


Indicators of poor fetal growth, such as low birth weight (⩽2500 g), are linked with increased offspring risk for neurodevelopmental disorders, Reference Hack, Youngstrom, Cartar, Schluchter, Taylor and Flannery1-Reference Ficks, Lahey and Waldman4 academic problems Reference Hack, Flannery, Schluchter, Cartar, Borawski and Klein5-Reference Matte, Bresnahan, Begg and Susser8 and poor social outcomes. Reference Hack, Flannery, Schluchter, Cartar, Borawski and Klein5 The developmental origins of health and disease hypothesis, which states that developmental plasticity contributes to fetal physiological adaptations made in response to the intrauterine environment, has been used to explain the identified associations. Reference Barker9 The mechanisms linking fetal growth with later psychiatric, academic and social problems are not straightforward, however. Impaired fetal growth may act as an independent, environmental risk factor, as twin studies have shown for attention-deficit hyperactivity disorder (ADHD). Reference Groen-Blokhuis, Middeldorp, van Beijsterveldt and Boomsma10-Reference Lehn, Derks, Hudziak, van Beijsterveldt and Boomsma12 Previously identified associations may also be a result of unmeasured selection factors, such as environmental confounding or shared genetic liability, that influence both the likelihood of experiencing the risk and the outcome. Reference Thapar and Rutter13,Reference Smith14 For example, low birth weight is associated with environmental risks that are themselves predictive of subsequent adverse outcomes Reference Weightman, Morgan, Shepherd, Kitcher, Roberts and Dunstan15 and family and twin studies indicate that genetic and shared environmental factors influence birth weight. Reference Lunde, Melve, Gjessing, Skjaerven and Irgens16 As such, the field should remain cautious in drawing causal conclusions between fetal growth and these outcomes. Conflicting results across outcomes also have been found, Reference Hack, Youngstrom, Cartar, Schluchter, Taylor and Flannery1,Reference Hack, Flannery, Schluchter, Cartar, Borawski and Klein5,Reference Saigal, Stoskopf, Streiner, Boyle, Pinelli and Paneth17-Reference Lawlor, Clark, Smith and Leon20 and a recent meta-analysis showed that associations between low birth weight and depression may be as the result of publication bias. Reference Wojcik, Lee, Colman, Hardy and Hotopf19 Further, previous studies have been limited by self- and parent-report of both risk and outcome. Reference Hack, Youngstrom, Cartar, Schluchter, Taylor and Flannery1,Reference Foley, Neale and Kendler21 Thus, analyses that determine precise and accurate estimates of the strength of the associations, as well as those that begin to pull apart genetic and environmental influences, are needed in the field. Reference Wojcik, Lee, Colman, Hardy and Hotopf19,Reference Kramer22
We sought to rigorously examine the associations between fetal growth and psychiatric and socioeconomic problems in a Swedish population cohort. Our outcomes included autism spectrum disorder (ASD), ADHD, psychotic or bipolar disorder, substance use problems, suicide attempts, criminality, failing grades in grade 9 (13-16 years old), low educational attainment and social welfare receipt. We estimated the magnitude of the associations from traditional, population-based epidemiological designs and examined the effect sizes using sibling-comparison models. Quasi-experimental approaches, such as sibling-comparison approaches, utilise design features to test alternative explanations. Reference Rutter23 By accounting for genetic and environmental factors that make siblings similar, sibling comparisons offer a way to pull apart genetic and environmental confounding. Reference Rutter23,Reference Lahey and D'Onofrio24 Sensitivity analyses were used to test alternative explanations and address limitations inherent in the sibling-comparison approach. Reference D'Onofrio, Lahey, Turkheimer and Lichtenstein25
Method
Sample
After approval from the Institutional Review Boards at Karolinska Institutet and Indiana University, we created a prospective national cohort by linking information in the following Swedish registries: (a) the Medical Birth Register includes data on more than 99% of all pregnancies in Sweden; (b) the Multi-Generation Register contains information about the biological relationships for all individuals living in Sweden; (c) the Migration Register contains information on dates of migration in or out of Sweden; (d) the Cause of Death Register supplies dates and causes of all deaths; (e) the Patient Register contains diagnoses for all in-patient hospital admissions since 1973 and out-patient care since 2001; (f) the National Crime Register includes information about all criminal convictions; (g) the National School Register includes all subject grades at the end of grade 9 since 1983; (h) the Education Register contains information on the highest level of completed formal education; and (i) the longitudinal integration database for health insurance and social studies (LISA) contains yearly assessments of childbearing, marital and social welfare status for all individuals at least 15 years old since 1990. Detailed information about these registers is available in the online data supplement and elsewhere. Reference D'Onofrio, Class, Rickert, Larsson, Langstrom and Lichtenstein26
The data-set began with 3 619 712 offspring born from 1973 to 2008. We removed multiple births (86 273, 2.4%) because birth outcomes are different in multiples as compared with singleton births. Reference Loos, Derom and Vlietinck27 We also removed offspring with missing birth weight information (9888, 0.3%) as well as recorded gestational age values of less than 23 weeks or greater than 42 weeks and 6 days (49 374, 1.4%). Offspring with no information regarding gender (3, <0.1%), invalid parity information (20, <0.1%) and those who had emigrated within the 25 year period (182 223, 5.0%) were removed. We also excluded offspring missing maternal identification numbers (158, <0.1%). The final sample consisted of 3 291 773 offspring born to 1 735 250 distinct biological mothers, representing 90.9% of all recorded Swedish births within the year range investigated.
Both ASD and ADHD were identified using in-patient and out-patient assessment information Reference Indring, Rai, Dal, Dalman, Sturm and Zander28 from individuals born between 1980 and 2001 (n = 2 032 803). In addition, we used a 2-year age criterion for ASD and ADHD diagnosis. For criminality, we used an age criterion of 15 years because of the Swedish legal age of responsibility. Therefore, the criminality subsample spanned the years 1973-1994 and included 2 044 992 individuals. For all other outcomes, we used a 12 year age criterion. Therefore, this subsample included 2 308 032 offspring born between 1973 and 1997.
Measures
Birth weight
To assess fetal growth, we utilised two different representations of birth weight while controlling for gestational age at birth. For the ordinal representation, birth weight was grouped into the following ranges: ⩽2500 g, 2501-3000 g, 3001-3500 g, 3501-4000 g (referent) and ⩾4001 g. Continuously measured birth weight was converted to a linear scale centred at 3750 g (reference 0 point), the approximate mean of the sample.
Offspring outcomes
We predicted six indices of psychiatric problems previously shown to be reliable measures. Reference Indring, Rai, Dal, Dalman, Sturm and Zander28-Reference D'Onofrio, Singh, Iliadou, Lambe, Hultman and Grann32 In particular (a) ASD and (b) ADHD were indexed using validated Reference Indring, Rai, Dal, Dalman, Sturm and Zander28,Reference Larsson, Chang, D'Onofrio and Lichtenstein33 in-patient and out-patient diagnoses according to ICD-9 34 and ICD-10 35 for offspring born between 1980 and 2001 and being at least 2 years old at the time of diagnosis. As the ICD follows a strict definition of ADHD and ASD, results apply to the most severe cases of these disorders. In addition, it was not possible to classify ADHD according to subtype (i.e. combined, primarily hyperactive-impulsive and primarily inattentive type), since these were not recorded across the registers using the ICD. Offspring had to have been at least 12 years old to receive any of the following disorders: (c) psychotic or bipolar disorder was defined as first in-patient admission for schizophrenia, bipolar disorder or another non-organic psychotic disorder according to ICD-8, 36 -9 and -10 criteria; Reference Lichtenstein, Yip, Bjork, Pawitan, Cannon and Sullivan29 (d) substance use problems was defined as first in-patient admission for a primary or secondary diagnosis of alcohol or any other non-nicotine substance use disorder; Reference D'Onofrio, Rickert, Langstrom, Donahue, Coyne and Larsson30 (e) age at suicide attempt was gathered using in-patient admission for a primary or secondary diagnosis; Reference Tidemalm, Langstrom, Lichtenstein and Runeson31 and (f) criminality was indicated by the first occurrence of any criminal conviction from age 15 years, the age of legal responsibility in Sweden. Reference D'Onofrio, Singh, Iliadou, Lambe, Hultman and Grann32 We chose not to examine broadly defined affective disorder because in-patient admissions for that diagnosis may indicate the presence of co-occurring suicidality or psychosis, and we had access to validated indicators of these associated possible outcomes. Reference Lichtenstein, Yip, Bjork, Pawitan, Cannon and Sullivan29,Reference Tidemalm, Langstrom, Lichtenstein and Runeson31 Respective ICD codes are presented in online Table DS1, and it should be noted that clinical evaluations, not structured interviews, were used by diagnosing medical providers to determine primary diagnoses.
We predicted three indices of socioeconomic outcomes: (a) failing grades indexed poor school performance in grade 9 commensurate with a mean failing grade across 16 academic subjects; Reference D'Onofrio, Singh, Iliadou, Lambe, Hultman and Neiderhiser37 (b) education under 10 years was an indication of low educational attainment 38 and (c) social welfare receipt, which was defined as the age of first receipt of government social welfare subsidies. For verification and converging support of these outcomes, we also predicted low income and higher education (further explained in online Fig. DS2).
Covariates
The Medical Birth Register provided offspring gender, birth order, year of birth and gestational age at birth. Measured maternal and paternal covariates included age at the offspring’s birth, highest level of completed education by 2008 (to capture some socioeconomic variability across families) and lifetime history of any criminal conviction. All covariates were associated with both birth weight and the outcomes.
Analyses
We used Cox survival analysis for right-censored outcomes because not all offspring have lived through the study period. If offspring did not receive a diagnosis within the study period, they contributed person-time at risk until death, emigration or the end date of follow-up (31 December 2009), whichever came first. We used logistic regression analyses when predicting failing grades and education under 10 years because they were dichotomous outcomes. Thus, results are presented as hazard ratios (HRs) or odds ratios (ORs).
We fit a series of models for each outcome. All models controlled for offspring gender, birth order and measures of linear and quadratic gestational age. Logistic models also controlled for offspring year of birth. Because we always adjusted gestational age at birth, our predictor may be considered an index of fetal growth. The first statistical model used the ordinal representation of birth weight to estimate clinically interpretable estimates of risk across outcomes. Second, we used a continuous representation of birth weight in two baseline models. One baseline model included both a linear and quadratic representation of birth weight, whereas the other baseline model only included the linear representation of birth weight. Akaike information criterion, a measure of relative merit that penalises for model complexity, was used to select the best fitting model, either linear or quadratic. Third, we included offspring-specific (gender, birth order, linear and quadratic gestational age and maternal and paternal age at childbearing) and parental-specific covariates (maternal and paternal highest level of education and history of criminal conviction) in an adjusted model of either continuous linear or quadratic representation of birth weight. Fourth, we fitted a fixed-effects model that clustered at the maternal level, which accounted for factors that siblings share, including all genetic and environmental factors that make siblings similar. Reference Lahey and D'Onofrio24 Covariates that may vary between siblings (i.e. offspring gender, birth order, gestational age and offspring year of birth (in logistic models)) were included in fixed-effects models. Siblings were identified as individuals sharing a biological mother (for example full or maternal half-siblings).
Sensitivity analyses
We ran several sensitivity analyses to test for biases because of preterm births, to examine whether there was converging evidence across related socioeconomic outcomes and to check assumptions inherent in the sibling-comparison design.
Results
Table 1 presents cohort demographics by birth weight category. Table 2 presents the number of offspring across outcomes by birth weight category.
Table 1 Demographic characteristics of 3 291 773 offspring born 1973-2008 in Sweden by birth weight
| Birth weight category, g | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Covariates | ⩽2500 (n = 114 580) |
2501-3000 (n = 366 500) |
3001-3500 (n = 1 075 447) |
3501-4000 (n = 1 152 337) |
⩾4000 (n = 583 909) |
|||||
| Offspring, birth year: 1973-2008 (n = 3 291 773) | ||||||||||
| Female, n (%)Footnote a | 58 657 | 51.19 | 207 481 | 56.61 | 573 332 | 53.31 | 533 202 | 46.27 | 220 119 | 37.70 |
| Gestational age, days: mean (s.d.) | 245.46 | 25.53 | 271.19 | 12.10 | 278.14 | 9.41 | 282.14 | 8.27 | 285.24 | 7.77 |
| Maternal, birth year: 1924-1995 (n = 1 732 107) | ||||||||||
| Age at birth, years: mean (s.d.) | 28.85 | 5.67 | 28.43 | 5.36 | 28.59 | 5.19 | 28.96 | 5.10 | 29.55 | 5.06 |
| Nationality, Swedish: n (%) | 54 045 | 83.77 | 169 706 | 83.00 | 491 255 | 84.77 | 518 302 | 87.12 | 254 761 | 88.68 |
| Upper secondary education,Footnote b n (%) | 31 870 | 49.35 | 105 639 | 51.62 | 323 120 | 55.71 | 347 214 | 58.32 | 170 492 | 59.31 |
| Adult severe psychopathology, n (%) | 1 748 | 2.71 | 4 493 | 2.20 | 10 606 | 1.83 | 9 629 | 1.62 | 4 377 | 1.52 |
| Criminality, n (%) | 8 939 | 13.84 | 26 443 | 12.92 | 65 981 | 11.38 | 61 356 | 10.31 | 28 207 | 9.81 |
| Paternal, birth year: 1904-1993 (n = 1 725 359) | ||||||||||
| Age at birth, years: mean (s.d.) | 31.75 | 6.55 | 31.38 | 6.28 | 31.49 | 6.07 | 31.78 | 5.96 | 32.28 | 5.91 |
| Nationality, Swedish: n (%) | 52 049 | 83.61 | 165 781 | 82.69 | 485 000 | 84.50 | 518 434 | 87.04 | 259 048 | 89.02 |
| Upper secondary education,Footnote b n (%) | 27 192 | 43.63 | 90 199 | 44.92 | 274 812 | 47.82 | 294 778 | 49.44 | 145 192 | 49.84 |
| Adult severe psychopathology, n (%) | 1 345 | 2.16 | 4 033 | 2.01 | 10 059 | 1.75 | 9 399 | 1.58 | 4 172 | 1.43 |
| Criminality, n (%) | 25 953 | 41.64 | 81 223 | 40.45 | 219 628 | 38.22 | 216 353 | 36.28 | 101 834 | 34.96 |
a. Percentage of individuals by birth weight group, for offspring, the total number by birth weight group is listed in the column header, for mother and father variables, the total number of distinct mothers and fathers are listed in the left column and percentages are based on the number of non-missing cases for each variable.
b. Upper secondary education: minimum 3 years.
Table 2 Psychiatric and socioeconomic outcomes by birth weight

| Birth weight category (g) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ⩽2500 (n = 114 580) |
2501-3000 (n = 366 500) |
3001-3500 (n = 1 075 447) |
3501-4000 (n = 1 152 337) |
⩾4000 (n = 583 909) |
||||||||
| Outcomes | Birth year | Total n | n | KME | n | KME | n | KME | n | KME | n | KME |
| Psychiatric Morbidity | ||||||||||||
| ADHDFootnote a | 1980-2001 | 2 032 803 | 521 | 0.75 | 925 | 0.43 | 2 125 | 0.33 | 2 279 | 0.33 | 1 437 | 0.41 |
| ASDFootnote a | 1980-2001 | 2 032 803 | 303 | 0.43 | 594 | 0.27 | 1 346 | 0.21 | 1 497 | 0.21 | 953 | 0.27 |
| Psychotic or bipolarFootnote b | 1973-1997 | 2 308 032 | 631 | 1.34 | 1 724 | 1.05 | 4 293 | 0.94 | 4 153 | 0.89 | 1 881 | 0.87 |
| Suicide attemptFootnote b | 1973-1997 | 2 308 032 | 1 094 | 2.19 | 3 728 | 2.11 | 9 138 | 1.84 | 8 272 | 1.62 | 3 567 | 1.51 |
| Substance use problemFootnote b | 1973-1997 | 2 308 032 | 1 584 | 2.70 | 5 130 | 2.68 | 13 347 | 2.48 | 13 691 | 2.28 | 5 698 | 2.20 |
| CriminalityFootnote b | 1973-1994 | 2 044 992 | 8 810 | 15.64 | 31 178 | 15.77 | 87 032 | 15.59 | 91 071 | 15.88 | 44 133 | 16.48 |
| Socioeconomic outcomes | ||||||||||||
| Failing gradesFootnote b | 1973-1992 | 1 776 454 | 11 635 | 17.13 | 35 962 | 16.52 | 89 712 | 14.63 | 72 391 | 11.42 | 22 626 | 7.57 |
| Education under 10 yearsFootnote b | 1973-1991 | 1 689 102 | 18 502 | 32.79 | 60 246 | 30.09 | 163 611 | 28.80 | 165 487 | 28.23 | 79 515 | 28.98 |
| Social welfare receiptFootnote b | 1973-1990 | 1 609 646 | 15 535 | 32.55 | 51 803 | 30.58 | 128 141 | 27.12 | 119 124 | 24.74 | 54 714 | 23.69 |
ADHD, attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; KME, Kaplan-Meier product-limit survival estimate.
a. KME at 25 years of age.
b. ME at 35 years of age.
Psychiatric problems
Figure 1 presents results from the baseline ordinal model (dark bars) with 95% confidence intervals. The corresponding results using the continuous measure of birth weight (the solid line in Fig. 1) also illustrate how fetal growth was associated with later psychiatric problems. For ease of interpretation, ordinal results are discussed here and continuous results are presented graphically.
Figure 1(a)-(c) present the strong inverse association between birth weight and ASD (HRBirth weight (BW):⩽2500 g = 1.79, 95% CI 1.64-1.96), ADHD (HRBW:⩽2500 g = 1.54, 95% CI 1.44-1.65), and psychotic or bipolar disorder (HRBW:⩽2500 g = 1.19, 95% CI 1.09-1.29) respectively. The associations remained robust when adjusting for offspring- and parental-specific covariates (not shown; see online Table DS2). Also in Fig. 1, the findings from fixed-effects modelling, which compared differentially exposed siblings (light bars with 95% confidence intervals and the dotted line), showed consistently elevated effect sizes for these outcomes. Fetal growth was associated with ASD (HRBW:⩽2500 g = 2.44, 95% CI 1.99-2.97), ADHD (HRBW:⩽2500 g = 1.65, 95% CI 1.40-1.93) and psychotic or bipolar disorder (HRBW:⩽2500 g = 1.24, 95% CI 1.02-1.51) independent of the measured covariates and the comparison of differentially exposed siblings, consistent with a causal inference.
A different pattern of results was found when predicting suicide attempt and substance use problems (Fig. 1(d) and (e)), however. As can be noted in the dark bars in Fig. 1, population models suggested that lower birth weight increased the risk for suicide attempt (HRBW:⩽2500 g = 1.19, 95% CI 1.11-1.28) and substance use problems (HRBW:⩽2500 g = 1.27, 95% CI 1.20-1.34). After adjusting for measured covariates (not shown; see online Table DS2) and in fixed-effects models (Fig. 1, light bars), the associations with suicide attempt (HRBW:⩽2500 g = 0.94, 95% CI 0.81-1.10) and substance use problems (HRBW:⩽2500 g = 0.93, 95% CI 0.83-1.04) were fully attenuated.
The pattern of association was distinct when predicting criminality (Fig. 1(f)). More specifically, while population models showed that lower birth weight increased the risk for criminality (HRBW:⩽2500 g = 1.15, 95% CI 1.12-1.18), the direction of association switched in fixed-effects models. In the fixed-effects models, lower birth weight was slightly protective against criminality (HRBW:⩽2500 g = 0.87, 95% CI 0.83-0.92).

Fig. 1 Associations derived from continuous (line) and ordinal (bar with 95% confidence interval) representation of birth weight when predicting psychiatric outcomes.
(a) Attention-deficit hyperactivity disorder (ADHD), (b) autism spectrum disorder (ASD), (c) psychotic or bipolar disorder, (d) suicide attempt, (e) substance use problems, and (f) criminality. Baseline, population-wide estimates are shown with the solid line and dark bars. Sibling-comparison, fixed-effects models are shown with dotted lines and light bars. Reference group are those born in the 3501-4000 g birth weight category. The maintenance of association magnitude across population and sibling-comparison models, consistent with a causal inference, can be noted when predicting ADHD, ASD and psychotic or bipolar disorder only. A protective effect can be noted when predicting criminality in the decrease of association in the sibling-comparison model.
As can be seen in Fig. 1, all psychiatric outcomes except suicide attempt and substance use problems were better explained by a quadratic representation of birth weight (see online Table DS3 for Akaike information criterion for linear and quadratic models). Adjusted models are not presented here or in Fig. 1 for ease of interpretation. Parameter estimates across all ordinal bins are presented in online Table DS4.
Socioeconomic outcomes
Figure 2 (a)-(c) present findings across ordinal and continuous birth weight representation for failing grades, education under 10 years and social welfare receipt, respectively. Population estimates suggested that lower birth weight was associated with increased risk for failing grades (HRBW:⩽2500 g = 1.66, 95% CI 1.62-1.71) and education under 10 years (HRBW:⩽2500 g = 1.46, 95% CI 1.42-1.49). These are presented in Fig. 2 with dark bars (ordinal) and a solid line (continuous). Fixed-effects models showed attenuated, although consistent, results for failing grades (HRBW:⩽2500 g = 1.07, 95% CI 1.01-1.13) and education under 10 years (HRBW:⩽2500 g = 1.18, 95% CI 1.12-1.24), as seen in the light bars (ordinal) and dotted line (continuous) in the figure. Thus, the results lend support to fetal growth being in the causal path towards failing grades and education under 10 years. A different pattern emerged for social welfare receipt, however (Fig. 2(c)). Although the population estimate for social welfare receipt showed that lower birth weights are associated with increased social welfare receipt (HRBW:⩽2500 g = 1.52, 95% CI 1.49-1.55), the relation was completely attenuated in the fixed-effects model (HRBW:⩽2500 g = 1.00, 95% CI 0.95-1.05).
Sensitivity analyses
First, to test whether results were biased by premature births, we limited the sample to full-term births only. Online Fig. DS1 shows that associations are comparable with those found in the main analyses, thus premature births were not driving the associations found. Second, we predicted two additional outcomes related to our main socioeconomic outcomes, low income and higher education. From these analyses we obtained converging evidence about the robust association between fetal growth and decreased odds of educational attainment, as well as the fully attenuated relationship between fetal growth and economic stability (online Fig. DS2). Third, we performed analyses to address some of the assumptions of the sibling-comparison design. To address concerns about the generalisability of findings from offspring with siblings to those without, we compared the population estimates in families with multiple children to those with only one child. Online Fig. DS3 shows that baseline population estimates were not different between offspring with one or more siblings as compared with only children. To address concerns about the generalisability of the findings from differentially exposed sibling to other populations, we conducted cousin-comparisons. Online Fig. DS4 presents the cousin-comparison results showing a commensurate pattern of results to the main analyses. These results suggest that assumptions in sibling-comparison analyses (for example no carry-over effects) may not account for our conclusions.
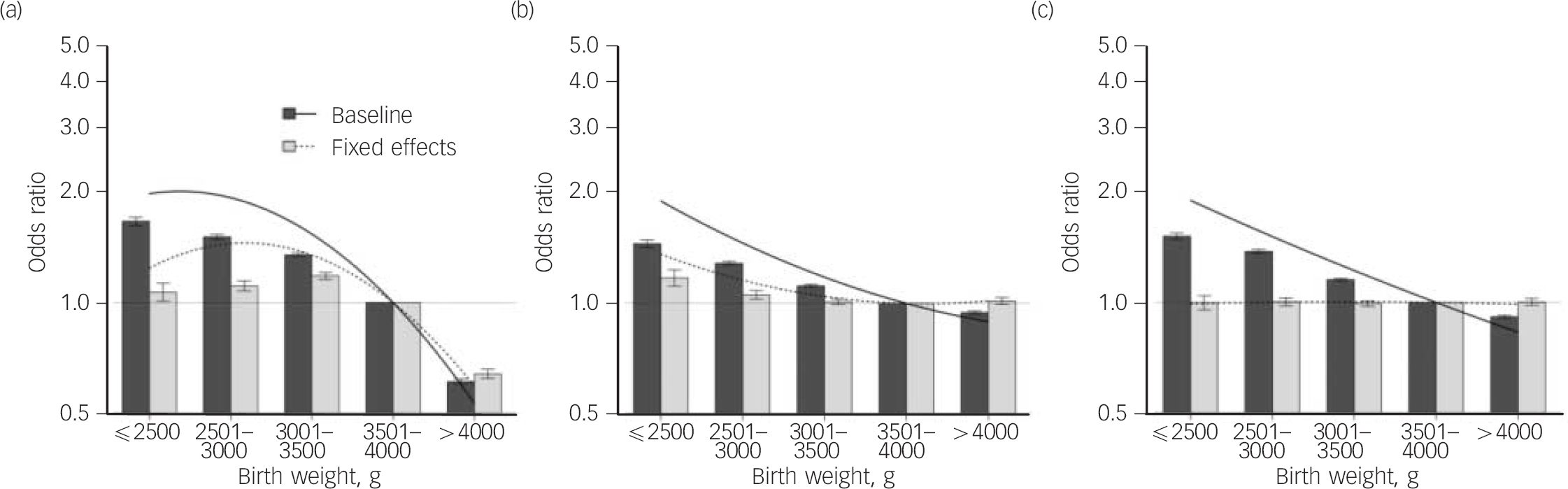
Fig. 2 Associations derived from continuous (line) and ordinal (bar with 95% confidence interval) representation of birth weight when predicting socioeconomic outcomes.
(a) Failing grades, (b) education under 10 years, and (c) social welfare receipt. Baseline, population-wide estimates are shown with the solid line and dark bars. Sibling-comparison, fixed-effects models are shown with dotted lines and light bars. Reference group are those born in the 3501-4000 g birth weight category. Although attenuated, the maintenance of association magnitude across population and sibling-comparison models, consistent with a causal inference, can be noted when predicting failing grades and education under 10 years only.
Discussion
The current study examined the degree to which familial confounding, because of genetic and shared environmental factors, accounts for the associations between fetal growth, indicated by birth weight while controlling for gestational age, and psychiatric and socioeconomic problems. We used a large, well-validated, population-based data-set. The size and scope of the data-set provided us with the opportunity to examine rare and serious outcomes while studying the specificity of our findings across a broad range of outcomes. Further, the data structure allowed us to utilise quasi-experimental designs (for example sibling- and cousin-comparison) with precise measures of predictors and covariates. This is one of the first studies on fetal growth to have the power to examine associations using a sibling-comparison design, an important step towards supporting or refuting causal inferences.
Across outcomes, and in agreement with most previous research, Reference Losh, Esserman, Anckarsater, Sullivan and Lichtenstein2-Reference Matte, Bresnahan, Begg and Susser8,Reference D'Onofrio, Class, Rickert, Larsson, Langstrom and Lichtenstein26,Reference Newcombe, Milne, Caspi, Poulton and Moffitt39 the population estimates suggested that impaired fetal growth, as evidenced by lower birth weights, was associated with greater risk of each outcome. Results from sibling-comparison analyses showed that associations are consistent with causal inferences in an outcome-dependent manner. After fitting sibling-comparison fixed-effects models, the results support causal inferences between fetal growth and ASD, as well as ADHD. Despite some attenuation in fixed-effects models, the relation between fetal growth and psychotic or bipolar disorder, as well as failing grades and education less than 10 years, also supports a causal inference. Therefore, genetic and/or environmental factors specific to fetal development, as indexed by lower birth weight, influence the likelihood of these outcomes. In contrast, our results showed attenuation of the associations between fetal growth and suicide attempt, substance use problems and social welfare receipt, thus suggesting that these associations are primarily as a result of selection effects correlated with fetal growth. Additionally, sensitivity analyses provided evidence against alternative explanations for the findings.
Associations consistent with a causal inference
The associations between birth weight and ADHD and ASD were independent of shared familial confounds and statistical covariates, as the magnitudes of association remained significantly elevated in fixed-effects models. Although some previous research has reported null findings, Reference Hack, Youngstrom, Cartar, Schluchter, Taylor and Flannery1,Reference Hack, Flannery, Schluchter, Cartar, Borawski and Klein5,Reference Ronald, Happe, Dworzynski, Bolton and Plomin18 the current results build on previous co-twin control Reference Losh, Esserman, Anckarsater, Sullivan and Lichtenstein2,Reference Ficks, Lahey and Waldman4,Reference Groen-Blokhuis, Middeldorp, van Beijsterveldt and Boomsma10-Reference Lehn, Derks, Hudziak, van Beijsterveldt and Boomsma12 and epidemiological study findings. Reference Hack, Taylor, Schluchter, Andreias and Drotar3 The associations between birth weight and psychotic or bipolar disorder were also independent of shared familial confounds and statistical covariates, although the magnitudes of association were attenuated in fixed-effects models. Even more attenuated, although still present, were the associations between birth weight and educational attainment variables in the fixed-effects models. Reference Hack, Flannery, Schluchter, Cartar, Borawski and Klein5-Reference Matte, Bresnahan, Begg and Susser8,Reference Newcombe, Milne, Caspi, Poulton and Moffitt39 The interpretation of sensitivity analyses that examined the associations in full-term births only, in families with only one child and when comparing differentially exposed cousins (see online Fig. DS1, DS3, and DS4, respectively) did not differ from the main results. Therefore, overall, our findings lend greater support to the conclusion that fetal growth is along a causal pathway for these outcomes. Our findings also complement previous sibling-comparison research focusing on the long-term outcomes following early gestational age at birth. Reference D'Onofrio, Class, Rickert, Larsson, Langstrom and Lichtenstein26
Comparing the associations across these outcomes, fetal growth appears to be more strongly related to early-onset neurodevelopmental disorders such as ADHD and ASD than for distal markers of neurodevelopmental problems, such as educational problems and later-onset disorders, such as psychotic or bipolar disorder. As evidence across studies converge on a consistent picture of the role of fetal growth on these outcomes, future research must examine possible mediating mechanisms. For example, previous research has shown white matter abnormalities because of brain injury associated with low birth weight. Reference Skranes, Evensen, Lohaugen, Martinussen, Kulseng and Myhr40 Other differences in brain development that correspond with neurodevelopmental problems, such as the amount of cortical surface area, brain volume and caudate volume, have also been noted even across variations within normal birth weight. Reference Walhovd, Fjell, Brown, Kuperman, Chung and Hagler41 Poor in utero nutrition may also be contributing to different fetal growth and altered brain development. Reference de Bie, Oostrom, Delemarre-van and Waal42 ADHD and ASD have been shown to share common genetic aetiology, Reference Pettersson, Anckarsater, Gillberg and Lichtenstein43 which will also have to be explored.
We also found that impaired fetal growth was associated with a decreased likelihood of criminality after fixed-effects modelling and across the sensitivity analyses. This result supports previous fetal growth Reference Hack, Flannery, Schluchter, Cartar, Borawski and Klein5 and gestational age research. Reference D'Onofrio, Class, Rickert, Larsson, Langstrom and Lichtenstein26,Reference Hack44 Fetal-growth-impaired individuals may display personality characteristics linked with decreased risk-taking behaviours, receive increased parental monitoring and/or form fewer relationships with delinquent peers. Investigating violent v. non-violent crimes may elucidate the association further. Reference Kuja-Halkola, Pawitan, D'Onofrio, Langstrom and Lichtenstein45
Associations fully attenuated
Once the genetic and environmental factors that siblings share were controlled, the associations between fetal growth and substance use problems, suicide attempt and social welfare receipt were fully attenuated.
We also found converging evidence for social welfare receipt when predicting low income (see online Fig. DS2). The lack of association with substance use problems is in contrast to a previous co-twin control Reference Foley, Neale and Kendler21 and an epidemiological Reference Hack, Flannery, Schluchter, Cartar, Borawski and Klein5 study showing heavier infants were at increased risk for alcohol and drug use than lower birth weight infants, although measurement varies across studies.
Strengths and limitations
The sibling-comparison design allowed us to begin to address possible genetic confounding Reference Bennedsen, Mortensen, Olesen and Henriksen46 while also offering improved generalisability from a co-twin control approach. Fetal growth differences in twins may be aetiologically distinct from fetal grown differences between singletons, and twins have a greater risk for growth restriction in utero than singletons. Reference Loos, Derom and Vlietinck27 Through the sensitivity analyses, we also explicitly tested some assumptions of the sibling-comparison design. Reference Lahey and D'Onofrio24 Other sensitivity analyses included examining whether associations were driven by gestational age extremes, searching for converging evidence across related outcomes, and using continuously measured birth weight. Further, it should be noted that although our predictor was birth weight, we adjusted all associations for gestational age at birth. Therefore, we consider the predictor an index of fetal growth.
Despite these strengths, however, several limitations must be considered and addressed in future research. Sibling comparisons are not randomised controlled studies; therefore, the design cannot rule out all possible confounding factors and causation cannot be proven. Independent risk associated with fetal growth factors have been shown by comparing birth-weight-discordant monozygotic twins, Reference Losh, Esserman, Anckarsater, Sullivan and Lichtenstein2 which suggest such genetic factors do not explain the associations. Fixed-effects models also have lower statistical power than population-based estimates. Reference Allison47 Additional quasi-experimental research that relies on methods with different assumptions and limitations than the sibling-comparison approach is warranted. Reference Rutter23 Replication in other countries, especially in countries differing in healthcare availability, is also needed.
Implications
Our findings contribute to the aetiological theory of neurodevelopmental disorders and socioeconomic outcomes, as causal inferences were divided by outcome type. The results suggest that efforts be made to reduce the incidence of low-birth-weight births. Results also call for public health initiatives providing services that target risks co-occurring with impaired fetal growth, as the associations between birth weight and substance use problems, suicide attempt, and social welfare receipt were as a result of selection factors that co-occur with birth weight. Further, our findings open an interesting line for future researchers to explore what factors associated with impaired fetal growth contribute to the decreased risk of criminality we identified in sibling-comparison analyses. Overall, the current study emphasises the importance of continued research on the role of fetal growth factors in offspring psychiatric and socioeconomic problems.
Funding
This study was supported by grants from the National Institute of Mental Health (MH094011), National Institute of Child Health and Development (HD061817), the Swedish Council for Working Life and Social Research and the Swedish Research Council (Medicine).






eLetters
No eLetters have been published for this article.