


Exploring neuroendocrine function in patients with post-traumatic stress disorder (PTSD) may give insight into the pathogenesis of this stress-related disorder. One focus in the scientific literature has been on possible disturbances in the hypothalamic–pituitary–adrenal (HPA) axis. During acute stress the HPA axis is activated; the hypothalamus secretes corticotropin-releasing hormone (CRH) under the influence of serotonin from the amygdala. Subsequently, CRH stimulates the pituitary to release adrenocorticotropic hormone (ACTH), which results in the production of glucocorticoids (cortisol) in the adrenal cortex. Cortisol serves to stop many metabolic, neuronal defensive and immune reactions. Consequently energy can be mobilised to cope adequately with the stressor. Studies using psychological stress to stimulate the HPA axis have shown an exaggerated cortisol response in PTSD (for review see Reference de Kloet, Vermetten and Geuzede Kloet et al, 2006). However, under basal conditions PTSD generally – but inconsistently – has been associated with lower levels of cortisol. To elucidate this association we performed a systematic review of studies reporting basal cortisol levels in people with PTSD to investigate whether specific circumstances contribute to these inconsistencies.
METHOD
Identification of studies
Relevant studies were identified by systematic searches of Medline, EMBASE, ScienceDirect and Psychlit for articles published between 1980 and March 2005. A free-text search was performed using the term posttraumatic stress disorder, OR PTSD AND cortisol, OR glucocorticoid. Reference lists of the articles obtained were checked for further relevant articles. We also considered inclusion of unpublished studies offered to us by researchers.
Inclusion criteria
Studies were included when cortisol was measured in adults (aged 18 and above) with current PTSD and in controls with no current Axis I disorder (according to DSM–III, DSM–III–R, or DSM–IV criteria; American Psychiatric Association, 1980, 1987, 1994) or history of PTSD. Cortisol levels had to be determined with a standard biological assay. Furthermore, mean cortisol levels and standard deviations (s.d.) for both groups had to be described or had to be presented by the authors upon request. In the case of multiple papers from a single study, only the results of the publication with the highest number of participants was included.
Exclusion criteria
Studies were excluded when: (a) focusing on a condition other than depression co-morbid with PTSD (e.g. borderline personality disorder, cancer); (b) reporting on lifetime, 12-month diagnosis of PTSD or sub-threshold/partial PTSD; (c) cortisol level was measured within 1 month of trauma; (d) the HPA axis was pharmacologically challenged (e.g. by dexamethasone) before first cortisol measurement; (e) participants were anticipating any kind of social stressor, such as cognitive stress challenge, combat noise or personalised trauma script; (f) reporting in a language other than English. M.M and G.V. independently assessed each retrieved study and disagreements with respect to inclusion were resolved through discussion with M.O.
Data analysis
For each individual study identified, we calculated the standardised mean difference (SMD) in cortisol levels between the PTSD and the control group and its associated variance. Hedges’ adjusted g was used to give a better estimate in cases of smaller sample sizes (Rosenthal et al, 1994). Random-effects models were fitted using inverse variance weighting to obtain pooled estimates of SMD and its corresponding 95% CI.
In all analyses, we used the SMD as our outcome measure to allow pooling across studies that used different types of measurement (i.e. urine, saliva, plasma, or serum) and to reduce the impact of measurement problems related to different sampling conditions.
Our first analysis included the data from all studies to obtain an overall pooled estimate and to examine whether there was heterogeneity in results between studies. Each study was included only once in this overall analysis. If a study reported multiple types and times of measurements, the following hierarchy was used to select one measurement. Plasma samples were preferred above saliva, saliva above urine, and morning measurement above afternoon or evening. We used data from the earliest sample, or when measurements were related to time of awakening we selected the sample 30 min past awakening to be closest to the peak level of cortisol in the morning. For afternoon samples, we included the latest possible sample to compare circadian curves at the nadir of cortisol values. The Q-test was performed to examine whether there was more heterogeneity in the results than could be expected from chance alone. We also calculated the I 2 statistic, which expresses the percentage of total variation that can be attributed to heterogeneity rather than chance. Within this data-set, we also examined whether there were systematic differences between the types of measurement.
We then performed several specific subgroup analyses to examine whether the difference in cortisol levels between PTSD and control groups was influenced by other factors. Successive models were built to examine whether the SMD was significantly different in subgroups defined by a particular factor. The following factors were examined: time of measurement; gender; characteristics of the PTSD group, including type of trauma, years elapsed since trauma, presence or absence of comorbid depression; whether or not the control group was also exposed to trauma; and year of publication. Results of the subgroup analysis are presented as mean SMD together with 95% CI for each level of the factor. In addition, a formal test of interaction (e.g. whether the differences in SMD between the levels of the factor are zero) was performed to avoid overinterpretation of effects found in subgroups (Reference Matthews and AltmanMatthews & Altman, 1996; Reference Altman and BlandAltman & Bland, 2003).
The MIXED procedure in SAS version 9.1 for Windows was used to fit the various random-effects models as described by van Houwelingen et al (Reference van Houwelingen, Arends and Stijnen2002). P-values less than 0.05 were considered statistically significant.
RESULTS
Search and inclusion
Our initial search identified 245 studies, of which 35 met our inclusion criteria (see data supplement to the online version of this paper). However, 6 only met the inclusion criteria when additional information was provided. Furthermore, 2 unpublished studies (Hopwood et al; Kaloupek et al) were identified. In 3 studies we excluded the traumatised control group (Yehuda et al, Reference Yehuda, Boisoneau and Lowy1995a , Reference Yehuda, Halligan and Grossman2002; Reference Stein, Yehuda and KoverolaStein et al, 1997), because several people in these groups had a history of PTSD.
A total of 1628 people were included across all studies, with 828 with PTSD and 800 controls. The median sample size of the studies was 20 for people with PTSD (range 7–75) and 18 for controls (range 7–113).
Study characteristics
Each study included in the meta-analysis and the assessed variables are shown in a data supplement to the online version of this paper. Cortisol was either assessed in plasma/serum (24 studies), saliva (8), or 24 h urinary free cortisol samples (7), or a combination of two types of assessment. In 7 studies, both trauma-exposed and non-exposed controls were used as comparison groups, whereas comparison solely with traumatised or non-traumatised controls was made in 9 and 8 studies respectively. In the remaining 13 studies trauma-exposed and non-exposed individuals were combined or left undefined in the comparison group. Studies reported on the following populations: combat veterans (18 studies), victims of (childhood) sexual or physical abuse (6), refugees (3), and various trauma (8). Two studies did not report information about the types of trauma in their population. Twenty-four studies matched their participants with PTSD and controls for gender and 8 studies matched them for age. Few studies matched their participants for other criteria such as smoking, race or menstrual cycle. Potential confounding factors such as medication usage, exclusion criteria and dietary restrictions varied greatly across studies (see data supplement to online version of this paper).
Overall comparison
Figure 1 shows a forest plot of the SMD of cortisol levels in people with PTSD relative to controls in each of the 37 studies, grouped according to the type of measurement. There was no overall difference in pooled effect size between people with PTSD and controls (SMD=–0.12, 95% CI –0.32 to 0.080, P=0.24). There was significant heterogeneity in results between studies: the P-value for the Q-test for heterogeneity beyond chance was 0.0001 and I 2 was 71% (indicating that 71% of variation across studies can be attributed to heterogeneity rather than chance). In the situation that all studies were measuring the same SMD, only sampling variation would be present and I 2 would be zero (Reference Higgins, Thompson and DeeksHiggins et al, 2003).
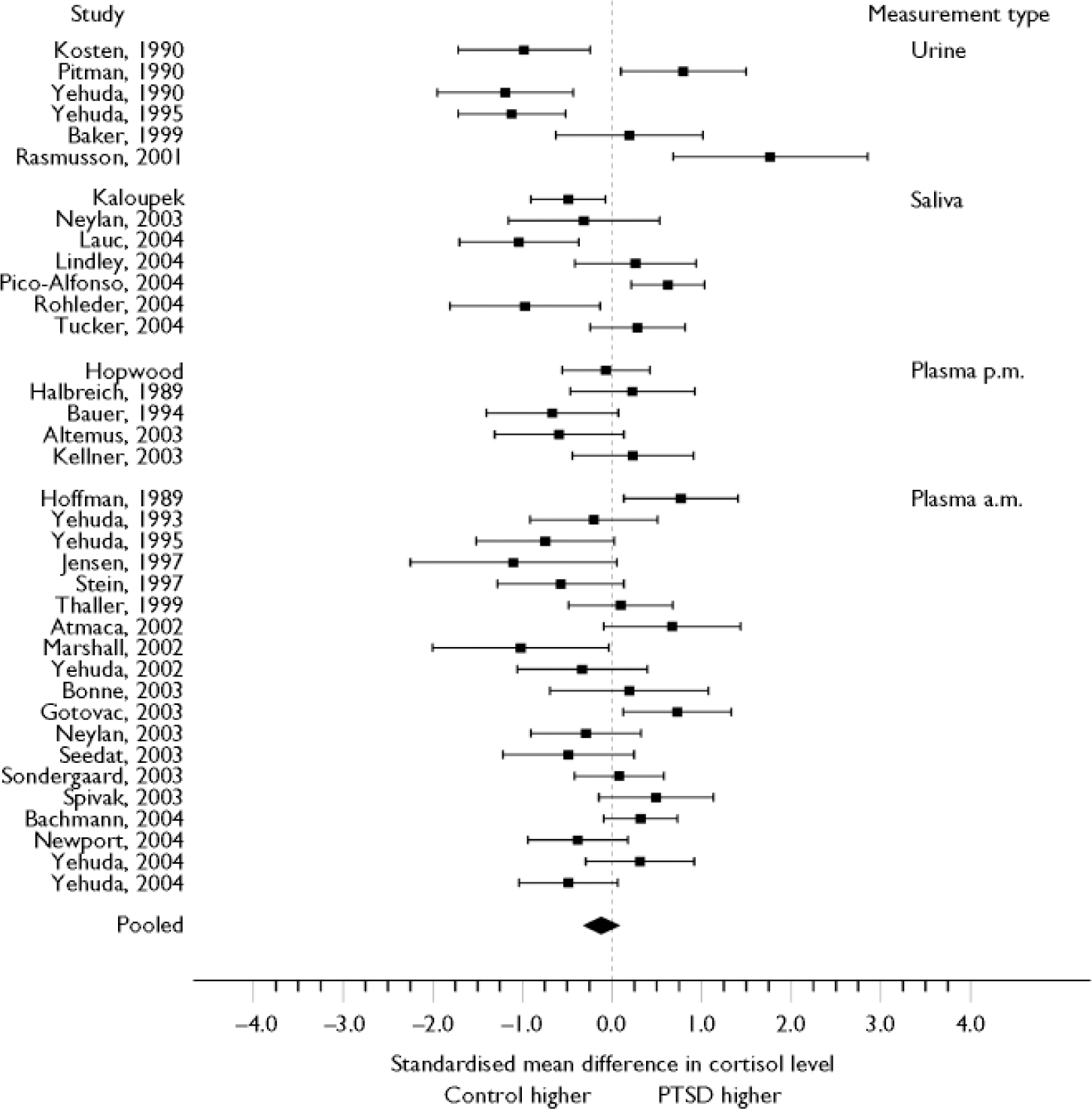
Fig. 1 Standardised mean difference (with 95% CI) of cortisol levels between people with post-traumatic stress disorder (PTSD) and controls (n=37 studies). Studies are grouped according to type of measurement and are identified by first-named author. Pooled estimate based on random-effects model using inverse variance weighting.
Type of assessment
We analysed whether the SMD in cortisol levels between people with PTSD and controls depended on the type of measurement: plasma/serum (24 studies), saliva (7), and 24 h urinary free cortisol (6). None of the measurements revealed differences between patients and controls (plasma/serum, SMD= –0.080, 95% CI –0.32 to 0.17; saliva, SMD=–0.19, 95% CI=–0.63 to 0.26; 24 h urine, SMD=–0.20, 95% CI –0.72 to 0.31).
Subgroup analyses
All the following subgroup analyses were performed with studies measuring cortisol in plasma/serum. The small numbers of studies measuring cortisol in saliva and urine prohibited any meaningful subgroup analysis.
Time of measurement
In this analysis we grouped studies according to whether measurements were taken between 08.00 and 09.00 h or in the afternoon. No differences were found for morning samples (n=15 studies, SMD=–0.0006, 95% CI –0.53 to 0.53, P=0.998), whereas in the afternoon people with PTSD had lower levels of cortisol than controls (n=7 studies, SMD=–0.79, 95% CI –1.58 to–0.003, P=0.049). However, the formal test for interaction did not reach significance, so the observed effect in the afternoon subgroup should be interpreted with caution (Fig. 2).
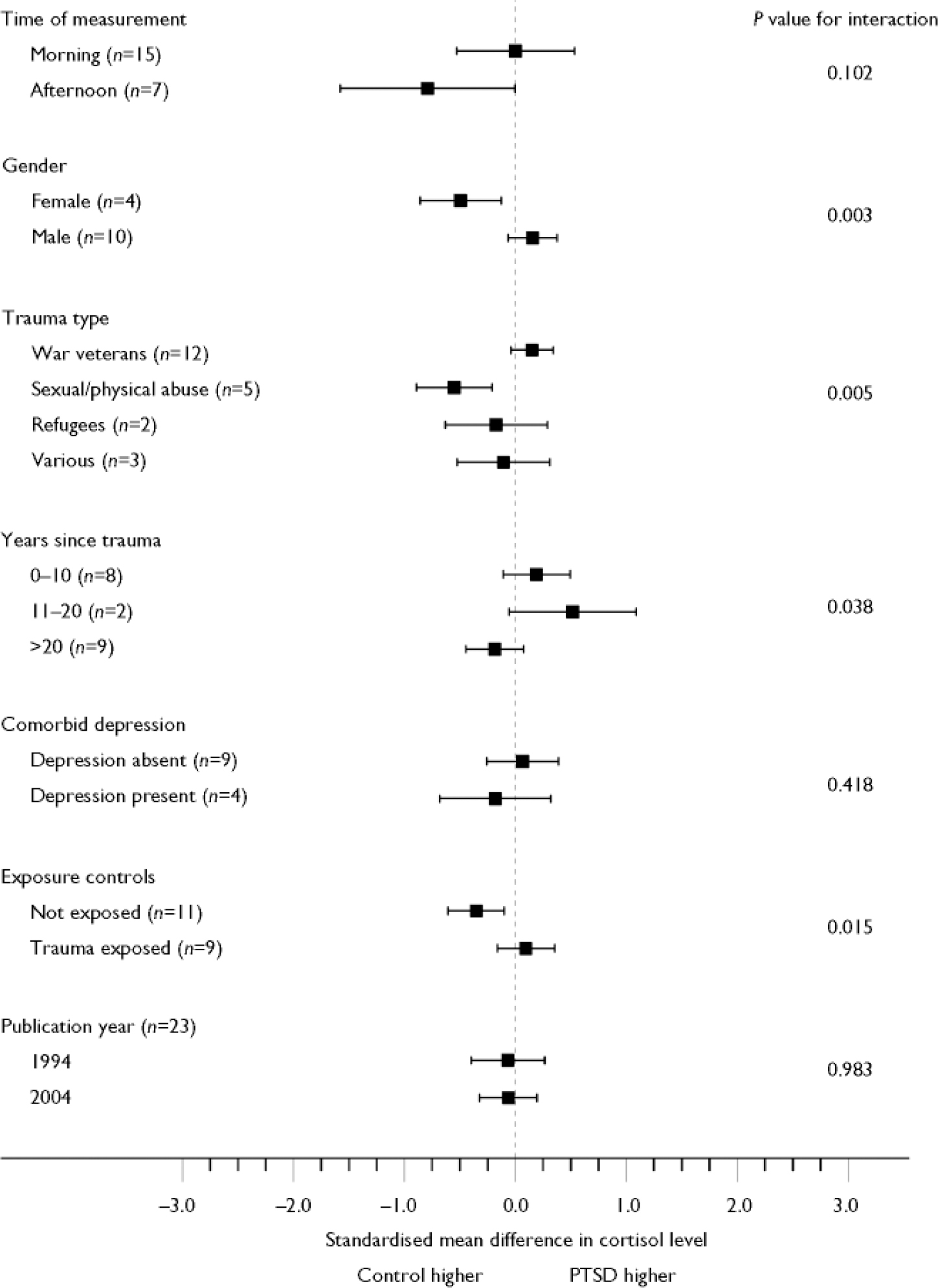
Fig. 2 Influence of variables on plasma/serum cortisol assessments. Standardised mean difference (with 95% CI) of plasma/serum cortisol levels between people with post-traumatic stress disorder (PTSD) and controls.
Gender
The influence of gender on cortisol level was examined in 10 studies which included only males and in 4 studies with only females. Whereas the analyses of cortisol in males with and without PTSD did not reveal any significant differences (SMD= 0.15, 95% CI –0.06 to 0.37, P=0.16), females with PTSD had highly significant lower cortisol levels than their comparison groups (SMD=–0.49, 95% CI –0.86 to –0.13, P=0.009). Because of this large difference in effect, significant interaction between male and female studies was also found.
Type of trauma
Four categories were used to examine whether type of trauma might have influenced the association between PTSD and cortisol: war veterans, victims of sexual or physical abuse, refugees and various trauma (Fig. 2). Subgroup analysis revealed significantly lower cortisol levels in people with PTSD due to sexual or physical abuse than in controls (n=5 studies, SMD=–0.55, 95% CI –0.89 to –0.21, P=0.002). No differences in cortisol level were found between controls and people with PTSD due to other types of trauma (war veterans, n=12 studies, SMD=0.15, 95% CI –0.03 to 0.34, P=0.12; refugees, n=2, SMD= –0.17, 95% CI –0.63 to 0.29, P=0.46; various trauma, n=3, SMD=–0.11, 95% CI –0.52 to 0.31, P=0.61). Analysis also revealed a significant interaction between types of trauma (n=22, F=4.31, d.f.=3, 1000, P=0.005).
Years since trauma
To analyse whether the number of years elapsed since the traumatic event was related to cortisol levels, we constructed three time categories: 0–10 years, 11–20 years and over 20 years. In studies where there were no such data, we approximated this time frame by using the duration of illness. For studies examining people with childhood abuse, we subtracted 12 years from their mean age. For those with war-related trauma we subtracted the year of study publication from the year in which that particular war ended. Among studies with the same time frame for years since trauma no differences were found for cortisol levels of people with PTSD and controls (0–10 years, n=8 studies, SMD=0.19, 95% CI –0.11 to 0.49, P=0.21; 11–20 years, n=2, SMD=0.52, 95% CI –0.058 to 1.09, P=0.078; >20 years, n=9, SMD=–0.19, 95% CI –0.44 to 0.071, P=0.16).
Exposure to trauma of control groups
To differentiate between exposure to trauma and exposure with subsequent development of PTSD, we analysed studies which indicated whether controls had previous exposure to trauma. In 17 studies we calculated effect sizes for PTSD compared with trauma-exposed controls and non-exposed controls separately. Lower cortisol levels were found for people with PTSD compared with non-exposed controls (n=11 studies, SMD=–0.35, 95% CI –0.61 to–0.098, P=0.007). No differences were found between people with PTSD and trauma-exposed controls (n=9, SMD=0.096, 95% CI –0.16 to 0.35, P=0.46). The test of interaction was also significant (n=20, F=5.93, d.f.=1, 1000, P=0.015).
Comorbid depression
The effect of comorbid depression in people with PTSD on cortisol level was analysed in 13 studies that reported whether depression was present or absent within their PTSD group. If a single study used two subgroups with PTSD, with and without comorbid depression, we included both comparisons in the analysis (2 studies). The results (see Fig. 2) showed that depression had no influence on the effect sizes.
Year of publication
Year of publication was examined to evaluate whether improved methodology might strengthen possible contrasts between groups. Using all published studies, year of publication was linearly modelled to estimate the change in SMD per year. Figure 2 shows the effect on SMD over a 10-year period (1994–2004). Results could not confirm this hypothesis.
DISCUSSION
Main findings
In this systematic review we included 37 studies examining basal cortisol levels in adults with current PTSD in comparison with adults without psychiatric disorders published between 1980 and March 2005. Combining all available data for meta-analysis we found no systematic difference in basal cortisol levels between people with PTSD and controls. However, results were highly heterogeneous, indicating that differences between subgroups might be present. Subsequent explanatory subgroup analyses revealed that studies assessing plasma or serum reported significantly lower cortisol levels in people with PTSD compared with controls when compared with controls with no previous exposure to trauma. Lower cortisol levels were also found in people with PTSD compared with controls in studies including only females, in studies on physical or sexual abuse and in afternoon samples. Although the general assumption is that cortisol levels are low in PTSD, we could not confirm this hypothesis even though we used homogeneous groups as a result of strict exclusion criteria. This study shows that low cortisol levels do not relate to PTSD in general, but rather seem to mirror trauma exposure and PTSD subgroups.
Type of assessment
The type of assessment (i.e. serum/plasma, saliva or 24 h urinary cortisol) did not account for the heterogeneity between the individual studies, and within studies using the same method of assessment, cortisol was not significantly different in people with PTSD compared with controls. It is important to stress the differences in the fluids used for cortisol measurement because of the varying compositions of cortisol in these fluids. Whereas salivary cortisol consists completely of the free (bioactive) fraction, in plasma less than 10% of cortisol is free. The majority is bound to cortisol-binding globulin (CBG) or other proteins and is biologically inactive. Changes in binding proteins can alter measured serum/plasma cortisol concentrations without influencing free concentrations (Reference Hamrahian, Oseni and ArafahHamrahian et al, 2004). Several conditions (e.g. pregnancy, hypothyroidism, marked adipositas) and oral contraceptive use are known to influence CBG levels (Reference Westermann, Demir and HerbstWestermann et al, 2004). However, only a few studies took this into account and excluded or matched on these features. Nevertheless, despite possible abnormal CBG levels in studies using plasma/serum measurements, differences in study results did not depend on body fluid used for cortisol assessment.
Time of assessment
Since cortisol has a circadian rhythm, with low values at awakening, followed by peak values 30 min after awakening and a steady decline during the rest of the day, time of assessment is expected to be an important factor in its measurement. Our findings revealed that during the afternoon, people with PTSD had significantly lower cortisol levels than controls. No such differences were found during the early morning. Since PTSD is known to be associated with difficulties in sleeping, and measures depended on fixed times, it is uncertain whether variability in awakening time between PTSD and controls influenced morning cortisol levels. Since cortisol secretion is relatively stable during the afternoon actual differences can be detected more easily.
Trauma-exposed v. non-exposed control groups
Some of the disparity in study results can be explained by whether studies used trauma-exposed or non-exposed controls. We found significantly lower plasma/serum cortisol levels in people with PTSD compared with controls not exposed to trauma but no such difference when comparisons were made with trauma-exposed controls. This suggests that differences in cortisol levels relate to being exposed to trauma generally rather than to PTSD.
Gender
In general, women appear to have a more sensitised HPA axis with lower overall plasma cortisol than men (Reference Van Cauter, Leproult and KupferVan Cauter et al, 1996), and our findings indicated that females with PTSD showed lower levels of basal cortisol than female controls. No such difference was apparent between males. This may explain why women are more vulnerable than men to the development of post-trauma symptoms and take longer to recover from them. In addition, the higher risk of PTSD in women may be due, at least in part, to the types of traumas they experience (more interpersonal violence, particularly of a sexual nature), to higher peri-traumatic dissociation in women, or to women's use of avoidant coping strategies (Reference Olff, Langeland and DraijerOlff et al, 2007). Gender-specific PTSD subgroups may exist – in particular arousal-related and dissociation-related variants – with distinct neuropsychological profiles and attendant symptoms. Hence, gender-specific psychobiological reactions to trauma may contribute to the higher risk for PTSD.
Physical or sexual abuse and years since trauma
Only people with PTSD due to physical or sexual abuse had lower cortisol levels than controls. This type of trauma is generally chronic and often starts in early development. An upbringing that is associated with adversity can produce detrimental effects on health (Reference Fish, Shahrokh and BagotFish et al, 2004) and it is likely that within a critical phase during development, functioning of the HPA axis alters. Years elapsed since trauma had no pronounced influence on cortisol levels of people with PTSD. The time of onset of PTSD in development and the ongoing traumatising character of abuse might be more crucial in distinguishing abuse-related PTSD from other types of trauma. It should be noted that for statistical analyses we could not disentangle female gender from victims of abuse because of overlap in studies. Therefore, we could not examine whether low cortisol levels found in women with PTSD are due to gender or type of trauma preceding PTSD, or an interaction of both.
Comorbid depression
Comorbid depression in people with PTSD had no influence on the association between PTSD and cortisol level. Although there seems to be consensus that people with depression demonstrate high cortisol levels (Reference HolsboerHolsboer, 2001), generally this hyperactivation of the HPA axis is typically found in severe depression not specifically due to traumatic stress. In accordance with our findings, PTSD and comorbid PTSD/depression following traumatic injury were indistinguishable and reflected a shared vulnerability with a range of similar predictive non-biological variables. Comorbid PTSD/depression and PTSD alone may reflect one and the same construct (Reference O'Donnell, Creamer and PattisonO'Donnell et al, 2004), as appears to be confirmed by similar cortisol values within the present study.
Year of publication/sensitivity of assays
We also examined whether year of publication affected the relationship between PTSD and cortisol. This variable was included in our subgroup analysis to serve as a proxy for changes in protocol or the use of more sensitive assays during the study period. Year of publication had no impact on the results and therefore did not explain any of the heterogeneity in results across studies.
Limitations and future research
We acknowledge several limitations of our meta-analyses. First, despite our efforts to include unpublished studies, publication bias might still have obscured our results, as studies which find significant differences are more likely to be published. Second, we performed several subgroup analyses based on characteristics of the PTSD or control group and used these as study-level covariates in our model. Owing to incomplete reporting, we could not use all studies in the subgroup analyses. In some cases, only a few studies were available within a specific stratum, which caused problems related to chance findings and lack of power. Subgroup analyses within systematic reviews have to be interpreted with care because by nature they are post hoc analyses. They can provide additional insight but have to be confirmed in well-designed prospective studies with sufficient power to examine differences in effect by subgroups. Furthermore, individual appraisal and coping mechanisms are crucial in determining levels of stress hormones such as cortisol (Olff et al, Reference Olff, Langeland and Gersons2005a ,Reference Olff, Langeland and Gersons b ), factors that have not been systematically assessed in most of the literature. Finally, substantial differences in the methodology of studies hampered comparison. For instance, restrictions regarding smoking, alcohol, drugs and medication usage varied widely across studies. Although we attempted to pool data of studies on important characteristics, these restrictions and comorbid conditions known to confound cortisol levels remained unattended.
In future studies consensus in data collection and sampling protocol of basal diurnal cortisol would facilitate comparison of data across studies. Given that saliva samples can be obtained by study participants themselves in their own environment and related to time of awakening and that salivary cortisol consists completely of the bioactive fraction, future studies could overcome several difficulties by sampling salivary cortisol.
In summary, across 37 studies people with PTSD and healthy controls did not differ in cortisol levels. Nevertheless, support was found for low cortisol levels dependent on the type of control group and specific subpopulations. Significantly lower cortisol levels were found in people with PTSD when compared with non-exposed controls, whereas no such differences were found when compared with trauma-exposed controls without PTSD. Subgroup analyses further revealed lower cortisol in people who seem to be at the greatest risk for developing PTSD, i.e. women and physically or sexually abused victims. The lower cortisol values in PTSD found in the afternoon endorse the need to choose the time of measurement carefully. It is important to note that numerous factors – which are frequently overlooked – may have a confounding influence on cortisol levels. Therefore, disentangling the relationship between PTSD and cortisol is more complex than it first appears.





eLetters
No eLetters have been published for this article.