



Childhood adversity, stressful life events and trauma have been repeatedly established as risk factors for psychopathology, and adversity has been estimated to be responsible for as much as 32% of the risk of psychopathology in adolescents.Reference Green, McLaughlin, Berglund, Gruber, Sampson and Zaslavsky1 This link has been established throughout the lifespan for different kinds of adversity and psychopathology.Reference Kessler, Davis and Kendler2 Childhood adversity may have stronger associations with psychopathology if repeated or cumulative.Reference Costello, Erkanli, Fairbank and Angold3 As many as one in four children may have suffered at least one severe incidence of childhood adversity in their lifetime.Reference Green, McLaughlin, Berglund, Gruber, Sampson and Zaslavsky1,Reference Costello, Erkanli, Fairbank and Angold3 Partial explanations of why some people go on to develop psychopathology and some do not despite similar or even identical risk profiles have been proposed, in terms of underlying genetic differences, neurobiological changes and family processes, as well as sensitisation to future adversity.Reference Caspi, Sugden, Moffitt, Taylor, Craig and Harrington4–Reference Amstadter, Myers and Kendler6 There is, however, a particular need for research into mechanisms that may be altered through intervention.Reference Socioemotional7 Mediation analysis is particularly useful for establishing the nature of these mechanisms, as mediators can explain the relationship between adversity and psychopathology rather than merely influencing that relationship or having a relationship with either adversity or psychopathology. Existing research has proposed some plausible candidates for such interventions, including family- and child-based mediators.Reference Grant, Compas, Thurm, McMahon, Gipson and Campbell5 Research including multiple kinds of mediator can more clearly identify which factors are responsible for more of the relationship, allowing for more effective interventions.Reference Grant, Compas, Thurm, McMahon, Gipson and Campbell5 Newer statistical methods, such as that developed by Karlson, Holm and Breen, allow comparison of coefficients between these mediators in a logistical regression model.Reference Kohler, Karlson and Holm8 This study aims to investigate a range of plausible candidate mediators of the relationship between childhood adversity and adolescent psychopathology, with a view to identifying candidates for intervention. We hypothesised that there are both child- and family-based mediators of the relationship between childhood adversity and psychopathology in adolescence. Our aim was to determine whether poor self-concept, lack of engagement with hobby participation and poor relationship with parents mediated the relationship between childhood adversity and internalising and externalising problems in childhood and adolescence.
Method
Participants
The study population comprised the child cohort of the Growing Up in Ireland study. This is a national longitudinal study of children and youth in Ireland.Reference Murray, McCrory, Thornton, Williams, Quail and Swords9,Reference Thornton, Williams, McCrory, Murray and Quail10 The child cohort was recruited at age 9 and comprises 8658 children and their families. Participants were recruited from 910 primary schools (82% of those invited to participate), selected to accurately represent the school population of Ireland as a whole, with respect to location, disadvantage of pupils, gender mix, denominational status and number of 9-year-old pupils.Reference Murray, McCrory, Thornton, Williams, Quail and Swords9 A maximum of 40 students were recruited from each school, to minimise burden on school staff and to prevent larger schools from biasing the sample.Reference Murray, McCrory, Thornton, Williams, Quail and Swords9 Multiple rounds of information and consent forms were given to families to minimise refusal. Between August 2007 and May 2008, 50% of the 17 054 invited families consented to participate and provided useable data. A follow-up study (wave two) was carried out at age 13 and 7423 (87.7%) were interviewed between August 2011 and March 2012. Interviews and questionnaires were undertaken with children, primary caregivers and teachers at both ages 9 and 13, (waves one and two). To account for the demographic differences between the baseline and follow-up caused by differential attrition, the data were ‘reweighted’ with respect to differential response characteristics,Reference Thornton, Williams, McCrory, Murray and Quail10 which gives rise to the reweighted sample size of 7505 participants.
Ethics and consent
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The quantitate aspects of the child cohort of Growing Up in Ireland study was granted ethical approval from the research ethics committee of the Health Research Board. Written consent was obtained from all participants and their parents/guardians in the Growing Up in Ireland study. Participants are not identifiable from the anonymised microdata file.
Exposures
Childhood adversity
At age 9, the primary caregiver was asked about stressful life events to which the child might have been exposed (see Supplementary Table 1 available at https://doi.org/10.1192/bjp.2019.108). These were death of a parent, death of a close family member, death of a close friend, parent in prison, drug taking/alcoholism in the immediate family, mental disorder in the immediate family, a stay in foster home/residential care, serious illness/injury, serious illness/injury of a family member, divorce/separation of parents, conflict between parents, moving house, moving country and other disturbing event/unspecified.
This questionnaire does not include any items on sexual or physical abuse. The questionnaire includes both severe (e.g. ‘death of a parent’) and mild events (e.g. ‘moving house’). Determining the subjective effect of each of these events is not possible from this questionnaire. For this paper we defined childhood adversity as experiencing three or more events, or at least one of the seven most stressful life events, which we defined a priori as death of a parent, death of a close friend, parent in prison, drug taking/alcoholism in the immediate family, mental disorder in the immediate family, serious illness/injury and a stay in foster home/residential care.
Outcomes
Adolescent and persistent psychopathology
The Strengths and Difficulties Questionnaire (SDQ)Reference Goodman11 was administered to primary caregivers at ages 9 and 13. Sum scores for internalising and externalising problems were used separately, with a predefined threshold for each scale, in line with the definition of the measure (a score above seven for internalising and above nine items endorsed for externalising).
Internalising and externalising problems were examined separately in the interest of identifying mediators that might support one or the other, in the context of mixed evidence for specificity of childhood adversity leading to kinds of psychopathology.Reference McMahon, Grant, Compas, Thurm and Ey12
A persistence measure was included in the analysis, using the SDQ internalising and externalising scores from both time-points. Persistent internalising or externalising problems were defined as scoring above the threshold at both time-points (i.e. ages 9 and 13).
Mediators
Mediators were chosen in an attempt to cover both internal and external child factors (thoughts about themselves as well as behaviours) and family factors. Mediators were measured at age 9, to best identify those to be targeted in interventions.
Self-concept
Our candidate ‘internal child factor’ was measured with the 60-item Piers-Harris 2 scaleReference Piers and Herzberg13 at age 9. This is a 6-item self-report questionnaire designed for use with children aged 7–18 years. It includes domain subscales with items on behavioural adjustment (e.g. ‘I am well behaved in school’), intellectual and school status (e.g. ‘I am good in my schoolwork’), physical appearance and attributes, freedom from anxiety (e.g. ‘I am often afraid’), popularity (‘I have many friends’) and happiness and satisfaction (e.g. ‘I like being the way I am’). The total score (the sum of these subscales) was used in the analysis, reverse-scored and standardised via z-score, so as to be directly comparable with the other variables in the path decomposition.
Parent–child relationship
Parent–child relationship was measured by primary caregiver report with the Pianta Child–Parent Relationship ScaleReference Pianta14 at age 9. The two longer subscales with items about conflict (e.g. ‘My child and I always seem to be struggling with each other’) or positive items (e.g. ‘I share an affectionate, warm relationship with my child’) were used as measures of positive and negative aspects of the relationship. The positive subscale was reverse-scored and both were standardised via z-score, so as to be directly comparable with other variables in the path decomposition.
Hobby participation
Our candidate ‘external child factor’ was measured as a category variable of participation in either sports or ‘cultural activities’ at age 9.
Confounds
Gender and handedness were both included as confounds, as they have previously been associated with differences in the development of psychopathology.Reference Leadbeater, Kuperminc, Blatt and Hertzog15,Reference van der Hoorn, Oldehinkel, Ormel, Bruggeman, Uiterwaal and Burger16 Nationality was also included, measured by proxy as whether or not the child was born in Ireland, as immigration from some countries or in some circumstances may be associated with increased risk of psychopathology.Reference Selten, Veen, Feller, Blom, Schols and Camoenie17 Socioeconomic status was also included as a confound, measured both as the highest level of education achieved by the primary caregiver and as the family's income quintile.
Childhood psychopathology, as measured by the parent-reported SDQ at age 9, was included as a confound as it is likely to be a predictor of psychopathology at age 13 and may relate to both childhood adversity and mediators.
Statistical analyses
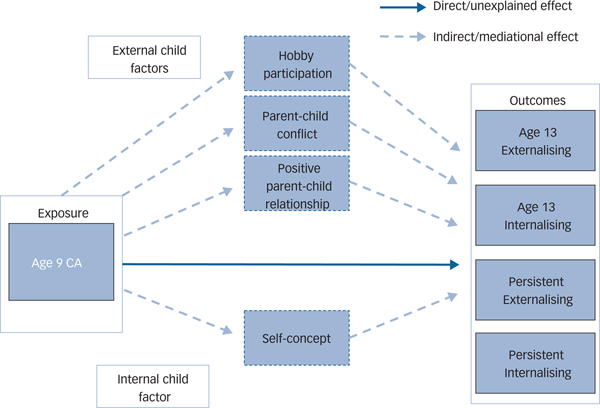
Logistic regression was used to examine the demographic differences between children with and without childhood adversity (Table 1). Mediation analysis was undertaken in line with Baron and Kenny's recommendations,Reference Baron and Kenny18 proposing the model shown in Fig. 1. Logistic regression was used to investigate whether childhood adversity (and confounds) predicted externalising and internalising behaviours at age 13 and persistence of psychopathology between ages 9 and 13 (Table 2). Second, linear regression was used to investigate whether childhood adversity predicted mediators (with the exception of hobby participation, the only categorical mediator, for which logistic regression was used). Third, non-significantly related mediators were then excluded, and logistic regression was used to investigate the association between mediators and psychopathology (Table 3).
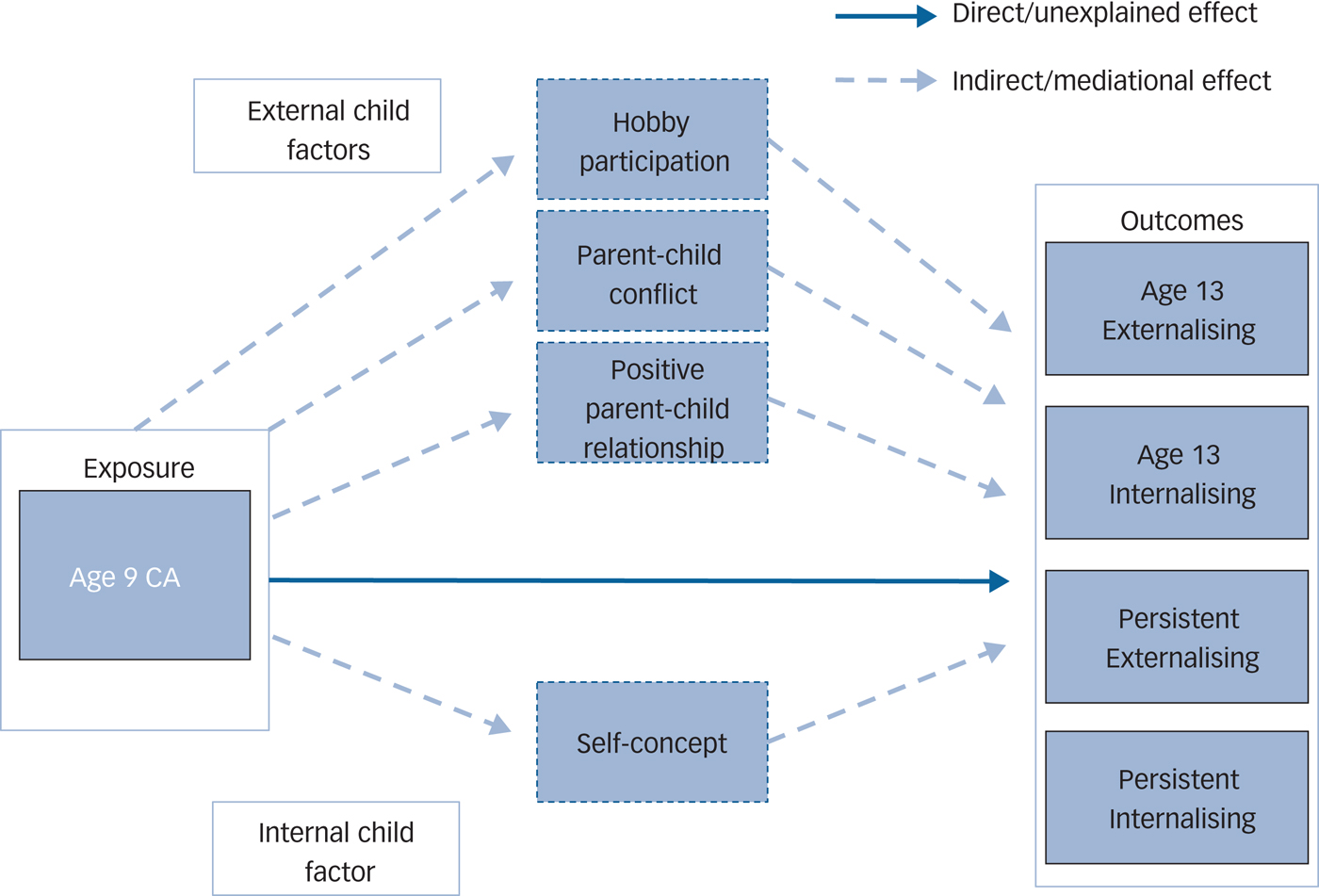
Fig. 1 Proposed models of the relationship between childhood adversity and psychopathology, with the total effects transmitting both directly and indirectly via proposed mediators: parent–child conflict and positive relationship, self-concept and hobby participation. Each mediator was investigated separately and multivariate path-decomposition was only conducted on variables that significantly mediated the relationship between childhood adversity and psychopathology.
Table 1 Demographic characteristic of participants who report childhood adversity and those who do not

a. Emboldened statistics are significant at the P < 0.05 level.
Table 2 The association between mediators and both childhood adversity and adolescent psychopathology
OR, odds ratio; CI, confidence interval.
a. Emboldened statistics are significant at the P < 0.05 level.
b. The relationship between CA and hobby participation was investigated using logistic regression. The relationship between CA and the other mediators variables was investigated using linear regression. The relationship between the mediators and the outcome variables were investigated using logistic regression.
c. Adjustment 1: Gender, Nationality, Maternal Education, Income Quintile,
d. Adjustment 2: Gender, Nationality, Maternal Education, Income Quintile, Age 9 Psychopathology.
e. Number of observations used in each analysis varies due to missing data. To account for this the data was re-analysed using multiple imputations. Minimal differences were found between the observed and imputed results (see Supplementary File 2).
Table 3 Pathway decomposition for mediators in the relationship between childhood adversity and psychopathologya

OR, Odds ratio; CI, confidence interval.
a. Emboldened statistics are significant at the P < 0.05 level.
b. Adjustment 1: Gender, Nationality, Maternal Education, Income Quintile, Age 9 Psychopathology.
c. Adjustment 2: Gender, Nationality, Maternal Education, Income Quintile.
d. Indirect relationship is the part of the relationship accounted for by the mediator, direct relationship is the part of the relationship which is not.
e. Number of observations in each analysis vary due to missing data. To account for this the data was re-analysed using multiple imputations. Minimal differences were found between the observed and imputed results (see Supplementary File 2).
The Karlson, Holm and Breen method,Reference Kohler, Karlson and Holm8 which allows comparison of estimated coefficients of two nested non-linear probability models, was used in Stata (version SE 15.1) for Windows to decompose the effects of the mediators in this logistic regression model (Table 3). The decomposed pathways are visually displayed in Fig. 1. Finally, a small proportion of participant were missing data on some variables, primarily income quintile (7.0%) and self-concept (6.7%). To ensure that this did not bias the results, we re-ran all analysis, using multiple imputation with five imputed data-sets (see Supplementary File 2). A comparison of the coefficients estimated from the observed findings and the imputed finding are reported in Supplementary File 2.
Data availability
Authors had access to the anonymised microdata file data in the Growing Up in Ireland study. This is ongoing for some of the authors who are undertaking continued work with this data-set. This data can be accessed through the Irish Social Science Data Archive.
Results
Prevalence and demographics of childhood adversity
A total of 28.2% (2114) of the participants met the definition for childhood adversity at age 9. These comprised both the 17.6% (1323) of participants who reported at least one severe life event and the 15.5% (1160) who reported three or more less severe life events. The prevalence of each stressful event is reported in Supplementary Table 1. The demographics of those who did and did not report these are shown in Table 1. Children who experienced childhood adversity were more likely to be female; born outside of Ireland; had primary caregivers who were educated at either only primary school, non-degree or postgraduate levels; or were in the lowest two income quintiles. They were also more likely to have met the cut-off for both externalising and internalising problems at age 9.
Childhood adversity and psychopathology
A total of 8.2% of the participants met the definition for externalising problems at age 13, and 39.5% of these participants reported childhood adversity at age 9. Childhood adversity at age 9 significantly predicted externalising problems at age 13 (odds ratio, 1.56; 95% CI 1.28–1.91).
For internalising problems, 8.7% of the participants met the definition at age 13, and 44.7% of these participants reported childhood adversity at age 9. Childhood adversity at age 9 significantly predicted internalising problems at age 13 (odds ratio, 1.83; 95% CI 1.52–2.21).
Similarly, 4.1% of the participants met the definition for persistent externalising problems. Of these participants, 39.8% reported childhood adversity. Age 9 childhood adversity was significantly associated with persistent externalising problems (odds ratio, 1.81; 95% CI 1.41–2.31).
A total of 4.0% of the participants met the cut-off for persistent internalising problems, and 55.3% of these participants reported childhood adversity. Age 9 childhood adversity was significantly associated with persistent internalising problems (odds ratio, 3.12; 95% CI 2.45–3.99).
Mediation analysis
Childhood adversity was positively associated with age 9 poor self-concept and parent–child conflict, and negatively associated with hobby participation (Tables 2 and 3). Childhood adversity was not associated with positive parent–child relationship. All mediators were associated with all psychopathology outcomes except positive parent–child relationship, which was not associated with age 13 externalising or internalising problems (see Table 2).
Path decomposition demonstrated that both parent–child conflict and self-concept explained a significant percentage of the relationship between childhood adversity and age 13 psychopathology and persistent psychopathology (Table 3). For example, parent–child conflict mediated over half of the relationship between childhood adversity and persistent externalising problems (indirect odds ratio, 1.30; 95% CI 1.19–1.43). The direct relationship remained significant in all of the path decompositions, with the exception of the mediation analysis for parent–child conflict with the age 13 and persistent externalising paths (Table 3).
Multivariate path-decomposition demonstrated that only parent–child conflict significantly mediated the relationship between childhood adversity and age 13 externalising problems (self-concept: odds ratio, 1.02; 95% CI 0.99–1.04; 4.2%; parent–child conflict: odds ratio, 1.10; 95% CI 1.05–1.15; 22.0%). Both self-concept and parent–child conflict mediated the relationship between childhood adversity and persistent externalising problems (self-concept: odds ratio, 1.03; 95% CI 1.00–1.06; 5.7%; parent–child conflict: odds ratio, 1.27; 95% CI 1.18–1.36; 45.6%) and persistent internalising problems (self-concept: odds ratio, 1.02; 95% CI 0.99–1.04; 2.6%; parent–child conflict: odds ratio, 1.21; 95% CI 1.14–1.29; 19.1%), with parent–child conflict accounting for a higher percentage of these relationships. In the multivariate path-decomposition, the direct pathway only remained significant for persistent internalising problems (odds ratio, 2.21; 95% CI 1.48–3.32).
Discussion
From this large, longitudinal, nationally representative sample, we found that parent–child conflict and, to a lesser extent, self-concept mediates the relationship between childhood adversity and psychopathology reported at age 13 and persistent psychopathology from age 9 to 13.
Parent–child conflict has previously been found to mediate the relationship between family-related negative life events and adolescent problem behaviours.Reference Dmitrieva, Chen, Greenberger and Gil-Rivas19 There is also strong evidence that parent–child conflict predicts a range of subsequent kinds of psychopathology.Reference Burt, Krueger, McGue and Iacono20,Reference Mamorstein and Iacono21 This is particularly important in the context of evidence showing bidirectional relationships between parent–child conflict and externalising behaviours over time.Reference Burt, McGue, Krueger and Iacono22 Additionally, parent–child conflict has been found to mediate the relationship between externalising and internalising problems in late childhood and early adolescence.Reference Yong, Fleming, McCarty and Catalano23 These findings suggest that childhood adversity can lead to a ‘downward spiral’ of increased risk for subsequent psychopathology, including conduct disorder in adolescence and depression in adulthood because of changes in the parent–child relationship.Reference Burt, McGue, Krueger and Iacono22,Reference Yong, Fleming, McCarty and Catalano23
The salient aspects of parent–child conflict to this relationship bear further investigation. Causes of parent–child conflict may include parent factors that, in some cases, are included in our childhood adversity measure (e.g. interparental conflict, parental mental illness and alcohol or drug use) and some that are not (e.g. genetic influences) as well as child factors, especially temperament.Reference Burt, Krueger, McGue and Iacono20,Reference Mamorstein and Iacono21,Reference Bradford, Vaughn and Barber24,Reference Scaramella and Leve25 It may be necessary to account for the various contributors to parent–child conflict in any attempt to design interventions in this pathway, and some of these contributors may themselves make targets for effective interventions.
Population-level interventions in parent–child conflict are a difficult proposition. Although intervention in situations of abuse and neglect is widely accepted as necessary, identifying those in need of intervention and designing effective interventions has its own challenges.Reference MacMillan, Wathen, Barlow, Fergusson, Leventhal and Taussig26 Within the realm of parenting style or quality, interference in families may be politically unpopular and requires significant cross-spectrum support.Reference Sanders and Prinz27 There have, however, been examples of success in home-visit interventions to reduce child abuse and neglect.Reference MacMillan, Wathen, Barlow, Fergusson, Leventhal and Taussig26 Targeted interventions providing parenting education and training have been shown to be effective in reducing children's antisocial behaviour, and this could be a plausible type of intervention to reduce parent–child conflict.Reference Scott, Spender, Doolan, Jacobs and Aspland28
Of note, positive parent–child relationship was not significantly associated with childhood adversity in this sample, but was protective against persistent psychopathology in the logistic regression analysis. This suggests that although there does not appear to be an increase in positive parent–child relationship after childhood adversity to compensate for its negative effects in this pathway, it might still have a role to play in reducing the rates of persistent psychopathology.
Contrary to our hypothesis, only one of our child-based factors accounted for a significant part of the relationship between childhood adversity and psychopathology. Organised hobby participation has been previously found to be related to psychopathology in adolescence, and this relationship was shown in our results.Reference Bohnert and Garber29 It does not, however, appear to have a protective role against psychopathology after adversity. Further research including a more in-depth investigation of free-time behaviours might find other external child-based factors that could mediate this pathway.
Self-concept significantly mediated a small proportions of the relationship between childhood adversity and psychopathology. Previous research has shown self-efficacy to be a mediator between childhood adversity and depressive symptoms in adults.Reference Maciejewski, Prigerson and Mazure30 Self-concept may be a promising focus or intervention, particularly in older adolescents, when the role of family relationships may be less significant. Moreover, targeting specific aspects of self-concept (such as self-efficacy) or self-concept in a given domain may be related to this pathway whereas other aspects of self-concept might not.
Strengths and limitations
The size and representative nature of the sample used and the validity of the outcome measures used strengthen the conclusions that can be drawn from the study and the applicability of the findings to the general population. Each analysis included confounds, and the findings were both robust to this and similar across both time-points.
The measure of childhood adversity in this study did not include measures of sexual or physical abuse or neglect, but that does not mean that they exercised no effect on the results. Both severe and moderate stressful events appear to cluster in time, and both may disproportionately affect children with other vulnerabilities.Reference Costello, Erkanli, Fairbank and Angold3 For this reason, our measure of childhood adversity may mask a stronger underlying relationship. Additionally, the increased risk of subsequent stressful life events after the first event, compounded by the fact that psychopathology at age 9 may increase risk of subsequent stressful life events before age 13, means that there is no certainty that this effect is solely due to stressful life events experienced before age 9.Reference Costello, Erkanli, Fairbank and Angold3,Reference Kim, Conger, Elder and Lorenz31
The measure of hobby participation is also not independent of service provision and available facilities for children in schools, and therefore may act as a proxy for deprivation or cuts to services for children. All analyses controlled for the influence of income bracket, and hence real effects of hobby participation may not be visible in this study.
This study was reliant on parent-reported measures, despite some evidence that child-reported measures of psychopathology may differ from parents’, particularly in adolescence.Reference Van Roy, Groholt, Heyerdahl and Clench-Aas32 This may result in some level of underestimation of both externalising and internalising problems, or perhaps varied underestimation depending on family structure.Reference Van Roy, Groholt, Heyerdahl and Clench-Aas32 Finally, we have combined a range of stressful events into a ‘childhood adversity’ measure. It is possible that the heterogeneity in events reduces the generalisability of the findings. For example, the relationship between different stressful events and psychopathology may be mediated by different variables. However, conducting a series of specific stressor investigations would likely produce a number of false positive observations and would not speak to childhood adversity, but rather the stressor-specific association with psychopathology. Further research would be required to investigate if the association between specific stressors and psychopathology are differentially mediated.
In conclusion, we found that the association between childhood adversity and both adolescent psychopathology and persistent psychopathology is mediated by parent–child conflict. This suggests that parent–child relationship quality is a key target for interventions in childhood to reduce the incidence of psychopathology in adolescents.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjp.2019.108
Funding
The Growing Up in Ireland study receives funding from the Department of Children and Youth Affairs (DCYA), and is overseen by the DCYA in association with the Central Statistics Office. This research was funded by the Health Research Board of Ireland through a summer studentship to N.D. and by a European Research Council consolidator grant to M. Cannon (grant 724809 iHEAR).
Acknowledgements
We would like to thank the families who took part in the Growing Up in Ireland study, as well as the researchers and study personnel for of their hard work.






eLetters
No eLetters have been published for this article.