groups of 180 would produce a significant difference in the rate of depression.) However, the absence of a clear impact of treatment on maternal mood is, perhaps, unsurprising. The social factors found to be associated with maternal mood disorder in these highly adverse circumstances (Reference Cooper, Tomlinson and SwartzCooper et al, 1999) relate to the inordinate difficulties of having a child in these circumstances and the absence of family support. It is, perhaps, over-optimistic to expect that a home visit once a week, however sympathetic and supportive, would be sufficient to counter such powerful social forces. The second finding requiring comment concerns the anthropometric data. Although it was the case that there was some evidence of a significant advantage for the intervention in terms of infant weight and height, this needs to be interpreted with caution. While the intervention appeared to protect against very low infant weight, it was also associated with rather high weights. It is possible that the additional attention the mothers who received the intervention were giving their infants could, despite advice to the contrary, have led to excessive feeding. Longer-term follow-up of a properly controlled sample would reveal whether there is a genuine benefit of the intervention to infant physical development.
The findings of the study are promising. They suggest that it might well be possible to improve the quality of the early mother—infant relationship in indigent peri-urban contexts using unqualified community workers to deliver an intervention. They also indicate that, despite the difficulties inherent in working in the peri-urban environment, it is possible to conduct rigorous research. In view of these considerations, a controlled clinical trial of this intervention is now being carried out in Khayelitsha.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
• The therapeutic input of unqualified community workers trained to deliver the intervention was enormously appreciated by the women who received it.
-
• The intervention appeared to be of benefit to the quality of the mother—infant relationship.
-
• The intervention appeared to have a positive impact on infant growth.
LIMITATIONS
-
• Since the study did not involve random assignment, the findings must be regarded as providing no more than tentative support for a benefit of the intervention.
-
• All assessments were made in the research unit and the extent to which the findings generalised to the home situation is uncertain.
-
• The impact of the intervention on infant socio-emotional and cognitive development was not determined.
Acknowledgements
The initiation of a research collaboration between the Reading and Cape Town groups was made possible by a British Council Link Award. The training of the community workers and the implementation of the intervention were supported by a grant from the World Health Organization. The control data were derived from an epidemiological study supported by a grant from the Wellcome Trust. We are grateful to Marjorie Feni, Laphina Makhanye, Nokwanda Tshikana and Nokhanyo Siko for carrying out the interventions, and to Nosisana Nama, Nomalanga Mosala, Nokwanda Mtotot and Pedis Mosala for help with the data collection. We are grateful to Dr Matt Woolgar and Helena Romaniuk for help with the data analysis.




eLetters
No eLetters have been published for this article.