


Since Goffman's Reference Goffman1 classic conceptualisation, stigma theory has made considerable progress. In principle, two major traditions can be distinguished: Reference Yang, Kleinman, Link, Phelan, Lee and Good2 social psychologists such as Jones et al, Reference Jones, Farina, Hastorf, Markus, Miller and Scott3 Crocker et al Reference Crocker, Major, Steele, Fiske, Gilbert and Lindzey4 and Corrigan & Watson Reference Corrigan and Watson5 have developed models that have advanced our understanding of how an individual's stigmatised identity is constructed through cognitive, affective and behavioural processes, whereas sociological models such as Scheff's labelling theory Reference Scheff6 and Link et al's modified labelling theory have focused on processes operating in the social environment that impinge on the stigmatised individual. Reference Link, Cullen, Struenung, Shrout and Dohrenwend7 Some years ago, Link & Phelan Reference Link and Phelan8 proposed a definition of stigma as a broad umbrella concept that links interrelated components of stigma, encompassing both social psychological and sociological models. Most contributions to the advancement of stigma theory have in common that they originate from the USA, i.e. they are looking at stigma through the lens of Western culture.
Yang et al Reference Yang, Kleinman, Link, Phelan, Lee and Good2 have proposed a new theory that includes accounting for how cultural influences have an impact on stigma specifically. The concept of ‘moral experience’ or ‘what is most at stake for actors in a local social world’ provides a new interpretative framework for the behaviours of both the stigmatiser and the stigmatised person. The authors maintain that culture affects stigma by threatening a person's capacity to participate in the activities that determine ‘what matters most’ within a cultural context. For example, because the perpetuation of one's lineage is something that is valued most within Chinese cultures, stigma is seen to most powerfully attack one's ability to extend one's lineage. Reference Yang, Kleinman, Link, Phelan, Lee and Good2
Not only theory but also empirical research on stigma shows a strong bias in favour of Western culture. A review of all population-based studies on beliefs and attitudes about mental illness published between 1990 and 2004 concluded that the vast majority has been conducted in Western countries and only 9 out of a total of 61 studies originated from non-Western countries. Reference Angermeyer and Dietrich9 Although in the meantime the number of studies in non-Western countries has increased considerably, studies from Western countries still predominate. In particular, studies comparing public beliefs and attitudes about mental illness between Western and non-Western cultures are scarce. Apart from the Stigma in Global Context-Mental Health Study, Reference Pescosolido, Medina, Martin and Long10 which covers 16 countries around the globe, population-based cross-cultural studies on public stigma of mental illness have focused mainly on East Asian cultures, comparing Japan with Australia, Reference Griffiths, Nakane, Christensen, Yoshioka, Jorm and Nakane11 Mongolia with Germany Reference Angermeyer, Buyantugs, Kenzine and Matschinger12 and Chinese immigrants with the rest of the US population. Reference Yang, Purdie-Vaughns, Kotabe, Link, Saw and Wong13 So far, no attempt has been made to compare attitudes prevalent in the Arab world with those observed in Western culture. This study sets out to fill this gap by comparing public beliefs and attitudes about schizophrenia in a country in Central Europe (Germany) and in North Africa (Tunisia). Up to now only two studies on the stigma of schizophrenia have been conducted in Tunisia. One of the main findings of a population study on social representations of mental illness, which had been carried out in a northern district of the country, was that the term ‘insane’ is dominated by pejorative connotations and the perception of dangerousness, unpredictability and violence. Reference Cherif, Elloumi, Ateb, Nacef, Cheour and Roelandt14 Similarly, in a study among relatives of patients with schizophrenia the perception of dangerousness and unpredictability was shared by the majority of participants. Reference Bouhlel, Ben Haouala, Klibi, Ghaouar, Chennoufi and Melki15 Apart from these stereotypes, which seem to be a common feature of the stigma of psychosis across Western as well as non-Western cultures, Reference Pescosolido, Medina, Martin and Long10 little is known about other stigma components and nothing about how the stigma prevalent in Tunisia compares in form and magnitude to that observed in Western countries like Germany.
Describing cultural differences between countries might always appear as an oversimplification, but it is generally agreed that family loyalty and the importance of the group are highly valued in Arab culture, which contrasts to the individualism and self-reliance that are stereotypically associated with Western culture. In Arab culture, intense feelings of loyalty and dependence are fostered and preserved by the family. Family loyalty and obligations take precedence over loyalty to friends or demands of a job. Members of the family are expected to support each other in disputes with outsiders regardless of personal antipathy among relatives, defending each other's honour and displaying group cohesion. Reference Nydell16–Reference Geertz, Geertz, Geertz and Rosen19 Following Yang et al's Reference Yang, Kleinman, Link, Phelan, Lee and Good2 reasoning, we would thus argue that family ‘matters most’ to people living in Tunisia. We therefore expect that stigma in Tunisia is particularly deleterious with regard to social roles related to the family, distinguishing these relationships from other, family-unrelated social contacts. This would contrast with the well-established pattern of rejection in Western countries such as Germany or the USA, Reference Angermeyer and Dietrich9 where rejection of people with mental illness follows a simple gradient from more distant to more intimate social relationships, centred around the individual and placing family relations between other closer and more distant social relations. Following Link et al's Reference Link and Phelan8,Reference Link, Angermeyer, Phelan, Thornicroft, Szmukler, Mueser and Drake20 conceptualisation of stigma we will investigate public beliefs about schizophrenia (for example causal attributions) and stereotypes that prevail about people with this illness (such as perception that they are dangerous). We further will investigate emotional reactions elicited by individuals with schizophrenia and the public's willingness to interact with them across situations that vary in intimacy. As proposed by Link et al, we conceive emotional reactions as mediator between beliefs and stereotypes on the one hand and social distance on the other.
Method
Participants
Population surveys were conducted in Germany in 2011 (n = 3642) and in Tunisia in 2012 (n = 834). In Germany, a multistage probability sampling was used with (a) sample points, (b) households, and (c) individuals within the target households. Target households within the sample points were determined according to the random route procedure (i.e. a household was selected randomly as a starting point from where a set route through the area was followed); target individuals within households were selected using random digits (response rate 64.0%). In Tunisia a quota sample was used with stratification for gender, age, family status, socioeconomic status and region. In Germany, the sample was drawn only from people with German citizenship, in Tunisia from those with Tunisian citizenship. Eligible respondents were individuals not living in institutions, in Germany aged 18 years and over, in Tunisia between 15 and 65 years. The sociodemographic characteristics of both samples are reported in online Tables DS1 and DS2. Comparison with official statistical data shows that our samples reflect fairly well the sociodemographic composition of the general population of both countries, except for an underrepresentation of people who are illiterate in Tunisia for methodological reasons (some questions had to be answered using paper and pencil).
Informed consent was considered to have been given when individuals agreed to complete the interview. Trained interviewers recruited from the respective countries conducted the interviews. Fieldwork was done by companies who specialise in market and social research (in Germany by USUMA GmbH (Berlin), in Tunisia by BJKA Consulting (Tunis)). For the sake of comparability of samples, only respondents aged 18–65 years were included in this study. We also included only respondents who had been presented with a vignette depicting a case of someone with schizophrenia (see below). This resulted in an effective sample size of 931 individuals in Germany and 404 individuals in Tunisia.
Interview
In both surveys, the same interview mode (face to face) was used. The interview had originally been developed in Germany and has already been used in several surveys. On both occasions, the fully structured interview was identical regarding the wording and sequence of questions. At the beginning of the interview respondents were presented with a vignette of a diagnostically unlabelled psychiatric case history. Then, respondents were asked a series of questions to assess their beliefs about the disorder described in the vignette as well as their attitudes towards the person with it. For use in this study, the interview was translated into colloquial Arab by a translator. A bilingual panel reviewed the translation, looking for any inconsistencies between the original and the translated version. The translated interview was then back-translated by an independent translator and both versions were compared by the panel. If significant differences were apparent, they were discussed until equivalence between both versions was achieved.
In Germany, vignettes depicting a case of someone with schizophrenia, major depressive disorder or alcohol dependence was used, in Tunisia only vignettes with schizophrenia or depression. The symptoms described in the vignettes fulfilled the criteria of DSM-IV for the respective disorder. 21 In a previous study, the vignettes had independently been rated by five experts on psychopathology masked to actual diagnosis, providing confirmation of the correct diagnosis for each case history. The gender of the individual presented in the vignettes was randomly varied. Respondents were randomly allocated to receive one of the vignettes.
Measures
Beliefs and stereotypes
Several items tapping into respondents' beliefs and stereotypes about schizophrenia were selected for this study. For all of them an association with attitudes towards those with schizophrenia had been shown in previous studies.
-
(a) One item measured belief in a continuum of symptom experience (‘Basically, we are all sometimes like this person. It's just a question how pronounced this state is’).
-
(b) Three items were included that according to previous analyses can be considered as representative of biological causes (‘brain disease’), current stress (‘work-related stress including unemployment’) and childhood adversities (‘lack of parental affection’). In Tunisia, an item referring to religious beliefs (‘lack of faith in God’) was added. This item was not included in the German survey since in a previous study only a small minority of less than 10% of respondents had endorsed this cause. Reference Angermeyer and Matschinger22
-
(c) One item served for assessment of treatment prognosis (‘after treatment, this person will be able to lead a normal life’).
-
(d) One item each measured onset responsibility (‘the person is himself/herself to blame for getting his/her condition’) and offset responsibility (‘the person only has to pull herself/himself together to get well again’).
-
(e) One item assessed the stereotype of dangerousness (‘this person is dangerous’), another one the stereotype of unpredictability (‘this person is unpredictable’).
We measured all individual items via five-point Likert scales ranging from ‘1’ (strong agreement) to ‘5’ (strong disagreement).
Attitudes
For the assessment of attitudes towards the person described in the vignette we used two well-established scales. Emotional reactions to the person described in the vignette were assessed by means of the Emotional Reactions to the Mentally Ill Scale (ERMIS). Reference Angermeyer and Matschinger23 The scale includes the following ten items: ‘I feel the need to help him/her’, ‘I feel sympathy for him/her’, ‘I feel uncomfortable’, ‘He/she makes me feel insecure’, ‘He/she scares me’, ‘I feel pity for him/her’, ‘I feel annoyed by him/her’, ‘I react angrily’, ‘I am amused by something like that’, ‘This person provokes my incomprehension’. Answers are given on five-point Likert scales anchored with 1, ‘applies completely’ and 5, ‘does not apply at all’.
For the assessment of respondents' desire for social distance we used the scale developed by Link et al. Reference Link, Cullen, Frank and Wozniak24 This scale encompasses the following social situations: rent a room, work together, have as neighbour, let take care of little children, have marry into family, introduce to friends, recommend for a job. With the help of five-point Likert scales, with the anchors 1, ‘certainly’ and 5, ‘certainly not’, respondents can indicate to what extent they are willing or unwilling to engage in the proposed relationships.
Statistical analysis
A detailed description of the statistical procedures employed is provided in online supplement DS1. In brief, we carried out analyses on item level for the combined sample, using multinomial logit regression models and collapsing the five-point Likert scales into three categories (for example ‘agree’, ‘undecided’, ‘disagree’). These models yield predicted probabilities for choosing each category in Germany and Tunisia as well as the predicted differences (probability change) between both countries, all given as percentages. For the analysis of the association between beliefs and attitudes a two-step approach was chosen. We first conducted separate explorative factor analyses for both countries using the entire scales on emotional reactions and social distance. Because these analyses yielded different factor solutions in both samples, we calculated factor scores for Germany and Tunisia that were then used in separate path analyses. The path models for both countries were fully saturated.
Results
Comparison of public beliefs about schizophrenia and stereotypes about people with this condition
The probability that respondents shared the view that there is a continuum of schizophrenic symptoms from the normal to the pathological was twice as high in Tunisia as in Germany (Table 1). German respondents three times as frequently endorsed brain disease as a cause compared with their Tunisian counterparts, who were more in favour of psychosocial explanations. The expectation that after treatment the person with schizophrenia will completely recover and will be able to lead a normal life was more prevalent among individuals from Tunisia. There was a stronger tendency among Tunisian respondents to hold the person with the disorder responsible for the onset of the condition. They also more frequently shared the view that this person has only to pull themselves together to get well again (offset responsibility). The stereotype of unpredictability was more common among Tunisian respondents, who at the same time were more frequently opposed to considering people with schizophrenia as dangerous (for raw percentages see online Table DS3).
Table 1 Beliefs about schizophrenia and stereotypes about people with schizophrenia: comparison between Germany and Tunisia (multinomial logit regressions)

| Predicted percentages | |||
|---|---|---|---|
| Response category | Germany | Tunisia | Difference a (95% CI) |
| Continuum between the ‘normal’ and the pathological | |||
| Agree | 27 | 59 | 32 (23 to 41) |
| Undecided | 26 | 19 | −7 (−15 to 1) |
| Disagree | 47 | 22 | −25 (−33 to −16) |
| Causal attribution to brain disease | |||
| A cause | 61 | 15 | −47 (−54 to −39) |
| Undecided | 22 | 9 | −13 (−19 to −7) |
| Not a cause | 17 | 76 | 60 (52 to 67) |
| Causal attribution to work-related stress | |||
| A cause | 63 | 75 | 12 (3 to 20) |
| Undecided | 22 | 12 | −10 (−17 to −4) |
| Not a cause | 15 | 14 | −1 (−8 to 5) |
| Causal attribution to lack of parental affection | |||
| A cause | 34 | 51 | 17 (8 to 27) |
| Undecided | 27 | 11 | −16 (−23 to −9) |
| Not a cause | 39 | 38 | −1 (−10 to 8) |
| After treatment person will lead a normal life | |||
| Agree | 50 | 83 | 33 (26 to 41) |
| Undecided | 36 | 10 | −26 (−33 to −19) |
| Disagree | 14 | 6 | −8 (−13 to −2) |
| Person to blame for getting his/her condition | |||
| Agree | 8 | 38 | 30 (22 to 39) |
| Undecided | 21 | 17 | −4 (−11 to 4) |
| Disagree | 71 | 45 | −27 (−36 to −18) |
| Person has to pull herself/himself together to get well again | |||
| Agree | 21 | 79 | 58 (50 to 66) |
| Undecided | 29 | 11 | −17 (−24 to −10) |
| Disagree | 50 | 10 | −41 (−48 to −33) |
| Person is unpredictable | |||
| Agree | 50 | 66 | 16 (7 to 25) |
| Undecided | 29 | 18 | −11 (−18 to −3) |
| Disagree | 21 | 16 | −5 (−12 to 2) |
| Person is dangerous | |||
| Agree | 24 | 23 | −1 (−9 to 7) |
| Undecided | 32 | 22 | −10 (−18 to −2) |
| Disagree | 45 | 55 | 11 (1 to 20) |
a. Because of rounding figures shown will not always equal the difference between predicted percentages. Statistically significant changes in bold.
Comparison of emotional reactions to people with schizophrenia
As reported in Table 2, across both countries, respondents most frequently showed prosocial reactions, followed by fear and related feelings; least frequently they reacted with anger. However, respondents from Tunisia were more likely to express sympathy for the person described in the vignette and to feel the need to help, whereas those from Germany tended to react with more fear and to feel more uncomfortable. Except for incomprehension, which respondents from Tunisia were more likely to express, there were no significant differences between both countries regarding angry feelings (for raw percentages see online Table DS4).
Table 2 Emotional reactions towards people with schizophrenia: comparison between Germany and Tunisia (multinomial logit regressions)

| Predicted percentages | |||
|---|---|---|---|
| Response category | Germany | Tunisia | Difference
a
(95% CI) |
| I feel the need to help him/her | |||
| Agree | 59 | 88 | 29 (22 to 37) |
| Undecided | 28 | 7 | −21 (−28 to −17) |
| Disagree | 13 | 5 | −8 (−13 to −4) |
| I feel pity for him/her | |||
| Agree | 69 | 77 | 8 (−0 to 16) |
| Undecided | 24 | 8 | −16 (−22 to −9) |
| Disagree | 7 | 14 | 7 (1 to 13) |
| I feel sympathy for him/her | |||
| Agree | 22 | 88 | 66 (59 to 72) |
| Undecided | 34 | 9 | −25 (−32 to −9) |
| Disagree | 44 | 3 | −41 (−47 to −34) |
| I feel uncomfortable | |||
| Agree | 49 | 32 | −17 (−26 to −8) |
| Undecided | 26 | 25 | −1 (−9 to 8) |
| Disagree | 25 | 43 | 18 (9 to 26) |
| He/she makes me feel insecure | |||
| Agree | 34 | 28 | −6 (−15 to 2) |
| Undecided | 29 | 26 | −3 (−11 to 6) |
| Disagree | 37 | 46 | 9 (0 to 18) |
| He/she scares me | |||
| Agree | 36 | 24 | −13 (−21 to −4) |
| Undecided | 25 | 14 | −10 (−17 to −3) |
| Disagree | 39 | 62 | 23 (14 to 32) |
| I feel annoyed by him/her | |||
| Agree | 13 | 18 | 5 (−1 to 12) |
| Undecided | 26 | 18 | −7 (−15 to 1) |
| Disagree | 62 | 64 | 2 (−7 to 11) |
| I react angrily | |||
| Agree | 7 | 8 | 4 (−4 to 5) |
| Undecided | 15 | 12 | −3 (−10 to 3) |
| Disagree | 77 | 80 | 3 (−5 to 11) |
| I am amused by something like that | |||
| Agree | 6 | 5 | −1 (−4 to 3) |
| Undecided | 7 | 8 | 0 (−5 to 5) |
| Disagree | 87 | 87 | 0 (−6 to 6) |
| The person provokes my incomprehension |
|||
| Agree | 19 | 49 | 30 (21 to 39) |
| Undecided | 25 | 24 | −2 (−10 to 7) |
| Disagree | 56 | 28 | −28 (−37 to −19) |
a. As a result of rounding figures shown will not always equal the difference between predicted percentages. Statistically significant changes in bold.
Separate principal component analyses of the ten items assessing emotional reactions for each country yielded different factor structures. In the German sample, we were able to replicate the three-factor structure that had been found in previous studies. Reference Angermeyer and Matschinger23 Items loading primarily on the first factor, which we termed ‘fear’ (eigenvalue 2.914), were ‘The person provokes fear’, ‘I feel uncomfortable’ and ‘I feel unsecure’. Items loading primarily on the second factor, which was termed ‘anger’ (eigenvalue 1.920), were ‘I react angrily’, ‘I am amused’, ‘I feel irritated’ and ‘The person provokes my incomprehension’. The third factor, termed ‘prosocial reactions’ (eigenvalue 1.396), comprised the items ‘I feel pity’, ‘I feel sympathy’ and ‘I feel the need to help’. The three factors accounted for a cumulative variance of 62.3%. Cronbach's alpha for the subscales representing the three emotional reactions was 0.78, 0.73 and 0.60.
In contrast, principal component factor analysis in the Tunisian sample yielded only two factors with eigenvalues >1. With the exception of ‘I feel amused’, the first factor (eigenvalue 2.610) comprised all the items describing feelings of fear and anger. We termed this factor ‘negative feelings’. The second factor, termed ‘prosocial reactions’ (eigenvalue 1.894), corresponded to the factor with the same label found in Germany, except that it also included the item ‘I am amused’, which loaded negatively on it. The two factors explained together only 45.5% of variance. Cronbach's alpha for ‘negative feelings’ was 0.71, for pro-social reactions 0.6. For both countries, rotated factor loadings of the ten items are reported in online Table DS5.
Comparison of the public's desire for social distance from people with schizophrenia
Whereas in Germany social distance increased stepwise from a low of 29% (have as neighbour) to a high of 76% (take care of children), in Tunisia rejection of the person in the vignette was rather dichotomised with very high percentages unwilling to have such a person marry into family (71%) and take care of children (93%) and relatively low percentages unwilling to engage in all other social relationships (maximum 32%). Although across all more distant relationships, Tunisian respondents' desire for social distance was much smaller than that expressed by those from Germany, they reacted with stronger rejection than German respondents when asked about intimate relationships (have marry into family, take care of children) (Table 3 and online Table DS6).
Table 3 Desire for social distance from people with schizophrenia: comparison between Germany and Tunisia (multinomial logit regressions)

| Predicted percentages | |||
|---|---|---|---|
| Response category | Germany | Tunisia | Difference
a
(95% CI) |
| Have as neighbour | |||
| Agree | 37 | 78 | 41 (33 to 49) |
| Undecided | 34 | 14 | −20 (−28 to −13) |
| Reject | 29 | 8 | −21 (−27 to −14) |
| Work together | |||
| Agree | 41 | 74 | 33 (25 to 42) |
| Undecided | 28 | 12 | −16 (−23 to −9) |
| Reject | 32 | 14 | −18 (−25 to −10) |
| Rent a room | |||
| Agree | 19 | 56 | 37 (28 to 46) |
| Undecided | 23 | 12 | −11 (−18 to −4) |
| Reject | 58 | 32 | −26 (−35 to −17) |
| Introduce to a friend | |||
| Agree | 19 | 73 | 54 (46 to 61) |
| Undecided | 23 | 16 | −7 (−15 to 0) |
| Reject | 58 | 12 | −46 (−53 to −39) |
| Recommend for a job | |||
| Agree | 11 | 54 | 42 (34 to 51) |
| Undecided | 26 | 18 | −8 (−15 to 0) |
| Reject | 63 | 28 | −35 (−43 to −26) |
| Have marry into family | |||
| Agree | 12 | 17 | 5 (−2 to 12) |
| Undecided | 28 | 12 | −17 (−23 to −10) |
| Reject | 60 | 71 | 11 (3 to 20) |
| Let take care of little children | |||
| Agree | 8 | 3 | −5 (−8 to −1) |
| Undecided | 17 | 4 | −13 (−18 to −7) |
| Reject | 76 | 93 | 17 (11 to 24) |
a. As a result of rounding figures shown will not always equal the difference between predicted percentages. Statistically significant changes in bold.
In Germany, we were able to replicate the uni-dimensional structure of Link's Social Distance Scale found in previous studies (eigenvalue 4.397, explained variance 62.8%). Reference Croker25 The internal consistency amounted to an alpha of 0.90. In contrast, in Tunisia principal component analysis yielded three factors with eigen-values >1. The first factor (eigenvalue 2.410) was represented by the items ‘Introduce to a friend’ and ‘Recommend for a job’, the second factor (eigenvalue 1.401) included the items ‘Rent a room’, ‘Work together’ and ‘Have as neighbour’, and the third factor (eigenvalue 1.003) comprised the items ‘Have marry into family’ and ‘Let take care of little children’. Since the three factors appear to represent a gradient from more distant to more close relationships we termed the first factor ‘rejection in intermediate relationships’, the second ‘rejection in distant relationships’ and the third factor ‘rejection in intimate relationships’. The three factors accounted for a cumulative variance of 68.7%. As a result of the small number of items, internal consistency of the three subscales was relatively low (alpha 0.71, 0.60, and 0.56 respectively). Factor loadings are reported in online Table DS7.
Association between beliefs about schizophrenia and attitudes towards those with it
Figures 1 and 2 summarise, separately for Germany and Tunisia, the results of the path analyses for the relationship between illness beliefs and stereotypes, emotional reactions and desire for social distance. Only significant paths are depicted (P<0.05). Numbers indicate standardised path coefficients (β). In Germany, our model explained 21% of the variance of fear, 20% of the variance of anger and 16% of the variance of prosocial reactions. In Tunisia, 41% of the variance of negative feelings and 27% of the variance of prosocial reactions were explained. In Germany, 27% of the variance of social distance (all relationships combined) could be explained, whereas in Tunisia explanation of variance amounted to 11% as regards distant relationships, 16% as regards intermediate relationships and 19% as regards intimate relationships.

Fig. 1 Path model for respondents in Germany of relationships between illness beliefs/stereotypes, emotional reactions and desire for social distance.
Standardised path coefficients; only statistically significant paths are shown. **P<0.01, ***P<0.001.
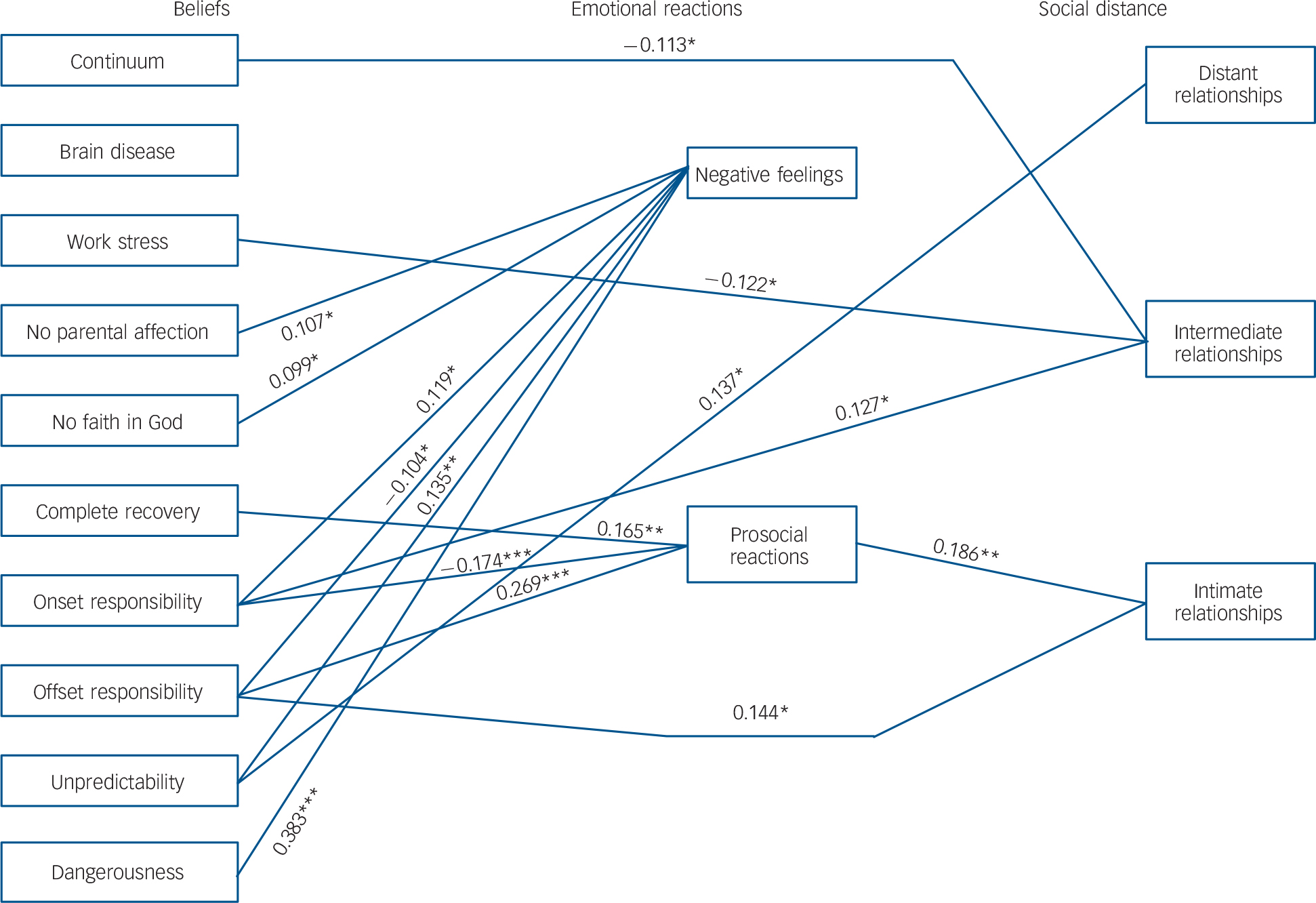
Fig. 2 Path model for respondents in Tunisia of relationships between illness beliefs/stereotypes, emotional reactions and desire for social distance.
Standardised path coefficients; only statistically significant paths are shown. *P<0.05, **P<0.01, ***P<0.001.
Germany
In Germany (Fig. 1), fear was most frequently elicited by the perception of unpredictability. The endorsement of brain disease as a cause was also associated with more fear. The same applied to the perception of dangerousness, which additionally evoked anger. The ascription of offset responsibility showed a strong association with anger: the more respondents shared the view that the person has to pull themselves together to get better, the more they reacted angrily. The attribution to a lack of parental affection was also related to more anger. The ascription of onset responsibility was associated with more anger and less prosocial reactions, whereas with work-related stress the opposite was found. Continuum beliefs had the strongest effect on prosocial reactions: the more respondents agreed with the notion that there is a continuum between the normal and the pathological, the more they were inclined to react prosocially. The expectation of complete recovery showed a less pronounced relationship in the same direction.
There was a strong link between the expression of fear and more social distance, whereas prosocial reactions were associated with less social distance and anger was unrelated. The perception of unpredictability was associated with an increase in social distance (total effect β = 0.179, P⩽0.001), directly (β = 0.108, P⩽0.01, Fig. 1), as well as indirectly (β = 0.071, P⩽0.001), mainly through an increase in fear (β = 0.062, P⩽0.001). In contrast, continuum beliefs and the expectation of complete recovery were accompanied by less social distance (total effect β = −0.253, P⩽0.001 and β = −0.145, P⩽0.001 respectively). With both, the direct effect on social distance (β = −0.189, P⩽0.001 and β = −0.123, P⩽0.001 respectively) was greater than the indirect effect (β = −0.064, P⩽0.001 and β = −0.022, P⩽0.05 respectively), which was mainly mediated through an increase in prosocial reactions (β = −0.054, P⩽0.001, and β = −0.032, P⩽0.001 respectively). Apart from that, there were a few exclusively indirect associations between beliefs and social distance: onset responsibility was indirectly related to greater social distance (β = 0.033, P⩽0.05) mainly through a decrease of prosocial reactions (β = 0.036, P⩽0.001) (total effect β = 0.068, P⩽0.05). The attribution to work-related stress exerted an indirect effect in the opposite direction (β = −0.039, P⩽0.01), which also was mediated through an increase of prosocial reactions (β = −0.039, P⩽0.05) (total effect non-significant.). The perception of dangerousness and the endorsement of brain disease as a cause were only indirectly associated with greater social distance through an increase in fear (β = 0.024, P⩽0.01 and β = 0.029, P⩽0.001 respectively; total effect β = 0.079, P⩽0.05 and β = 0.017, non-significant respectively).
Tunisia
In Tunisia (Fig. 2), the perception of dangerousness showed the strongest association with negative feelings: the more respondents considered the person in the vignette to be dangerous, the more negative feelings they expressed. Also, attributing the condition to a lack of parental affection or to a lack of faith in God, was associated with stronger negative reactions. The strongest relationship with prosocial reactions displayed the ascription of offset responsibility, which, contrary to expectations, was associated with more prosocial reactions (and less negative feelings). The opposite pattern was found with onset responsibility, which was related to less prosocial and more negative feelings. The perception of unpredictability was accompanied by more negative feelings, whereas the expectation of complete recovery was associated with more prosocial reactions.
Negative feelings showed no significant association with either one of the three dimensions of social distance. Prosocial reactions were significantly related only to social distance regarding intimate relationships: contrary to what one might have expected and to what has been observed in Germany, they were associated with greater rejection of the person in the vignette. As regards distant relationships, there was only one single significant association between illness beliefs/stereotypes and the desire for social distance: the perception of unpredictability was directly related to greater social distance (β = 0.137, P⩽0.05) (total effect β = 0.116, P⩽0.05). As regards intermediate relationships, there were also only direct links between beliefs and social distance: continuum beliefs and the endorsement of work-related stress as a cause were directly associated with less desire for social distance (β = −0.113, P⩽0.05 and β = −0.122, P⩽0.05 respectively; total effect β = −0.110, P⩽0.05 and β = −0.112, P⩽0.05 respectively), whereas onset responsibility was associated with greater desire for social distance (direct effect β = −0.127, P⩽0.05; total effect β = 0.132, P⩽0.05). Offset responsibility was related to greater social distance in intimate relationships directly (β = 0.144, P⩽0.05) and (to lesser extent) also indirectly (β = 0.047, P⩽0.05), mediated mainly through an increase in prosocial reactions (β = 0.050, P⩽0.05); both effects yielded a total effect of β = 0.191 (P⩽0.01).
Discussion
Social distance from people with schizophrenia
Whereas in Germany a notion of social distance seems to prevail that encompasses all social relationships in question, in Tunisia a clear distinction was made according to the degree of closeness. For people from Tunisia it appears to make a difference whether the relationship to another person is rather distant and instrumental such as having them as a neighbour, colleague at work or tenant, or the relationship is somewhat closer, placing more personal responsibility on the actor (recommending for a job, introducing to friends) or the relationship is very intimate, involving one's own family (have someone marry into family, let someone take care of little children). Tunisian people seem to draw a clear line particularly between family roles and relationships outside the family: marrying into the family was rejected by almost three-quarters of respondents and letting take care of little children by almost everyone, whereas in all other social relationships rejection was relatively low or practically non-existance. In contrast, in Germany no such sharp distinction was made between family-related and other social roles. Regarding the two family-related relationships, Tunisian respondents expressed more desire for social distance than their German counterparts however, with regard to all other relationships the opposite was the case, i.e. people from Tunisia were much more accepting (on average, the percentage of those who would accept a person with schizophrenia in more distant relationships was twice as high as in Germany).
Our findings on social distance clearly reflect Arab culture as summarised in the introduction, placing great importance on the family. For people in Tunisia, as in Arab countries in general, their first obligation usually is to their families and this affects most of the other things in their lives, everything else will take a back seat to family issues. Reference Demeerseman17 In a vignette study conducted in Egypt, Croker Reference Croker25 found that the notion of social distance may differ from what it denotes in Western culture: ‘Practical considerations of role-appropriateness take precedence over fears of social “closeness”’. Far from being concerned about the potential danger emanating from the person with mental illness (which plays an important role in Western cultures, see our results in Germany), respondents appear instead to be focused on the ability of the individual to fulfil the social role implied in the proposed relationship. Croker concluded that ‘social distance or stigma in Egypt is a reflection of a series of practical and moral judgments about the person's ability to fulfil a given role, their moral worth and their place in the social fabric’. Reference Croker25
This leads directly to Yang et al's concept of ‘moral experience’, or ‘what is most at stake for actors in a local social world’, which has already been discussed. Reference Yang, Kleinman, Link, Phelan, Lee and Good2 Stigma seems to exert its core effects by threatening the loss or diminution of what is most at stake in Arab culture, namely meaningfully participating in family life and fulfilling family obligations. As social ideals of ‘personhood’ lay in taking responsibility for the family and contributing to its well-being, people with schizophrenia might fail to affirm these ideals. Being denied marrying into a family or taking care of little children, they are excluded from what ‘matters most’ in this culture. The importance of fulfilling family-related roles is also highlighted by the result that the ascription of offset responsibility was related to social distance only regarding the most intimate relationships. Taking responsibility for getting well again was considered of key importance here. If the person was to blame for not making efforts to improve their condition they were facing more rejection. By contrast, rejection in distant relationships was most strongly associated with the perception of unpredictability.
The concept of ‘what matters most’ may also help interpret the results from Germany. Apart from introducing someone to friends, the difference between Tunisia and Germany in social distance was greatest as regards recommending the person in the vignette for a job: in Germany only every tenth respondent was willing to do that, whereas it was every second in Tunisia. In Germany, recommending such a person for a job was equally frequently denied as having them marry into family. This may be a reflection of the role work plays in German culture. This interpretation is supported by results of a focus group study among patients with schizophrenia, their relatives and mental health professionals that was conducted in Germany a few years ago. Reference Schulze and Angermeyer26 Among the obstacles denying access to important social roles, barriers on the access to employment and related professional roles were mentioned most frequently. People with schizophrenia may have experienced stigma most acutely in the area of work because they might not exhibit the achievement or competitiveness needed for high-performing jobs that are central to societal recognition. Reference Yang, Thornicroft, Alvarado, Vega and Link27 Another indication of the importance attributed to work in Germany may also be seen in that the notion of ‘burnout’ because of too much stress at work seems particular popular in this country. Reference Angermeyer, Schomerus, Carta, Moro, Toumi and Millier28
Emotional reactions to people with schizophrenia
In Tunisia, respondents expressed more prosocial reactions than in Germany, which is in line with the fact that helping others who are in need represents an important value in Arab culture. Reference Nydell16 However, in contrast to Germany, where prosocial reactions were strongly associated with less social distance, in Tunisia prosocial reactions proved to be unrelated to social distance in distant and intermediate relationships, whereas in intimate relationships they were associated with more rather than less desire for social distance. In search of an explanation for this at first glance counterintuitive finding Croker's Reference Croker25 observation may prove useful that, in the context of Arab culture, the notion of social distance may indicate less the willingness to engage in a distant or close relationship with a target individual (which is the prevailing meaning in Western culture) than the willingness to engage in relationships that emphasise reciprocity and the role responsibilities that the target individual must fulfil. The more someone evokes the feeling that they need to be helped, the more people might be hesitant to entrust the person with role obligations they are considered unable to fulfil. This is particularly relevant when it comes to family obligations. Thus, there is the paradox that people from Tunisia react more prosocially to people with schizophrenia than their German counterparts but at the same time they tend to keep them away from roles implying taking responsibility for their families.
In Germany, respondents reacted with more fear than in Tunisia. In Germany, perceptions of unpredictability and dangerousness were significantly associated with more fear, which in turn was significantly associated with more social distance. Thus, both misperceptions were indirectly linked to social distance. In Tunisia, the picture was different. Although, similar to Germany, the perceptions of dangerousness and unpredictability were associated with more negative feelings, in Tunisia negative feelings were not significantly related to social distance. Thus, in Germany fear seems to play a more prominent role in the relationship to people with schizophrenia than in Tunisia. This underscores the fact that stigma may operate in different cultures in different ways and that what, based on Western theorising, might have been considered to be a ‘universal’ pathway does not necessarily apply to non-Western cultures.
Beliefs about schizophrenia and stereotypes about people with it
Compared with Germany, respondents from Tunisia showed a much lower tendency to draw a sharp line between mental health and mental illness. The notion of a continuum of symptoms between the normal and the pathological enjoyed more acceptance in Tunisia than in Germany. In Tunisia, thinking in diagnostic dichotomies as promoted by Western psychiatry has obviously penetrated the lay concept of mental illness to a limited extent only, and the perception that psychopathological phenomena are rather variations of normal experiences still prevails. Most notably, in Tunisia as in Germany, continuum beliefs were associated with less desire for social distance
Over the past decade the public in Germany as in other Western countries has been increasingly exposed to information on biochemical and genetic aetiological theories, with the consequence that a biomedical model of mental disorders nowadays enjoys growing popularity. Reference Schomerus, Schwahn, Holzinger, Corrigan, Grabe, Carta and Angermeyer29 This may be one of the reasons why in Germany four times as many respondents endorsed brain disease as a cause than in Tunisia, where respondents were more inclined to endorse psychosocial causes like work-related stress or lack of parental affection. Instead of conceptualising the deviant behaviour described in the vignette as originating from a disease located in the individual, Tunisian people were more inclined to seek the cause for the condition in difficulties of life.
Whereas in Germany, a largely secularised Western country, medical–psychiatric conceptualisations of mental illness have permeated the public notion of mental illness, in Tunisia, a country where around 98% of the population are Muslims, religious beliefs are still of great importance. Islam views mental disorders as an outcome of an inadequate relationship with God. According to this perception, an inadequate relationship with God can be expressed by failure to observe the laws of Islam as prescribed in the Koran and the petitions of the Prophet Muhammad. Reference Nydell16 In fact, 61% of our Tunisian respondents attributed the cause to a lack of faith in Allah. Similarly, in a previous study in Tunisia among relatives of patients with schizophrenia, 77% of respondents had cited religious causes. Reference Bouhlel, Ben Haouala, Klibi, Ghaouar, Chennoufi and Melki15 This tendency to see mental illness as resulting from an inadequate relationship with God and, consequently, as a divine punishment, may exacerbate negative attitudes towards mentally ill people. Reference Haj-Yahia30 Indeed, the more our Tunisian respondents endorsed this view the more they reacted with negative feelings.
On the other hand, there may also be a good side to the perception of mental illness as punishment from God. As we have seen, people from Tunisia were more likely to share the view that after treatment the person in the vignette will recover completely and be able to lead a normal life, whereas German respondents were more sceptical in this regard. One reason for this optimistic view may be that illness is seen as an opportunity to remedy disconnections from God through regular prayer. Reference Ciftci, Jones and Corrigan31 In this context it is of interest that 75% of our respondents in Tunisia recommended seeking help from an imam (as compared with only 10% recommending a priest in Germany). In both countries treatment optimism was positively related to prosocial reactions, however, it had no significant influence on the desire for social distance. This contradicts the widely shared belief that if we could only cure mental illness, then, there would be no stigma.
Strengths and limitations
The strength of our study is that it is based on the first population-based survey on attitudes and beliefs about mental illness that has been conducted in North Africa on a national scale. However, before extrapolating from our findings to Arab culture in general, replications in other Arab countries are needed. The fact that in both countries the same interview has been used for measuring attitudes and beliefs represents another strength of our study. As mentioned, only a few population-based studies exist so far that allow direct comparison between different cultures. However, what is a strength of our study could also be seen as a weakness. As mentioned in the Method section, the instrument for the assessment of emotional reactions of respondents had been developed in Germany and the assessment of the desire for social distance originated from the USA. These instruments might be suited for adequately measuring the two stigma components in the German context, and, in fact, we were able to replicate the dimensional structure found in previous studies, Reference Angermeyer and Matschinger23 but it is questionable whether this also holds for Tunisia. For instance, principal component analyses explained less variance of emotional reactions in Tunisia (45.5%) than in Germany (62%). The same applied to social distance, with 46% explained variance in Tunisia and 63% in Germany. In Tunisia our measures may also have been less able to mirror what social distance means in this cultural context; we may also have missed emotions that may play a greater role in Tunisia than in Germany when people are confronted with mental illness (for example honour and shame). Moreover, another consequence of the approach we have chosen might be that we were able to capture culture-specific aspects of stigma only to a limited extent. Complementing our quantitative analysis by qualitative methods would certainly help increase our insight into the role of culture-specific factors in the stigmatisation of people with schizophrenia. An in-depth qualitative follow-up study would also help to find out more about the underlying mechanisms of relevant cultural phenomena. It would be of great interest, for example, to find out to what extent notions of shame and honour contribute to those family values that matter most with regard to individuals with schizophrenia, and how this compares to relevant family values in other non-Western cultures, for example in India or China. Reference Yang, Thornicroft, Alvarado, Vega and Link27 Another limitation is that we have not assessed family loyalty, which would have allowed us to study empirically how both cultures differ in this respect and to examine directly how this affects stigma. Although great pains have been taken with the translation of the interview, linguistic equivalence does not necessarily mean cultural equivalence. Because of its correlational design, our path models preclude definite causal inferences between the different stigma components. Finally, for methodological reasons people who were illiterate were excluded from the Tunisian sample. As traditional ways of responding to mental illness may prevail among this group more than among better educated people, differences between both countries may be even more pronounced than those observed in this study.
Main findings
Across all three stigma components studied we found significant differences between both countries: whereas in Germany the stereotype of dangerousness is more common and treatment prognosis is judged less optimistically, in Tunisia more people share the perception that persons with schizophrenia are unpredictable and more people tend to blame the person with the condition for the onset of it and place on them the responsibility for the further course of the disorder. In Tunisia, fewer people react with fear and more people show prosocial reactions, however, as we have seen, the latter does not translate into less rejection, as in Germany, it can even have the opposite effect. And whether the desire for social distance is greater in Germany or Tunisia depends on the type of relationship studied.
There is no yes-or-no answer to the question as to whether the stigma attached to schizophrenia is more pronounced in Germany or Tunisia. It is just different. Whereas acceptance of people with schizophrenia was very high in Tunisia regarding more distant relationships, the opposite was true as regards close, family-related relationships. When it comes to those social roles that ‘matter most’ in Arab culture, people with schizophrenia are facing strong rejection, even stronger rejection than in Central Europe. Thus, although in Tunisia reintegration of patients in the social world outside the family may prove somewhat easier, there is a higher risk of exclusion from family-related roles.






eLetters
No eLetters have been published for this article.