


Recent mental health policy in England has mandated the provision of assertive outreach teams (Department of Health, 1999) as an adjunct to services provided by community mental health teams (Reference Johnson, Zinkler and PriebeJohnson son et al, 2001). The required characteristics of assertive outreach teams (Department of Health, 2001) are based on the assertive community treatment (ACT) model developed in the USA, where it has demonstrated reduced hospital bed use (Reference Stein and TestStein & Test, 1980). Studies in the UK have not replicated these findings (Reference Thornicroft, Wykes and HollowayThornicroft et al, 1998; Reference Burns, Creed and FahyBurns et al, 1999). Critics have queried the fidelity of the UK teams to the ACT model (Reference Marshall, Bond and SteinMarshall et al, 1999). It is unknown how far UK assertive outreach teams show low fidelity and whether this represents an essential adaptation to a non-US service environment. The current study explores the service characteristics of assertive outreach teams in London, their ACT model fidelity and whether specific ‘types’ of team could be identified.
METHOD
This paper reports results from the first module of the three-module Pan-London Assertive Outreach Study. It seeks to answer three questions: what are the characteristics of the assertive outreach teams across London; with regard to components of care, do the teams cluster into particular groups with shared characteristics, differing from other groups; and do such clusters correlate with independent scales of fidelity for the ACT model?
All existing teams in London that designated themselves as ‘assertive outreach’, ‘assertive community treatment’ or ‘intensive case management’ were screened to see whether they met the basic inclusion criteria, which included: having a patient: staff ratio of 15: 1 or less; having staff from more than one mental health profession; and providing long-term care, mainly in the community, for people with severe and enduring mental illness. Teams with assertive outreach posts integrated into community mental health teams or with a specialised clinical focus (e.g. homeless individuals, forensic patients, etc.) were excluded. All 24 teams meeting the criteria agreed to take part in the study, and data were collected during the summer of 2001.
Research assistants interviewed the leaders/managers of these teams using a semi-structured interview containing the following instruments:
-
(a) The Team Organisation Questionnaire: a semi-structured questionnaire, developed specifically for the study, that collects information on team staffing, case-load, relationship to other providers in local health and social care provision and policies and protocols.
-
(b) The Dartmouth Assertive Community Treatment Scale (DACTS; Reference Teague, Bond and DrakeTeague et al, 1998): a measure of fidelity to the model of ACT with 28 fidelity items, each scored 1–5, with anchors provided for each point to facilitate scoring. Higher scores represent high fidelity. The scale is divided into three dimensions (human resources, organisational boundaries and nature of services) and is accompanied by brief guidelines for the scoring of each item. The wording of these guidelines was adapted for the current study.
-
(c) The International Classification of Mental Health Care (ICMHC; Reference de Jongde Jong, 1996): a World Health Organization tool encompassing, in ten modules, the disparate range of care that mental health services may provide and the level of expertise provided by a particular service.
The five researchers, who already knew the teams well through regular contact, received training in the questionnaires and had their initial interviews supervised (P.J.). Scoring was supplemented with additional information from the team, such as operational policies and case-load data. Following data collection, researchers met with two of the investigators (P.J. and C.W.) to check the data collected on all teams. This enabled anomalies to be resolved and ensured that scoring was conducted consistently.
Patient and carer contact recording
Recording of all contacts by teams with both patients and carers was undertaken during March 2002. This used a contact recording system already developed by Ford et al (Reference Ford, Repper and Cooke1993) and further adapted for use in the UK700 study (Reference Burns, Fiander and KentBurns et al, 2000), after some simplification and re-piloting. Individual workers, using booklets for each of the 4 weeks, recorded data on duration, site and primary purpose of each contact (telephone as well as face to face). The research assistants remained in regular contact with the teams during the month. Reliability checks on the contact recording were carried out by comparing the contact recording data with case note contact data collected in two censuses.
The patient and carer contact recording data were used in descriptive analysis of the provision of team contact with patients and also as a variable (‘proportion of patient contact in vivo’) in the team typology analysis.
Analysis
Descriptive statistics were derived using data from the questionnaires and the contact recording, and are presented in Table 1.
Table 1 Team organisation and patient and carer contacts for all 24 London assertive outreach teams
| Variable | Mean | s.d. | Median where mean is invalid1 | Range |
|---|---|---|---|---|
| Age of team (months) | 39.7 | 33.9 | 24.5 | 4-120 |
| Team case-load | 50.8 | 19.0 | N/A | 15-104 |
| Total staff FTEs | 7.7 | 2.9 | N/A | 3.1-15.0 |
| Ratio of full-time to part-time staff | 3.4 | 2.3 | 3.1 | 0.4-8 |
| Number of professional disciplines | 3.5 | 1.1 | N/A | 2-5 |
| FTE psychiatrist per 100 patients | 0.6 | 0.3 | N/A | 0-2.3 |
| Individual care coordinator case-load | 9.4 | 2.1 | N/A | 5-14 |
| Patients discharged in previous 6 months | 2.6 | 3.1 | 1.0 | 0-10 |
| Contacts per patient per week | 1.3 | 0.5 | N/A | 0.3-2.3 |
| Duration of contact (min) | 39.4 | 42.5 | 30.0 | 0-570 |
| Contacts out-of-hours (%) | 10.5 | 11.3 | 5.8 | 0-46.2 |
| Face to face contacts in community (%) | 61.6 | 13.9 | N/A | 25-88 |
| Face to face contacts in service setting (%) | 27.8 | 14.0 | 26.5 | 9-69 |
| Primary focus of contact (%) | ||||
| Engagement | 22.6 | 9.6 | 20.1 | 8-45 |
| Medication | 13.1 | 11.9 | 11.0 | 0-46 |
| Mental health assessment/intervention | 14.1 | 6.5 | 13.9 | 2-31 |
| Failed contacts per week | 9.6 | 6.6 | 8.6 | 1-22 |
For the cluster analysis, 14 variables were judged to be key to the classification and were used to characterise the 24 assertive outreach teams. These variables were determined by the research team as a result of literature searching: a previous systematic review of home treatment studies carried out by the same research group, which included a Delphi exercise on experts' views (Reference Burns, Knapp and CattyBurns et al, 2001), and preliminary experiential information gained by the research assistants about the London assertive outreach teams. These 14 variables are listed in Table 2. Where possible continuous variables were used, although some of necessity remained binary. Because the variables were on different scales, it was necessary to re-scale them to give equal weight. This was done by replacing each variable with its rank among the teams. Ties were dealt with by assigning average ranks.
Table 2 Variables used in cluster analysis, with descriptions of the three clusters identified from average linkage, LI cluster analysis

| Variable | % of mean across all teams (range where applicable) (n=24) | Cluster A (n=14) | Cluster B (n=4) | Cluster C (n=6) |
|---|---|---|---|---|
| Statutory status (%) | 71 | 100 | 75 | 0 |
| Responsible for CPA (%) | 75 | 100 | 100 | 0 |
| FTE psychiatrist per 100 patients | 0.6 (0.0-2.3) | 1.0 | 0.0 | 0.0 |
| Has integrated health and social care (%) | 71 | 93 | 100 | 0 |
| Number of professional disciplines1 | 3.5 (2.0-5.0) | 4.0 | 3.0 | 2.7 |
| Patient contacts in vivo (%) | 41 (16-67) | 36 | 31 | 45 |
| Number of FTE clinical staff | 7.7 (3.1-15.1) | 8.4 | 7.7 | 6.2 |
| Ratio of full-time to part-time clinical staff | 3.4 (0.4-8.0) | 2.0 | 5.8 | 5.2 |
| Team leader's time in clinical work (%) | 29 (0-90) | 30 | 58 | 6 |
| Operates outside Monday to Friday (%) | 50 | 64 | 50 | 17 |
| Regularly operates outside normal office hours (Monday-Friday, 08.30-17.30 h) (%) | 38 | 57 | 25 | 0 |
| Has 24-h responsibility for psychiatric crises2 | 1.9 (1-4) | 1.79 | 2.5 | 1.8 |
| Has dedicated in-patient beds (%) | 21 | 36 | 0 | 0 |
| Mean individual case-load | 9.5 (5.0-14.0) | 8.7 | 10.4 | 10.8 |
| Variable not used to construct cluster Age (months) | 40 (4-120) | 39 | 36 | 44 |
Hierarchical methods of cluster analysis were then used with an L1 (City Block) dissimilarity measure applied to the ranks (Reference Everitt, Landau and LeeseEveritt et al, 2001). The L2 (Euclidean) measure was used as a sensitivity analysis, as were complete- and single-linkage methods (average linkage having been used in the main analysis). Individual team and individual variable omission were used in the sensitivity analysis to determine whether individual items were highly significant to the classification results. The number of clusters was determined by viewing the dendrogram in order to identify well-separated groups.
RESULTS
Who are these assertive outreach teams?
Table 1 lists results from the Team Organisation Questionnaire, their means and ranges and ‘patient and carer contacts’. Thirteen teams (54.2%) identified their locality population by aligning by borough, with a further eight (33%) by geographical area. Seven of the 24 assertive outreach teams were run by not-for-profit voluntary agencies.
Staff composition
Team size varied considerably, both in total case-load and in total staff full-time equivalents (FTEs). Two teams (8.3%) had fewer than six FTE staff and nine teams (52.9%) had a full-time/part-time staff ratio of 2 or less (i.e. a high proportion of part-time staff). All teams were multi-disciplinary. Nursing was the predominant profession, with a mean of 5.6 total FTE per 100 patients, followed by support workers (4.6 FTE per 100). Seven teams (29.2%) had no unqualified staff. All teams except one had some social worker input but with a range per 100 patients of between 1 FTE or less in one team (4.2%) to 5–7 FTEs in four teams (16.7%). Ten teams (42%) had no input from a psychiatrist and six teams (25%) had less than 1 FTE per 100 patients. A further six teams (25%) had between 1 and 2 FTEs and two teams (8.4%) had between 2 and 3 FTEs. Clinical psychologists were only present in a minority of ten teams.
Integration of health and social care
Of the 17 statutory teams, eight (47.1%) had no integration of health and social care. Sixteen statutory teams (94%) had a social worker co-located and managed within the assertive outreach team as a care coordinator.
In-patient responsibility
Only five teams (20.8%) had designated in-patient beds for their patients, with a mean number of beds per team of 9.8 (s.d.=4.9, range 5–18). Six teams (25%) retained full medical responsibility for all their patients during periods of admission to hospital, one team retained responsibility for some patients and the other 17 teams (71%) handed over medical responsibility.
Case-loads and referrals
Individual case-loads varied considerably, with a mean average of 9.4 (s.d.=2.1, range 5–14) per FTE. All assertive outreach teams accepted patients referred from community mental health teams or other specialist mental health services, but acceptance from other agencies was more limited. Nine teams (37.5%) accepted from other health agencies, seven (29.2%) from each of primary care, social care agencies and voluntary agencies, five (20.8%) from self-referral and three (12.5%) from other sources.
Criteria for acceptance of patients onto the team case-load included the age of the patient (21 teams, 87.5%), previous difficulty in engagement (20 teams, 83.3%), specific diagnoses (19 teams, 79.2%), previous hospitalisations (15 teams, 62.5%) and minimum duration of illness (13 teams, 54.2%); 22 teams (91.7%) reported ‘other’ acceptance criteria, such as geographical catchment area and being in contact with other mental health services.
Patient and carer contact recording
Contact timing and frequency
The total number of contacts (both successfully achieved and failed contacts) by staff in assertive outreach teams with their patients during the 1-month recording period was 7012. The mean number of contacts received by an assertive outreach patient per week ranged from 0.3 to 2.3. Considering only successful contacts, the median duration for these contacts for all teams was 30 min, with a range of 1–570 min and the majority between 1 and 15 min. Most contacts (81.5%) were within office hours (Monday–Friday, 08.00–18.00 h); only 9.3% were recorded as ‘out of hours’.
Nature of contacts
Of the assertive outreach team contacts, 67.7% were face to face with the patient, 13.1% were by telephone, 11.1% of all attempts at contact ended in failure and a further 6.1% involved contact with the carer (face to face or by phone). Of the face to face contacts with patients, 63% took place in the patient's home or neighbourhood (so called ‘in vivo’), 27.4% in service settings and 9.7% in other settings.
Team staff also recorded the primary focus of their contact with the patient. The most common of the ten focus categories was engagement (21.3%), followed by medication (17.1%) and specific mental health assessment or intervention (15.1%). All other primary focus topics were present with less than 10% frequency: housing (7.5%), occupation and leisure (7.6%), daily living skills (7.0%), finance (5.1%), carers/significant others (2.9%), physical health (2%) and criminal justice system (1.0%).
Cluster analysis results
Table 2 lists the variables used in the cluster analysis, their distribution and (where appropriate) their means and ranges, for both the total sample and for the three clusters identified from the dendrogram illustrated in Fig. 1.
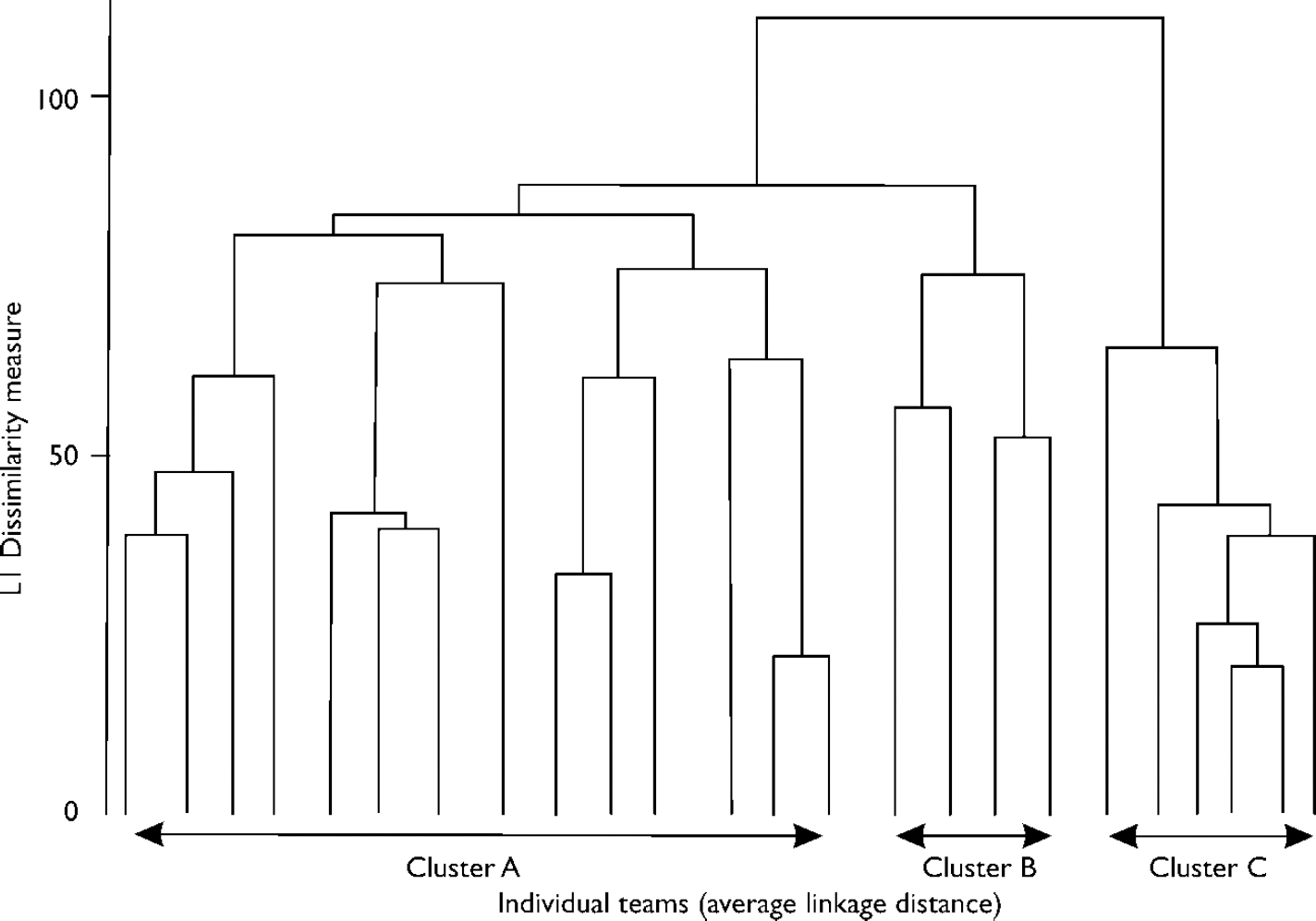
Fig. 1 Dendrogram of teams using average linkage method. All methods use the L1 dissimilarity measure and ranked data.
Cluster C, the most distinct cluster identified by the analysis, consists entirely of voluntary agency teams that do not hold formal clinical responsibility (e.g. the Care Programme Approach, CPA). Inevitably, they lack integrated health and social care provision and dedicated beds. These teams have no input from a psychiatrist, fewer disciplines represented (mean=2.7) and tend to be smaller (mean=6.2 FTE staff, range 5–9). However, they provide the highest percentage of ‘in vivo’ contacts to patients (45%). They have very little service provision outside of weekday office hours, with only one team offering some weekend service.
Clusters A and B comprise teams with CPA responsibility, although cluster B includes one voluntary agency team. All but one of the teams provide integrated health and social care. Clusters A and B differ in several regards. Cluster B teams have no psychiatrist input and no dedicated in-patient beds, whereas cluster A teams had a mean of 1.0 FTE psychiatrist per 100 patients and 36% had dedicated in-patient beds. Cluster A teams also tended to be more multi-disciplinary (mean of four per team v. three in cluster B) and to have more part-time staff (full-time: part-time ratio of 2.0 v. 5.8). They also tended to have smaller individual case-loads (mean of 8.7 v. 10.4) and to operate more outside of office hours (57% of teams v. 25%).
The frequency of patient contacts also varied by cluster. The overall figure for all teams is approximately 1.3 (s.d.=0.5) contacts per week. However, this varied with 1.36 contacts per week for cluster A teams, 1.45 for cluster B teams and 0.97 for cluster C teams. Thus, the voluntary sector teams of cluster 3 showed a tendency to have fewer contacts per week but with a higher proportion of contacts taking place in the patient's home or community setting.
Sensitivity analyses
Use of the L2 metric clearly identified clusters A, B and C (Fig. 1). Scaling by the standard deviation and the range also clearly identified cluster C but failed to identify cluster B. This is probably because the distinctive characteristics of cluster B are described by skewed continuous variables that have less influence with these approaches. Omitting the ‘percentage of patient contacts in vivo’ variable did not detract from the clear identification of clusters A, B and C. Taken together, these analyses support the definition of three main clusters.
To see whether any individual teams were highly influential, we omitted one team at a time and examined the impact on the classification of the remaining teams. Of these 24 analyses, 20 identified cluster C as most distinct, followed by clusters A and B. One analysis identified cluster A as most distinct, followed by clusters B and C. The remaining analyses separated cluster A from cluster C but did not identify cluster B.
Correlation with independent scales
The Dartmouth Assertive Community Treatment Scale
The mean DACTS score for all teams was 3.4 (s.d.=0.4), with a range of 2.3–4.1. Three teams (12.5%) scored a mean of 4 or more (usually taken as ‘high fidelity’), seventeen teams (71%) scored means of 3–3.9 and four teams (16.5%) scored means of 2–2.9 (‘low fidelity’).
The 28 individual items in the DACTS were ranked according to their mean score. Nine items had a mean score of 4–5 (high fidelity), eleven items had a mean score of 3–3.9 and eight items had scores of less than 2.9 (low fidelity). Of these, four had a mean score of 2–2.9 and four had a mean score of 1–1.9. Table 3 lists those variables where London teams showed high and low fidelity.
Table 3 Dartmouth Assertive Community Treatment Scale variables demonstrating ‘high model fidelity’ (> 4) and ‘low model fidelity’ (< 3) across London assertive outreach teams
| Score of ≥ 4 (‘high fidelity’ items) | Mean | Score of < 3 (‘low fidelity’ items) | Mean |
|---|---|---|---|
| H1 Small individual case-load | 4.7 | H7 Senior permanent psychiatrist on staff | 2.9 |
| H6 High proportion of team posts filled | 4.1 | H9 Substance misuse specialist on staff | 2.2 |
| O1 Explicit intake criteria for patients | 4.4 | H10 Vocational specialist on staff | 1.8 |
| O2 Intake rate of patients low | 4.9 | O4 Responsibility for 24-h crises | 1.9 |
| O3 Full responsibility for treatment services | 4.2 | S5 Frequency of contact | 2.7 |
| O7 Time-unlimited services | 4.4 | S7 Individualised substance misuse treatment | 2.7 |
| S1 High proportion of service in vivo | 4.1 | S8 Dual disorder treatment groups | 1.1 |
| S2 ‘No drop-out’ policy | 4.4 | S10 Role of users on team | 1.7 |
| S3 Assertive engagement mechanisms used | 4.5 |
Figure 2 shows the mean DACTS score for all teams and for clusters A, B and C. It also presents the DACTS mean scores by its three dimensions: human resources, organisational boundaries and nature of services.
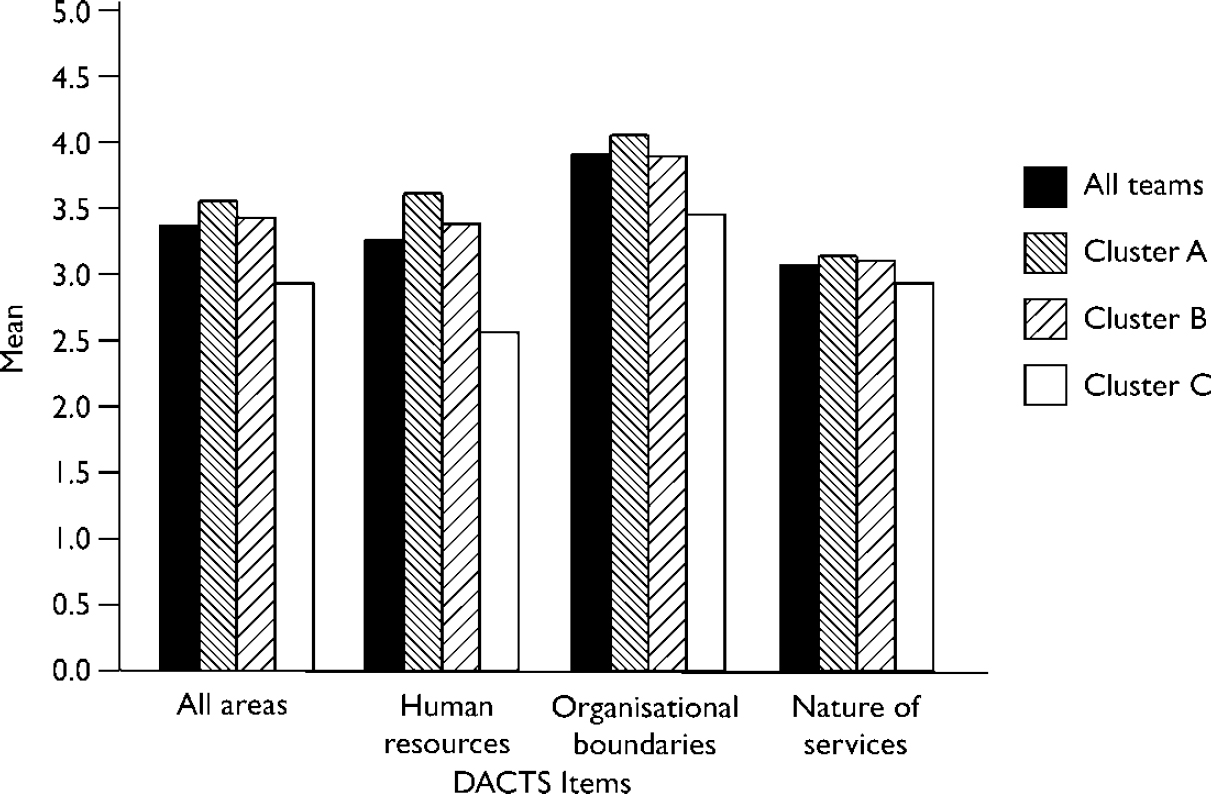
Fig. 2 Mean Dartmouth Assertive Community Treatment Scale (DACTS) scores for all teams, for each cluster and for each dimension of the scale.
Teams in cluster A tended to show higher fidelity in all three dimensions, although this was less marked in the ‘nature of services’ dimension. In the ‘human resources’ dimension, cluster C's fidelity score was reduced by their employing support workers without mental health qualifications. However, they also scored lower on other items in this dimension that were not staff-dependent: degree to which a team approach is used, how often a team meets to review all patients and how clinically active the team leader is. Within organisation boundaries, two of the seven items differentiated cluster C teams from A and B. Not surprisingly, given their voluntary agency status, these were their lack of involvement in the hospital admission and discharge of their patients.
The ‘nature of services’ dimension did not clearly differentiate between the three clusters.
The International Classification of Mental Health Care
Each of ten modules of care are scored high (3), medium (2) or low (1) on the level of specialisation provided by the team. It is also possible to rate the service as not applicable to the module of care (0). Figure 3 shows the mean ICHMC scores for each module of care, both for all teams and by cluster.

Fig. 3 Mean International Classification of Mental Health Care scores for each module of care, by all teams and by team cluster: module 1, establishing and maintaining relationships; module 2, assessment; module 3, care coordination; module 4, general health care; module 5, taking over activities of daily living; module 6, psychopharmacological and other somatic interventions; module 7, psychological interventions; module 8, (re)educating basic, interpersonal and social skills; module 9, interventions related to daily activities; module 10, interventions aimed at family, relatives and others.
All teams scored 3 for module 1, ‘establishing and maintaining relationships’. Teams scored highly on modules 2 (‘assessment’) and 3 (‘care coordination’), with means of 2.4 and 2.5, respectively. Overall mean scores for other modules were lower and mostly in the range 1.5–2. Cluster C teams consistently scored lower than cluster A and B teams in all modules other than module 1.
DISCUSSION
Role of the voluntary sector
Almost one-third of London's assertive outreach teams are run by voluntary agencies. One further team previously had been non-statutory but was recently incorporated into a National Health Service trust. These non-statutory teams were clearly identifiable as a distinct group on the cluster analysis as well as on the DACTS and ICMHC, where they held a lower fidelity to the assertive outreach model as measured by the DACTS and offered lower levels of specialisation on the ICMHC modules.
The cluster C teams differed in other ways also, often having a specific target group or holding to a particular ideology of care: two teams have a particular focus on African–Caribbean patients; one team focuses on young people (less than 25 years old); and another team targets asylum seekers and recent immigrants. Several spoke of working to a ‘social inclusion model’ and of holding a ‘true team approach’. In two teams all staff are employed as mental health workers or support workers rather than by their professional backgrounds, and in one team all staff received the same salary. Voluntary agency staff were also more likely to be reported as living in the area served. One team spoke of having a ‘pre-engagement’ role, with a view to later engagement of their clients in the local statutory services.
Voluntary agency teams may not play such a strong role in assertive outreach provision outside London but their role within London is clearly significant. There would appear to be a need for more consideration of the place of the non-statutory sector teams within the local health economies and service provision. Their role in implementing the statutory responsibility of the CPA – a set of principles for organising mental health care in the UK that is required in law – is already developing. One team already holds CPA responsibility and agreement is in place for a further team to take this on in the near future. Only one voluntary agency team reported poor relationships with local statutory services.
Integrated health and social care provision and hospitalisation
An integrated health and social care service was one of only two components demonstrated to be associated with reduced hospitalisation in a systematic review of home treatment services (Reference Burns, Knapp and CattyBurns et al, 2001). In our sample only half of the statutory teams fulfilled this integrated provision, although it was clear that this was changing rapidly: 79.2% of teams (19) had no designated in-patient beds and only 29% (7) retained any medical responsibility for their admitted patients. There is a fault-line in patients' care at the point of hospital admission. Receiving teams may not fully understand or accept assertive outreach approaches, and thereby fail to achieve the earlier discharge that has been identified as one of its strengths. This has implications for expectations of the effectiveness of assertive outreach teams in reducing the length of hospital stay. Continuity of responsibility of medical care across community and in-patient provision by assertive outreach services requires careful consideration.
Contact with patients
Several of the assertive outreach teams within the study were already employing some form of patient and carer contact recording, either as part of a wider patient information database or for the purposes of clinical audit. Although issues of quality and comparability made it impossible to use these in this study, this is an encouraging development. These do not, as yet, record the provision of specific, defined interventions, and it is highly likely that it is such interventions (rather than patterns of contacts) that affect outcomes (Reference Burns, Creed and FahyBurns et al, 1999).
The Dartmouth Assertive Community Treatment Scale
The mean score on the DACTS for all teams was 3.41, which would indicate moderate fidelity. Compared with the US teams investigated by Teague et al (Reference Teague, Bond and Drake1998) this is close to the ‘ACT-like’ teams (mean=3.47) but lower than the ACT replication teams (mean=4.01).
More striking, however, is the great variation in the London teams' DACTS mean scores. Most teams (71%) reflected a moderate level of fidelity, with three teams scoring above 4. However, with the highest at 4.14, this indicates that even these teams were not implementing some of the features of the model. Four of the teams scored a mean of below 3, suggesting that there were many items of the DACTS that were not being adhered to. Cluster A teams have the highest fidelity scores. When ranked by the DACTS mean score, ten of the top eleven teams were from cluster A. Conversely, four of the six cluster C teams had the lowest DACTS means (the other two cluster C teams being ranked sixteenth and seventeenth).
The DACTS is a multi-dimensional measure and mean scores have limited value. Nine individual DACTS criteria scored a mean of 4 or above, spread across the three dimensions of DACTS, indicating that most London assertive outreach teams are doing well at implementing these elements of ACT. Some of these were expected, given our team inclusion criteria, such as having ‘small individual case-loads’ and ‘time-unlimited services’. Others included providing a ‘high proportion of service in vivo’ and the team having ‘full responsibility for treatment services’ (such as housing and employment support). However, eight DACTS items scored a mean of less than 3, suggesting that London assertive outreach teams differ significantly from their US counterparts in score. Of these eight, three related to expertise and service provision in substance misuse care and a further two to the low level of senior psychiatrist and vocational specialist input to the teams. The ‘frequency of contact’ with patients, the ‘role of users on team’ and having ‘responsibility for 24-h crises’ also showed poor fidelity within DACTS.
Exporting health care structures from one national system to another is likely to reveal differences. Examples of this are: the presence of staff in the team who have at least one year of training or experience in substance misuse or vocational specialities; and the details of what ‘integrated health and social care’ means. An understanding of how the teams fit into their own national system of health care is essential for interpreting their ‘fidelity’ scores.
In addition, we found that the DACTS omits team characteristics that we considered important, both from the literature and from clinical experience for assessing care within a non-US context. Only 6 out of 14 variables that were considered in the cluster analysis are reflected in the DACTS. We believe that the DACTS is a more ‘culture-bound’ instrument than has been acknowledged previously and we would recommend that in a non-US context the other eight items used in this cluster analysis be included.
The DACTS overall mean score tells us little about the profile of the service characteristics of teams. It is quite possible for two teams to score equally on the overall DACTS while incorporating substantially different components of care. More work needs to be done to establish the relative importance of different components of care within the assertive outreach model.
Implications for future assertive outreach services in the UK
The role of assertive outreach teams in mental health services in the UK is developing rapidly, with policy support in the National Service Framework for Mental Health (Department of Health, 1999) and the Mental Health Policy Implementation Guide (Department of Health, 2001). Our study suggests that currently the term ‘assertive outreach team’ is not indicative in London of a single implementation model, nor necessarily of teams including the characteristics required by Department of Health guidance. Recruiting clinical psychologists was reported as particularly difficult and few teams had achieved it. Similarly, there were some teams with a high proportion of part-time staff, which was seen as unsatisfactory. It is also clear that some of the accepted wisdom of the US ACT model and the means of assessing its implementation through the DACTS do not easily translate to the UK system of care. Assertive community treatment is being adopted as policy in a number of countries outside the USA. We would propose that their likely heterogeneity presents a clinical challenge but also a research opportunity in distinguishing effective from redundant components of the prescribed model.
APPENDIX
Members of the Pan–London Assertive Outreach Study Group
Tom Burns, Christine Wright, Peter James, Adele Greaves, Christine Benfell, Nan Greenwood (St George's Hospital Medical School); Paul Bebbington, Sonia Johnson, Joanne Billings (University College London and Camden and Islington Mental Health and Social Care Trust); Stefan Priebe, Walid Fakhoury, Joanna Watts (Unit for Social and Community Psychiatry, Barts and The London School of Medicine); Matt Muijen, Iain Ryrie, Rebecca Walwyn (Sainsbury Centre for Mental Health); Ian White (Medical Research Council Biostatistics Unit).
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ London assertive outreach teams vary considerably in their service characteristics and in their fidelity to the assertive community treatment model.
-
▪ The teams form three groups on cluster analysis, supported by differences in scores on independent scales of model fidelity and interventions. Teams in the voluntary sector are clearly distinct in their practice.
-
▪ Currently, assertive outreach teams in London do not necessarily match the characteristics proposed in UK guidance.
LIMITATIONS
-
▪ We cannot assume that London teams are representative of assertive outreach teams elsewhere in the UK.
-
▪ We cannot comment on the relative effectiveness of the teams in each of the three clusters.
-
▪ Teams are rapidly evolving and practice was not consolidated in all services.
Acknowledgements
We thank those who were involved in the development of the study: Peter Tyrer, Kevin Gournay, Graham Thornicroft, Tom Craig and Angela Greatley. This study was also developed and carried out partly under the auspices of The London Mental Health Virtual Institute for Research and Development (LoMHR&D).







eLetters
No eLetters have been published for this article.